Proposal for Endoscopic Ultrasonography Classification for Small Pancreatic Cancer

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
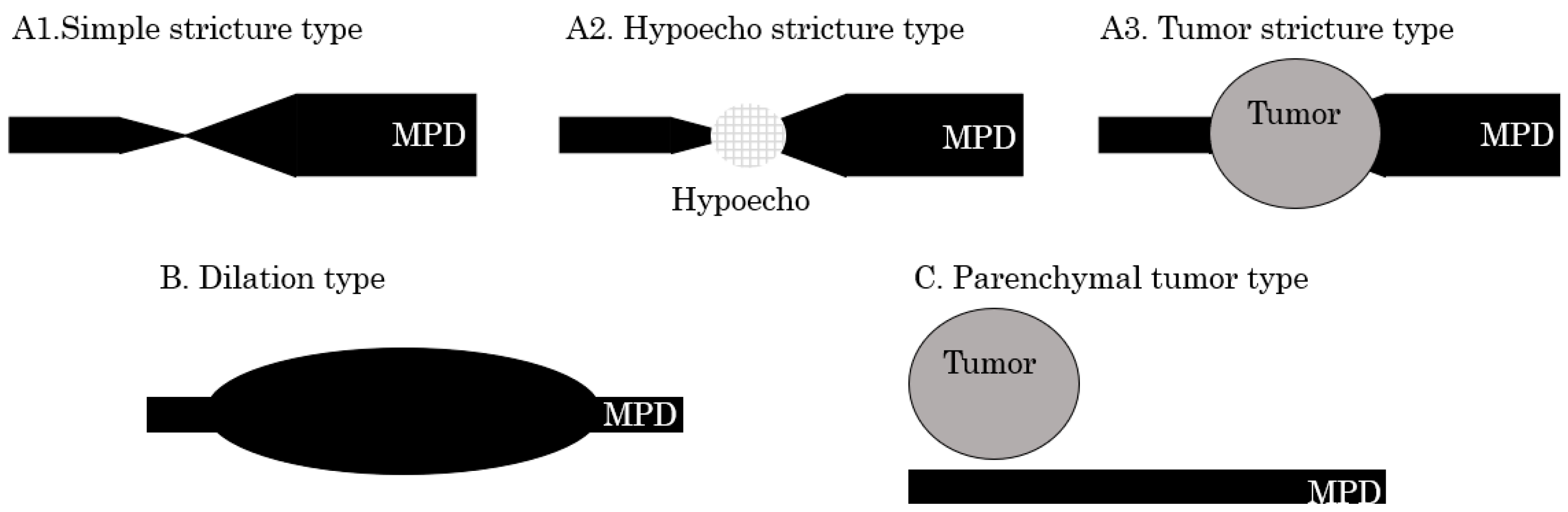
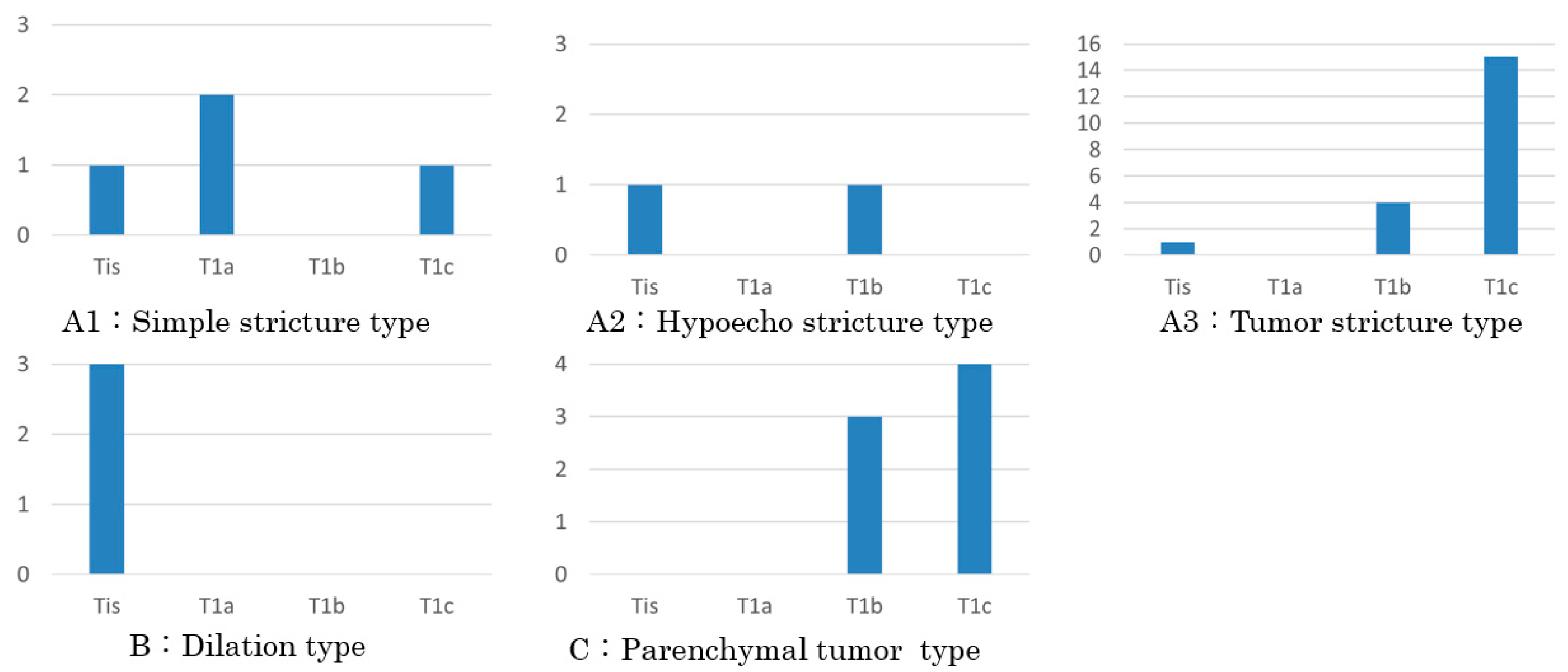
