
Prediction of the Sleep Apnea Severity Using 2D-Convolutional Neural Networks and Respiratory Effort Signals

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
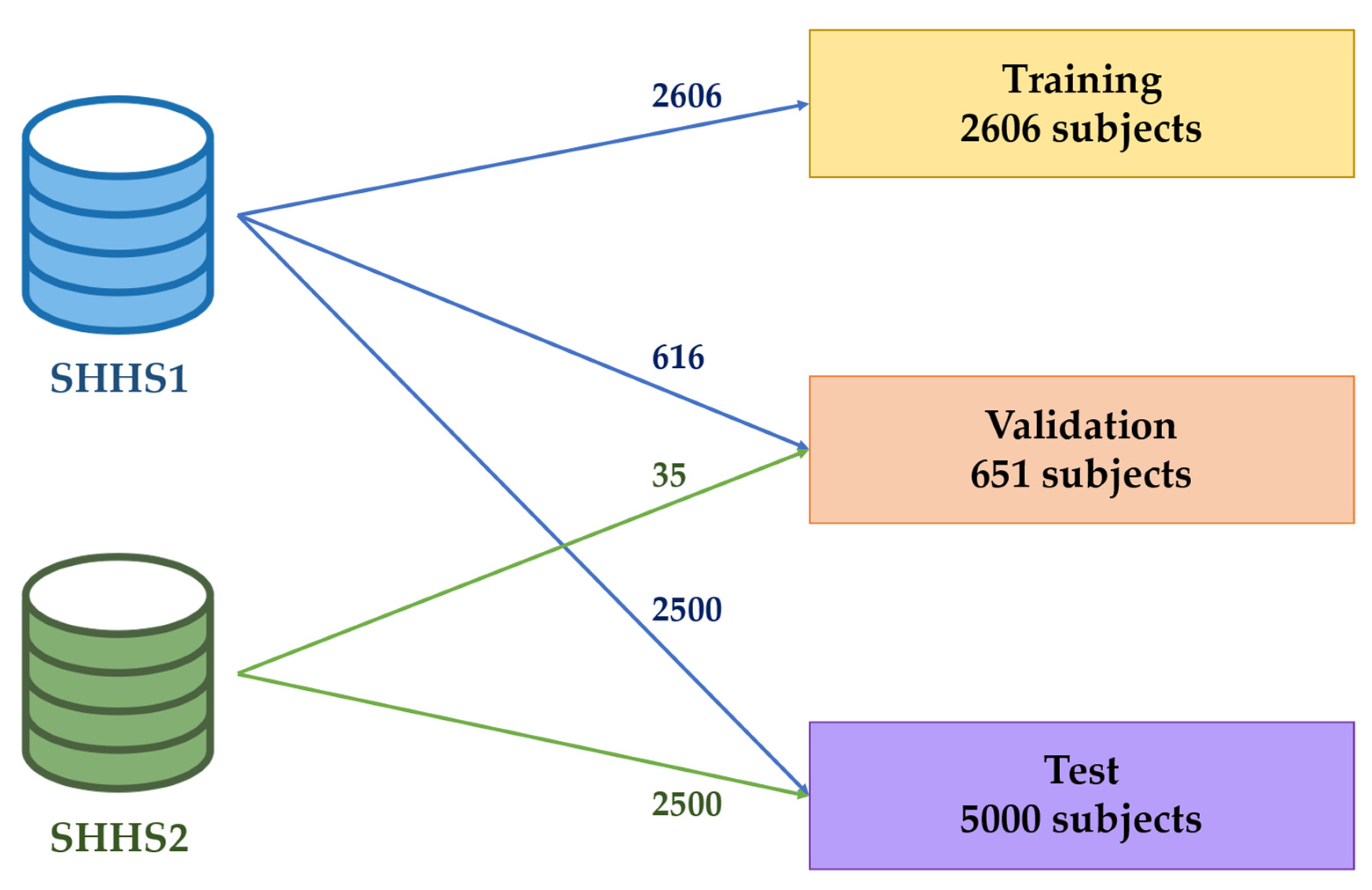
2.1. Database
2.2. Preprocessing and Data Augmentation
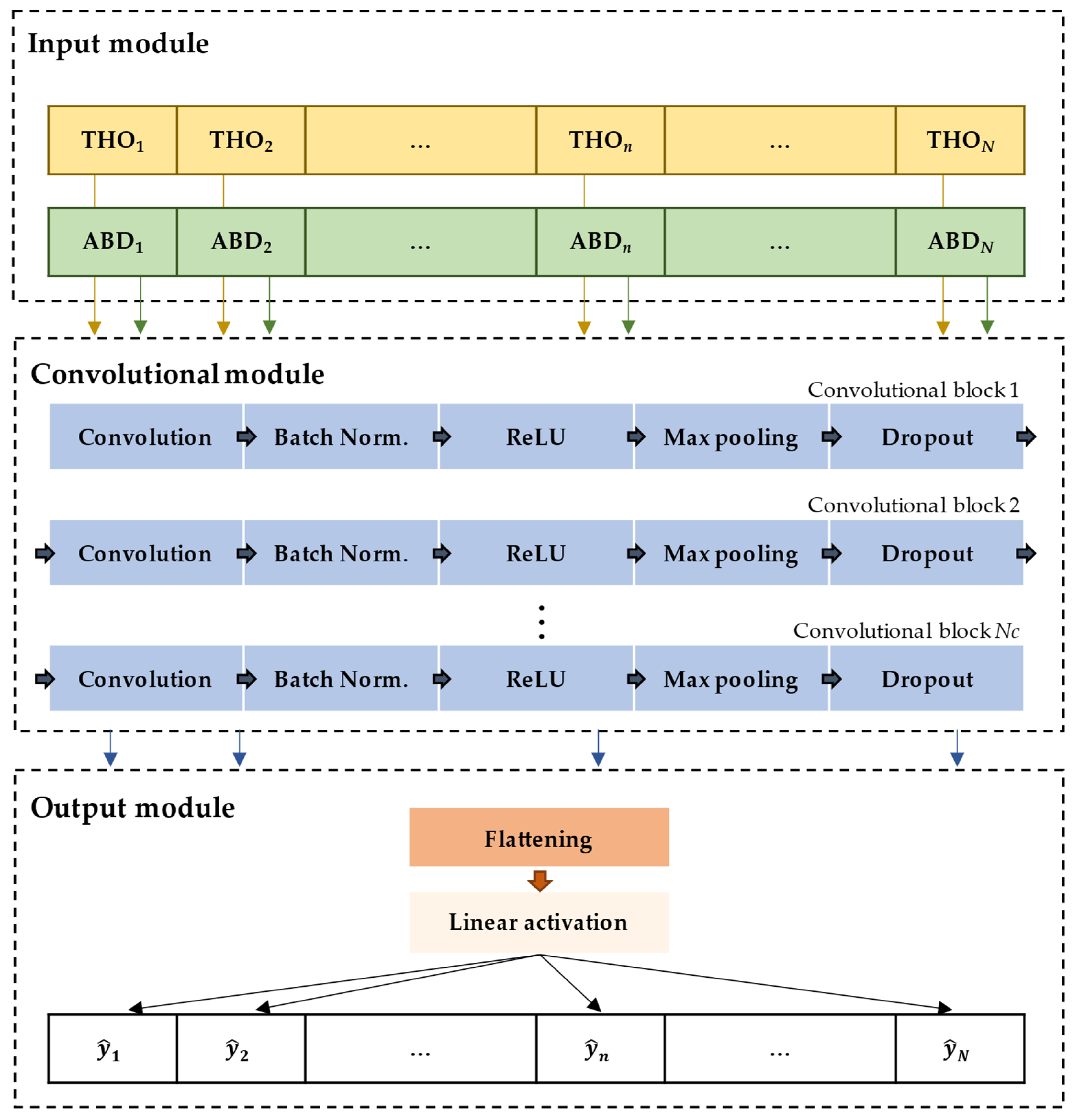
2.3. Convolutional Neural Network Architecture
- Convolution: It applies a kernel function to the input data to obtain feature maps [30,31]. This layer is defined by three parameters: kernel, padding, and stride. In our study, a padding value of 0 was assigned to prevent artificial expansion of the input data borders, thus maintaining consistent input and output lengths [30,43]. Regarding the stride, it was set to (1, 2) to ensure that the convolutional process preserves the spatial relationships within the data while efficiently extracting meaningful features, leading to a more accurate representation of the input data in the subsequent layers of the network [30,43]. In addition, the number Nk and size Sk of the kernel were values to be optimized.
- Normalization: This layer normalizes the feature maps using a batch normalization [30,44]. As the network learns, the input distribution of each layer may change, hindering training. Batch normalization mitigates this effect by normalizing the inputs for each channel, subtracting the batch mean, and dividing it by the batch standard deviation. Thus, this normalization not only stabilizes and accelerates the training process but also allows for more efficient learning across all layers of the network [43].
- Pooling: This layer reduces the feature maps size by extracting dominant and translationally invariant features [30]. Particularly, we applied a max pooling of (1, 2) with stride (1, 1) [39,42], which divides the feature map into overlapping regions of (1, 2) and selects the maximum value from each region.
- Flattening: It concatenates all feature maps elements into a single dimension array to allow the next layer to process the data [30].
- Linear activation: This fully connected layer has a single neuron that receives the activations from the previous layer and performs a linear combination of them to conduct the regression task [30]. The output of this perceptron is the estimation of the number of events contained in each 20 min segment [45].
