
Predictors of Bone Metastases at 68Ga-PSMA-11 PET/CT in Hormone-Sensitive Prostate Cancer (HSPC) Patients with Early Biochemical Recurrence or Persistence

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Objectives
2.3. Procedures and Image Interpretation
2.4. Statistical Analysis
3. Results
3.1. Cohort Characteristics
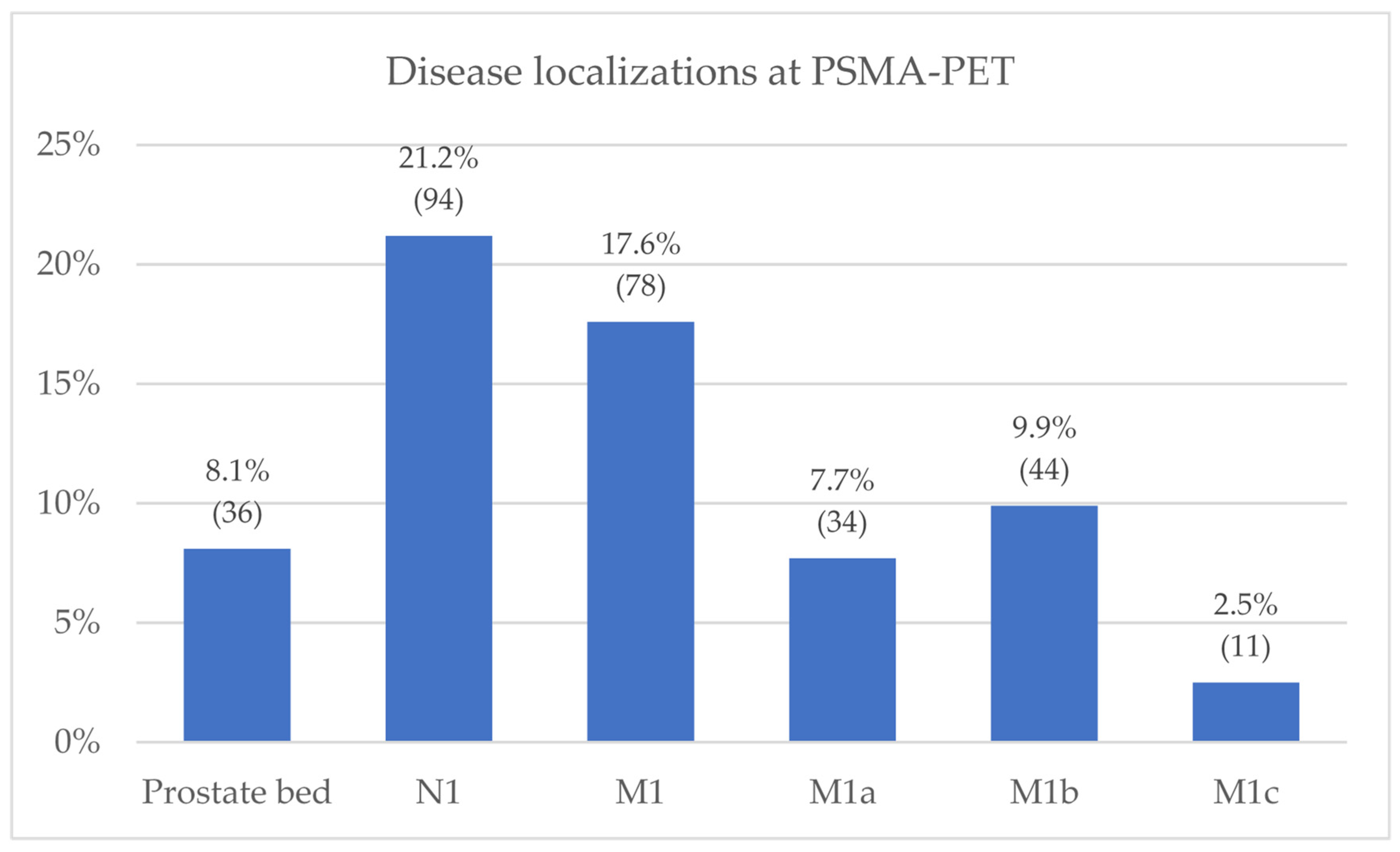
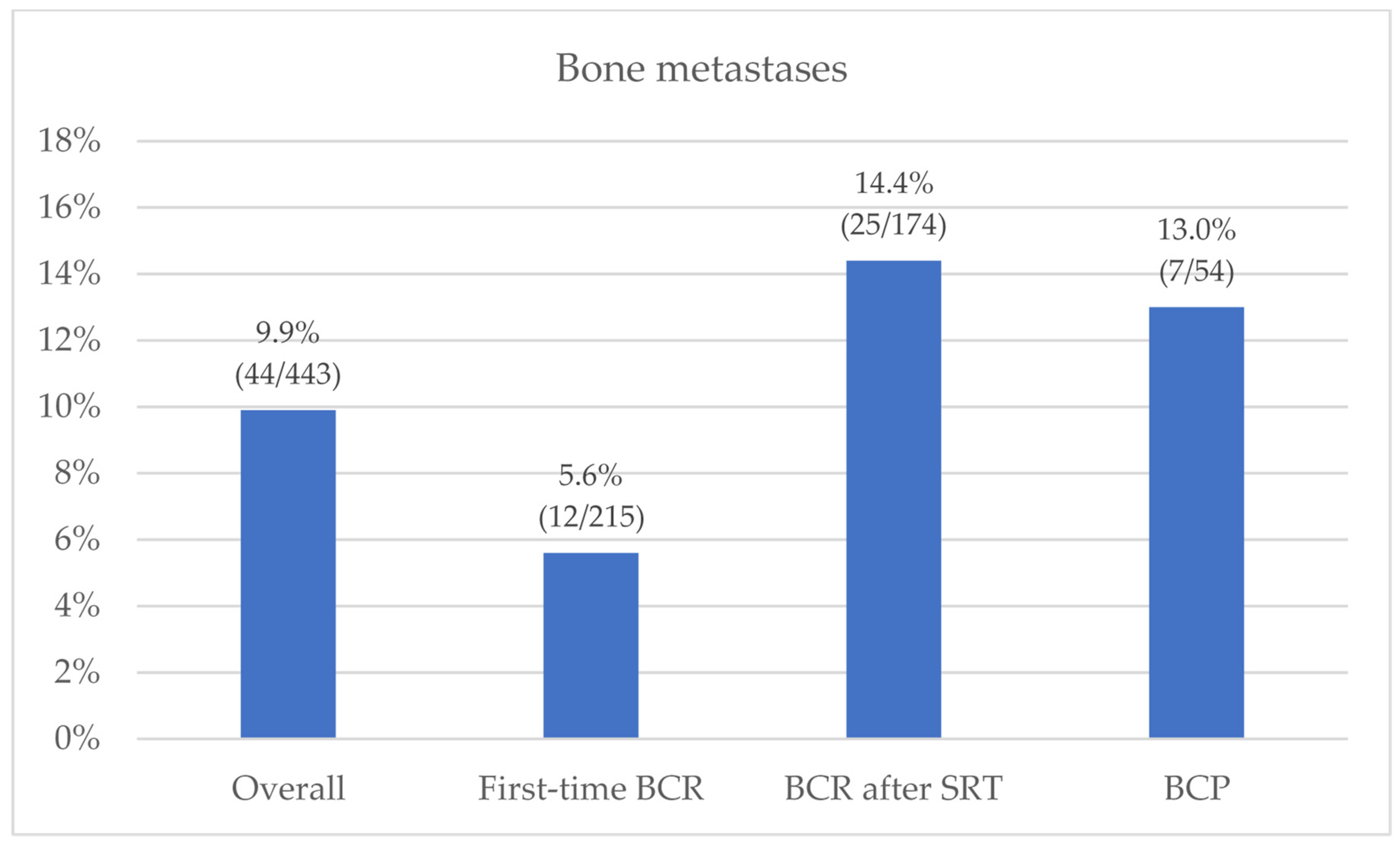
3.2. PSMA-PET Results
3.3. Predictors Analysis
4. Discussion
4.1. Future Perspectives
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beresford, M.J.; Gillatt, D.; Benson, R.J.; Ajithkumar, T. A Systematic Review of the Role of Imaging before Salvage Radiotherapy for Post-Prostatectomy Biochemical Recurrence. Clin. Oncol. 2010, 22, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-Specific Membrane Antigen PET-CT in Patients with High-Risk Prostate Cancer before Curative-Intent Surgery or Radiotherapy (ProPSMA): A Prospective, Randomised, Multicentre Study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Ferraro, D.A.; Garcia Schüler, H.I.; Muehlematter, U.J.; Eberli, D.; Müller, J.; Müller, A.; Gablinger, R.; Kranzbühler, H.; Omlin, A.; Kaufmann, P.A.; et al. Impact of 68Ga-PSMA-11 PET Staging on Clinical Decision-Making in Patients with Intermediate or High-Risk Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 652–664. [Google Scholar] [CrossRef] [PubMed]
- Emmett, L.; Metser, U.; Bauman, G.; Hicks, R.J.; Weickhardt, A.; Davis, I.D.; Punwani, S.; Pond, G.; Chua, S.; Ho, B.; et al. Prospective, Multisite, International Comparison of 18F-Fluoromethylcholine PET/CT, Multiparametric MRI, and 68Ga-HBED-CC PSMA-11 PET/CT in Men with High-Risk Features and Biochemical Failure After Radical Prostatectomy: Clinical Performance and Patient Outcomes. J. Nucl. Med. 2019, 60, 794–800. [Google Scholar] [CrossRef] [Green Version]
- Calais, J.; Ceci, F.; Eiber, M.; Hope, T.A.; Hofman, M.S.; Rischpler, C.; Bach-Gansmo, T.; Nanni, C.; Savir-Baruch, B.; Elashoff, D.; et al. 18F-Fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in Patients with Early Biochemical Recurrence after Prostatectomy: A Prospective, Single-Centre, Single-Arm, Comparative Imaging Trial. Lancet Oncol. 2019, 20, 1286–1294. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Mier, W.; Haufe, S.; Debus, N.; Eder, M.; Eisenhut, M.; Schäfer, M.; et al. Diagnostic Performance of 68Ga-PSMA-11 (HBED-CC) PET/CT in Patients with Recurrent Prostate Cancer: Evaluation in 1007 Patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1258–1268. [Google Scholar] [CrossRef] [Green Version]