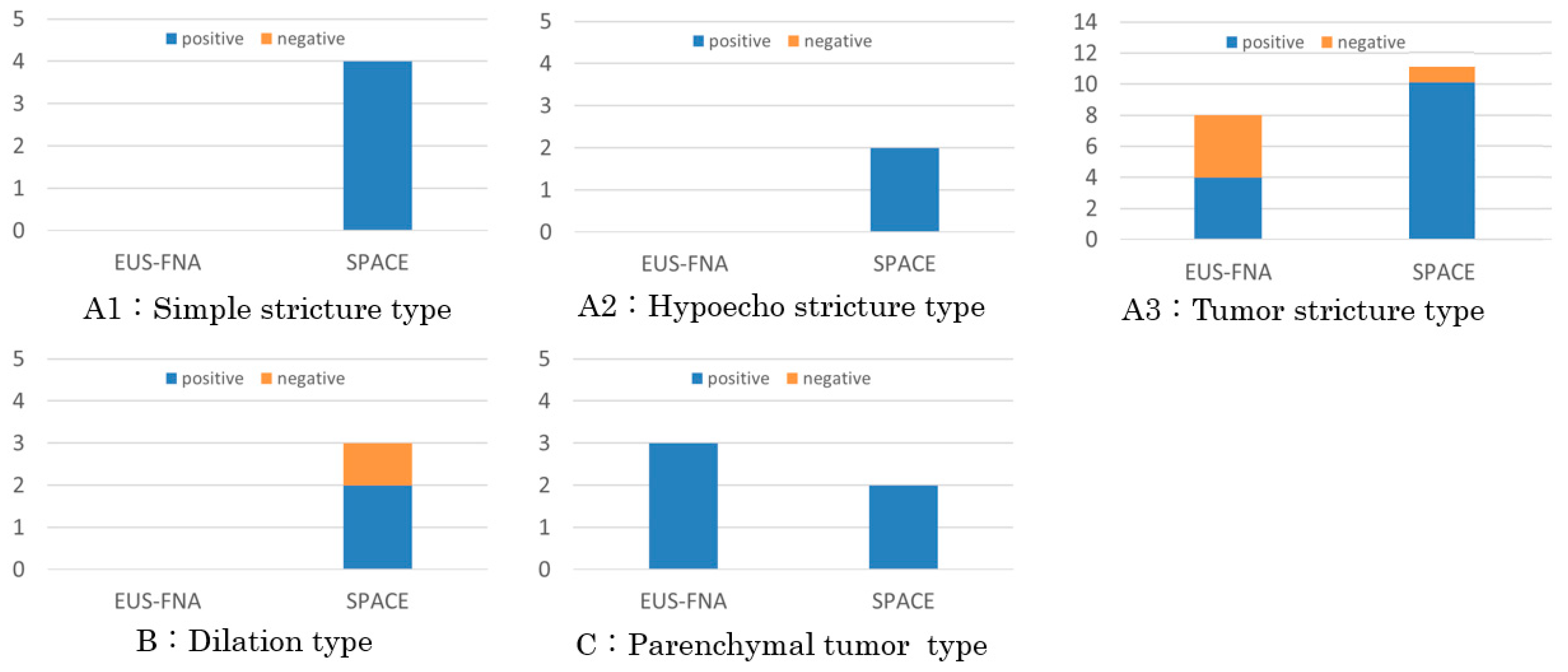
3. Classification of EUS findings
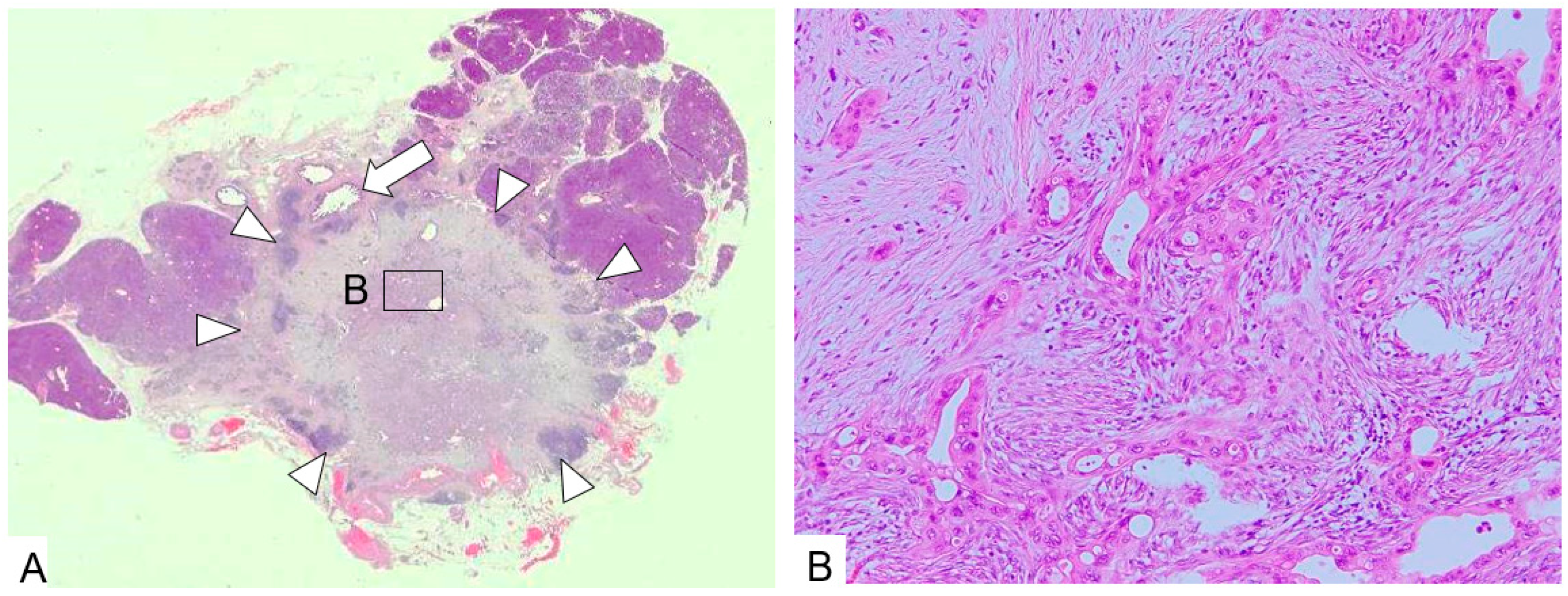
- A1: Simple stricture type—an MPD was strictured without any other findings;
- A2: Hypoecho stricture type—a strictured part was surrounded by a focal hypoechoic area without clear demarcation;
- A3: Tumor stricture type—a tumor with clear demarcation was recognized in the strictured part.