2.4. Convolutional Neural Network Training and Optimization
2.5. Apnea-Hypopnea Index Regression
2.6. Statistical Analysis
3. Results
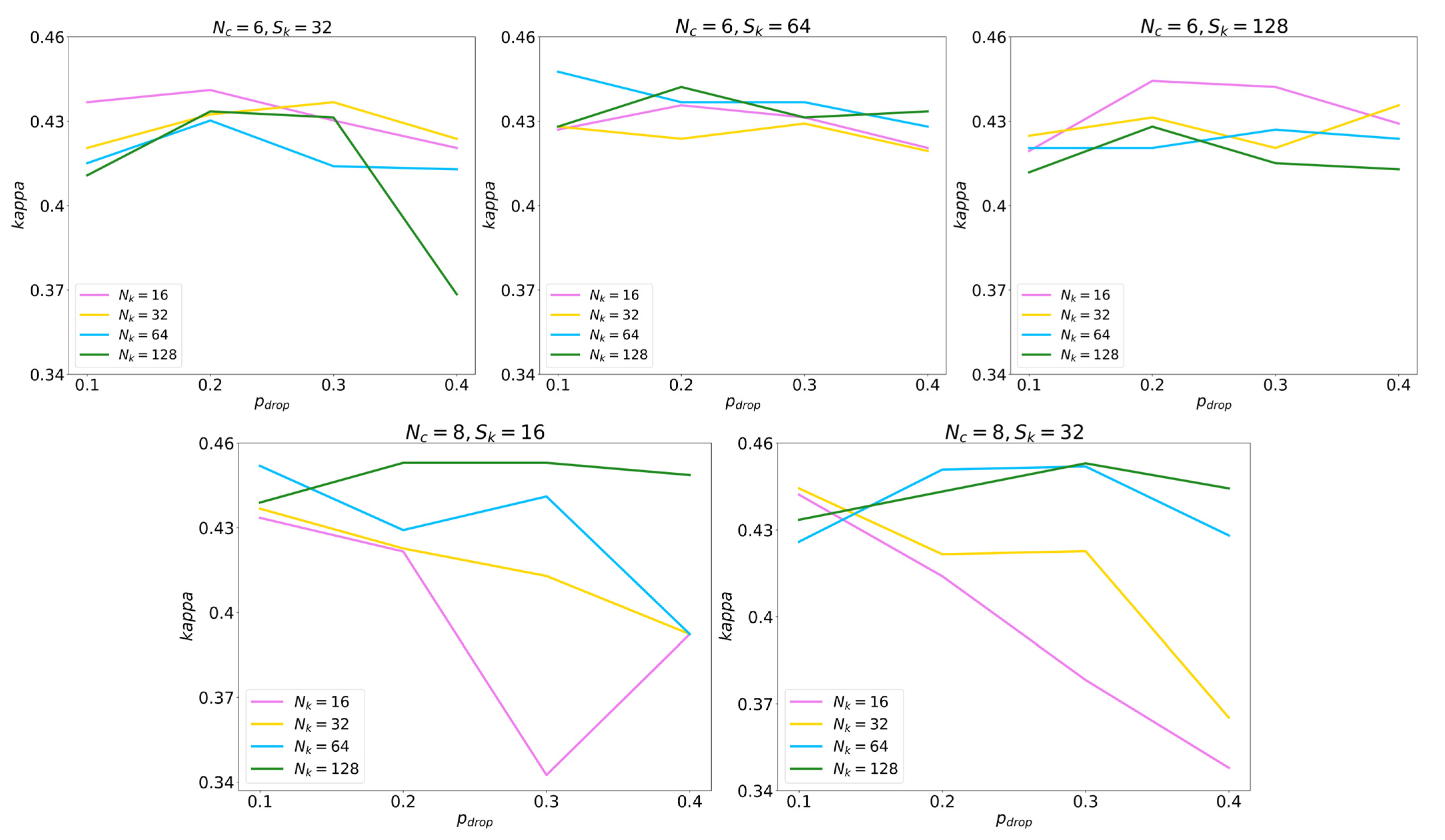
3.1. Convolutional Neural Network Optimization
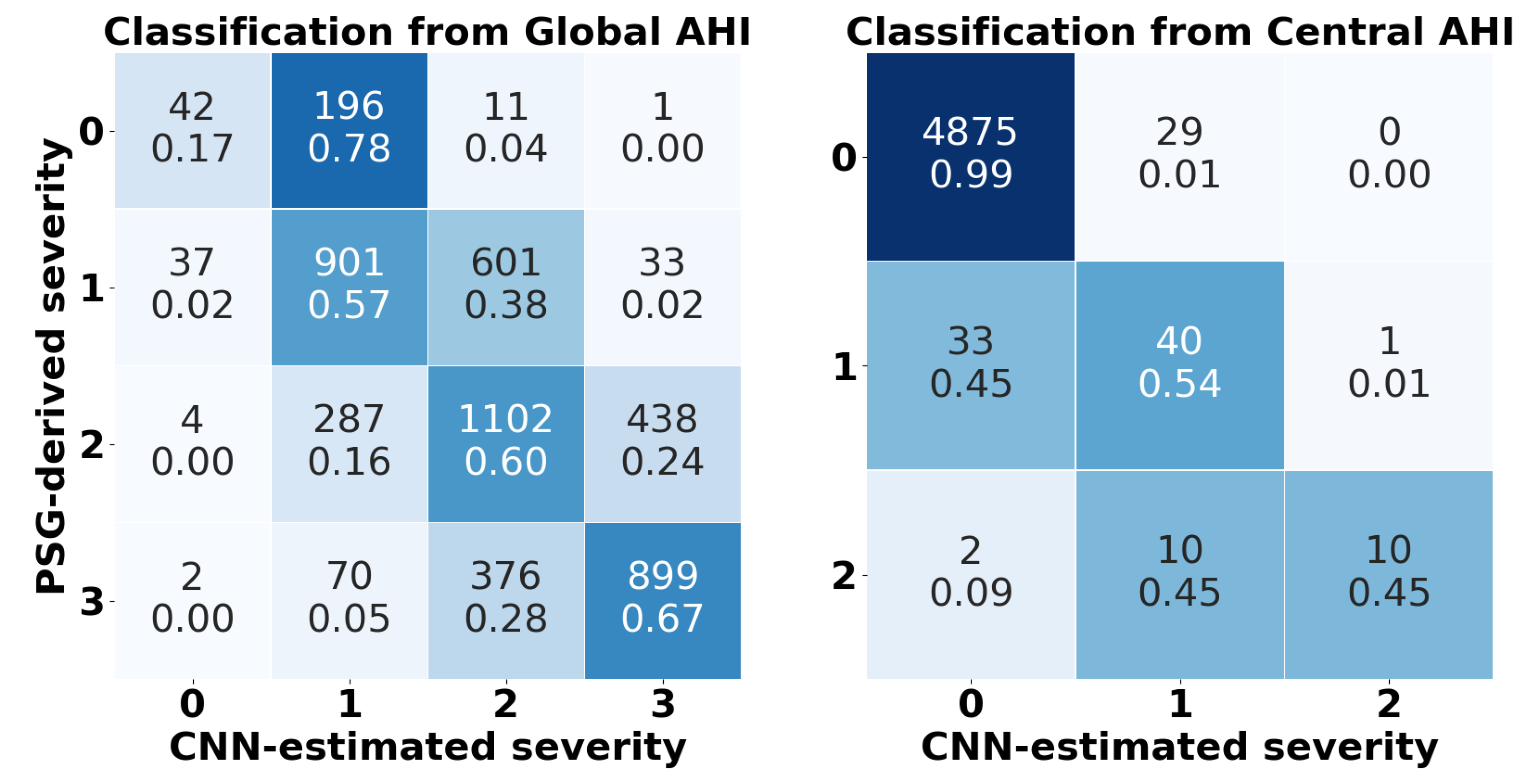
3.2. Convolutional Neural Network Diagnostic Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef]
- Young, T.; Skatrud, J.; Peppard, P.E. Risk Factors for Obstructive Sleep Apnea in Adults. JAMA 2004, 291, 2013–2016. [Google Scholar] [CrossRef]
- Sin, D.D.; Fitzgerald, F.; Parker, J.D.; Newton, G.; Floras, J.S.; Bradley, T.D. Risk Factors for Central and Obstructive Sleep Apnea in 450 Men And Women with Congestive Heart Failure. Am. J. Respir. Crit. Care Med. 1999, 160, 1101–1106. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical Guideline for the Evaluation, Management and Long-term Care of Obstructive Sleep Apnea in Adults. J. Clin. Sleep Med. 2009, 5, 263. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-De-La-Torre, M.; Cubillos, C.; Veatch, O.J.; Garcia-Rio, F.; Gozal, D.; Martinez-Garcia, M.A. Potential Pathophysiological Pathways in the Complex Relationships between OSA and Cancer. Cancers 2023, 15, 1061. [Google Scholar] [CrossRef]
- Lopez-Jimenez, F.; Kuniyoshi, F.H.S.; Gami, A.; Somers, V.K. Obstructive Sleep Apnea: Implications for Cardiac and Vascular Disease. Chest 2008, 133, 793–804. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2012, 165, 1217–1239. [Google Scholar] [CrossRef]
- Kapur, V.; Strohl, K.P.; Redline, S.; Iber, C.; O’Connor, G.; Nieto, J. Underdiagnosis of Sleep Apnea Syndrome in U.S. Communities. Sleep Breath. 2002, 6, 49–54. [Google Scholar] [CrossRef]
- Young, T.; Evans, L.; Finn, L.; Palta, M. Estimation of the Clinically Diagnosed Proportion of Sleep Apnea Syndrome in Middle-aged Men and Women. Sleep 1997, 20, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Rundo, J.V.; Downey, R. Polysomnography. Handb. Clin. Neurol. 2019, 160, 381–392. [Google Scholar] [CrossRef]
- Flemons, W.W.; Littner, M.R.; Rowley, J.A.; Gay, P.; Anderson, W.M.; Hudgel, D.W.; McEvoy, R.D.; Loube, D.I. Home Diagnosis of Sleep Apnea: A Systematic Review of the Literature: An Evidence Review Cosponsored by the American Academy of Sleep Medicine, the American College of Chest Physicians, and the American Thoracic Society. Chest 2003, 124, 1543–1579. [Google Scholar] [CrossRef]
- Bennett, J.A.; Kinnear, W.J.M. Sleep on the cheap: The role of overnight oximetry in the diagnosis of sleep apnoea hypopnoea syndrome. Thorax 1999, 54, 958–959. [Google Scholar] [CrossRef]
- de Almeida, F.R.; Ayas, N.T.; Otsuka, R.; Ueda, H.; Hamilton, P.; Ryan, F.C.; Lowe, A.A. Nasal pressure recordings to detect obstructive sleep apnea. Sleep Breath. 2006, 10, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, S.S.; Mendonça, F.; Ravelo-García, A.G.; Morgado-Dias, F. A Systematic Review of Detecting Sleep Apnea Using Deep Learning. Sensors 2019, 19, 4934. [Google Scholar] [CrossRef] [PubMed]
