
An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review

 , , , , and
, , , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. COVID-19 ARDS
3. Pneumothorax
4. Pneumomediastinum, Pneumopericardium and Subcutaneous Emphysema
5. Ventilator-Associated Pneumonia (VAP) and Invasive Pulmonary Aspergillosis (IPA)
6. Vascular Complications
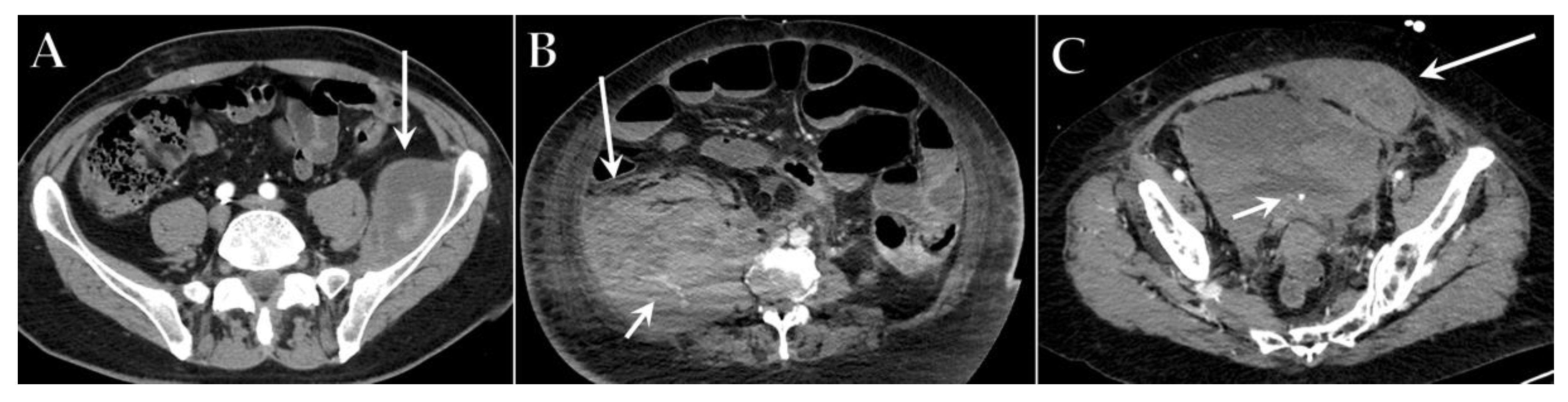
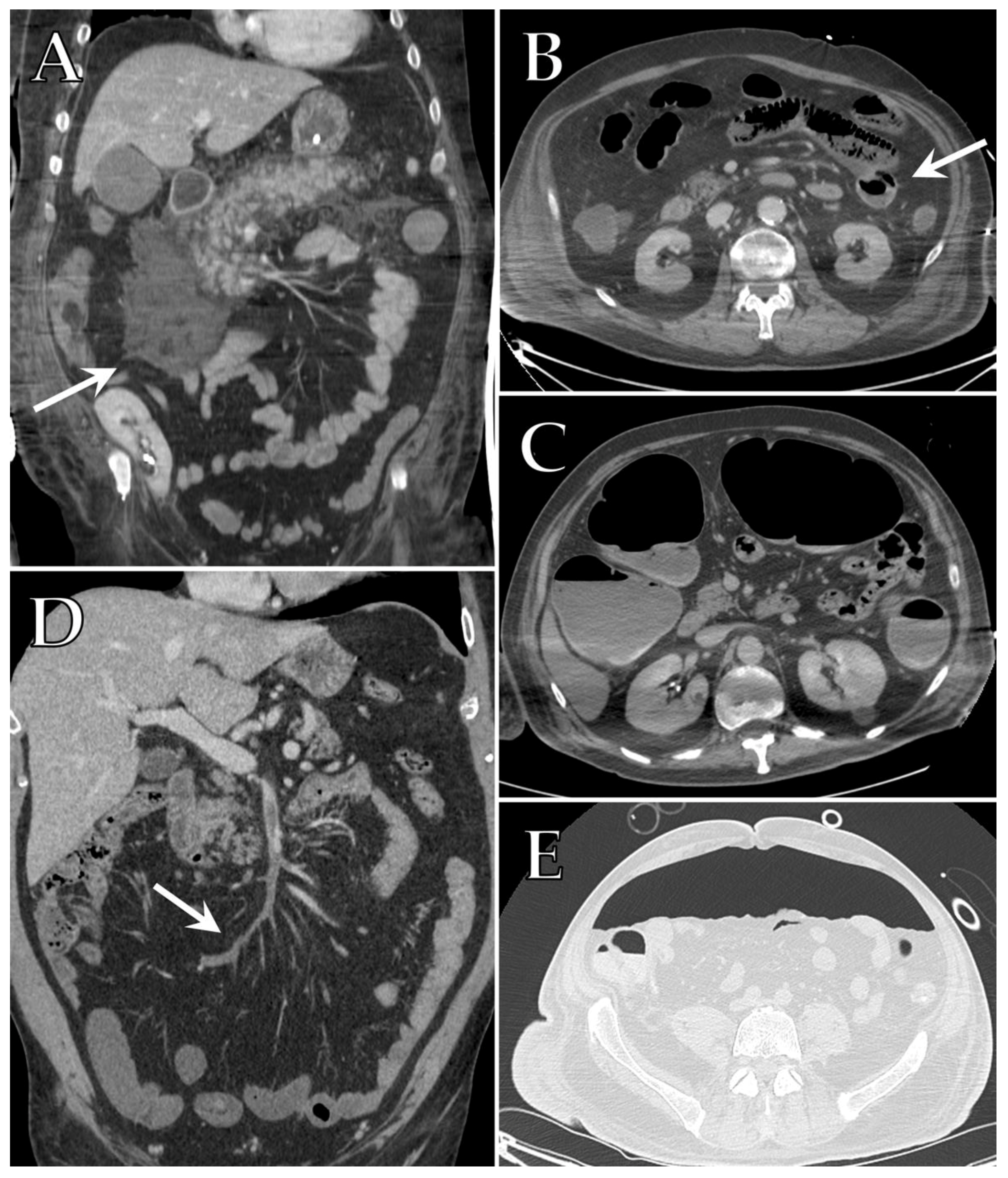
7. Gastrointestinal Complications
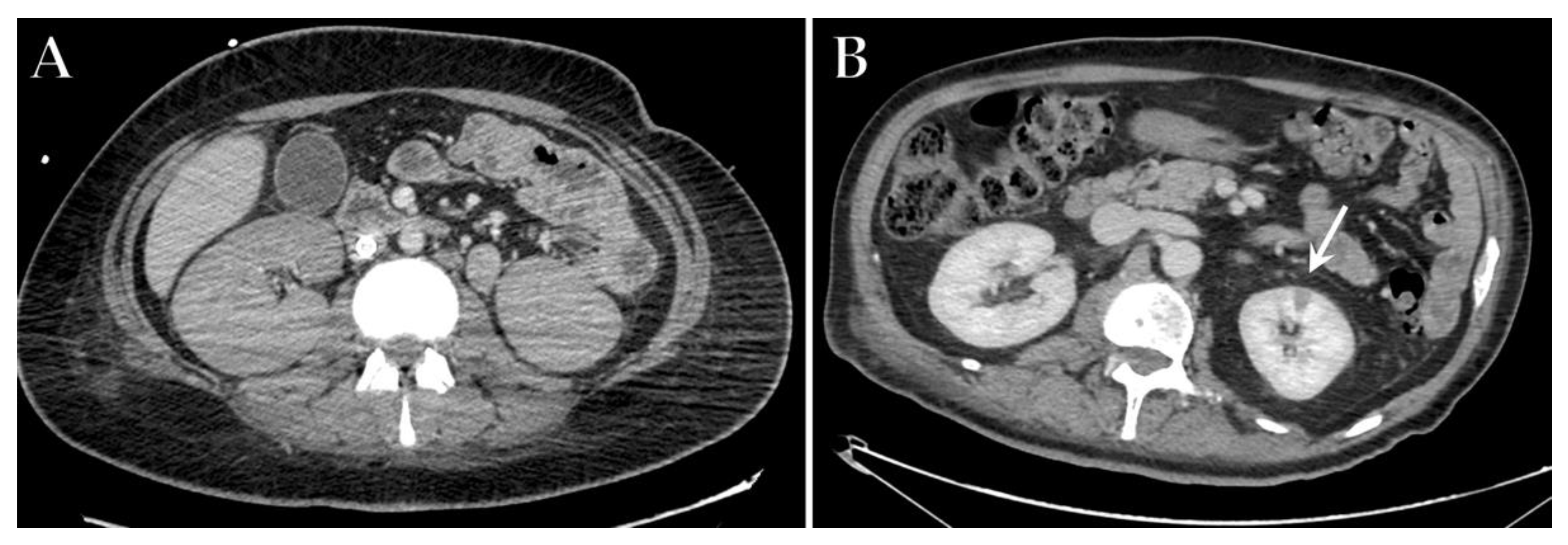
8. Renal Complications
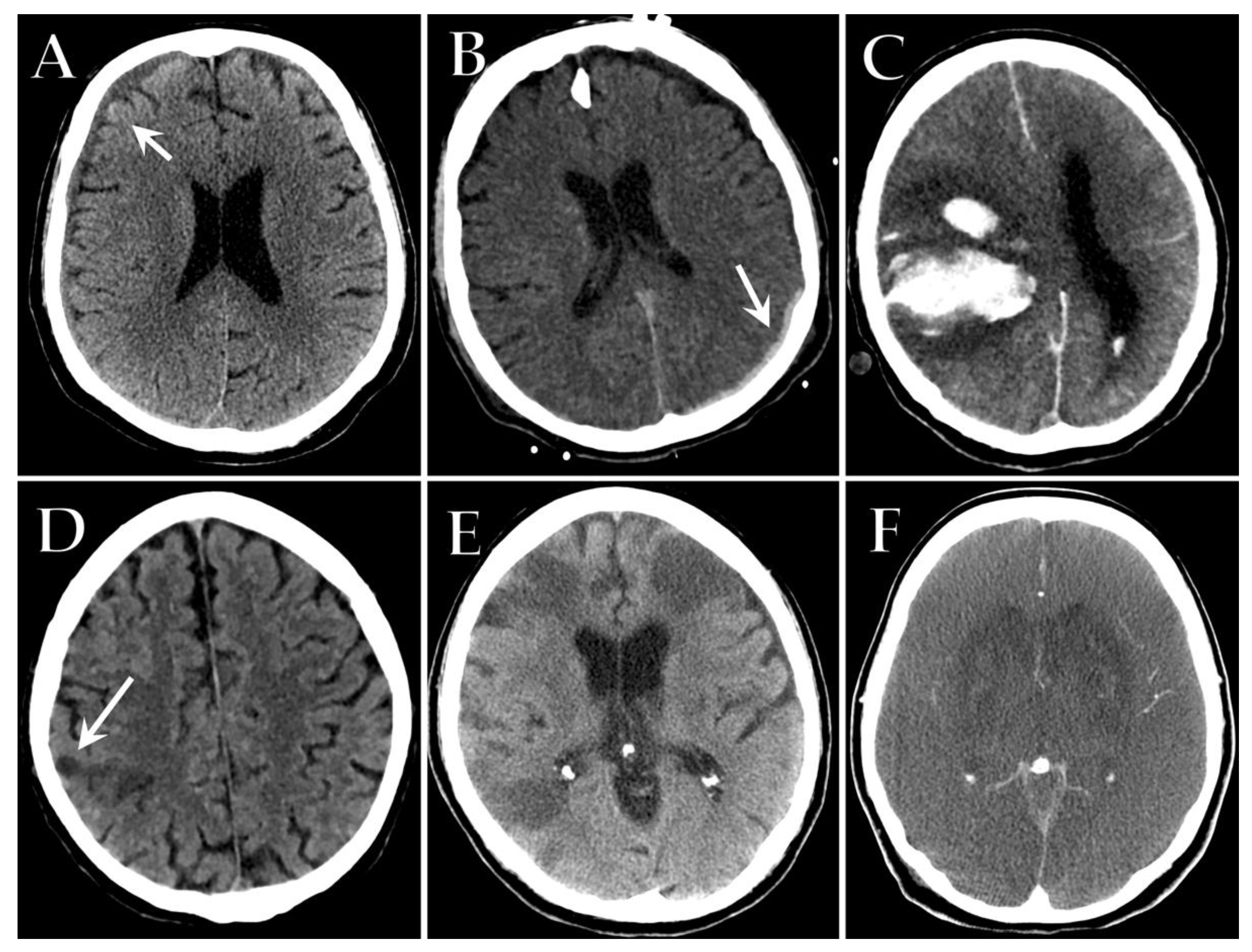
9. Neurological Complications
10. Sarcopenia
11. Current Limits of Imaging in Critically Ill COVID-19 Patients
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA—Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef]
- Balacchi, C.; Brandi, N.; Ciccarese, F.; Coppola, F.; Lucidi, V.; Bartalena, L.; Parmeggiani, A.; Paccapelo, A.; Golfieri, R. Comparing the first and the second waves of COVID-19 in Italy: Differences in epidemiological features and CT findings using a semi-quantitative score. Emerg. Radiol. 2021, 28, 1055–1067. [Google Scholar] [CrossRef] [PubMed]
- Ciccarese, F.; Coppola, F.; Spinelli, D.; Galletta, G.L.; Lucidi, V.; Paccapelo, A.; DE Benedittis, C.; Balacchi, C.; Golfieri, R. Diagnostic Accuracy of North America Expert Consensus Statement on Reporting CT Findings in Patients Suspected of Having COVID-19 Infection: An Italian Single-Center Experience. Radiol. Cardiothorac. Imaging 2020, 2, e200312. [Google Scholar] [CrossRef] [PubMed]
- Angeli, E.; Dalto, S.; Marchese, S.; Setti, L.; Bonacina, M.; Galli, F.; Rulli, E.; Torri, V.; Monti, C.; Meroni, R.; et al. Prognostic value of CT integrated with clinical and laboratory data during the first peak of the COVID-19 pandemic in Northern Italy: A nomogram to predict unfavorable outcome. Eur. J. Radiol. 2021, 137, 109612. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei, S.M.H.; Talari, H.; Moghaddas, F.; Rajebi, H. CT Features and Short-term Prognosis of COVID-19 Pneumonia: A Single-Center Study from Kashan, Iran. Radiol. Cardiothorac. Imaging 2020, 2, e200130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Bianco, G.; Di Pietro, S.; Mazzuca, E.; Imburgia, A.; Tarantino, L.; Accurso, G.; Benenati, V.; Vernuccio, F.; Bucolo, C.; Salomone, S.; et al. Multidisciplinary Approach to the Diagnosis and In-Hospital Management of COVID-19 Infection: A Narrative Review. Front. Pharmacol. 2020, 11, 572168. [Google Scholar] [CrossRef] [PubMed]
- Pezoulas, V.C.; Kourou, K.D.; Papaloukas, C.; Triantafyllia, V.; Lampropoulou, V.; Siouti, E.; Papadaki, M.; Salagianni, M.; Koukaki, E.; Rovina, N.; et al. A Multimodal Approach for the Risk Prediction of Intensive Care and Mortality in Patients with COVID-19. Diagnostics 2021, 12, 56. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481, Erratum in Lancet Respir. Med. 2020, 8, e26. [Google Scholar] [CrossRef] [Green Version]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.-C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with (COVID-19). Clin. Infect. Dis. 2020, 27, ciaa478. [Google Scholar] [CrossRef] [PubMed]
- Bai, C.; Chotirmall, S.H.; Rello, J.; Alba, G.A.; Ginns, L.C.; Krishnan, J.A.; Rogers, R.; Bendstrup, E.; Burgel, P.-R.; Chalmers, J.D.; et al. Updated guidance on the management of COVID-19: From an American Thoracic Society/European Respiratory Society coordinated International Task Force (29 July 2020). Eur. Respir. Rev. 2020, 29, 200287. [Google Scholar] [CrossRef]
- Wang, I.E.; Cooper, G.; Mousa, S.A. Diagnostic Approaches for COVID-19 and Its Associated Complications. Diagnostics 2021, 11, 2071. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Falaschi, Z.; Paschè, A.; Danna, P.; Arioli, R.; Arru, C.D.; Zagaria, D.; Tricca, S.; Suri, J.S.; Karla, M.K.; et al. Computed tomography findings of COVID-19 pneumonia in Intensive Care Unit-patients. J. Public Health Res. 2021, 10, 2270. [Google Scholar] [CrossRef]
- Franco, C.; Facciolongo, N.; Tonelli, R.; Dongilli, R.; Vianello, A.; Pisani, L.; Scala, R.; Malerba, M.; Carlucci, A.; Negri, E.A.; et al. Feasibility and clinical impact of out-of-ICU noninvasive respiratory support in patients with COVID-19-related pneumonia. Eur. Respir. J. 2020, 56, 2002130. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, S.R.; Condella, A. Emergency Department Management of Severe Hypoxemic Respiratory Failure in Adults with COVID-19. J. Emerg. Med. 2021, 60, 729–742. [Google Scholar] [CrossRef]
- Cornejo, R.A.; Díaz, J.C.; Tobar, E.; Bruhn, A.; Ramos, C.A.; González, R.A.; Repetto, C.A.; Romero, C.M.; Gálvez, L.R.; Llanos, O.; et al. Effects of Prone Positioning on Lung Protection in Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2013, 188, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Busana, M.; Giosa, L.; Macrì, M.M.; Quintel, M. Prone Positioning in Acute Respiratory Distress Syndrome. Semin. Respir. Crit. Care Med. 2019, 40, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaramuzzo, G.; Gamberini, L.; Tonetti, T.; Zani, G.; Ottaviani, I.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Reggiani, M.L.B.; Bertellini, E.; et al. Sustained oxygenation improvement after first prone positioning is associated with liberation from mechanical ventilation and mortality in critically ill COVID-19 patients: A cohort study. Ann. Intensiv. Care 2021, 11, 63. [Google Scholar] [CrossRef]