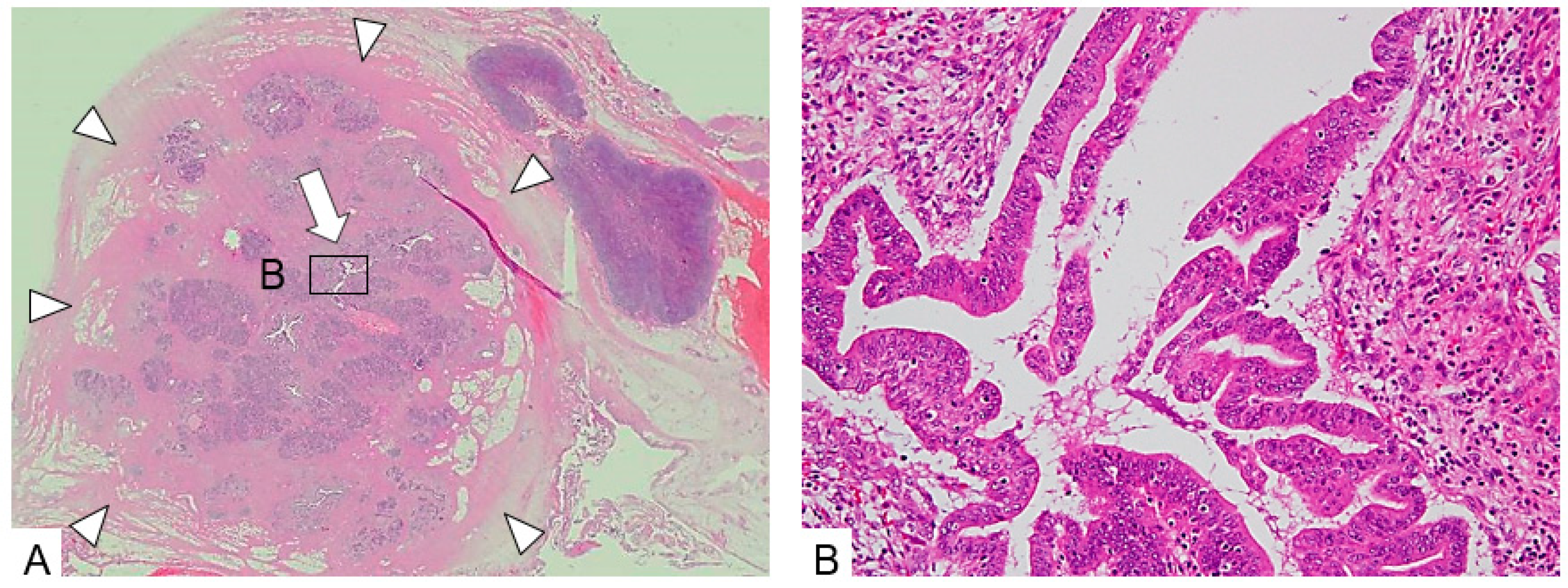
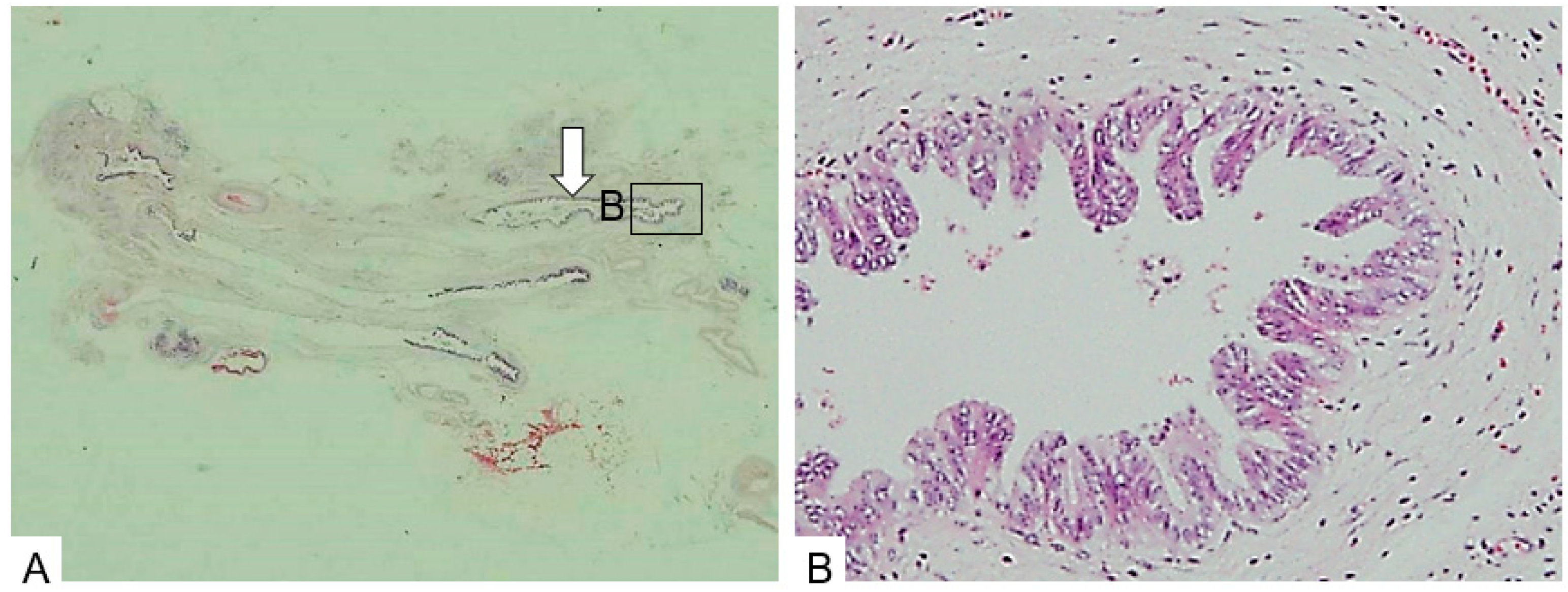
- B: Dilation type—an MPD or a branch duct was dilated without a downstream stricture;