- Fendler, W.P.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.B.; Okamoto, S.; et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019, 5, 856–863. [Google Scholar] [CrossRef] [Green Version]
- Pienta, K.J.; Gorin, M.A.; Rowe, S.P.; Carroll, P.R.; Pouliot, F.; Probst, S.; Saperstein, L.; Preston, M.A.; Alva, A.S.; Patnaik, A.; et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate-Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J. Urol. 2021, 206, 52–61. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; De Santis, M.; Fanti, S.; Gillessen, S.; Grummet, J.; Henry, A.M.; Lam, T.B.; et al. European Association of Urology Guidelines. 2020 Edition. In Proceedings of the EAU Annual Congress, Amsterdam, The Netherlands, 17–21 May 2020. [Google Scholar]
- Calais, J.; Fendler, W.P.; Eiber, M.; Gartmann, J.; Chu, F.-I.; Nickols, N.G.; Reiter, R.E.; Rettig, M.B.; Marks, L.S.; Ahlering, T.E.; et al. Impact of 68Ga-PSMA-11 PET/CT on the Management of Prostate Cancer Patients with Biochemical Recurrence. J. Nucl. Med. 2018, 59, 434–441. [Google Scholar] [CrossRef] [Green Version]
- Deandreis, D.; Guarneri, A.; Ceci, F.; Lillaz, B.; Bartoncini, S.; Oderda, M.; Nicolotti, D.G.; Pilati, E.; Passera, R.; Zitella, A.; et al. 68Ga-PSMA-11 PET/CT in Recurrent Hormone-Sensitive Prostate Cancer (HSPC): A Prospective Single-Centre Study in Patients Eligible for Salvage Therapy. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2804–2815. [Google Scholar] [CrossRef]
- Valle, L.; Shabsovich, D.; de Meerleer, G.; Maurer, T.; Murphy, D.G.; Nickols, N.G.; Vapiwala, N.; Calais, J.; Kishan, A.U. Use and Impact of Positron Emission Tomography/Computed Tomography Prior to Salvage Radiation Therapy in Men with Biochemical Recurrence After Radical Prostatectomy: A Scoping Review. Eur. Urol. Oncol. 2021, 4, 339–355. [Google Scholar] [CrossRef] [PubMed]