- Pan, C.; Chen, L.; Lu, C.; Zhang, W.; Xia, J.-A.; Sklar, M.C.; Du, B.; Brochard, L.; Qiu, H. Lung Recruitability in COVID-19–associated Acute Respiratory Distress Syndrome: A Single-Center Observational Study. Am. J. Respir. Crit. Care Med. 2020, 201, 1294–1297. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensiv. Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Bonnesen, B.; Jensen, J.-U.S.; Jeschke, K.N.; Mathioudakis, A.G.; Corlateanu, A.; Hansen, E.F.; Weinreich, U.M.; Hilberg, O.; Sivapalan, P. Management of COVID-19-Associated Acute Respiratory Failure with Alternatives to Invasive Mechanical Ventilation: High-Flow Oxygen, Continuous Positive Airway Pressure, and Noninvasive Ventilation. Diagnostics 2021, 11, 2259. [Google Scholar] [CrossRef]
- Gresser, E.; Rueckel, J.; Puhr-Westerheide, D.; Schwarze, V.; Fink, N.; Kunz, W.G.; Wassilowsky, D.; Irlbeck, M.; Ricke, J.; Ingrisch, M.; et al. Prognostic Value of Admission Chest CT Findings for Invasive Ventilation Therapy in COVID-19 Pneumonia. Diagnostics 2020, 10, 1108. [Google Scholar] [CrossRef] [PubMed]
- Rola, P.; Farkas, J.; Spiegel, R.; Kyle-Sidell, C.; Weingart, S.; Duggan, L.; Garrone, M.; Thomas, A. Rethinking the early intubation paradigm of COVID-19: Time to change gears? Clin. Exp. Emerg. Med. 2020, 7, 78–80. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, G.; Zhan, C.; Rosenberg, N.; Azour, L.; Wickstrom, M.; Mason, D.M.; Thomas, K.M.; Moore, W.H. Increased Incidence of Barotrauma in Patients with COVID-19 on Invasive Mechanical Ventilation. Radiology 2020, 297, E252–E262. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581, Erratum in JAMA 2021, 325, 2120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ñamendys-Silva, S.A. ECMO for ARDS due to COVID-19. Heart Lung 2020, 49, 348–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.; Liang, M.; Ding, M.; Liu, W.; Ma, H.; Zhou, X.; Ren, H. Extracorporeal Membrane Oxygenation (ECMO) in Critically Ill Patients with Coronavirus Disease 2019 (COVID-19) Pneumonia and Acute Respiratory Distress Syndrome (ARDS). Med. Sci. Monit. 2020, 26, e925364. [Google Scholar] [CrossRef] [PubMed]
- Douraghi-Zadeh, D.; Logaraj, A.; Lazoura, O.; Downey, K.; Gill, S.; Finney, S.J.; Padley, S. Extracorporeal membrane oxygenation (ECMO): Radiographic appearances, complications and imaging artefacts for radiologists. J. Med. Imaging Radiat. Oncol. 2021, 65, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Gabelloni, M.; Faggioni, L.; Cioni, D.; Mendola, V.; Falaschi, Z.; Coppola, S.; Corradi, F.; Isirdi, A.; Brandi, N.; Coppola, F.; et al. Extracorporeal membrane oxygenation (ECMO) in COVID-19 patients: A pocket guide for radiologists. Radiol. Med. 2022, 13, 1–14. [Google Scholar] [CrossRef]
- Zheng, M.-H.; Feng, G.; Liu, W.; Targher, G.; Byrne, C.D.; Zheng, M. Extrapulmonary complications of COVID-19: A multisystem disease? J. Med. Virol. 2021, 93, 323–335. [Google Scholar] [CrossRef]
- Belletti, A.; Todaro, G.; Valsecchi, G.; Losiggio, R.; Palumbo, D.; Landoni, G.; Zangrillo, A. Barotrauma in Coronavirus Disease 2019 Patients Undergoing Invasive Mechanical Ventilation: A Systematic Literature Review. Crit. Care Med. 2022, 50, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Papi, C.; Spagni, G.; Alexandre, A.; Calabresi, P.; Della Marca, G.; Broccolini, A. Unprotected stroke management in an undiagnosed case of Severe Acute Respiratory Syndrome Coronavirus 2 infection. J. Stroke Cerebrovasc. Dis. 2020, 29, 104981. [Google Scholar] [CrossRef] [PubMed]
- ARDS Definition of Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Arrivé, F.; Coudroy, R.; Thille, A.W. Early Identification and Diagnostic Approach in Acute Respiratory Distress Syndrome (ARDS). Diagnostics 2021, 11, 2307. [Google Scholar] [CrossRef]
- Wong, K.T.; Antonio, G.E.; Hui, D.; Lee, N.; Yuen, E.H.Y.; Wu, A.; Leung, C.B.; Rainer, T.; Cameron, P.; Chung, S.S.C.; et al. Severe Acute Respiratory Syndrome: Radiographic Appearances and Pattern of Progression in 138 Patients. Radiology 2003, 228, 401–406. [Google Scholar] [CrossRef]
- Valente, T.; Lassandro, F.; Marino, M.; Squillante, F.; Aliperta, M.; Muto, R. H1N1 pneumonia: Our experience in 50 patients with a severe clinical course of novel swine-origin influenza A (H1N1) virus (S-OIV). Radiol. Med. 2012, 117, 165–184. [Google Scholar] [CrossRef]
- Franquet, T.; Jeong, Y.J.; Lam, H.Y.S.; Wong, H.Y.F.; Chang, Y.-C.; Chung, M.J.; Lee, K.S. Imaging findings in coronavirus infections: SARS-CoV, MERS-CoV, and SARS-CoV-2. Br. J. Radiol. 2020, 93, 20200515. [Google Scholar] [CrossRef] [PubMed]
- Sheard, S.; Rao, P.; Devaraj, A. Imaging of Acute Respiratory Distress Syndrome. Respir. Care 2012, 57, 607–612. [Google Scholar] [CrossRef] [Green Version]
