
Validation of Three MicroScan® Antimicrobial Susceptibility Testing Plates Designed for Low-Resource Settings

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Antibiotic Susceptibility Testing in Low-Resource Settings
1.2. Development of Adapted AST Solution for LRS within the Context of Mini-Lab
2. Materials and Methods
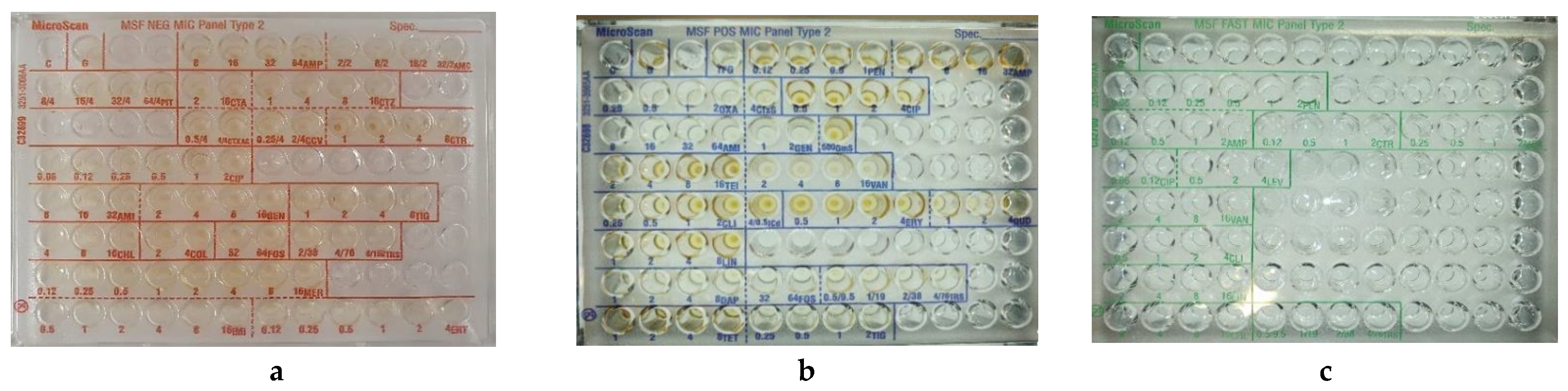
2.1. MicroScan MSF MIC Panels
2.2. Clinical Isolates and Reference Strains
2.3. Reference Antimicrobial Susceptibility Testing Methods
2.4. Inoculum Preparation
2.5. Comparison between Standard Inoculum Method and Prompt Inoculation Method
2.6. Panel Inoculation and Incubation
2.7. Manual Panel Reading and Inter Observer Variability
2.8. Ease of Use
2.9. Data Analysis
2.10. Quality Control
2.11. Resolution of Discrepancies
3. Results
3.1. Evaluation of the MSF MicroScan MIC Panels
3.1.1. MSF Gram-Pos Panel Results
3.1.2. MSF Gram-Neg Panel Results
3.1.3. MSF FAST Panel Results
3.2. Results of the Evaluation of the Prompt Performance
3.3. Inter-Observer Variability
3.4. Ease of Use
4. Discussion
4.1. Performance Evaluation of the MSF MIC Panels
4.2. Performance Evaluation of the Prompt Inoculation Method
4.3. Inter-Observer Variability
4.4. Adaptation to LRS: Stability, Ease-of-Use
4.5. Recommendations for Use and Further Development of the MicroScan System
4.6. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nadimpalli, M.; Delarocque-Astagneau, E.; Love, D.C.; Price, L.B.; Huynh, B.-T.; Collard, J.-M.; Lay, K.S.; Borand, L.; Ndir, A.; Walsh, T.; et al. Combating Global Antibiotic Resistance: Emerging One Health Concerns in Lower-and Middle-Income Countries. Clin. Infect. Dis. 2018, 66, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Catena, F.; Coccolini, F.; Hardcastle, T.C.; Roques, C.; Salameh, P. Drivers of antibiotic resistance transmission in low-and middle-income countries from a ‘one health’ perspective—A review. Antibiotics 2020, 9, 372. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; The Review on Antimicrobial Resistance: London, UK, May 2016. [Google Scholar]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef]
- Bebell, L.M.; Muiru, A.N. Antibiotic use and emerging resistance: How can resource-limited countries turn the tide? Glob. Heart 2014, 9, 347–358. [Google Scholar] [CrossRef]
- Clift, C. Review of Progress on Antimicrobial Resistance. In The Royal Institute of International Affairs; Forest Stewardship Council: Bonn, Germany, 2019. [Google Scholar]
- Gelband, H.; Molly Miller, P.; Pant, S.; Gandra, S.; Levinson, J.; Barter, D.; White, A.; Laxminarayan, R. State of the World’s Antibiotics 2015. Wound Health S. Afr. 2015, 8, 30–34. [Google Scholar]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2016–2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Presentation WHO Report on Antibacterial Resistance; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Ashley, E.A.; Recht, J.; Chua, A.; Dance, D.; Dhorda, M.; Thomas, N.; Ranganathan, N.; Turner, P.; Guerin, P.J.; White, N.J. Antimicrobial Resistance in Low and Middle Income Countries. In An Analysis of Surveillance Networks; IDDO: Oxford, UK, 2016. [Google Scholar]
- Welcome Trust. The Global Response to AMR: Momentum, Success, and Critical Gaps; Wellcome Trust: London, UK, 2020. [Google Scholar]
- Gandra, S.; Alvarez-Uria, G.; Turner, P.; Joshi, J.; Limmathurotsakul, D.; van Doorn, H.R. Antimicrobial resistance surveillance in low-and middle-income countries: Progress and challenges in eight South Asian and Southeast Asian countries. Clin. Microbiol. Rev. 2020, 33, e00048-19. [Google Scholar] [CrossRef]