- Moridian, P.; Shoeibi, A.; Khodatars, M.; Jafari, M.; Pachori, R.B.; Khadem, A.; Alizadehsani, R.; Ling, S.H. Automatic diagnosis of sleep apnea from biomedical signals using artificial intelligence techniques: Methods, challenges, and future works. WIREs Data Min. Knowl. Discov. 2022, 12, e1478. [Google Scholar] [CrossRef]
- Gutiérrez-Tobal, G.C.; Álvarez, D.; Vaquerizo-Villar, F.; Barroso-García, V.; Gómez-Pilar, J.; del Campo, F.; Hornero, R. Conventional Machine Learning Methods Applied to the Automatic Diagnosis of Sleep Apnea. Adv. Exp. Med. Biol. 2022, 1384, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-Y.; Wu, H.-T.; Hsu, C.-A.; Huang, P.-C.; Huang, Y.-H.; Lo, Y.-L. Sleep Apnea Detection Based on Thoracic and Abdominal Movement Signals of Wearable Piezoelectric Bands. IEEE J. Biomed. Health Inform. 2016, 21, 1533–1545. [Google Scholar] [CrossRef] [PubMed]
- Folke, M.; Cernerud, L.; Ekström, M.; Hök, B. Critical review of non-invasive respiratory monitoring in medical care. Med. Biol. Eng. Comput. 2003, 41, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Varady, P.; Bongar, S.; Benyo, Z. Detection of airway obstructions and sleep apnea by analyzing the phase relation of respiration movement signals. IEEE Trans. Instrum. Meas. 2003, 52, 2–6. [Google Scholar] [CrossRef]
- Ng, A.S.; Chung, J.W.; DI Gohel, M.; Yu, W.W.; Fan, K.L.; Wong, T.K. Evaluation of the performance of using mean absolute amplitude analysis of thoracic and abdominal signals for immediate indication of sleep apnoea events. J. Clin. Nurs. 2008, 17, 2360–2366. [Google Scholar] [CrossRef]
- Al-Angari, H.M.; Sahakian, A.V. Automated Recognition of Obstructive Sleep Apnea Syndrome Using Support Vector Machine Classifier. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Guijarro-Berdiñas, B.; Hernández-Pereira, E.; Peteiro-Barral, D. A mixture of experts for classifying sleep apneas. Expert Syst. Appl. 2012, 39, 7084–7092. [Google Scholar] [CrossRef]
- Sezgin, N.; Tagluk, M.E. Energy based feature extraction for classification of sleep apnea syndrome. Comput. Biol. Med. 2009, 39, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Tagluk, M.E.; Akin, M.; Sezgin, N. Classıfıcation of sleep apnea by using wavelet transform and artificial neural networks. Expert Syst. Appl. 2010, 37, 1600–1607. [Google Scholar] [CrossRef]
- Fontenla-Romero, O.; Guijarro-Berdiñas, B.; Alonso-Betanzos, A.; Moret-Bonillo, V. A new method for sleep apnea classification using wavelets and feedforward neural networks. Artif. Intell. Med. 2005, 34, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Aydoğan, O.; Öter, A.; Güney, K.; Kıymık, M.K.; Tuncel, D. Automatic Diagnosis of Obstructive Sleep Apnea/Hypopnea Events Using Respiratory Signals. J. Med. Syst. 2016, 40, 274. [Google Scholar] [CrossRef] [PubMed]