- Gosangi, B.; Rubinowitz, A.N.; Irugu, D.; Gange, C.; Bader, A.; Cortopassi, I. COVID-19 ARDS: A review of imaging features and overview of mechanical ventilation and its complications. Emerg. Radiol. 2022, 29, 23–34, Erratum in Emerg. Radiol. 2022, 29, 225. [Google Scholar] [CrossRef]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef]
- Gattinoni, L.; Coppola, S.; Cressoni, M.; Busana, M.; Rossi, S.; Chiumello, D. COVID-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 201, 1299–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: Is it “typical” ARDS? Crit. Care 2020, 24, 198. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Gandet, F.F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Goldberg, M.F.; Goldberg, M.F. Neuroradiologic manifestations of COVID-19: What the emergency radiologist needs to know. Emerg. Radiol. 2020, 27, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Bhayana, R.; Som, A.; Li, M.D.; Carey, D.E.; Anderson, M.A.; Blake, M.A.; Catalano, O.; Gee, M.S.; Hahn, P.F.; Harisinghani, M.; et al. Abdominal Imaging Findings in COVID-19: Preliminary Observations. Radiology 2020, 297, E207–E215. [Google Scholar] [CrossRef] [PubMed]
- Gamberini, L.; Tonetti, T.; Spadaro, S.; Zani, G.; Mazzoli, C.A.; Capozzi, C.; Giampalma, E.; Reggiani, M.L.B.; Bertellini, E.; Castelli, A.; et al. Factors influencing liberation from mechanical ventilation in coronavirus disease 2019: Multicenter observational study in fifteen Italian ICUs. J. Intensiv. Care 2020, 8, 80, Erratum in J. Intensiv. Care 2020, 8, 96. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943, Erratum in JAMA Intern. Med. 2020, 180, 1031. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Li, J.; Liu, H.; Han, N.; Ju, J.; Kou, Y.; Chen, L.; Jiang, M.; Pan, F.; Zheng, Y.; et al. Long-term bone and lung consequences associated with hospital-acquired severe acute respiratory syndrome: A 15-year follow-up from a prospective cohort study. Bone Res. 2020, 8, 8, Erratum in Bone Res. 2020, 8, 34. [Google Scholar] [CrossRef] [Green Version]
- Das, K.M.; Lee, E.Y.; Singh, R.; Enani, M.A.; Al Dossari, K.; Van Gorkom, K.; Larsson, S.G.; Langer, R.D. Follow-up chest radiographic findings in patients with MERS-CoV after recovery. Indian J. Radiol. Imaging 2017, 27, 342–349. [Google Scholar] [CrossRef]
- Mineo, G.; Ciccarese, F.; Modolon, C.; Landini, M.P.; Valentino, M.; Zompatori, M. Post-ARDS pulmonary fibrosis in patients with H1N1 pneumonia: Role of follow-up CT. La Radiol. Med. 2011, 117, 185–200. [Google Scholar] [CrossRef]
- Urciuoli, L.; Guerriero, E. Chest CT Findings after 4 Months from the Onset of COVID-19 Pneumonia: A Case Series. Diagnostics 2020, 10, 899. [Google Scholar] [CrossRef]
- González, J.; Benítez, I.D.; Carmona, P.; Santisteve, S.; Monge, A.; Moncusí-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratalá, A.; Zuil, M.; et al. Pulmonary Function and Radiologic Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021, 160, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Garfield, J.M. One-year Multidisciplinary Follow-Up of COVID-19 Patients Requiring Invasive Mechanical Ventilation. J. Cardiothorac. Vasc. Anesthesia 2021, 36, 1354–1363. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, D.B.; Sedhai, Y.R.; Budhathoki, P.; Adhikari, A.; Pokharel, N.; Dhakal, R.; Kafle, S.; Mir, W.A.Y.; Acharya, R.; Kashiouris, M.G.; et al. Pulmonary barotrauma in COVID-19: A systematic review and meta-analysis. Ann. Med. Surg. 2022, 73, 103221. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.K.; Alkandari, B.M.; Mohammed, W.; Tobar, A.M.; Abdelmohsen, M.A. Ventilator associated lung injury in severe COVID-19 pneumonia patients—Case Reports: Ventilator associated lung injury in COVID-19. Eur. J. Radiol. Open 2020, 8, 100310. [Google Scholar] [CrossRef] [PubMed]
- Udwadia, Z.F.; Toraskar, K.K.; Pinto, L.; Mullerpatan, J.; Wagh, H.D.; Mascarenhas, J.M.; Gandhi, B.M.; Tripathi, A.; Sunavala, A.; Agrawal, U.; et al. Increased frequency of pneumothorax and pneumomediastinum in COVID-19 patients admitted in the ICU: A multicentre study from Mumbai, India. Clin. Med. 2021, 21, e615–e619. [Google Scholar] [CrossRef]
- Chopra, A.; Al-Tarbsheh, A.H.; Shah, N.J.; Yaqoob, H.; Hu, K.; Feustel, P.J.; Ortiz-Pacheco, R.; Patel, K.M.; Oweis, J.; Kozlova, N.; et al. Pneumothorax in critically ill patients with COVID-19 infection: Incidence, clinical characteristics and outcomes in a case control multicenter study. Respir. Med. 2021, 184, 106464. [Google Scholar] [CrossRef]
- Protti, A.; Greco, M.; Filippini, M.; Vilardo, A.M.; Langer, T.; Villa, M.; Frutos-Vivar, F.; Santini, A.; Caruso, P.F.; Spano, S.; et al. Barotrauma in mechanically ventilated patients with Coronavirus disease 2019: A survey of 38 hospitals in Lombardy, Italy. Minerva Anestesiol. 2021, 87, 193–198. [Google Scholar] [CrossRef]
