
Revisiting the Awareness and Understanding the Associations between Intracranial Tumors and Optic Neuropathy


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentations
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Case 4
2.5. Case 5
3. Discussion
3.1. Neuroophthalmologist Perspective
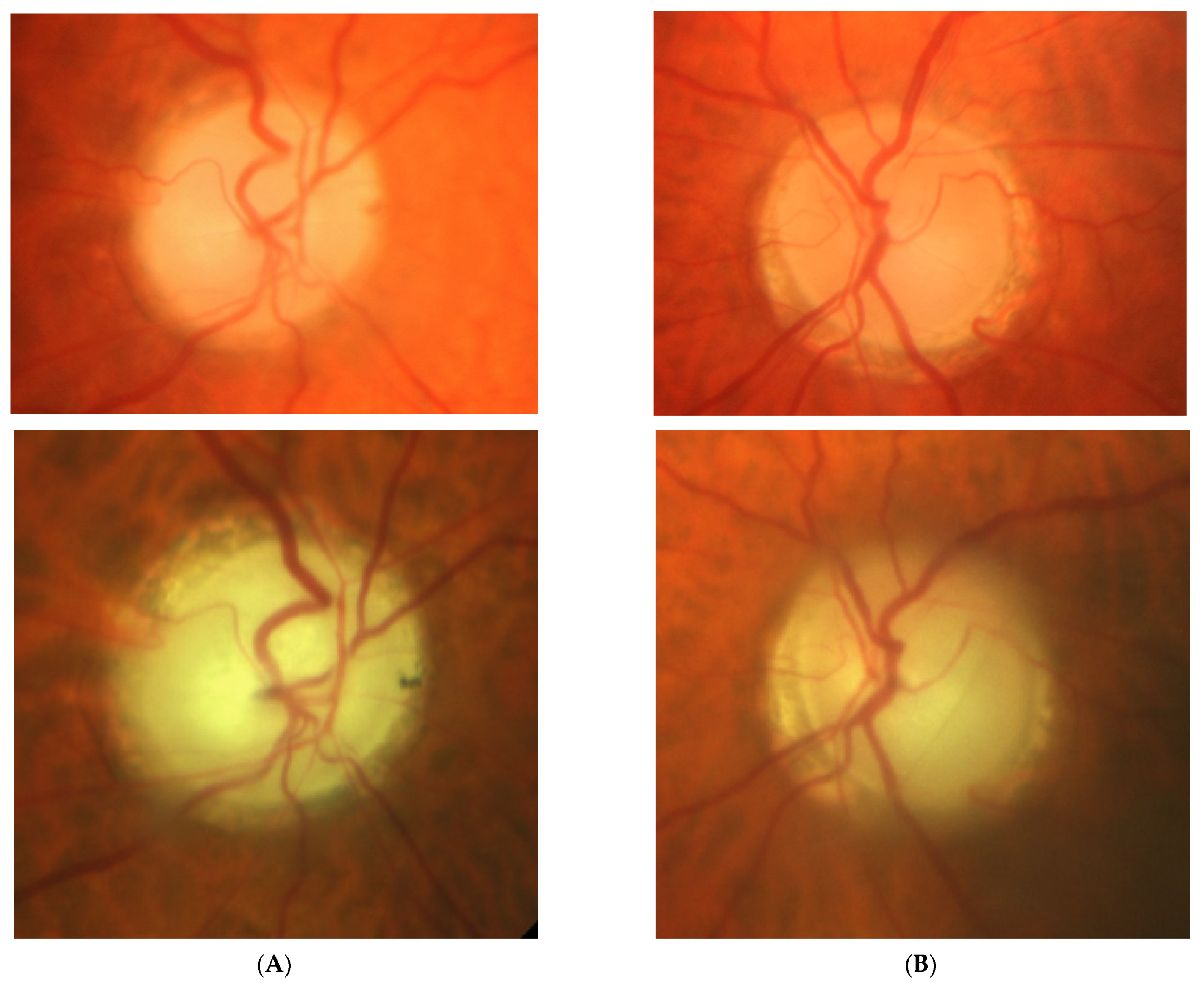