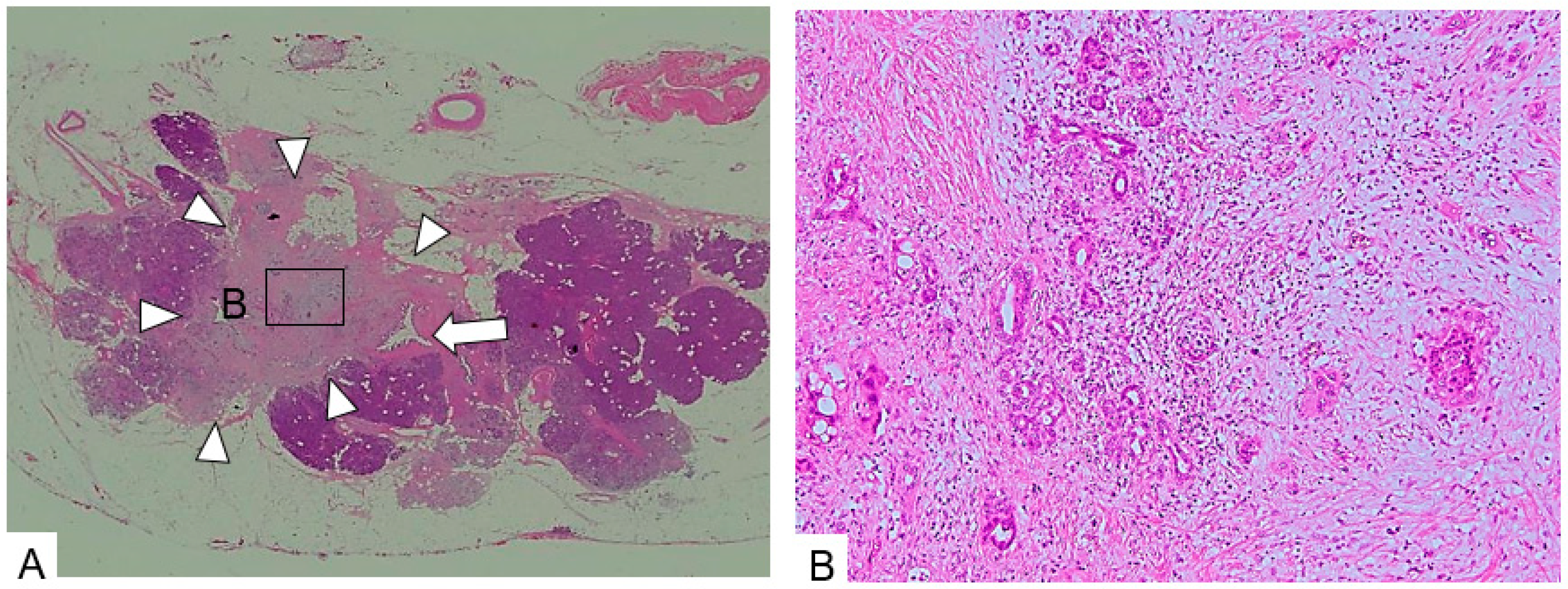
- C: Parenchymal tumor type—a pancreatic tumor with clear demarcation located apart from the MPD.