- Koley, B.L.; Dey, D. Classification of sleep apnea using cross wavelet transform. In Proceedings of the 2013 IEEE 1st International Conference on Condition Assessment Techniques in Electrical Systems (CATCON), Kolkata, India, 6–8 December 2013; pp. 275–280. [Google Scholar] [CrossRef]
- Avcı, C.; Akbaş, A. Sleep apnea classification based on respiration signals by using ensemble methods. Bio-Med. Mater. Eng. 2015, 26, S1703–S1710. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Van Steenkiste, T.; Groenendaal, W.; Deschrijver, D.; Dhaene, T. Automated Sleep Apnea Detection in Raw Respiratory Signals Using Long Short-Term Memory Neural Networks. IEEE J. Biomed. Health Inform. 2019, 23, 2354–2364. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Koprinska, I.; Jeffries, B. Sleep Apnea Prediction Using Deep Learning. IEEE J. Biomed. Health Inform. 2023, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Haidar, R.; McCloskey, S.; Koprinska, I.; Jeffries, B. Convolutional Neural Networks on Multiple Respiratory Channels to Detect Hypopnea and Obstructive Apnea Events. In Proceedings of the 2018 International Joint Conference on Neural Networks (IJCNN), Rio de Janeiro, Brazil, 8–13 July 2018; pp. 1–7. [Google Scholar] [CrossRef]
- Quan, S.F.; Howard, B.V.; Iber, C.; Kiley, J.P.; Nieto, F.J.; O’Connor, G.T.; Rapoport, D.M.; Redline, S.; Robbins, J.; Samet, J.M.; et al. The Sleep Heart Health Study: Design, rationale, and methods. Sleep 1997, 20, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.-Q.; Cui, L.; Mueller, R.; Tao, S.; Kim, M.; Rueschman, M.; Mariani, S.; Mobley, D.; Redline, S. The National Sleep Research Resource: Towards a sleep data commons. J. Am. Med. Inform. Assoc. 2018, 25, 1351. [Google Scholar] [CrossRef] [PubMed]
- Karhu, T.; Myllymaa, S.; Nikkonen, S.; Mazzotti, D.R.; Töyräs, J.; Leppänen, T. Longer and Deeper Desaturations Are Associated With the Worsening of Mild Sleep Apnea: The Sleep Heart Health Study. Front. Neurosci. 2021, 15, 657126. [Google Scholar] [CrossRef] [PubMed]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning; Springer: Berlin/Heidelberg, Germany, 2013; Volume 112. [Google Scholar]
- Vaquerizo-Villar, F.; Alvarez, D.; Kheirandish-Gozal, L.; Gutierrez-Tobal, G.C.; Barroso-Garcia, V.; Santamaria-Vazquez, E.; del Campo, F.; Gozal, D.; Hornero, R. A Convolutional Neural Network Architecture to Enhance Oximetry Ability to Diagnose Pediatric Obstructive Sleep Apnea. IEEE J. Biomed. Health Inform. 2021, 25, 2906–2916. [Google Scholar] [CrossRef] [PubMed]
- Brouillette, R.T.; Morielli, A.; Leimanis, A.; Waters, K.A.; Luciano, R.; Ducharme, F.M. Nocturnal Pulse Oximetry as an Abbreviated Testing Modality for Pediatric Obstructive Sleep Apnea. Pediatrics 2000, 105, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Leino, A.; Korkalainen, H.; Kalevo, L.; Nikkonen, S.; Kainulainen, S.; Ryan, A.; Duce, B.; Sipila, K.; Ahlberg, J.; Sahlman, J.; et al. Deep Learning Enables Accurate Automatic Sleep Staging Based on Ambulatory Forehead EEG. IEEE Access 2022, 10, 26554–26566. [Google Scholar] [CrossRef]