- Lewis, J.M.; Feasey, N.A.; Rylance, J. Aetiology and outcomes of sepsis in adults in sub-Saharan Africa: A systematic review and meta-analysis. Crit. Care 2019, 23, 212. [Google Scholar] [CrossRef]
- Girosi, F.; Olmsted, S.S.; Keeler, E.; Burgess, D.C.H.; Lim, Y.-W.; Aledort, J.E.; Rafael, M.E.; Ricci, K.A.; Boer, R.; Hilborne, L.; et al. Developing and interpreting models to improve diagnostics in developing countries. Nature 2006, 444, 3–8. [Google Scholar] [CrossRef]
- Jacobs, J.; Hardy, L.; Semret, M.; Lunguya, O.; Phe, T.; Affolabi, D.; Yansouni, C.; Vandenberg, O. Diagnostic Bacteriology in District Hospitals in Sub-Saharan Africa: At the Forefront of the Containment of Antimicrobial Resistance. Front. Med. 2019, 6, 205. [Google Scholar] [CrossRef]
- Ombelet, S.; Barbé, B.; Affolabi, D.; Ronat, J.-B.; Lompo, P.; Lunguya, O.; Jacobs, J.; Hardy, L. Best Practices of Blood Cultures in Low- and Middle-Income Countries. Front. Med. 2019, 6, 131. [Google Scholar] [CrossRef] [PubMed]
- Saeed, D.K.; Hasan, R.; Naim, M.; Zafar, A.; Khan, E.; Jabeen, K.; Irfan, S.; Ahmed, I.; Zeeshan, M.; Wajidali, Z.; et al. Readiness for antimicrobial resistance (AMR) surveillance in Pakistan; a model for laboratory strengthening. Antimicrob. Resist. Infect. Control 2017, 6, 101. [Google Scholar] [CrossRef] [PubMed]
- Hazim, C.; Ibrahim, R.A.; Westercamp, M.; Belete, G.A.; Kibret, B.A.; Kanter, T.; Yimer, G.; Adem, T.S.; Stevenson, K.B.; Urrego, M.; et al. Establishment of a Sentinel Laboratory-Based Antimicrobial Resistance Surveillance Network in Ethiopia. Health Secur. 2018, 16 (Suppl. S1), S30–S36. [Google Scholar] [CrossRef]
- Ombelet, S.; Ronat, J.-B.; Walsh, T.; Yansouni, C.P.; Cox, J.; Vlieghe, E.; Martiny, D.; Semret, M.; Vandenberg, O.; Jacobs, J.; et al. Clinical bacteriology in low-resource settings: Today’s solutions. Lancet Infect. Dis. 2018, 18, e248–e258. [Google Scholar] [CrossRef]
- Baron, E.J. Clinical Microbiology in Underresourced Settings. Clin. Lab. Med. 2019, 39, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Okeke, I.N.; Feasey, N.; Parkhill, J.; Turner, P.; Limmathurotsakul, D.; Georgiou, P.; Holmes, A.; Peacock, S.J. Leapfrogging laboratories: The promise tech solutions for and pitfalls of high-tech solutions for antimicrobial resistance surveillance in low-income settings. BMJ Glob. Health 2020, 5, e003622. [Google Scholar] [CrossRef] [PubMed]
- Ronat, J.-B.; Natale, A.; Kesteman, T.; Andremont, A.; Elamin, W.; Hardy, L.; Kanapathipillai, R.; Michel, J.; Langendorf, C.; Vandenberg, O.; et al. AMR in low-resource settings: Médecins Sans Frontières bridges surveillance gaps by developing a turnkey solution, the Mini-Lab. Clin. Microbiol. Infect. 2021, 27, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Natale, A.; Ronat, J.-B.; Mazoyer, A.; Rochard, A.; Boillot, B.; Hubert, J.; Baillet, B.; Ducasse, M.; Mantelet, F.; Oueslati, S.; et al. The Mini-Lab: Accessible clinical bacteriology for low-resource settings. Lancet Microbe 2020, 1, e56–e58. [Google Scholar] [CrossRef]
- Ombelet, S.; Natale, A.; Ronat, J.-B.; Kesteman, T.; Vandenberg, O.; Jacobs, J.; Hardy, L. Biphasic versus monophasic manual blood culture bottles for low-resource settings: An in-vitro study. The Lancet Microbe 2022, 3, e124–e132. [Google Scholar] [CrossRef]