- Wang, X.H.; Duan, J.; Han, X.; Liu, X.; Zhou, J.; Wang, X.; Zhu, L.; Mou, H.; Guo, S. High incidence and mortality of pneumothorax in critically Ill patients with COVID-19. Heart Lung 2021, 50, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Alhumaid, S.; Al Mutair, A.; Alghazal, H.A.; Alhaddad, A.J.; Al-Helal, H.; Al Salman, S.A.; Alali, J.; Almahmoud, S.; Alhejy, Z.M.; Albagshi, A.A.; et al. Extracorporeal membrane oxygenation support for SARS-CoV-2: A multi-centered, prospective, observational study in critically ill 92 patients in Saudi Arabia. Eur. J. Med. Res. 2021, 26, 141. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, A.W.; Ingle, T.; Newman, J.; Nadeem, I.; Jackson, K.; Lane, N.D.; Melhorn, J.; Davies, H.E.; Rostron, A.J.; Adeni, A.; et al. COVID-19 and pneumothorax: A multicentre retrospective case series. Eur. Respir. J. 2020, 56, 2002697. [Google Scholar] [CrossRef] [PubMed]
- Zantah, M.; Castillo, E.D.; Townsend, R.; Dikengil, F.; Criner, G.J. Pneumothorax in COVID-19 disease- incidence and clinical characteristics. Respir. Res. 2020, 21, 236. [Google Scholar] [CrossRef] [PubMed]
- Kohli, A.; Hande, P.C.; Chugh, S. Role of chest radiography in the management of COVID-19 pneumonia: An overview and correlation with pathophysiologic changes. Indian J. Radiol. Imaging 2021, 31 (Suppl. 1), S70–S79. [Google Scholar] [CrossRef] [PubMed]
- Ziter, F.M., Jr.; Westcott, J.L. Supine subpulmonary pneumothorax. Am. J. Roentgenol. 1981, 137, 699–701. [Google Scholar] [CrossRef] [Green Version]
- Akdogan, R.E.; Mohammed, T.; Syeda, A.; Jiwa, N.; Ibrahim, O.; Mutneja, R. Pneumothorax in Mechanically Ventilated Patients with COVID-19 Infection. Case Rep. Crit. Care 2021, 2021, 6657533. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, D.; Zangrillo, A.; Belletti, A.; Guazzarotti, G.; Calvi, M.R.; Guzzo, F.; Pennella, R.; Monti, G.; Gritti, C.; Marmiere, M.; et al. A radiological predictor for pneumomediastinum/pneumothorax in COVID-19 ARDS patients. J. Crit. Care 2021, 66, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; Fraccaro, A.; Landini, N.; Zanardi, G.; Catino, C.; Savoia, F.; Malacchini, N.; Zeraj, F.; Peditto, P.; Catalanotti, V.; et al. Pneumothorax and/or Pneumomediastinum Worsens the Prognosis of COVID-19 Patients with Severe Acute Respiratory Failure: A Multicenter Retrospective Case-Control Study in the North-East of Italy. J. Clin. Med. 2021, 10, 4835. [Google Scholar] [CrossRef] [PubMed]
- Gahona, C.C.T.; Raj, K.; Bhandari, K.; Nuguru, S.; Bukhari, A. Subcutaneous Emphysema in Patients With COVID-19 Infection: A Report of Three Cases. Cureus 2020, 12, e10559. [Google Scholar] [CrossRef]
- Scacciavillani, R.; Iannaccone, G.; Del Buono, M.G.; Bello, G. Pneumopericardium following mechanical ventilation in COVID-19 pneumonia. Eur. Heart J.-Case Rep. 2020, 4, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Belletti, A.; Palumbo, D.; Zangrillo, A.; Fominskiy, E.V.; Franchini, S.; Dell’Acqua, A.; Marinosci, A.; Monti, G.; Vitali, G.; Colombo, S.; et al. Predictors of Pneumothorax/Pneumomediastinum in Mechanically Ventilated COVID-19 Patients. J. Cardiothorac. Vasc. Anesth. 2021, 35, 3642–3651. [Google Scholar] [CrossRef] [PubMed]
- Lemmers, D.H.; Abu Hilal, M.; Bnà, C.; Prezioso, C.; Cavallo, E.; Nencini, N.; Crisci, S.; Fusina, F.; Natalini, G. Pneumomediastinum and subcutaneous emphysema in COVID-19: Barotrauma or lung frailty? ERJ Open Res. 2020, 6, 00385–02020. [Google Scholar] [CrossRef] [PubMed]
- Bejvan, S.M.; Godwin, J.D. Pneumomediastinum: Old signs and new signs. AJR Am. J. Roentgenol. 1996, 166, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Zylak, C.M.; Standen, J.R.; Barnes, G.R.; Zylak, C.J. Pneumomediastinum Revisited. RadioGraphics 2000, 20, 1043–1057, Erratum in Radiographics 2001, 21, 1616. [Google Scholar] [CrossRef] [PubMed]
- Kouritas, V.K.; Papagiannopoulos, K.; Lazaridis, G.; Baka, S.; Mpoukovinas, I.; Karavasilis, V.; Lampaki, S.; Kioumis, I.; Pitsiou, G.; Papaiwannou, A.; et al. Pneumomediastinum. J. Thorac. Dis. 2015, 7 (Suppl. 1), S44–S49. [Google Scholar] [CrossRef] [PubMed]
- Rouyer, M.; Strazzulla, A.; Youbong, T.; Tarteret, P.; Pitsch, A.; de Pontfarcy, A.; Cassard, B.; Vignier, N.; Pourcine, F.; Jochmans, S.; et al. Ventilator-Associated Pneumonia in COVID-19 Patients: A Retrospective Cohort Study. Antibiotics 2021, 10, 988. [Google Scholar] [CrossRef]
- Wicky, P.-H.; Niedermann, M.S.; Timsit, J.-F. Ventilator-associated pneumonia in the era of COVID-19 pandemic: How common and what is the impact? Crit. Care 2021, 25, 153. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Higginson, E.; Pereira-Dias, J.; Curran, M.D.; Parmar, S.; Khokhar, F.; Cuchet-Lourenço, D.; Lux, J.; Sharma-Hajela, S.; Ravenhill, B.; et al. Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit. Care 2021, 25, 25, Erratum in Crit. Care 2021, 25, 130. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Razazi, K.; Arrestier, R.; Haudebourg, A.F.; Benelli, B.; Carteaux, G.; Decousser, J.-W.; Fourati, S.; Woerther, P.L.; Schlemmer, F.; Charles-Nelson, A.; et al. Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit. Care 2020, 24, 699, Erratum in Crit. Care 2021, 25, 118. [Google Scholar] [CrossRef]