4. Results
4.1. Patient Characteristics
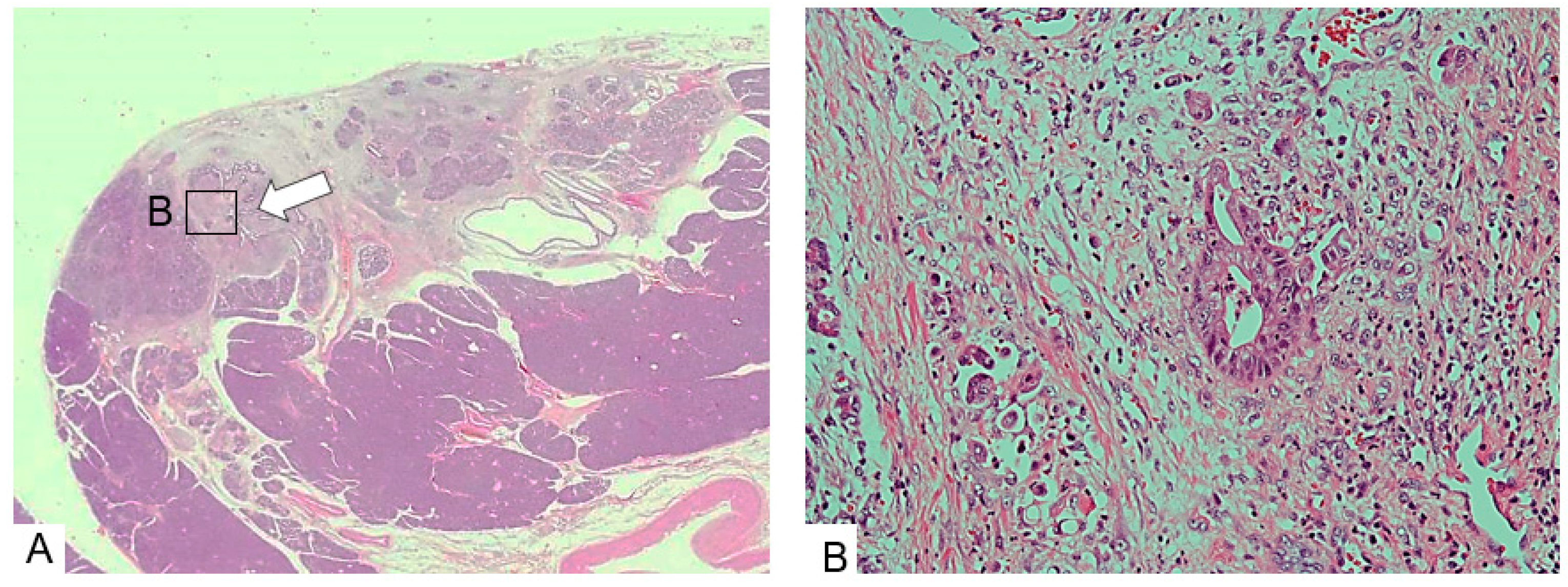
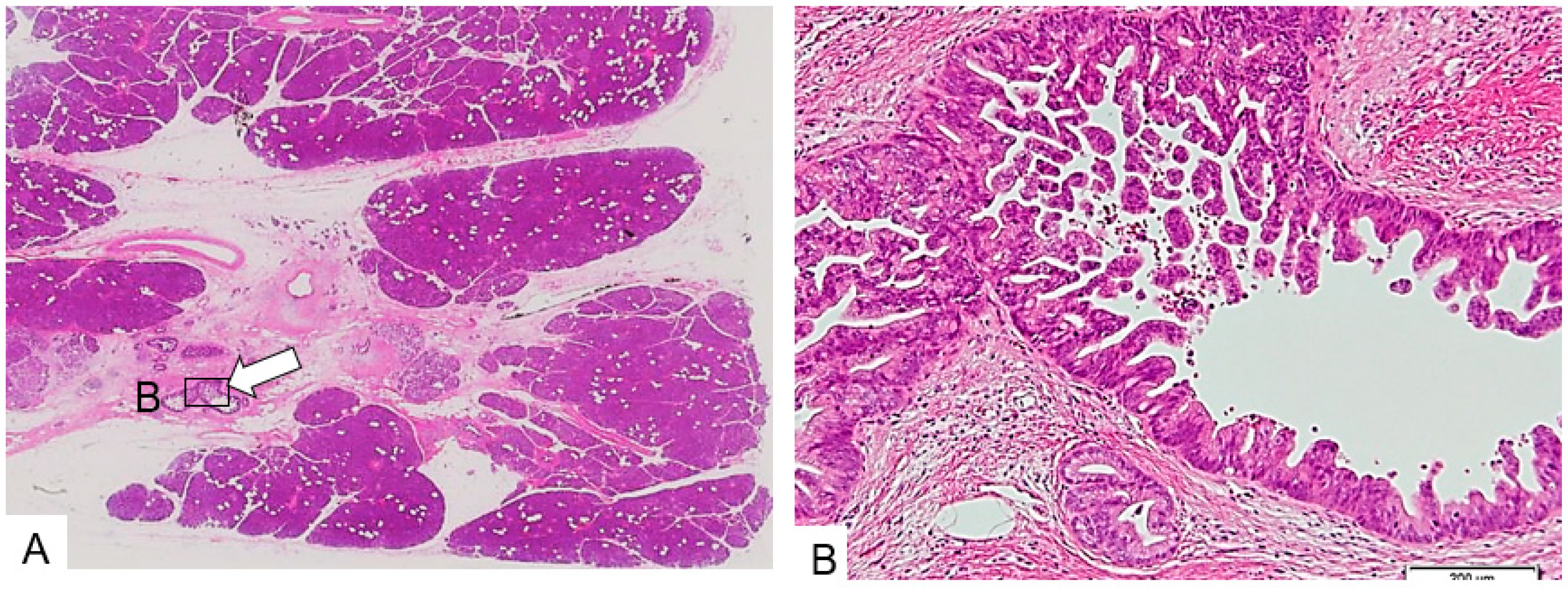
4.2. EUS Findings and Pathological Findings
4.3. Preoperative Diagnostic Procedures
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- Sǎftoiu, A.; Vilmann, P. Role of endoscopic ultrasound in the diagnosis and staging of pancreatic cancer. J. Clin Ultrasound 2009, 37, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, S.H.; Lee, J.M.; Cho, J.Y.; Lee, K.B.; Kim, J.E.; Moon, S.K.; Kim, S.J.; Baek, J.H.; Kim, S.H.; Kim, S.H.; et al. Small (≤20 mm) pancreatic adenocarcinoma: Analysis of enhancement patterns and secondary signs with multiphasic multidetector CT. Radiology 2011, 259, 442–459. [Google Scholar] [CrossRef] [PubMed]
- Harinck, F.; Konings, I.C.A.W.; Kluijt, I.; Poley, J.W.; van Hooft, J.E.; van Dullemen, H.M.; Nio, C.Y.; Krak, N.C.; Hermans, J.J.; Aalfs, C.M.; et al. A multicenter comparative prospective blinded analysis of EUS and MRI for screening of pancreatic cancer in high-risk individuals. Gut 2016, 65, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Kamata, K.; Kitano, M.; Kudo, M.; Sakamoto, H.; Kadosaka, K.; Miyata, T.; Imai, H.; Maekawa, K.; Chikugo, T.; Kumano, M.; et al. Value of EUS in early detection of pancreatic ductal adenocarcinomas in patients with intraductal papillary mucinous neoplasms. Endoscopy 2014, 46, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, C.; Luigiano, C.; Maimone, A.; Tarantino, I.; Baccarini, P.; Fornelli, A.; Liotta, R.; Polifemo, A.; Barresi, L.; Traina, M.; et al. Endoscopic ultrasound-guided fine-needle biopsy of small solid pancreatic lesions using a 22-gauge needle with side fenestration. Surg. Endosc. 2015, 29, 1586–1590. [Google Scholar] [CrossRef] [PubMed]
- Iiboshi, T.; Hanada, K.; Fukuda, T.; Yonehara, S.; Sasaki, T.; Chayama, K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer. Pancreas 2012, 41, 523–529. [Google Scholar] [CrossRef]
- Hanada, K.; Okazaki, A.; Hirano, N.; Izumi, Y.; Teraoka, Y.; Ikemoto, J.; Kanemitsu, K.; Hino, F.; Fukuda, T.; Yonehara, S. Diagnostic strategies for early pancreatic cancer. J. Gastroenterol. 2015, 50, 147–154. [Google Scholar] [CrossRef]
- Satoh, T.; Kikuyama, M.; Kawaguchi, S.; Kanemoto, H.; Muro, H.; Hanada, K. Acute pancreatitis-onset carcinoma in situ of the pancreas with focal fat replacement diagnosed using serial pancreatic juice aspiration cytologic examination (SPACE). Clin. J. Gastroenterol. 2017, 10, 541–545. [Google Scholar] [CrossRef]