- Ong, W.L.; Koh, T.L.; Lim Joon, D.; Chao, M.; Farrugia, B.; Lau, E.; Khoo, V.; Lawrentschuk, N.; Bolton, D.; Foroudi, F. Prostate-Specific Membrane Antigen-Positron Emission Tomography/Computed Tomography (PSMA-PET/CT)-Guided Stereotactic Ablative Body Radiotherapy for Oligometastatic Prostate Cancer: A Single-Institution Experience and Review of the Published Literature. BJU Int. 2019, 124 (Suppl. S1), 19–30. [Google Scholar] [CrossRef] [PubMed]
- Onal, C.; Ozyigit, G.; Akgun, Z.; Atalar, B.; Igdem, S.; Oymak, E.; Agaoglu, F.; Selek, U.; Guler, O.C.; Hurmuz, P.; et al. Oligometastatic Bone Disease in Castration-Sensitive Prostate Cancer Patients Treated with Stereotactic Body Radiotherapy Using 68Ga-PSMA PET/CT: TROD 09-004 Study. Clin. Nucl. Med. 2021, 46, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Koerber, S.A.; Sprute, K.; Kratochwil, C.; Winter, E.; Haefner, M.F.; Katayama, S.; Schlampp, I.; Herfarth, K.; Kopka, K.; Afshar-Oromieh, A.; et al. Clinical Outcome of PSMA-Guided Radiotherapy for Patients with Oligorecurrent Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 143–151. [Google Scholar] [CrossRef]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs. Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef] [Green Version]
- Rovera, G.; Oprea-Lager, D.E.; Ceci, F. Health Technology Assessment for PSMA-PET: Striving towards a Cost-Effective Management of Prostate Cancer. Clin. Transl. Imaging 2021, 9, 409–412. [Google Scholar] [CrossRef]
- Fendler, W.P.; Eiber, M.; Beheshti, M.; Bomanji, J.; Ceci, F.; Cho, S.; Giesel, F.; Haberkorn, U.; Hope, T.A.; Kopka, K.; et al. 68Ga-PSMA PET/CT: Joint EANM and SNMMI Procedure Guideline for Prostate Cancer Imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1014–1024. [Google Scholar] [CrossRef]
- Ceci, F.; Oprea-Lager, D.E.; Emmett, L.; Adam, J.A.; Bomanji, J.; Czernin, J.; Eiber, M.; Haberkorn, U.; Hofman, M.S.; Hope, T.A.; et al. E-PSMA: The EANM Standardized Reporting Guidelines v1.0 for PSMA-PET. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1626–1638. [Google Scholar] [CrossRef]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed MiTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Carter, H.B.; Epstein, J.I.; Miller, M.C.; Landis, P.; Walsh, P.W.; Partin, A.W.; Veltri, R.W. Can Prostate Specific Antigen Derivatives and Pathological Parameters Predict Significant Change in Expectant Management Criteria for Prostate Cancer? J. Urol. 2003, 170, 2274–2278. [Google Scholar] [CrossRef]