- Blonz, G.; Kouatchet, A.; Chudeau, N.; Pontis, E.; Lorber, J.; Lemeur, A.; Planche, L.; Lascarrou, J.-B.; Colin, G. Epidemiology and microbiology of ventilator-associated pneumonia in COVID-19 patients: A multicenter retrospective study in 188 patients in an un-inundated French region. Crit. Care 2021, 25, 72. [Google Scholar] [CrossRef] [PubMed]
- Moretti, M.; Van Laethem, J.; Minini, A.; Pierard, D.; Malbrain, M.L. Ventilator-associated bacterial pneumonia in coronavirus 2019 disease, a retrospective monocentric cohort study. J. Infect. Chemother. 2021, 27, 826–833. [Google Scholar] [CrossRef]
- Póvoa, H.C.C.; Chianca, G.C.; Iorio, N.L.P.P. COVID-19: An Alert to Ventilator-Associated Bacterial Pneumonia. Infect. Dis. Ther. 2020, 9, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Marchiori, E.; Nobre, L.F.; Hochhegger, B.; Zanetti, G. Pulmonary cavitation in patients with COVID-19. Clin. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of Invasive Pulmonary Aspergillosis Among Intubated Patients With COVID-19: A Prospective Study. Clin. Infect. Dis. 2020, 73, e3606–e3614. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef]
- Song, G.; Liang, G.; Liu, W. Fungal Co-infections Associated with Global COVID-19 Pandemic: A Clinical and Diagnostic Perspective from China. Mycopathologia 2020, 185, 599–606. [Google Scholar] [CrossRef]
- Patti, R.K.; Dalsania, N.R.; Somal, N.; Sinha, A.; Mehta, S.; Ghitan, M.; Seneviratne, C.; Kupfer, Y. Subacute Aspergillosis “Fungal Balls” Complicating COVID-19. J. Investig. Med. High Impact Case Rep. 2020, 8. Erratum in J. Investig. Med. High Impact Case Rep. 2021, 25, 118. [Google Scholar] [CrossRef]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.-M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A Clinical Algorithm to Diagnose Invasive Pulmonary Aspergillosis in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64, Erratum in Am. J. Respir. Crit. Care Med. 2012, 186, 808. [Google Scholar] [CrossRef] [Green Version]
- Jenks, J.D.; Nam, H.H.; Hoenigl, M. Invasive aspergillosis in critically ill patients: Review of definitions and diagnostic approaches. Mycoses 2021, 64, 1002–1014. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Tandon, A.; Bhatt, S.; Aggarwal, A.; Dagar, S.; Bansal, H. COVID19 pneumonia with cavitation and cystic lung changes: Multi-detector computed tomography spectrum of a gamut of etiologies. BJR Open 2021, 3, 20210007. [Google Scholar] [CrossRef] [PubMed]
- Zoumot, Z.; Bonilla, M.-F.; Wahla, A.S.; Shafiq, I.; Uzbeck, M.; El-Lababidi, R.M.; Hamed, F.; Abuzakouk, M.; ElKaissi, M. Pulmonary cavitation: An under-recognized late complication of severe COVID-19 lung disease. BMC Pulm. Med. 2021, 21, 24. [Google Scholar] [CrossRef]
- Brandi, N.; Bartalena, L.; Mosconi, C.; Golfieri, R. A unique case of miliary pulmonary tuberculosis induced by bacillus Calmette-Guérin intravesical instillation with COVID-19 superinfection. S. Afr. J. Radiol. 2021, 25, 3. [Google Scholar] [CrossRef]
- Amaral, L.T.W.; Beraldo, G.L.; Brito, V.M.; Rosa, M.E.E.; De Matos, M.J.R.; Fonseca, E.K.U.N.; Yokoo, P.; Silva, M.M.A.; Teles, G.B.D.S.; Shoji, H.; et al. Lung cavitation in COVID-19: Co-infection complication or rare evolution? Einstein 2020, 18, eAI5822. [Google Scholar] [CrossRef]
- Adams, H.J.; Kwee, T.C.; Yakar, D.; Hope, M.D.; Kwee, R.M. Chest CT Imaging Signature of Coronavirus Disease 2019 Infection: In Pursuit of the Scientific Evidence. Chest 2020, 158, 1885–1895. [Google Scholar] [CrossRef]
- Moll, M.; Zon, R.L.; Sylvester, K.W.; Chen, E.C.; Cheng, V.; Connell, N.; Fredenburgh, L.E.; Baron, R.M.; Cho, M.H.; Woolley, A.E.; et al. VTE in ICU Patients With COVID-19. Chest 2020, 158, 2130–2135. [Google Scholar] [CrossRef] [PubMed]
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier-Decrucq, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S.; et al. Pulmonary Embolism in Patients With COVID-19: Awareness of an Increased Prevalence. Circulation 2020, 142, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Mirsadraee, S.; Gorog, D.A.; Mahon, C.F.; Rawal, B.; Semple, T.R.; Nicol, E.D.; Arachchillage, D.R.J.; Devaraj, A.; Price, S.; Desai, S.R.; et al. Prevalence of Thrombotic Complications in ICU-Treated Patients with Coronavirus Disease 2019 Detected with Systematic CT Scanning. Crit. Care Med. 2021, 49, 804–815. [Google Scholar] [CrossRef]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.-P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef] [PubMed]
- Longhitano, Y.; Racca, F.; Zanza, C.; Piccioni, A.; Audo, A.; Muncinelli, M.; Santi, R.; Kozel, D.; Geraci, C.; Taverna, M.; et al. Venous thromboembolism in critically ill patients affected by ARDS related to COVID-19 in Northern-West Italy. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9154–9160. [Google Scholar] [CrossRef] [PubMed]