- Jiménez-García, J.; García, M.; Gutiérrez-Tobal, G.C.; Kheirandish-Gozal, L.; Vaquerizo-Villar, F.; Álvarez, D.; del Campo, F.; Gozal, D.; Hornero, R. A 2D convolutional neural network to detect sleep apnea in children using airflow and oximetry. Comput. Biol. Med. 2022, 147, 105784. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. Deep Learning with Python; Simon and Schuster: Shelter Island, NY, USA, 2021. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch Normalization Accelerating Deep Network Training by Reducing Internal Covariate Shift. In Proceedings of the International Conference on Machine Learning, Lille, France, 6–11 July 2015; pp. 448–456. [Google Scholar]
- Leino, A.; Nikkonen, S.; Kainulainen, S.; Korkalainen, H.; Töyräs, J.; Myllymaa, S.; Leppänen, T.; Ylä-Herttuala, S.; Westeren-Punnonen, S.; Muraja-Murro, A.; et al. Neural network analysis of nocturnal SpO2 signal enables easy screening of sleep apnea in patients with acute cerebrovascular disease. Sleep Med. 2021, 79, 71–78. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Delving Deep into Rectifiers: Surpassing Human-Level Performance on ImageNet Classification. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Santiago, Chile, 7–13 December 2015. [Google Scholar]
- Kingma, D.P.; Ba, J.L. Adam: A Method for Stochastic Optimization. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Huber, P.J. Robust Estimation of a Location Parameter. Ann. Math. Stat. 1964, 35, 73–101. [Google Scholar] [CrossRef]
- Deviaene, M.; Testelmans, D.; Buyse, B.; Borzee, P.; Van Huffel, S.; Varon, C. Automatic Screening of Sleep Apnea Patients Based on the SpO2 Signal. IEEE J. Biomed. Health Inform. 2018, 23, 607–617. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Javaheri, S.; Barbe, F.; Campos-Rodriguez, F.; Dempsey, J.A.; Khayat, R.; Javaheri, S.; Malhotra, A.; Martinez-Garcia, M.A.; Mehra, R.; Pack, A.I.; et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol. 2017, 69, 841–858. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Altman, D.G. Diagnostic tests 4: Likelihood ratios. BMJ 2004, 329, 168–169. [Google Scholar] [CrossRef] [PubMed]
- Staats, B.A.; Bonekat, H.W.; Harris, C.D.; Offord, K.P. Chest wall motion in sleep apnea. Am. Rev. Respir. Dis. 1984, 130, 59–63. [Google Scholar]
- Rolón, R.; Larrateguy, L.; Di Persia, L.; Spies, R.; Rufiner, H. Discriminative methods based on sparse representations of pulse oximetry signals for sleep apnea–hypopnea detection. Biomed. Signal Process. Control 2017, 33, 358–367. [Google Scholar] [CrossRef]
- Rolon, R.; Gareis, I.; Larrateguy, L.; Di Persia, L.; Spies, R.; Rufiner, H. Automatic scoring of apnea and hypopnea events using blood oxygen saturation signals. Biomed. Signal Process. Control 2020, 62, 102062. [Google Scholar] [CrossRef]