- Ombelet, S.; Natale, A.; Ronat, J.-B.; Vandenberg, O.; Hardy, L.; Jacobs, J. Evaluation of MicroScan Bacterial Identification Panels for Low-Resource Settings. Diagnostics 2021, 11, 349. [Google Scholar] [CrossRef]
- World Health Organization. GLASS Manual for Early Implementation; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Jorgensen, J.H.; Ferraro, M.J. Antimicrobial susceptibility testing: A review of general principles and contemporary practices. Clin. Infect. Dis. 2009, 49, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- The European Committee and Antimicrobial Susceptibility Testing. Testing Breakpoint Tables for Interpretation of MICs and Zone Diameters; EUCAST: Växjö, Sweden, 2020; Volume 10. [Google Scholar]
- World Health Organization. World health organization model list of essential medicines. In Mental and Holistic Health: Some International Perspectives; WHO: Geneva, Switzerland, 2019; Volume 21, pp. 119–134. [Google Scholar]
- Sharland, M.; Pulcini, C.; Harbarth, S.; Zeng, M.; Gandra, S.; Mathur, S.; Magrini, N. Classifying antibiotics in the WHO Essential Medicines List for optimal use—Be AWaRe. Lancet Infect. Dis. 2018, 18, 18–20. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). M100 Performance Standards for Antimicrobial Susceptibility Testing M100-Ed29; CLSI: Wayne, PA, USA, 2019. [Google Scholar]
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters; EUCAST: Växjö, Sweden, 2019; Volume 9. [Google Scholar]
- EUCAST. EUCAST System for Antimicrobial Abbreviations; EUCAST: Växjö, Sweden, 2018. [Google Scholar]
- ISO. Clinical Laboratory Testing and In Vitro Diagnostic Test Systems—Susceptibility Testing of Infectious Agents and Evaluation of Performance of Antimicrobial Susceptibility Test Devices—Part 2: Evaluation of Performance of Antimicrobial Susceptibility Test Devices Against Reference Broth Micro-Dilution; ISO: Geneva, Switzerland, 2007. [Google Scholar]
- CLSI. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard—Ninth Edition 32; CLSI: Wayne, PA, USA, 2012. [Google Scholar]
- Matuschek, E.; Brown, D.F.J.; Kahlmeter, G. Development of the EUCAST disk diffusion antimicrobial susceptibility testing method and its implementation in routine microbiology laboratories. Clin. Microbiol. Infect. 2014, 20, O255–O266. [Google Scholar] [CrossRef] [PubMed]
- Flejzor, B.; Bokkenheuser, V.D. Performance of the prompt system in identification and antimicrobial susceptibility testing of clinical isolates. J. Clin. Microbiol. 1985, 21, 267–268. [Google Scholar] [CrossRef] [PubMed]
- EUCAST. EUCAST reading guide for broth microdilution (version 2.0). In European Committee on Antimicrobial Susceptibility Testing; EUCAST: Växjö, Sweden, 2020; pp. 1–20. [Google Scholar]
- Stelling, J.M. News and Notes WHONET: An Information System for Monitoring Recommendations for Preventing the Spread of Antimicrobial resistance. Emerg. Infect. Dis. 1995, 1, 66–67. [Google Scholar]
- Hindler, J.; Stelling, J. Analysis and presentation of cumulative antibiograms: A new consensus guideline from the Clinical and Laboratory Standards Institute. Clin. Infect. Dis. 2007, 44, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Bankert, D.A.; Crist, A.E.; George, W.; Eastman, J.T.; Han, A.; Horning, A. Multicenter Evaluation of Four Automated ID/AST Systems for Antimicrobial Susceptibility Testing of Commonly Isolated Enterococcus spp. and Staphylococcus spp.; American Society of Microbiology: Washington, DC, USA, 2007; pp. 1–4. [Google Scholar]