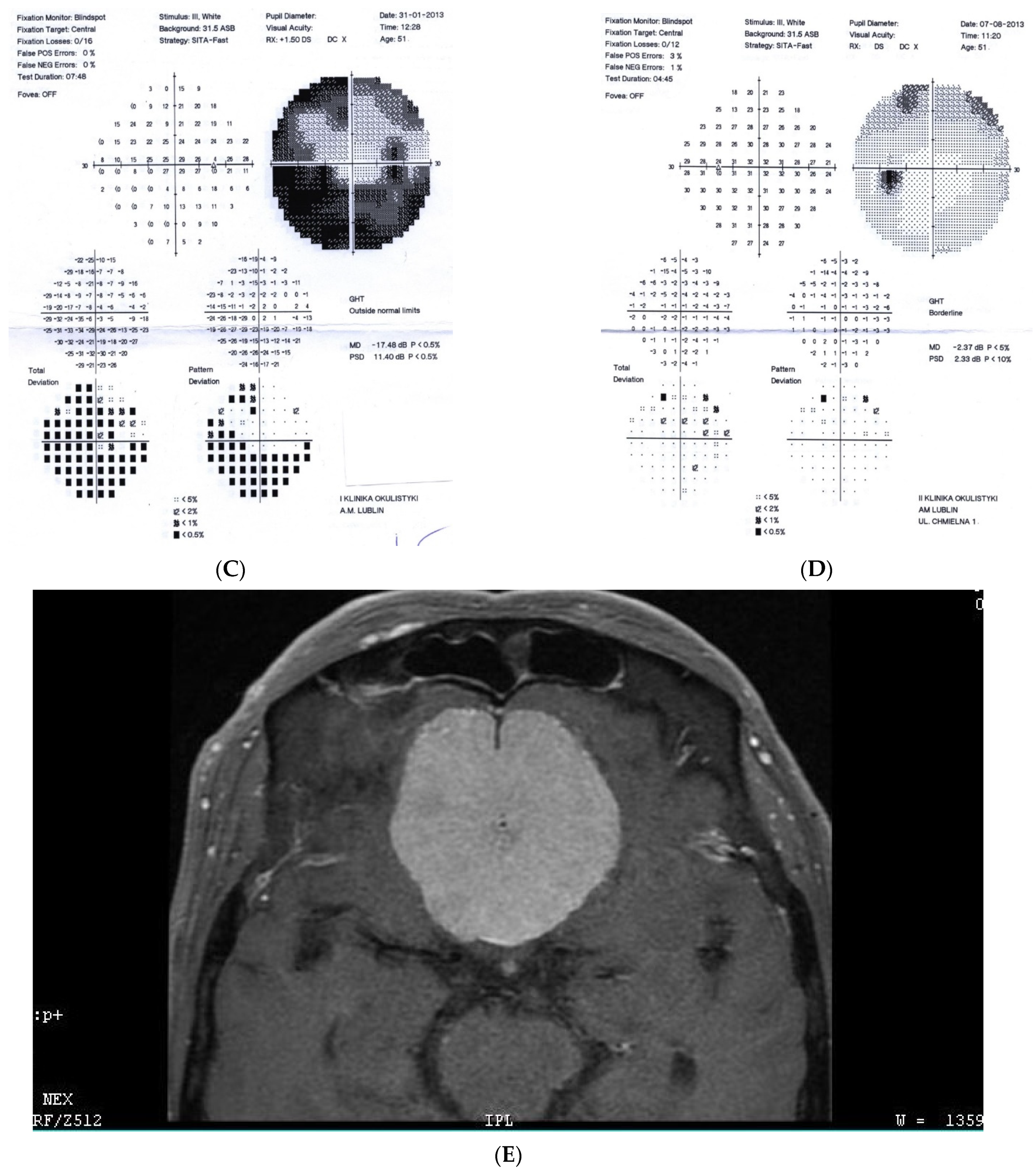
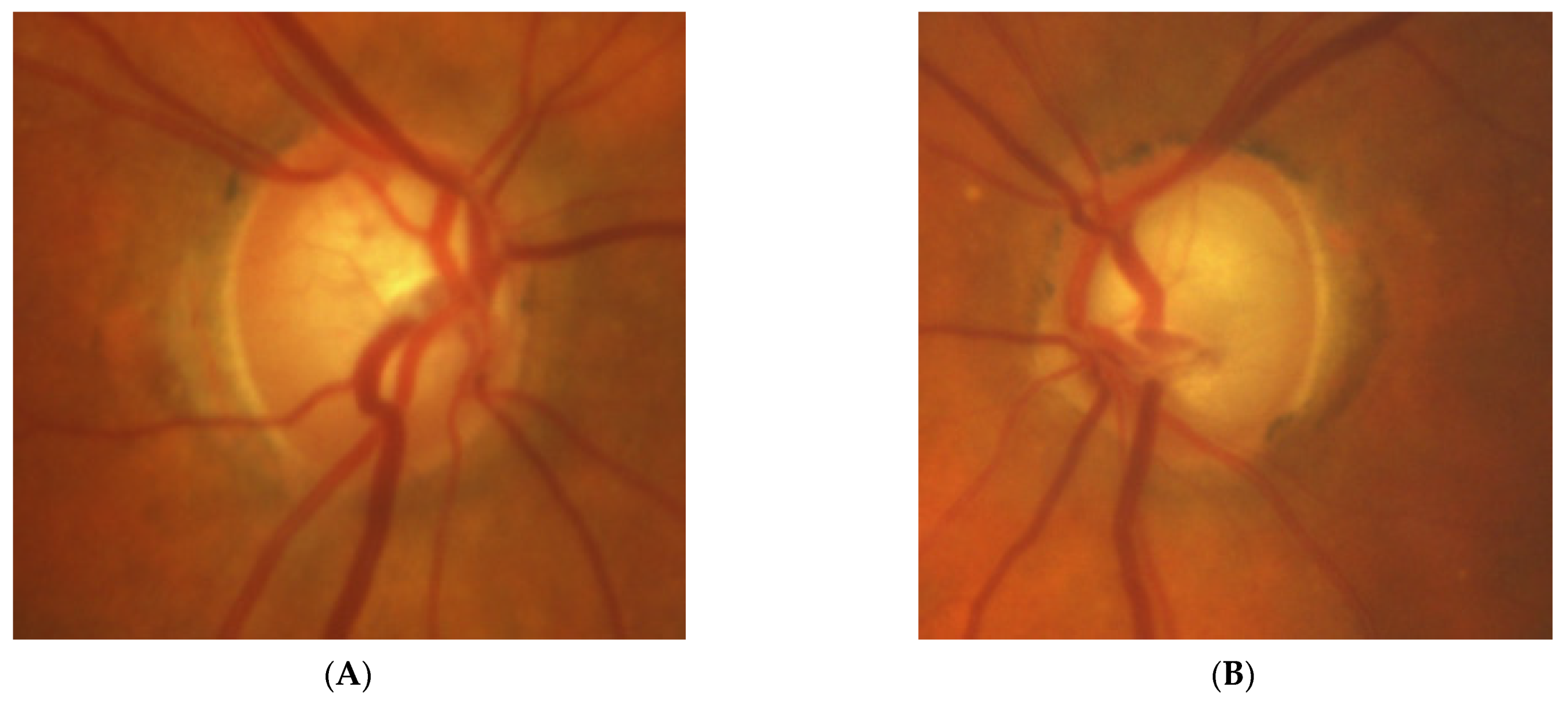
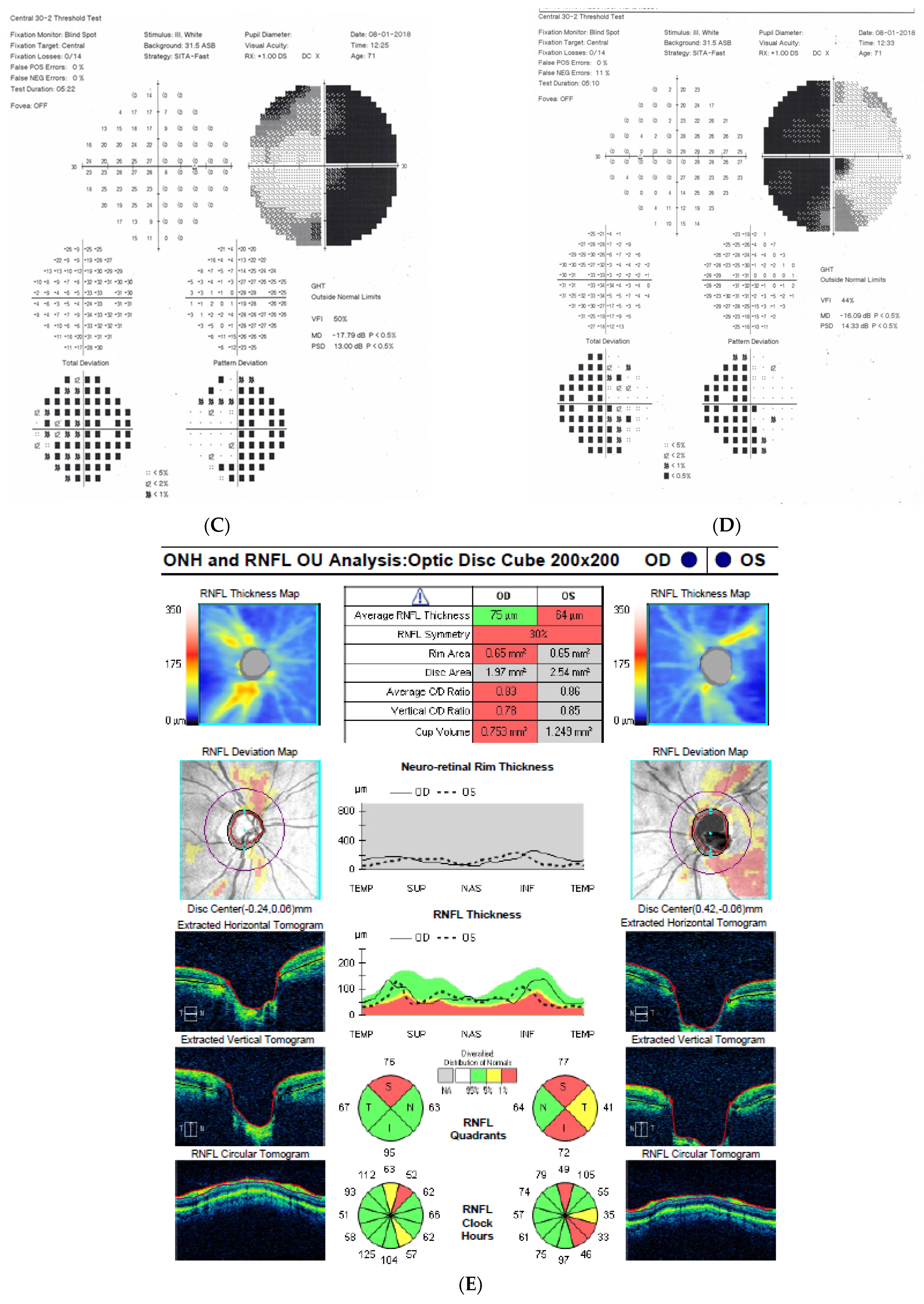
- Lesions developing in association with an optic nerve develop unilaterally and are characterized by optic disc pallor, VF defects, and OCT findings (their morphology may differ from classical glaucomatous defects).