- Lamarche, Y.; Chow, B.; Bédard, A.; Johal, N.; Kaan, A.; Humphries, K.H.; Cheung, A. Thromboembolic events in patients on extracorporeal membrane oxygenation without anticoagulation. Innovations 2010, 5, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hajage, D.; Lebreton, G.; Monsel, A.; Voiriot, G.; Levy, D.; Baron, E.; Beurton, A.; Chommeloux, J.; Meng, P.; et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome associated with COVID-19: A retrospective cohort study. Lancet Respir. Med. 2020, 8, 1121–1131. [Google Scholar] [CrossRef]
- Gidaro, A.; Vailati, D.; Gemma, M.; Lugli, F.; Casella, F.; Cogliati, C.; Canelli, A.; Cremonesi, N.; Monolo, D.; Cordio, G.; et al. Retrospective survey from vascular access team Lombardy net in COVID-19 era. J. Vasc. Access 2021, 1129729821997252. [Google Scholar] [CrossRef] [PubMed]
- Lang, M.; Som, A.; Carey, D.; Reid, N.; Mendoza, D.P.; Flores, E.J.; Li, M.D.; Shepard, J.-A.O.; Little, B.P. Pulmonary Vascular Manifestations of COVID-19 Pneumonia. Radiol. Cardiothorac. Imaging 2020, 2, e200277. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.E.; Gong, A.J.; Gawande, R.S.; Fishman, E.K.; Vadvala, H.V. Vascular findings in CTA body and extremity of critically ill COVID-19 patients: Commonly encountered vascular complications with review of literature. Emerg. Radiol. 2022, 29, 263–279. [Google Scholar] [CrossRef] [PubMed]
- Faqihi, F.; Alharthy, A.; Balhamar, A.; Nasim, N.; AlAnezi, K.; Alaklobi, F.; Memish, Z.A.; Blaivas, M.; Alqahtani, S.A.; Karakitsos, D. A Retrospective Analysis of Thromboembolic Phenomena in Mechanically Ventilated Patients with COVID-19. Crit. Care Res. Pract. 2021, 2021, 8737580. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, D.; Guazzarotti, G.; De Cobelli, F. Spontaneous Major Hemorrhage in COVID-19 Patients: Another Brick in the Wall of SARS-CoV-2–Associated Coagulation Disorders? J. Vasc. Interv. Radiol. 2020, 31, 1494–1496. [Google Scholar] [CrossRef]
- Angileri, S.A.; Petrillo, M.; Di Meglio, L.; Arrichiello, A.; Rodà, G.M.; Ierardi, A.M.; Uberoi, R.; Carrafiello, G. Adverse Events in Coronavirus Disease Patients Management: A Pictorial Essay. J. Clin. Imaging Sci. 2020, 10, 42. [Google Scholar] [CrossRef]
- Bargellini, I.; Cervelli, R.; Lunardi, A.; Scandiffio, R.; Daviddi, F.; Giorgi, L.; Cicorelli, A.; Crocetti, L.; Cioni, R. Spontaneous Bleedings in COVID-19 Patients: An Emerging Complication. Cardiovasc. Interv. Radiol. 2020, 43, 1095–1096. [Google Scholar] [CrossRef] [PubMed]
- Abdelmohsen, M.A.; Alkandari, B.M.; Razek, A.A.K.A.; Tobar, A.M.; Gupta, V.K.; Elsebaie, N. Abdominal Computed Tomography Angiography and Venography in Evaluation of Hemorrhagic and Thrombotic lesions in Hospitalized COVID-19 patients. Clin. Imaging 2021, 79, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Revzin, M.V.; Raza, S.; Srivastava, N.C.; Warshawsky, R.; D’Agostino, C.; Malhotra, A.; Bader, A.S.; Patel, R.D.; Chen, K.; Kyriakakos, C.; et al. Multisystem Imaging Manifestations of COVID-19, Part 2: From Cardiac Complications to Pediatric Manifestations. RadioGraphics 2020, 40, 1866–1892. [Google Scholar] [CrossRef]
- Vaidya, T.; Nanivadekar, A.; Patel, R. Imaging spectrum of abdominal manifestations of COVID-19. World J. Radiol. 2021, 13, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, C.A.; Zapata, M.; Gómez, C.I.; Pino, L.F.; Herrera, M.A.; González-Hadad, A. Large intestinal perforation secondary to COVID-19: A case report. Int. J. Surg. Case Rep. 2021, 87, 106362. [Google Scholar] [CrossRef] [PubMed]
- Keshavarz, P.; Rafiee, F.; Kavandi, H.; Goudarzi, S.; Heidari, F.; Gholamrezanezhad, A. Ischemic gastrointestinal complications of COVID-19: A systematic review on imaging presentation. Clin. Imaging 2020, 73, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Kaafarani, H.M.A.; El Moheb, M.; Hwabejire, J.O.; Naar, L.; Christensen, M.A.; Breen, K.; Gaitanidis, A.; Alser, O.; Mashbari, H.; Bankhead-Kendall, B.; et al. Gastrointestinal Complications in Critically Ill Patients with COVID-19. Ann. Surg. 2020, 272, e61–e62. [Google Scholar] [CrossRef] [PubMed]
- El Moheb, M.; Naar, L.; Christensen, M.A.; Kapoen, C.; Maurer, L.R.; Farhat, M.; Kaafarani, H.M.A. Gastrointestinal Complications in Critically Ill Patients with and without COVID-19. JAMA 2020, 324, 1899–1901, Erratum in JAMA 2021, 325, 1113. [Google Scholar] [CrossRef]
- Serban, D.; Tribus, L.C.; Vancea, G.; Stoian, A.P.; Dascalu, A.M.; Suceveanu, A.I.; Tanasescu, C.; Costea, A.C.; Tudosie, M.S.; Tudor, C.; et al. Acute Mesenteric Ischemia in COVID-19 Patients. J. Clin. Med. 2021, 11, 200. [Google Scholar] [CrossRef] [PubMed]
- Caruso, D.; Zerunian, M.; Pucciarelli, F.; Lucertini, E.; Bracci, B.; Polidori, T.; Guido, G.; Polici, M.; Rucci, C.; Iannicelli, E.; et al. Imaging of abdominal complications of COVID-19 infection. BJR Open 2021, 3, 20200052. [Google Scholar] [CrossRef]