- Anderson, K.F.; Lonsway, D.R.; Rasheed, J.K.; Biddle, J.; Jensen, B.; McDougal, L.K.; Carey, R.B.; Thompson, A.; Stocker, S.; Limbago, B.; et al. Evaluation of methods to identify the Klebsiella pneumoniae carbapenemase in Enterobacteriaceae. J. Clin. Microbiol. 2007, 45, 2723–2725. [Google Scholar] [CrossRef]
- Bankert, D.A. C-122 Multicenter Evaluation of Four Automated ID/AST Systems for Antimicrobial Susceptibility Testing of Enterobacteriaceae and Commonly Isolated Glucose Non-Fermenting Gram-Negative Bacilli. In ASM2; American Society of Microbiology: Washington, DC, USA, 2006; p. 122. [Google Scholar]
- Roe, D. A Multicenter Evaluation of a MicroScan Dried Overnight Panel for Screening E. coli and Klebsiella spp. for the Presence of ESBLs; American Society of Microbiology: Washington, DC, USA, 1999; pp. 1–5. [Google Scholar]
- Rennie, R. et al. Multicenter Evaluation of Daptomycin and Ertapenem in a MicroScan Dried Overnight Panel with Gram-Positive Bacteria; American Society of Microbiology: Washington, DC, USA, 2005; pp. 1–6. [Google Scholar]
- Creely, D.; Zambardi, G.; Van Belkum, A.; Dunne, W.M.; Peyret, M.; Gayral, J.P.; Shortridge, D.; Shubert, C. International dissemination of Escherichia coli strains with discrepant behaviour in phenotypic antimicrobial susceptibility tests. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 997–1002. [Google Scholar] [CrossRef]
- Shubert, C.; Slaughter, J.; Creely, D.; van Belkum, A.; Gayral, J.P.; Dunne, W.M.; Zambardi, G.; Shortridge, D. Population analysis of Escherichia coli isolates with discordant resistance levels by piperacillin-tazobactam broth microdilution and agar dilution testing. Antimicrob. Agents Chemother. 2014, 58, 1779–1781. [Google Scholar] [CrossRef]
- Lo-Ten-Foe, J.R.; de Smet, A.M.G.A.; Diederen, B.M.W.; Kluytmans, J.A.J.W.; van Keulen, P.H.J. Comparative evaluation of the VITEK 2, disk diffusion, etest, broth microdilution, and agar dilution susceptibility testing methods for colistin in clinical isolates, including heteroresistant Enterobacter cloacae and Acinetobacter baumannii strains. Antimicrob. Agents Chemother. 2007, 51, 3726–3730. [Google Scholar] [CrossRef] [PubMed]
- Nicoloff, H.; Hjort, K.; Levin, B.R.; Andersson, D.I. The high prevalence of antibiotic heteroresistance in pathogenic bacteria is mainly caused by gene amplification. Nat. Microbiol. 2019, 4, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Andersson, D.I.; Nicoloff, H.; Hjort, K. Mechanisms and clinical relevance of bacterial heteroresistance. Nat. Rev. Microbiol. 2019, 17, 479–496. [Google Scholar] [CrossRef] [PubMed]
- Lund, M.E.; Hawkinson, R.W. Evaluation of the prompt inoculation system for preparation of standardized bacterial inocula. J. Clin. Microbiol. 1983, 18, 84–91. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Target Product Profiles for Priority Diagnostics to Support Response to the COVID-19 Pandemic; WHO: Geneva, Switzerland, 2020; Volume 0. [Google Scholar]
- World Health Organization. Technical Guidance Series (TGS) for WHO Prequalification—Diagnostic Assessment Guidance on Test Guidance on Test Method Validation for In Vitro Diagnostic Medical Devices TGS–4; Tech. Guid. Ser. WHO Prequalification—Diagnostic Assess 2017. Available online: http://apps.who.int/iris/bitstream/10665/258971/1/WHO-EMP-RHT-PQT-TGS4-2017.04-eng.pdf?ua=1 (accessed on 5 May 2022).