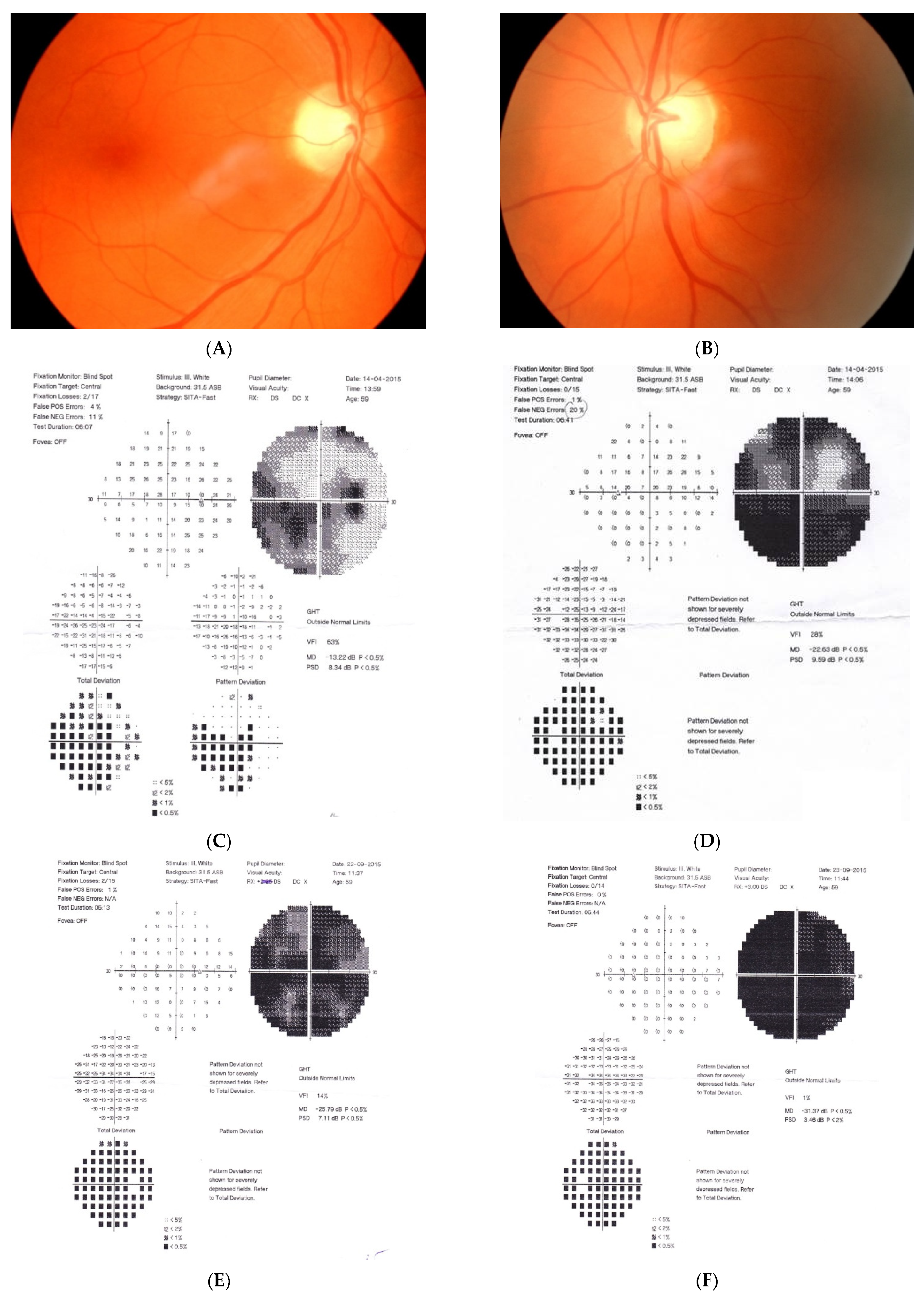
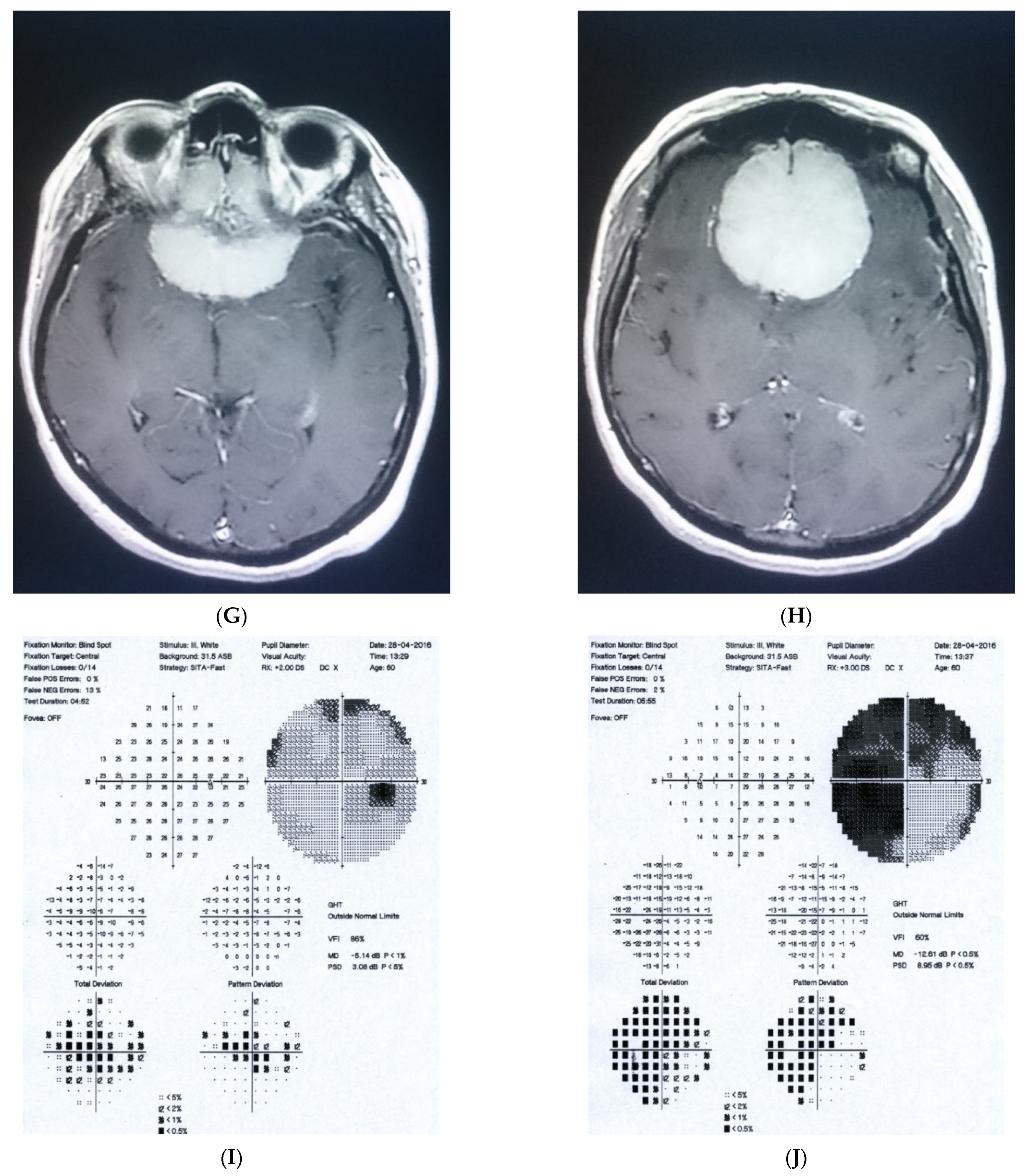
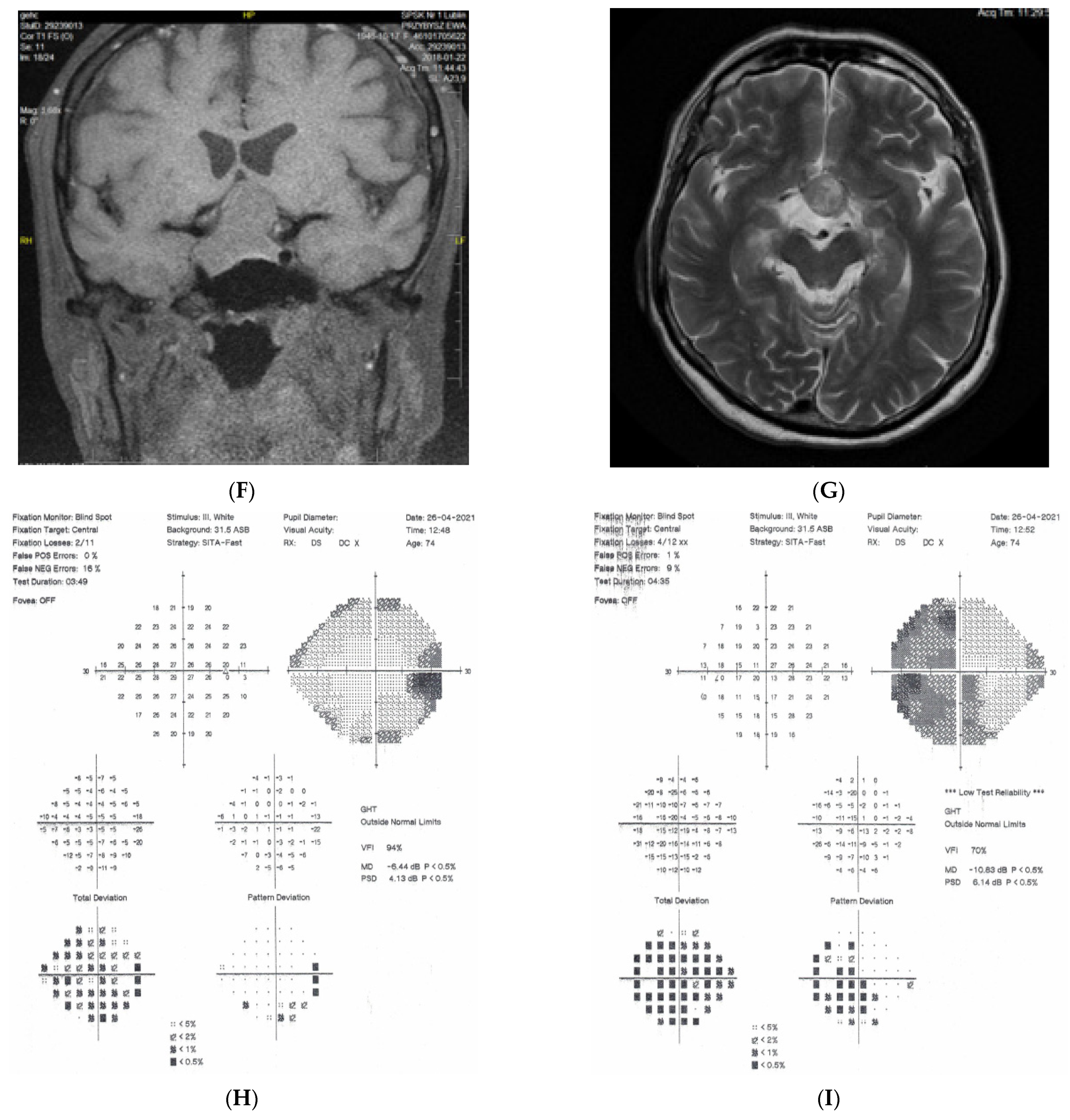
- Chiasmal lesions develop slowly and frequently, bilaterally but asymmetrically. MR scans usually suggest pituitary adenoma, craniopharyngioma, or olfactory groove meningioma of this region. In almost two thirds of the patients with chiasmal syndrome, this is due to pituitary macroadenomas [7]. Virtually all patients have asymmetrical bilateral visual field loss, majority decreased color vision, half decreased visual acuity, and only one-third optic disc pallor [8].