- Kanno, A.; Masamune, A.; Hanada, K.; Maguchi, H.; Shimizu, Y.; Ueki, T.; Hasebe, O.; Ohtsuka, T.; Nakamura, M.; Takenaka, M.; et al. Multicenter study of early pancreatic cancer in Japan. Pancreatology 2018, 18, 61–67. [Google Scholar] [CrossRef]
- Kikuyama, M.; Hanada, K.; Ueki, T. Pancreatic carcinoma in situ presenting prominent fatty change of the pancreatic body on CT: Experiences from 3 cases. Suizo 2015, 30, 626–632, (In Japanese with English abstract). [Google Scholar] [CrossRef]
- Seki, M.; Ninomiya, E.; Takano, K.; Fujita, R.; Aruga, A.; Yamada, K.; Tanaka, H.; Matsueda, K.; Mikami, K.; Hiki, N.; et al. Pancreatogram findings for carcinoma in situ (CIS) of the pancreas seen on endoscopic retrograde cholangiopancreatography and postoperative pancreatography of resected specimens: Can CIS be diagnosed preoperatively? Pancreatology 2008, 8, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. UICC TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2016. [Google Scholar]
- Kawaguchi, S.; Kikuyama, M.; Satoh, T.; Terada, S.; Kanemoto, H.; Arai, K. Minimally invasive ductal pancreatic carcinoma without low echoic area on endoscopic ultrasound examinations: a case report. Suizo 2017, 32, 852–858. (In Japanese) [Google Scholar] [CrossRef]
- Schlitter, A.M.; Jesinghaus, M.; Jäger, C.; Konukiewitz, B.; Muckenhuber, A.; Demir, I.E.; Bahra, M.; Denkert, C.; Friess, H.; Kloeppel, G.; et al. pT but not pN stage of the 8th TNM classification significantly improves prognostication in pancreatic ductal adenocarcinoma. Eur. J. Cancer 2017, 84, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Kikuyama, M.; Kamisawa, T.; Kuruma, S.; Chiba, K.; Kawaguchi, S.; Terada, S.; Satoh, T. Early Diagnosis to Improve the Poor Prognosis of Pancreatic Cancer. Cancers (Basel) 2018, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Minami, T.; Hanada, K.; Hirano, N.; Okazaki, A.; Ikemoto, J.; Fukuhara, M. Diagnosis of pancreatic carcinoma in situ. Suizo 2017, 32, 50–55. (In Japanese) [Google Scholar] [CrossRef]
- Kato, S.; Chinen, K.; Shinoura, S.; Kunishima, F. Pancreatic Duct Stricture That Rapidly Progressed to Pancreatic Ductal Adenocarcinoma and Formed a Mass within 3 Months: A Case Report. Case Rep. Gastroenterol. 2018, 12, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Kuang, C.; Xiao, Y.; Liu, X.; Stringfield, T.M.; Zhang, S.; Wang, Z.; Chen, Y. In vivo disruption of TGF-β signaling by Smad 7 leads to premalignant ductal lesions in the pancreas. PNAS 2006, 103, 1858–1863. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Zakimi, M.; Yamada, K. Efficacy of repeated cytology of pancreatic juice obtained by endoscopic nasopancreatic drainage tube for early diagnosis of pancreatic cancer: A case series including a case of carcinoma in situ. Clin. J. Gastroenterol. 2015, 8, 240–246. [Google Scholar] [CrossRef]