- Gillet, P.; Maltha, J.; Hermans, V.; Ravinetto, R.; Bruggeman, C.; Jacobs, J. Malaria rapid diagnostic kits: Quality of packaging, design and labelling of boxes and components and readability and accuracy of information inserts. Malar. J. 2011, 10, 39. [Google Scholar] [CrossRef]
- A Reddy, E.; Shaw, A.V.; A Crump, J. Community-acquired bloodstream infections in Africa: A systematic review and meta-analysis. Lancet Infect. Dis. 2010, 10, 417–432. [Google Scholar] [CrossRef]
- Kern, W.V.; Rieg, S. Burden of bacterial bloodstream infection—A brief update on epidemiology and significance of multidrug-resistant pathogens. Clin. Microbiol. Infect. 2019, 26, 151–157. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Species | Total Number of Isolates Tested | Africa | Asia | South America | Europe |
|---|---|---|---|---|---|
| Species Tested on the MSF Pos MIC Panel | |||||
| Staphylococcus aureus | 47 | 23 | 13 | 6 | 5 |
| Staphylococcus epidermidis | 11 | 5 | 3 | 1 | 2 |
| Staphylococcus hominis | 15 | 7 | 4 | 2 | 2 |
| Staphylococcus haemolyticus | 10 | 5 | 3 | 1 | 1 |
| Staphylococcus warneri | 1 | 1 | - | - | - |
| Enterococcus faecium | 35 | 14 | 10 | 4 | 4 |
| Enterococcus faecalis | 14 | 6 | 4 | 2 | 2 |
| Total isolates tested on the panel | 133 | 61 | 37 | 16 | 16 |
| Species Tested on the MSF Neg MIC Panel | |||||
| Escherichia coli | 25 | 12 | 7 | 3 | 3 |
| Klebsiella pneumoniae | 29 | 14 | 8 | 4 | 3 |
| Klebsiella oxytoca | 9 | 4 | 3 | 1 | 1 |
| Klebsiella ozaena | 1 | 1 | - | - | - |
| Morganella morganii | 1 | 1 | - | - | - |
| Salmonella Paratyphi A | 8 | 4 | 2 | 1 | 1 |
| Salmonella Typhimurium a | 8 | 4 | 2 | 1 | 1 |
| Salmonella Choleraesuis | 7 | 3 | 2 | 1 | 1 |
| Enterobacter cloacae | 16 | 7 | 5 | 2 | 2 |
| Enterobacter hermannii | 1 | 1 | - | - | - |
| Enterobacter kobei | 1 | 1 | - | - | - |
| Enterobacter asburiae | 1 | 1 | - | - | - |
| Citrobacter freundii complex | 5 | 2 | 1 | 1 | 1 |
| Pseudomonas aeruginosa | 15 | 7 | 4 | 2 | 2 |
| Acinetobacter baumannii complex | 14 | 6 | 4 | 2 | 2 |
| Burkholderia cepacia | 10 | 5 | 3 | 1 | 1 |
| Stenotrophomonas maltophilia | 6 | 3 | 2 | 1 | - |
| Total isolates tested on the panel | 157 | 76 | 43 | 20 | 18 |
| Species Tested on the MSF FAST MIC Panel | |||||
| Streptococcus pneumoniae | 54 | 26 | 15 | 7 | 6 |
| Streptococcus agalactiae | 37 | 17 | 12 | 4 | 4 |
| Streptococcus pyogenes | 30 | 14 | 9 | 4 | 3 |
| Streptococcus mitis | 22 | 10 | 6 | 3 | 2 |
| Streptocococcus oralis | 6 | 3 | 2 | 1 | 1 |
| Streptococcus anginosus | 10 | 5 | 3 | 1 | 1 |
| Streptococcus constellatus | 2 | 1 | 1 | - | - |
| Haemophilus influenzae | 20 | 10 | 6 | 2 | 2 |
| Total isolates tested on the panel | 181 | 86 | 54 | 22 | 19 |
| No. of Isolates AST Reference a | No. of Isolates MICPOS1 b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | Total | R | I | S | R | I | S | CA c (no. [%]) | mE d (no. [%]) | ME e (no. [%]) | VME f (no. [%]) |
| Penicillin | 63 | 59 | 0 | 4 | 59 | 0 | 4 | 63 (100) | 0 (0) | 0 (0) | 0 (0) |
| Ciprofloxacin | 74 | 37 | 0 | 37 | 39 | 0 | 35 | 72 (97) | 0 (0) | 2 (3) | 0 (0) |
| Amikacin | 74 | 17 | 4 | 53 | 16 | 8 | 50 | 69 (93) | 4 (5) | 1 (1) | 0 (0) |
| Gentamicin | 74 | 28 | 0 | 46 | 30 | 0 | 44 | 72 (97) | 0 (0) | 2 (3) | 0 (0) |
| Teicoplanin | 74 | 3 | 0 | 71 | 1 | 0 | 73 | 72 (97) | 0 (0) | 0 (0) | 2 (3) |
| Vancomycin | 74 | 2 | 0 | 72 | 2 | 0 | 72 | 74 (100) | 0 (0) | 0 (0) | 0 (0) |
| Quinupristin-dalfopristin | 74 | 0 | 7 | 67 | 0 | 7 | 67 | 74 (100) | 0 (0) | 0 (0) | 0 (0) |
| Erythromycin | 74 | 30 | 0 | 44 | 30 | 1 | 43 | 71 (96) | 1 (1) | 1 (1) | 1 (1) |