- Perera, M.; Papa, N.; Roberts, M.; Williams, M.; Udovicich, C.; Vela, I.; Christidis, D.; Bolton, D.; Hofman, M.S.; Lawrentschuk, N.; et al. Gallium-68 Prostate-Specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer-Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-Specific Membrane Antigen-Avid Lesions: A Systematic Review and Meta-Analysis. Eur. Urol. 2020, 77, 403–417. [Google Scholar] [CrossRef] [PubMed]
- Ceci, F.; Castellucci, P.; Graziani, T.; Farolfi, A.; Fonti, C.; Lodi, F.; Fanti, S. 68Ga-PSMA-11 PET/CT in Recurrent Prostate Cancer: Efficacy in Different Clinical Stages of PSA Failure after Radical Therapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Ceci, F.; Rovera, G.; Iorio, G.C.; Guarneri, A.; Chiofalo, V.; Passera, R.; Oderda, M.; Dall’Armellina, S.; Liberini, V.; Grimaldi, S.; et al. Event-Free Survival after 68 Ga-PSMA-11 PET/CT in Recurrent Hormone-Sensitive Prostate Cancer (HSPC) Patients Eligible for Salvage Therapy. Eur. J. Nucl. Med. Mol. Imaging 2022. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi Bidakhvidi, N.; Laenen, A.; Jentjens, S.; Deroose, C.M.; Van Laere, K.; De Wever, L.; Mai, C.; Berghen, C.; De Meerleer, G.; Haustermans, K.; et al. Parameters Predicting [18F]PSMA-1007 Scan Positivity and Type and Number of Detected Lesions in Patients with Biochemical Recurrence of Prostate Cancer. EJNMMI Res. 2021, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Pomykala, K.L.; Czernin, J.; Grogan, T.R.; Armstrong, W.R.; Williams, J.; Calais, J. Total-Body 68Ga-PSMA-11 PET/CT for Bone Metastasis Detection in Prostate Cancer Patients: Potential Impact on Bone Scan Guidelines. J. Nucl. Med. 2020, 61, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Briganti, A.; Suardi, N.; Gallina, A.; Abdollah, F.; Novara, G.; Ficarra, V.; Montorsi, F. Predicting the Risk of Bone Metastasis in Prostate Cancer. Cancer Treat. Rev. 2014, 40, 3–11. [Google Scholar] [CrossRef]
- Verburg, F.A.; Pfister, D.; Heidenreich, A.; Vogg, A.; Drude, N.I.; Vöö, S.; Mottaghy, F.M.; Behrendt, F.F. Extent of Disease in Recurrent Prostate Cancer Determined by [(68)Ga]PSMA-HBED-CC PET/CT in Relation to PSA Levels, PSA Doubling Time and Gleason Score. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 397–403. [Google Scholar] [CrossRef]