- Gutiérrez-Tobal, G.C.; Álvarez, D.; Vaquerizo-Villar, F.; Crespo, A.; Kheirandish-Gozal, L.; Gozal, D.; del Campo, F.; Hornero, R. Ensemble-learning regression to estimate sleep apnea severity using at-home oximetry in adults. Appl. Soft Comput. 2021, 111, 107827. [Google Scholar] [CrossRef]
- Olsen, M.; Mignot, E.; Jennum, P.J.; Sorensen, H.B.D. Robust, ECG-based detection of Sleep-disordered breathing in large population-based cohorts. Sleep 2020, 43, zsz276. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.B.; Chow, C.-M.; Ling, S.; Su, S.W. A novel algorithm for automatic diagnosis of sleep apnea from airflow and oximetry signals. Physiol. Meas. 2021, 42, 015001. [Google Scholar] [CrossRef] [PubMed]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | All | Training | Validation | Test |
|---|---|---|---|---|
| #Subjects | 8257 | 2606 (31.56%) | 651 (7.88%) | 5000 (60.56%) |
| Age (years) | 65 [16] | 64 [21] | 62 [12] | 65 [16] |
| #Male | 3887 (47.08%) | 1275 (48.93%) | 322 (49.46%) | 2290 (45.80%) |
| BMI (kg/m2) | 27.54 [6.10] | 27.15 [6.18] | 28.02 [6.32] | 27.68 [6.02] |
| CAI (e/h) | 0 [0.26] | 0 [0.33] | 0.12 [0.26] | 0 [0.26] |
| AHI (e/h) | 21.68 [21.52] | 25.62 [23.08] | 26.08 [26.48] | 19.38 [19.51] |
| #No apnea | 338 (4.09%) | 77 (2.95%) | 11 (1.69%) | 250 (5.00%) |
| #Mild | 2244 (27.18%) | 529 (20.30%) | 143 (21.97%) | 1572 (31.44%) |
| #Moderate | 3003 (36.37%) | 958 (36.76%) | 214 (32.87%) | 1831 (36.62%) |
| #Severe | 2672 (32.36%) | 1042 (39.99%) | 283 (43.47%) | 1347 (26.94%) |
| Hyperparameter | Search Space | Optimal Value |
|---|---|---|
| 6, 8 | 8 | |
| 32, 64, 128 (), 16, 32 () | 16 | |
| 16, 32, 64, 128 | 128 | |
| 0.1, 0.2, 0.3, 0.4 | 0.3 |
| AHI events/h | Se (%) | Sp (%) | Acc (%) | PPV (%) | NPV (%) | LR+ | LR- | kappa | Acc4 (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| CNN-AHIGlobal | 5 | 99.09 | 16.80 | 94.98 | 95.77 | 49.41 | 1.19 | 0.05 | 0.3960 | 58.88 |
| 15 | 88.58 | 64.54 | 79.82 | 81.33 | 76.41 | 2.50 | 0.18 | |||
| 30 | 66.74 | 87.08 | 81.60 | 65.57 | 87.66 | 5.17 | 0.38 | |||
| CNN-AHICentral | 1 | 59.87 | 97.70 | 94.10 | 73.26 | 95.86 | 26.05 | 0.41 | 0.5903 ** | 98.50 ** |
| 5 | 63.54 | 99.41 | 98.72 | 67.78 | 99.29 | 107.45 | 0.37 | |||
| 10 | 68.57 | 99.86 | 99.64 | 77.42 | 99.78 | 486.37 | 0.31 | |||
| 15 | 45.45 | 99.98 | 99.74 | 90.91 | 99.76 | 2262.72 | 0.55 | |||
| 30 * | - | - | - | - | - | - | - |
| Study | #Subjects | Signal | Approach | AHI | Se (%) | Sp (%) | Acc (%) | Kappa |
|---|---|---|---|---|---|---|---|---|
| Ng et al. (2008) [21] | 26 | THO, ABD | Event detection by temporal features | - | 88.29 | 90.19 | 89.20 ** | - |
| Lin et al. (2017) [18] | 34 | THO, ABD | Event detection by temporal and frequency features | - | - | - | 84.42 | - |
| Varady et al. (2003) [20] | 6 | THO, ABD | Event detection by phase features | - | - | - | 90.63 | - |
| Al-Angari et al. (2012) [22] | 100 (SHHS) | THO, ABD | Event detection by phase features | - | 85.7 | 92.20 | 89.00 | - |
| Guijarro-Berdiñas et al. (2012) [23] | 6 | AF, THO, ABD | Obstructive event detection by wavelet features | - | 89.63 | 97.11 | 94.62 | - |