| Clindamycin | 74 | 14 | 0 | 60 | 12 | 1 | 61 | 72 (97) | 1 (1) | 0 (0) | 1 (1) |
| Daptomycin | 74 | 1 | 0 | 73 | 1 | 0 | 73 | 74 (100) | 0 (0) | 0 (0) | 0 (0) |
| Fosfomycin | 74 | 29 | 0 | 45 | 30 | 0 | 44 | 73 (99) | 0 (0) | 1 (1) | 0 (0) |
| Trimethoprim/Sulfamethoxazole | 74 | 18 | 0 | 56 | 19 | 3 | 52 | 70 (95) | 3 (4) | 1 (1) | 0 (0) |
| Linezolid | 74 | 5 | 0 | 69 | 5 | 0 | 69 | 74 (100) | 0 (0) | 0 (0) | 0 (0) |
| Tetracycline | 74 | 37 | 0 | 37 | 39 | 0 | 35 | 72 (97) | 0 (0) | 2 (3) | 0 (0) |
| Tigecycline | 74 | 0 | 0 | 74 | 1 | 0 | 73 | 73 (99) | 0 (0) | 1 (1) | 0 (0) |
| No. of Isolates AST Reference a | No. of Isolates MICPOS1 b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | Total | R | I | S | R | I | S | CA c (no. [%]) | mE d (no. [%]) | ME e (no. [%]) | VME f (no. [%]) |
| Ampicillin | 49 | 30 | 0 | 19 | 29 | 1 | 18 | 47 (96) | 0 (0) | 1 (2) | 1 (2) |
| Ciprofloxacin | 49 | 29 | 0 | 20 | 30 | 0 | 19 | 48 (98) | 0 (0) | 1 (2) | 0 (0) |
| Teicoplanin | 49 | 23 | 0 | 26 | 23 | 0 | 26 | 49 (100) | 0 (0) | 0 (0) | 0 (0) |
| Vancomycin | 49 | 23 | 0 | 26 | 23 | 0 | 26 | 49 (100) | 0 (0) | 0(0) | 0 (0) |
| Quinupristin-dalfopristin | 49 | 19 | 16 | 14 | 19 | 16 | 14 | 45 (91) | 4 (9) | 0 (0) | 0 (0) |
| Linezolid | 49 | 2 | 0 | 47 | 2 | 0 | 47 | 49 (100) | 0 (0) | 0 (0) | 0 (0) |
| Tigecycline | 49 | 4 | 0 | 45 | 4 | 0 | 45 | 47 (96) | 0 (0) | 1 (2) | 1 (2) |
| No. of Isolates AST Reference a | No. of Isolates MICPNEG1 b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | Total | R | I | S | R | I | S | CA c (no. [%]) | mE d (no. [%]) | ME e (no. [%]) | VME f (no. [%]) |
| Ampicillin | 112 | 100 | 0 | 12 | 99 | 0 | 13 | 111 (99) | 0 (0) | 0 (0) | 1 (1) |
| Amoxicillin/Clavulanic Acid | 112 | 72 | 0 | 40 | 73 | 0 | 39 | 109 (97) | 0 (0) | 2 (2) | 1 (1) |
| Ceftazidime | 112 | 47 | 2 | 63 | 49 | 0 | 64 | 108 (96) | 3 (3) | 1 (1) | 0 (0) |
| Ceftriaxone | 112 | 50 | 0 | 62 | 51 | 1 | 60 | 110 (98) | 1 (1) | 1 (1) | 0 (0) |
| Piperacillin/Tazobactam | 112 | 39 | 4 | 69 | 39 | 4 | 69 | 106 (93) | 6 (7) | 0 (0) | 0 (0) |
| Ciprofloxacin | 112 | 51 | 4 | 57 | 53 | 4 | 55 | 106 (93) | 4 (4) | 2 (2) | 0 (0) |
| Amikacin | 112 | 16 | 4 | 92 | 14 | 5 | 93 | 106 (93) | 5 (6) | 0 (0) | 1 (1) |
| Gentamicin | 112 | 40 | 5 | 67 | 40 | 4 | 68 | 104 (92) | 4 (4) | 2 (2) | 2 (2) |
| Trimethoprim/Sulfamethoxazole | 112 | 69 | 1 | 42 | 69 | 0 | 43 | 108 (96) | 1 (1) | 1 (1) | 2 (2) |
| Chloramphenicol | 112 | 47 | 0 | 65 | 47 | 0 | 65 | 112 (100) | 0 (0) | 0 (0) | 0 (0) |
| Colistin | 112 | 12 | 0 | 77 | 12 | 0 | 77 | 110 (98) | 0 (0) | 1 (1) | 1 (1) |
| Fosfomycin | 112 | 1 | 0 | 111 | 1 | 0 | 111 | 112 (100) | 0 (0) | 0 (0) | 0 (0) |
| Tigecycline | 112 | 0 | 0 | 112 | 0 | 0 | 112 | 112 (100) | 0 (0) | 0 (0) | 0 (0) |
| Meropenem | 112 | 16 | 6 | 90 | 17 | 6 | 79 | 106 (93) | 5 (6) | 1 (1) | 0 (0) |
| Imipenem | 112 | 19 | 7 | 86 | 19 | 7 | 86 | 112 (100) | 0 (0) | 0 (0) | 0 (0) |
| Ertapenem | 112 | 33 | 0 | 79 | 32 | 0 | 80 | 111 (99) | 0 (0) | 0 (0) | 1 (1) |
| No. of Isolates AST Reference a | No. of Isolates MICPNEG1 b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | Total | R | I | S | R | I | S | CA c (no. [%]) | mE d (no. [%]) | ME e (no. [%]) | VME f (no. [%]) |
| Ceftazidime | 15 | 8 | 3 | 4 | 8 | 2 | 5 | 14 (96) | 1 (4) | 0 (0) | 0 (0) |
| Piperacillin/Tazobactam | 15 | 4 | 0 | 11 | 4 | 0 | 11 | 15 (100) | 0 (0) | 0 (0) | 0 (0) |
| Ciprofloxacin | 29 | 12 | 6 | 11 | 12 | 6 | 11 | 29 (100) | 0 (0) | 0 (0) | 0 (0) |