- Ceci, F.; Bianchi, L.; Borghesi, M.; Polverari, G.; Farolfi, A.; Briganti, A.; Schiavina, R.; Brunocilla, E.; Castellucci, P.; Fanti, S. Prediction Nomogram for 68Ga-PSMA-11 PET/CT in Different Clinical Settings of PSA Failure after Radical Treatment for Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 136–146. [Google Scholar] [CrossRef]
- Ferdinandus, J.; Fendler, W.P.; Farolfi, A.; Washington, S.; Mohamad, O.; Pampaloni, M.H.; Scott, P.J.H.; Rodnick, M.; Viglianti, B.L.; Eiber, M.; et al. PSMA PET Validates Higher Rates of Metastatic Disease for European Association of Urology Biochemical Recurrence Risk Groups: An International Multicenter Study. J. Nucl. Med. 2022, 63, 76–80. [Google Scholar] [CrossRef]
- Meijer, D.; Donswijk, M.L.; Bodar, Y.J.L.; van Leeuwen, P.J.; van der Poel, H.G.; Vogel, W.V.; Nieuwenhuijzen, J.A.; Hendrikse, N.H.; Oprea-Lager, D.E.; Vis, A.N. Biochemical Persistence of Prostate-Specific Antigen After Robot-Assisted Laparoscopic Radical Prostatectomy: Tumor Localizations Using PSMA PET/CT Imaging. J. Nucl. Med. 2021, 62, 961–967. [Google Scholar] [CrossRef]
- Farolfi, A.; Gafita, A.; Calais, J.; Eiber, M.; Afshar-Oromieh, A.; Spohn, F.; Barbato, F.; Weber, M.; Ilhan, H.; Cervati, V.; et al. 68Ga-PSMA-11 Positron Emission Tomography Detects Residual Prostate Cancer after Prostatectomy in a Multicenter Retrospective Study. J. Urol. 2019, 202, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, L.; Nini, A.; Bianchi, M.; Gandaglia, G.; Fossati, N.; Suardi, N.; Moschini, M.; Dell’Oglio, P.; Schiavina, R.; Montorsi, F.; et al. The Role of Prostate-Specific Antigen Persistence After Radical Prostatectomy for the Prediction of Clinical Progression and Cancer-Specific Mortality in Node-Positive Prostate Cancer Patients. Eur. Urol. 2016, 69, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Pereira Mestre, R.; Treglia, G.; Ferrari, M.; Pascale, M.; Mazzara, C.; Azinwi, N.C.; Llado’, A.; Stathis, A.; Giovanella, L.; Roggero, E. Correlation between PSA Kinetics and PSMA-PET in Prostate Cancer Restaging: A Meta-Analysis. Eur. J. Clin. Investig. 2019, 49, e13063. [Google Scholar] [CrossRef]
- Mena, E.; Rowe, S.P.; Shih, J.H.; Lindenberg, L.; Turkbey, B.; Fourquet, A.; Lin, F.I.; Adler, S.; Eclarinal, P.; McKinney, Y.L.; et al. Predictors of 18F-DCFPyL-PET/CT Positivity in Patients with Biochemical Recurrence of Prostate Cancer After Local Therapy. J. Nucl. Med. 2021. [Google Scholar] [CrossRef]