- Hatori, T.; Fukuda, A.; Onizawa, S.; Tomioka, H.; Yamamoto, M.; Imaizumi, T.; Takasaki, K. Carcinoma In Situ Of The Pancreas: 3 Case Reports. Pancreas 2005, 31, 445–446. [Google Scholar] [CrossRef]
- Takano, Y.; Nagahama, M.; Yamamura, E. A case of concurrent pancreatic intraepithelial neoplasia and type 1 autoimmune pancreatitis with marked pancreatic duct dilatation. Clin. J. Gastroenterol. 2016, 9, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, K.; Yamamoto, Y. Endoscopic measurement of pancreatic main ductal pressure in the various stages of chronic pancreatitis and the effect of exogenous secretin and glucagon on pancreatic ductal pressure. Nihon Shokakibyo Gakkai Zasshi 1985, 82, 1924–1931. (In Japanese) [Google Scholar] [PubMed]
- Yasuda, I.; Iwashita, T.; Doi, S.; Nakashima, M.; Moriwaki, H. Role of EUS in the early detection of small pancreatic cancer. Dig. Endosc. 2011, 23, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Takeda, Y.; Onoyama, T.; Kawata, S.; Kurumi, H.; Ueki, M.; Miura, N.; Isomoto, H. Role of the preoperative usefulness of the pathological diagnosis of pancreatic diseases. World J. Gastrointest. Oncol. 2016, 15, 656–662. [Google Scholar] [CrossRef] [PubMed]










© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terada, S.; Kikuyama, M.; Kawaguchi, S.; Kanemoto, H.; Yokoi, Y.; Kamisawa, T.; Kuruma, S.; Chiba, K.; Honda, G.; Horiguchi, S.; et al. Proposal for Endoscopic Ultrasonography Classification for Small Pancreatic Cancer. Diagnostics 2019, 9, 15. https://doi.org/10.3390/diagnostics9010015
Terada S, Kikuyama M, Kawaguchi S, Kanemoto H, Yokoi Y, Kamisawa T, Kuruma S, Chiba K, Honda G, Horiguchi S, et al. Proposal for Endoscopic Ultrasonography Classification for Small Pancreatic Cancer. Diagnostics. 2019; 9(1):15. https://doi.org/10.3390/diagnostics9010015
Chicago/Turabian StyleTerada, Shuzo, Masataka Kikuyama, Shinya Kawaguchi, Hideyuki Kanemoto, Yoshihiro Yokoi, Terumi Kamisawa, Sawako Kuruma, Kazuro Chiba, Goro Honda, Shinichiro Horiguchi, and et al. 2019. "Proposal for Endoscopic Ultrasonography Classification for Small Pancreatic Cancer" Diagnostics 9, no. 1: 15. https://doi.org/10.3390/diagnostics9010015