| Amikacin | 29 | 7 | 2 | 20 | 7 | 2 | 20 | 29 (100) | 0 (0) | 0 (0) | 0 (0) |
| Gentamicin | 29 | 15 | 0 | 14 | 15 | 0 | 14 | 29 (100) | 0 (0) | 0 (0) | 0 (0) |
| Trimethoprim/Sulfamethoxazole | 29 | 10 | 0 | 20 | 9 | 1 | 20 | 28 (99) | 1 (1) | 0 (0) | 0 (0) |
| Chloramphenicol | 9 | 4 | 3 | 2 | 4 | 3 | 2 | 9 (100) | 0 (0) | 0 (0) | 0 (0) |
| Colistin | 15 | 3 | 0 | 12 | 3 | 0 | 12 | 15 (100) | 0 (0) | 0 (0) | 0 (0) |
| Meropenem | 45 | 14 | 6 | 25 | 14 | 6 | 25 | 43 (96) | 2 (4) | 0 (0) | 0 (0) |
| Imipenem | 29 | 12 | 0 | 17 | 10 | 1 | 18 | 27 (94) | 1 (3) | 0 (0) | 1 (3) |
| No. of Isolates AST Reference a | No. of Isolates MICPFAST1 b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | Total | R | I | S | R | I | S | CA c (no. [%]) | mE d (no. [%]) | ME e (no. [%]) | VME f (no. [%]) |
| Penicillin | 87 | 10 | 9 | 68 | 12 | 8 | 67 | 84 (97) | 2 (2) | 1 (1) | 0 (0) |
| Meropenem g | 53 | 0 | 0 | 53 | 1 | 0 | 52 | 52 (98) | 0 (0) | 1 (2) | 0 (0) |
| Ceftriaxone f | - | - | - | - | - | - | - | - | - | - | - |
| Ampicillin g | 53 | 12 | 6 | 35 | 14 | 2 | 37 | 49 (92) | 4 (8) | 0 (0) | 0 (0) |
| Levofloxacin h | 63 | 1 | 0 | 62 | 1 | 0 | 62 | 63 (100) | 0 (0) | 0 (0) | 0 (0) |
| Vancomycin | 87 | 2 | 0 | 85 | 1 | 0 | 86 | 86 (99) | 0 (0) | 0 (0) | 1 (1) |
| Clindamycin | 87 | 16 | 0 | 71 | 16 | 0 | 71 | 85 (98) | 0 (0) | 1 (1) | 1 (1) |
| Trimethoprim/Sulfamethoxazole | 87 | 4 | 0 | 83 | 4 | 0 | 83 | 85 (98) | 0 (0) | 1 (1) | 1 (1) |
| Chloramphenicol | 87 | 3 | 0 | 84 | 2 | 0 | 85 | 86 (99) | 0 (0) | 0 (0) | 1 (1) |
| Linezolid i | 63 | 0 | 0 | 63 | 0 | 0 | 63 | 63 (100) | 0 (0) | 0 (0) | 0 (0) |
| No. of Isolates AST Reference a | No. of Isolates MICPFAST1 b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | Total | R | I | S | R | I | S | CA c (no. [%]) | mE d (no. [%]) | ME e (no. [%]) | VME f (no. [%]) |
| Meropenem | 20 | 0 | 0 | 20 | 0 | 0 | 20 | 20 (100) | 0 (0) | 0 (0) | 0 (0) |
| Ceftriaxone | 20 | 3 | 0 | 17 | 3 | 0 | 17 | 20 (100) | 0 (0) | 0 (0) | 0 (0) |
| Ampicillin | 20 | 2 | 0 | 18 | 2 | 0 | 18 | 20 (100) | 0 (0) | 0 (0) | 0 (0) |
| Ciprofloxacin | 20 | 3 | 0 | 17 | 3 | 0 | 17 | 20 (100) | 0 (0) | 0 (0) | 0 (0) |
| Levofloxacin | 20 | 2 | 0 | 18 | 2 | 0 | 18 | 20 (100) | 0 (0) | 0 (0) | 0 (0) |
| Trimethoprim/Sulfamethoxazole | 20 | 6 | 1 | 13 | 7 | 0 | 13 | 19 (95) | 1 (5) | 0 (0) | 0 (0) |
| Chloramphenicol | 20 | 0 | 0 | 20 | 0 | 0 | 20 | 20 (100) | 0 (0) | 0 (0) | 0 (0) |
| No. of Isolates | AST Referencea | MSF Panel b | ||||||
|---|---|---|---|---|---|---|---|---|
| Multidrug Resistant Organism | Total | R | S | R | S | CA c (no. [%]) | ME d (no. [%]) | VME e (no. [%]) |
| Methicillin-resistant Staphylococcus aureus f | 47 | 33 | 14 | 33 | 14 | 47 (100) | 0 (0) | 0 (0) |
| Inducible clindamycin-resistant Staphylococci f | 74 | 26 | 48 | 26 | 48 | 74 (100) | 0(0) | 0 (0) |
| Vancomycin-resistant Staphylococcus aureus f | 47 | 2 | 45 | 2 | 45 | 47 (100) | 0 (0) | 0 (0) |
| High-level gentamicin resistance Staphylococci f | 49 | 25 | 24 | 25 | 24 | 47 (96) | 1 (2) | 1 (2) |
| Vancomycin-resistant Enterococci f | 49 | 23 | 26 | 23 | 26 | 49 (100) | 0(0) | 0 (0) |
| Extended-spectrum beta-lactamase-producing Enterobacterales g | 112 | 19 | 93 | 19 | 93 | 112 (100) | 0 (0) | 0 (0) |
| Carbapenem-resistant Enterobacterales g | 112 | 33 | 79 | 32 | 80 | 111 (99) | 0 (0) | 1 (1) |
| Colistin-resistant Enterobacterales g | 112 | 12 | 77 | 12 | 77 | 110 (98) | 1 (1) | 1 (1) |