- Mena, E.; Lindenberg, M.L.; Turkbey, I.B.; Shih, J.H.; Harmon, S.A.; Lim, I.; Lin, F.; Adler, S.; Eclarinal, P.; McKinney, Y.L.; et al. 18F-DCFPyL PET/CT Imaging in Patients with Biochemically Recurrent Prostate Cancer After Primary Local Therapy. J. Nucl. Med. 2020, 61, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, D.A.; Rüschoff, J.H.; Muehlematter, U.J.; Kranzbühler, B.; Müller, J.; Messerli, M.; Husmann, L.; Hermanns, T.; Eberli, D.; Rupp, N.J.; et al. Immunohistochemical PSMA Expression Patterns of Primary Prostate Cancer Tissue Are Associated with the Detection Rate of Biochemical Recurrence with 68Ga-PSMA-11-PET. Theranostics 2020, 10, 6082–6094. [Google Scholar] [CrossRef] [PubMed]
- Salter, C.A.; Cullen, J.; Kuo, C.; Chen, Y.; Hurwitz, L.; Metwalli, A.R.; Dimitrakoff, J.; Rosner, I.L. Alkaline Phosphatase Kinetics Predict Metastasis among Prostate Cancer Patients Who Experience Relapse Following Radical Prostatectomy. BioMed Res. Int. 2018, 2018, 4727089. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.J.; Rowe, S.P.; Gorin, M.A.; Saperstein, L.; Pouliot, F.; Josephson, D.Y.; Wong, J.Y.; Pantel, A.R.; Cho, S.Y.; Gage, K.L.; et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase 3, Multicenter Study. Clin. Cancer Res. 2021, 27, 3674–3682. [Google Scholar] [CrossRef]
- Bianchi, L.; Castellucci, P.; Farolfi, A.; Droghetti, M.; Artigas, C.; Leite, J.; Corona, P.; Shagera, Q.A.; Moreira, R.; González, C.; et al. Multicenter External Validation of a Nomogram for Predicting Positive Prostate-Specific Membrane Antigen/Positron Emission Tomography Scan in Patients with Prostate Cancer Recurrence. Eur. Urol. Oncol. 2021, 30–40. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Features | Median | IQR | |
|---|---|---|---|
| Age (years) | 74 | 68–78 | |
| iPSA (ng/mL) | 7.85 | 5.73–12.00 | |
| PSA at PET scan (ng/mL) | 0.60 | 0.38–1.04 | |
| PSAdt at PET scan (months) | 8.2 | 4.2–14.6 | |
| PSAvel at PET scan (ng/mL/year) | 0.5 | 0.3–1.2 | |
| Clinical features | Frequency n (%) | ||
| ISUP Grade | 1 | 49 (11.1%) | |
| 2 | 96 (21.7%) | ||
| 3 | 137 (30.9%) | ||
| 4 | 80 (18.1%) | ||
| 5 | 57 (12.9%) | ||
| Missing | 24 (5.4%) | ||
| pT stage | <3a | 192 (43.3%) | |
| ≥3a | 228 (51.5%) | ||
| Missing | 23 (5.2%) | ||
| pN stage | N1 | 42 (9.5%) | |