| Central event detection by wavelet features | - | 88.98 | 98.71 | 95.47 | - | |||
| Mixed event detection by wavelet features | - | 92.20 | 89.58 | 90.45 | - | |||
| Sezgin et al. (2009) [24] | 21 | THO, ABD | Obstructive, central, and mixed event distinction by wavelet features | - | - | - | 86.84 | - |
| Emin et al. (2010) [25] | 21 | ABD | Obstructive, central, and mixed event distinction by wavelet features | - | - | - | 75.85 | - |
| Fontenla-Romero et al. (2005) [26] | 6 | AF, THO | Obstructive, central, and mixed event distinction by wavelet features | - | - | - | 83.78 | - |
| Koley et al. (2013) [28] | 20 | AF, THO | Obstructive, central, and mixed event distinction by wavelet features | - | - | - | 85.00 | - |
| Avci et al. (2015) [29] | 8 | ABD | Event detection by wavelet features | - | - | - | 92.75 | 0.9250 |
| THO | Event detection by wavelet features | - | - | - | 95.87 | 0.9360 | ||
| Haidar et al. (2018) [34] | 2056 | AF, THO, ABD | Event detection using CNN | - | - | - | 83.50 | - |
| Wang et al. (2023) [33] | 1507 | AF, THO, ABD | Event detection using CNN | - | 77.14 | 86.19 | 81.67 | - |
| Event detection using LSTM | - | 77.68 | 84.43 | 81.56 | - | |||
| Event detection using 1D-CNN-LSTM | - | 81.73 | 85.30 | 83.53 | - | |||
| Event detection using 2D-CNN-LSTM | - | 81.21 | 86.59 | 83.90 | - | |||
| Van Steenkiste et al. (2019) [32] | 2100 (SHHS) | ABD | AHI estimation using a LSTM method to detect apneic events | 5 | 99.34 | 5.88 | 97.75 | 0.3293 |
| 15 | 91.04 | 37.61 | 78.76 | |||||
| 30 | 67.19 | 81.51 | 76.01 | |||||
| Our proposal | 8257 | THO, ABD | Global AHI estimation using a CNN method | 5 | 99.09 | 16.80 | 94.98 | 0.3960 |
| 15 | 88.58 | 64.54 | 79.82 | |||||
| 30 | 66.74 | 87.08 | 81.60 | |||||
| Central AHI estimation using a CNN method | 5 | 63.54 | 99.41 | 98.72 | 0.5903 | |||
| 15 | 45.45 | 99.98 | 99.74 | |||||
| 30 * | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barroso-García, V.; Fernández-Poyatos, M.; Sahelices, B.; Álvarez, D.; Gozal, D.; Hornero, R.; Gutiérrez-Tobal, G.C. Prediction of the Sleep Apnea Severity Using 2D-Convolutional Neural Networks and Respiratory Effort Signals. Diagnostics 2023, 13, 3187. https://doi.org/10.3390/diagnostics13203187
Barroso-García V, Fernández-Poyatos M, Sahelices B, Álvarez D, Gozal D, Hornero R, Gutiérrez-Tobal GC. Prediction of the Sleep Apnea Severity Using 2D-Convolutional Neural Networks and Respiratory Effort Signals. Diagnostics. 2023; 13(20):3187. https://doi.org/10.3390/diagnostics13203187
Chicago/Turabian StyleBarroso-García, Verónica, Marta Fernández-Poyatos, Benjamín Sahelices, Daniel Álvarez, David Gozal, Roberto Hornero, and Gonzalo C. Gutiérrez-Tobal. 2023. "Prediction of the Sleep Apnea Severity Using 2D-Convolutional Neural Networks and Respiratory Effort Signals" Diagnostics 13, no. 20: 3187. https://doi.org/10.3390/diagnostics13203187