| Carbapenem-resistant Pseudomonas aeruginosa g | 15 | 4 | 11 | 4 | 11 | 15 (100) | 0 (0) | 0 (0) |
| Colistin-resistant Pseudomonas aeruginosa g | 15 | 4 | 11 | 4 | 11 | 15 (100) | 0 (0) | 0 (0) |
| Carbapenem-resistant Acinetobacter baumannii g | 14 | 8 | 6 | 8 | 6 | 15 (100) | 0 (0) | 0 (0) |
| Staphylococci and Enterococci | Gram-negative bacilli | Fastidious organisms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | n a | Kappa Cohen | R1 CA b [%] | R2 CA c [%] | n a | Kappa Cohen | R1 CA b [%] | R2 CA c [%] | n a | Kappa Cohen | R1 CA b [%] | R2 CA c [%] |
| Penicillin | 63 | 0.95 | 98 | 98 | 87 | 0.99 | 97 | 97 | ||||
| Ampicillin | 123 | 0.76 | 96 | 92 | 112 | 0.91 | 99 | 98 | 107 | 1.00 | 98 | 98 |
| Amoxicillin/Clavulanic Ac | 112 | 0.97 | 99 | 98 | ||||||||
| Cefoxitin screening/Oxacillin | 74 | 0.95 | 92 | 93 | ||||||||
| Ceftazidime | 127 | 0.95 | 97 | 96 | ||||||||
| Ceftriaxone | 112 | 0.89 | 97 | 98 | 20 | 1.00 | 100 | 100 | ||||
| ESBL test | 112 | 0.97 | 99 | 97 | ||||||||
| Piperacillin/Tazobactam | 127 | 0.97 | 99 | 93 | ||||||||
| Levofloxacin | 83 | 0.98 | 100 | 100 | ||||||||
| Ciprofloxacin | 49 | 0.89 | 99 | 99 | 141 | 0.95 | 94 | 96 | ||||
| Amikacin | 123 | 0.78 | 78 | 76 | 141 | 0.99 | 99 | 93 | ||||
| Gentamicin | 123 | 0.92 | 100 | 96 | 141 | 1.00 | 92 | 92 | ||||
| Gentamicin (high level) | 49 | 0.90 | 90 | 90 | ||||||||
| Teicoplanin | 123 | 0.79 | 99 | 96 | ||||||||
| Vancomycin | 123 | 1.00 | 97 | 97 | 87 | 1.00 | 98 | 98 | ||||
| Quinupristin-dalfopristin | 123 | 0.93 | 89 | 91 | ||||||||
| Erythromycin | 74 | 0.97 | 96 | 96 | ||||||||
| Clindamycin | 74 | 0.99 | 97 | 97 | 87 | 0.64 | 100 | 100 | ||||
| Inducible clindamycin resistance | 74 | 0.96 | 97 | 95 | ||||||||
| Daptomycin | 74 | 0.37 | 96 | 96 | ||||||||
| Fosfomycin | 74 | 0.63 | 76 | 77 | 112 | 0.76 | 100 | 100 | ||||
| Trimethoprim/Sulfamethoxazole | 74 | 0.62 | 95 | 95 | 142 | 0.87 | 96 | 96 | 107 | 0.92 | 98 | 93 |
| Linezolid | 123 | 0.37 | 97 | 96 | 63 | 1.00 | 100 | 100 | ||||
| Tetracycline | 74 | 0.94 | 97 | 97 | ||||||||
| Tigecycline | 123 | 0.82 | 95 | 94 | 112 | 0.97 | 100 | 100 | ||||
| Chloramphenicol | 121 | 0.90 | 99 | 99 | 107 | 1.00 | 98 | 98 | ||||
| Colistin | 127 | 0.97 | 98 | 98 | ||||||||
| Meropenem | 157 | 0.96 | 93 | 93 | 73 | 0.97 | 98 | 98 | ||||
| Imipenem | 141 | 0.96 | 100 | 100 | ||||||||
| Ertapenem | 112 | 0.97 | 99 | 99 | ||||||||
| Average all molecules | 0.82 | 94 | 93 | 0.94 | 98 | 97 | 0.95 | 99 | 98 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ronat, J.-B.; Oueslati, S.; Natale, A.; Kesteman, T.; Elamin, W.; Langendorf, C.; Hardy, L.; Vandenberg, O.; Naas, T. Validation of Three MicroScan® Antimicrobial Susceptibility Testing Plates Designed for Low-Resource Settings. Diagnostics 2022, 12, 2106. https://doi.org/10.3390/diagnostics12092106
Ronat J-B, Oueslati S, Natale A, Kesteman T, Elamin W, Langendorf C, Hardy L, Vandenberg O, Naas T. Validation of Three MicroScan® Antimicrobial Susceptibility Testing Plates Designed for Low-Resource Settings. Diagnostics. 2022; 12(9):2106. https://doi.org/10.3390/diagnostics12092106
Chicago/Turabian StyleRonat, Jean-Baptiste, Saoussen Oueslati, Alessandra Natale, Thomas Kesteman, Wael Elamin, Céline Langendorf, Liselotte Hardy, Olivier Vandenberg, and Thierry Naas. 2022. "Validation of Three MicroScan® Antimicrobial Susceptibility Testing Plates Designed for Low-Resource Settings" Diagnostics 12, no. 9: 2106. https://doi.org/10.3390/diagnostics12092106