| R (margin) | R1 | 160 (36.1%) | |
| Time to PSA relapse (months) | >12 | 314 (70.9%) | |
| ≤12 | 124 (28.0%) | ||
| Primary therapy | RP ± LND ± adjuvant RT | 417 (94.1%) | |
| Primary RT | 20 (4.5%) | ||
| Clinical stage of PSA failure at PSMA PET/CT | First-time BCR (subgroup-1) | 215 (48.5%) | |
| PSA relapse after prostate-bed SRT (subgroup-2) | 174 (39.3%) | ||
| BCP after RP (subgroup-3) | 54 (12.2%) | ||
| Potential Predictors of Bone Recurrence | Univariate Model | Multivariate Model | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| T stage (≥3a) | 2.59 | 1.26–5.30 | 0.009 | 2.52 | 1.13–5.60 | 0.024 |
| ISUP Grade (≥4) | 2.37 | 1.24–4.54 | 0.009 | - | - | 0.146 |
| Clinical Setting BCR after SRT vs. first-BCR BCP vs. first-BCR | ||||||
| 2.84 | 1.38–5.83 | 0.005 | 2.90 | 1.32–6.35 | 0.008 | |
| 2.52 | 0.94–6.74 | 0.066 | - | - | - | |
| PSA (ng/mL) at PSMA-PET | 0.98 | 0.82–1.17 | 0.84 | - | - | - |
| Time to recurrence (months) | 1.00 | 0.99–1.01 | 0.46 | - | - | - |
| PSA doubling time (months) | 0.91 | 0.86–0.97 | 0.004 | 0.93 | 0.88–0.99 | 0.026 |
| PSA velocity (ng/mL/year) | 1.03 | 0.98–1.09 | 0.27 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rovera, G.; Grimaldi, S.; Dall’Armellina, S.; Passera, R.; Oderda, M.; Iorio, G.C.; Guarneri, A.; Gontero, P.; Ricardi, U.; Deandreis, D. Predictors of Bone Metastases at 68Ga-PSMA-11 PET/CT in Hormone-Sensitive Prostate Cancer (HSPC) Patients with Early Biochemical Recurrence or Persistence. Diagnostics 2022, 12, 1309. https://doi.org/10.3390/diagnostics12061309
Rovera G, Grimaldi S, Dall’Armellina S, Passera R, Oderda M, Iorio GC, Guarneri A, Gontero P, Ricardi U, Deandreis D. Predictors of Bone Metastases at 68Ga-PSMA-11 PET/CT in Hormone-Sensitive Prostate Cancer (HSPC) Patients with Early Biochemical Recurrence or Persistence. Diagnostics. 2022; 12(6):1309. https://doi.org/10.3390/diagnostics12061309
Chicago/Turabian StyleRovera, Guido, Serena Grimaldi, Sara Dall’Armellina, Roberto Passera, Marco Oderda, Giuseppe Carlo Iorio, Alessia Guarneri, Paolo Gontero, Umberto Ricardi, and Désirée Deandreis. 2022. "Predictors of Bone Metastases at 68Ga-PSMA-11 PET/CT in Hormone-Sensitive Prostate Cancer (HSPC) Patients with Early Biochemical Recurrence or Persistence" Diagnostics 12, no. 6: 1309. https://doi.org/10.3390/diagnostics12061309