- It is noteworthy that retrotectal or even retrochiasmal lesions are unlikely to be misdiagnosed as causes of optic neuropathy. Intracranial lesions, if develop rapidly, may evoke intracranial hypertension that will usually be diagnosed promptly as, e.g., papilloedema. If not diagnosed, sooner or later the patient will be referred due to the consequences of raised intracranial pressure or malignancy itself. If the lesion develops slowly, the ophthalmic presentation will be a visual field defect, with respect to the vertical meridian, but pallor does not develop as the lesion is located distal to ganglion cells. In these typical situations when retrotectal areas of visual pathways are involved, a picture of the right or left homonymous hemianopia is present, with normal discs and pupillary reflexes. Such pictures develop in stroke, tumors, and trauma, etc.
3.2. Glaucomatologist Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sefi-Yurdakul, N. Visual findings as primary manifestations in patients with intracranial tumors. Int. J. Ophthalmol. 2015, 8, 800–803. [Google Scholar] [CrossRef] [PubMed]
- Pruett, R.C.; Wepsic, J.G. Delayed Diagnosis of Chiasmal Compression. Am. J. Ophthalmol. 1973, 76, 229–236. [Google Scholar] [CrossRef]
- Kosior-Jarecka, E.; Wróbel-Dudzińska, D.; Pietura, R.; Pankowska, A.; Szczuka, B.; Żarnowska, I.; Łukasik, U.; Żarnowski, T. Results of Neuroimaging in Patients with Atypical Normal-Tension Glaucoma. BioMed Res. Int. 2020, 2020, 9093206. [Google Scholar] [CrossRef]
- Choudhari, N.S.; Neog, A.; Fudnawala, V.; George, R. Cupped disc with normal intraocular pressure: The long road to avoid misdiagnosis. Indian J. Ophthalmol. 2011, 59, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.I.K.; Feldman, F.; Kucharczyk, W.; Trope, G.E. Neuroradiologic Screening in Normal-Pressure Glaucoma: Study Results and Literature Review. J. Glaucoma 2002, 11, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, D.S.; Siatkowski, R.; Glaser, J.S.; Schatz, N.J.; Parrish, R.K. The cupped disc: Who needs neuroimaging? Ophthalmology 1998, 105, 1866–1874. [Google Scholar] [CrossRef]
- Mejico, L.J.; Miller, N.R.; Dong, L.M. Clinical features associated with lesions other than pituitary adenoma in patients with an optic chiasmal syndrome. Am. J. Ophthalmol. 2004, 137, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Poon, A.; McNeill, P.; Harper, A.; O’Day, J. Patterns of visual loss associated with pituitary macroadenomas. Aust. N. Z. J. Ophthalmol. 1995, 23, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Kupersmith, M.J.; Krohn, D. Cupping of the optic disc with compressive lesions of the anterior visual pathway. Ann. Ophthalmol. 1984, 16, 948–953. [Google Scholar] [PubMed]











Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żarnowski, T.; Łukasik, U.; Żarnowska, I.; Kosior-Jarecka, E. Revisiting the Awareness and Understanding the Associations between Intracranial Tumors and Optic Neuropathy. Diagnostics 2021, 11, 2374. https://doi.org/10.3390/diagnostics11122374
Żarnowski T, Łukasik U, Żarnowska I, Kosior-Jarecka E. Revisiting the Awareness and Understanding the Associations between Intracranial Tumors and Optic Neuropathy. Diagnostics. 2021; 11(12):2374. https://doi.org/10.3390/diagnostics11122374
Chicago/Turabian StyleŻarnowski, Tomasz, Urszula Łukasik, Iwona Żarnowska, and Ewa Kosior-Jarecka. 2021. "Revisiting the Awareness and Understanding the Associations between Intracranial Tumors and Optic Neuropathy" Diagnostics 11, no. 12: 2374. https://doi.org/10.3390/diagnostics11122374