- Bozdag, A.; Eroglu, Y.; Tartar, A.S.; Bozdag, P.G.; Aglamis, S. Pancreatic Damage and Radiological Changes in Patients with COVID-19. Cureus 2021, 13, e14992. [Google Scholar] [CrossRef]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients With Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Kurihara, Y.; Maruhashi, T.; Wada, T.; Osada, M.; Oi, M.; Yamaoka, K.; Asari, Y. Pancreatitis in a Patient with Severe Coronavirus Disease Pneumonia Treated with Veno-venous Extracorporeal Membrane Oxygenation. Intern. Med. 2020, 59, 2903–2906. [Google Scholar] [CrossRef] [PubMed]
- Hadi, A.; Werge, M.; Kristiansen, K.T.; Pedersen, U.G.; Karstensen, J.G.; Novovic, S.; Gluud, L.L. Coronavirus Disease-19 (COVID-19) associated with severe acute pancreatitis: Case report on three family members. Pancreatology 2020, 20, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Kumaran, N.K.; Karmakar, B.K.; Taylor, O.M. Coronavirus disease-19 (COVID-19) associated with acute necrotising pancreatitis (ANP). BMJ Case Rep. 2020, 13, e237903. [Google Scholar] [CrossRef] [PubMed]
- Kataria, S.; Sharif, A.; Rehman, A.U.; Ahmed, Z.; Hanan, A. COVID-19 Induced Acute Pancreatitis: A Case Report and Literature Review. Cureus 2020, 12, e9169. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Reis, T.; Husain-Syed, F. Management of acute kidney injury in patients with COVID-19. Lancet Respir. Med. 2020, 8, 738–742. [Google Scholar] [CrossRef]
- Wang, P.; Tan, X.; Li, Q.; Qian, M.; Cheng, A.; Ma, B.; Zhang, X.; Guo, C.; Sheng, M.; Yi, M.; et al. Extra-pulmonary complications of 45 critically ill patients with COVID-19 in Yichang, Hubei province, China: A single-centered, retrospective, observation study. Medicine 2021, 100, e24604. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Liu, J.; Gao, Z.; Hu, F. Clinical Features and Outcomes of Acute Kidney Injury in Patients Infected with COVID-19 in Xiangyang, China. Blood Purif. 2021, 50, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Batlle, D.; Soler, M.J.; Sparks, M.A.; Hiremath, S.; South, A.M.; Welling, P.A.; Swaminathan, S. COVID-19 and ACE2 in Cardiovascular, Lung, and Kidney Working Group Acute Kidney Injury in COVID-19: Emerging Evidence of a Distinct Pathophysiology. J. Am. Soc. Nephrol. 2020, 31, 1380–1383. [Google Scholar] [CrossRef]
- Liu, Q.; Song, N.C.; Zheng, Z.K.; Li, J.S.; Li, S.K. Laboratory findings and a combined multifactorial approach to predict death in critically ill patients with COVID-19: A retrospective study. Epidemiol. Infect. 2020, 148, e129. [Google Scholar] [CrossRef]
- Ahmad, Z.; Goswami, S.; Paneerselvam, A.; Kabilan, K.; Choudhury, H.; Roy, A.; Guleria, R.; Soni, K.D.; Baruah, U.; Das, C.J. Imaging of Coronavirus Disease 2019 Infection From Head to Toe: A Primer for the Radiologist. Curr. Probl. Diagn. Radiol. 2021, 50, 842–855. [Google Scholar] [CrossRef] [PubMed]
- Akin, I.B.; Altay, C.; Kutsoylu, O.E.; Secil, M. Possible radiologic renal signs of COVID-19. Abdom. Radiol. 2021, 46, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Reis, T. Kidney involvement in COVID-19 and rationale for extracorporeal therapies. Nat. Rev. Nephrol. 2020, 16, 308–310. [Google Scholar] [CrossRef] [Green Version]
- Post, A.; den Deurwaarder, E.S.G.; Bakker, S.J.L.; de Haas, R.J.; van Meurs, M.; Gansevoort, R.T.; Berger, S.P. Kidney Infarction in Patients With COVID-19. Am. J. Kidney Dis. 2020, 76, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Yang, M.; Wan, C.; Yi, L.-X.; Tang, F.; Zhu, H.-Y.; Yi, F.; Yang, H.-C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Alves, V.D.P.V.; Altoé, A.; Veloso, V.; Ferreira, C.L.S.; Ventura, N.; Corrêa, D.G. Computed tomography features of cerebrovascular complications in intensive care unit patients with severe COVID-19. Radiol. Bras. 2021, 54, 283–288. [Google Scholar] [CrossRef]
- Sklinda, K.; Dorobek, M.; Wasilewski, P.G.; Dreżewski, K.; Dȩbicka, M.; Walecki, J.; Mruk, B. Radiological Manifestation of Neurological Complications in the Course of SARS-CoV-2 Infection. Front. Neurol. 2021, 12, 711026. [Google Scholar] [CrossRef]
- Choi, Y.; Lee, M.K. Neuroimaging findings of brain MRI and CT in patients with COVID-19: A systematic review and meta-analysis. Eur. J. Radiol. 2020, 133, 109393. [Google Scholar] [CrossRef]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Schenck, M.; Severac, F.; Clere-Jehl, R.; Studer, A.; Radosavljevic, M.; Kummerlen, C.; Monnier, A.; et al. Delirium and encephalopathy in severe COVID-19: A cohort analysis of ICU patients. Crit. Care 2020, 24, 491. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Gigli, G.L.; Bnà, C.; Morassi, M. Stroke in patients with COVID-19: Clinical and neuroimaging characteristics. Neurosci. Lett. 2020, 743, 135564. [Google Scholar] [CrossRef] [PubMed]
- Heman-Ackah, S.M.; Su, Y.S.; Spadola, M.; Petrov, D.; Chen, H.I.; Schuster, J.; Lucas, T. Neurologically Devastating Intraparenchymal Hemorrhage in COVID-19 Patients on Extracorporeal Membrane Oxygenation: A Case Series. Neurosurgery 2020, 87, E147–E151. [Google Scholar] [CrossRef]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Masur, J.; Freeman, C.; Mohan, S. A Double-Edged Sword: Neurologic Complications and Mortality in Extracorporeal Membrane Oxygenation Therapy for COVID-19–Related Severe Acute Respiratory Distress Syndrome at a Tertiary Care Center. Am. J. Neuroradiol. 2020, 41, 2009–2011. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.K.; Paliwal, V.K.; Malhotra, H.S.; Sharma, P.K. Neuroimaging Patterns in Patients with COVID-19-Associated Neurological Complications: A Review. Neurol. India 2021, 69, 260–271. [Google Scholar] [CrossRef]
- Rapalino, O.; Pourvaziri, A.; Maher, M.; Jaramillo-Cardoso, A.; Edlow, B.; Conklin, J.; Huang, S.; Westover, B.; Romero, J.; Halpern, E.; et al. Clinical, Imaging, and Lab Correlates of Severe COVID-19 Leukoencephalopathy. Am. J. Neuroradiol. 2021, 42, 632–638. [Google Scholar] [CrossRef]
- Radmanesh, A.; Derman, A.; Lui, Y.W.; Raz, E.; Loh, J.P.; Hagiwara, M.; Borja, M.J.; Zan, E.; Fatterpekar, G.M. COVID-19—Associated Diffuse Leukoencephalopathy and Microhemorrhages. Radiology 2020, 297, E223–E227. [Google Scholar] [CrossRef]
- Soares, M.N.; Eggelbusch, M.; Naddaf, E.; Gerrits, K.H.L.; van der Schaaf, M.; van den Borst, B.; Wiersinga, W.J.; van Vugt, M.; Weijs, P.J.M.; Murray, A.J.; et al. Skeletal muscle alterations in patients with acute Covid-19 and post-acute sequelae of Covid-19. J. Cachex. Sarcopenia Muscle 2022, 13, 11–22. [Google Scholar] [CrossRef]
- Schiaffino, S.; Albano, D.; Cozzi, A.; Messina, C.; Arioli, R.; Bnà, C.; Bruno, A.; Carbonaro, L.A.; Carriero, A.; Carriero, S.; et al. CT-derived Chest Muscle Metrics for Outcome Prediction in Patients with COVID-19. Radiology 2021, 300, E328–E336. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Giannini, M.; Oulehri, W.; Riou, M.; Marcot, C.; Pizzimenti, M.; Debrut, L.; Charloux, A.; Geny, B.; Meyer, A. Long Term Follow-Up of Sarcopenia and Malnutrition after Hospitalization for COVID-19 in Conventional or Intensive Care Units. Nutrients 2022, 14, 912. [Google Scholar] [CrossRef] [PubMed]
- Welch, C.; Greig, C.; Masud, T.; Wilson, D.; Jackson, T.A. COVID-19 and Acute Sarcopenia. Aging Dis. 2020, 11, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Pironi, L.; Sasdelli, A.S.; Ravaioli, F.; Baracco, B.; Battaiola, C.; Bocedi, G.; Brodosi, L.; Leoni, L.; Mari, G.A.; Musio, A. Malnutrition and nutritional therapy in patients with SARS-CoV-2 disease. Clin. Nutr. 2020, 40, 1330–1337. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646, Erratum in Lancet 2019, 393, 2590. [Google Scholar] [CrossRef]
- Lee, K.; Shin, Y.; Huh, J.; Sung, Y.S.; Lee, I.-S.; Yoon, K.-H.; Kim, K.W. Recent Issues on Body Composition Imaging for Sarcopenia Evaluation. Korean J. Radiol. 2019, 20, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Giraudo, C.; Librizzi, G.; Fichera, G.; Motta, R.; Balestro, E.; Calabrese, F.; Carretta, G.; Cattelan, A.M.; Navalesi, P.; Pelloso, M.; et al. Reduced muscle mass as predictor of intensive care unit hospitalization in COVID-19 patients. PLoS ONE 2021, 16, e0253433. [Google Scholar] [CrossRef] [PubMed]
- Damanti, S.; Cristel, G.; Ramirez, G.A.; Bozzolo, E.P.; Da Prat, V.; Gobbi, A.; Centurioni, C.; Di Gaeta, E.; Del Prete, A.; Calabrò, M.G.; et al. Influence of reduced muscle mass and quality on ventilator weaning and complications during intensive care unit stay in COVID-19 patients. Clin. Nutr. 2021, in press. [CrossRef]
- Ng, M.-Y.; Lee, E.Y.; Yang, J.; Yang, F.; Li, X.; Wang, H.; Lui, M.M.-S.; Lo, C.S.-Y.; Leung, B.; Khong, P.-L.; et al. Imaging Profile of the COVID-19 Infection: Radiologic Findings and Literature Review. Radiol. Cardiothorac. Imaging 2020, 2, e200034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, D.; Jain, N.; Khanna, K.; Li, S.; Patel, L.; Gupta, N. Current role of imaging in COVID-19 infection with recent recommendations of point of care ultrasound in the contagion: A narrative review. Ann. Transl. Med. 2020, 8, 1094. [Google Scholar] [CrossRef] [PubMed]
- Frija, G.; Blažić, I.; Frush, D.P.; Hierath, M.; Kawooya, M.; Donoso-Bach, L.; Brkljačić, B. How to improve access to medical imaging in low- and middle-income countries? EClinicalMedicine 2021, 38, 101034. [Google Scholar] [CrossRef]
- Blažić, I.; Brkljačić, B.; Frija, G. The use of imaging in COVID-19—results of a global survey by the International Society of Radiology. Eur. Radiol. 2021, 31, 1185–1193. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brandi, N.; Ciccarese, F.; Rimondi, M.R.; Balacchi, C.; Modolon, C.; Sportoletti, C.; Renzulli, M.; Coppola, F.; Golfieri, R. An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review. Diagnostics 2022, 12, 846. https://doi.org/10.3390/diagnostics12040846
Brandi N, Ciccarese F, Rimondi MR, Balacchi C, Modolon C, Sportoletti C, Renzulli M, Coppola F, Golfieri R. An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review. Diagnostics. 2022; 12(4):846. https://doi.org/10.3390/diagnostics12040846
Chicago/Turabian StyleBrandi, Nicolò, Federica Ciccarese, Maria Rita Rimondi, Caterina Balacchi, Cecilia Modolon, Camilla Sportoletti, Matteo Renzulli, Francesca Coppola, and Rita Golfieri. 2022. "An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review" Diagnostics 12, no. 4: 846. https://doi.org/10.3390/diagnostics12040846