
Prognostic Value of Quantitative [18F]FDG-PET Features in Patients with Metastases from Soft Tissue Sarcoma

 , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Patient Characteristics
2.3. [18F]FDG-PET/CT
2.4. [18F]]FDG-PET Features
2.5. Statistical Analyses
3. Results
3.1. Patients and Follow-Up
3.2. Univariate Analysis
3.3. Multivariate Analysis
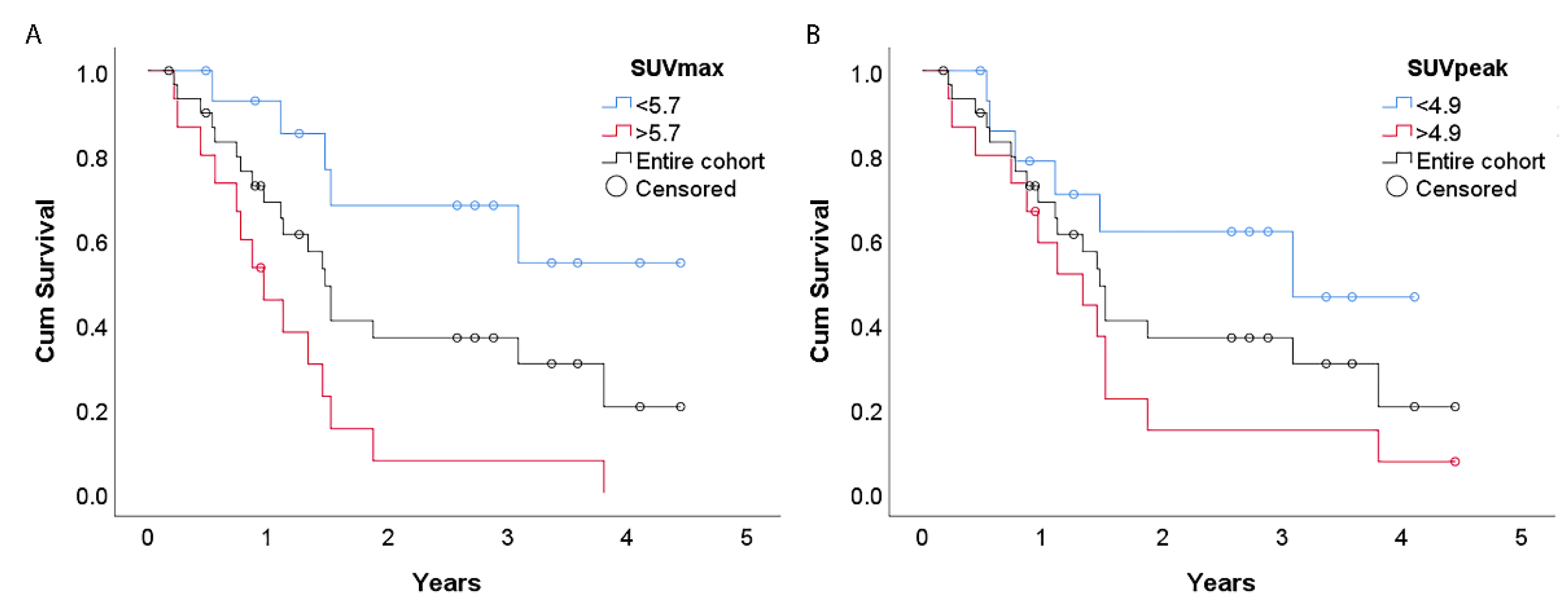
3.4. Survival Estimates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Literature Search

References
- Society, A.C. Cancer Facts & Figures 2017; American Cancer Society: Atlanta, GA, USA, 2017. [Google Scholar]
- Callegaro, D.; Miceli, R.; Bonvalot, S.; Ferguson, P.; Strauss, D.C.; Levy, A.; Griffin, A.; Hayes, A.J.; Stacchiotti, S.; Pechoux, C.L.; et al. Development and external validation of two nomograms to predict overall survival and occurrence of distant metastases in adults after surgical resection of localised soft-tissue sarcomas of the extremities: A retrospective analysis. Lancet Oncol. 2016, 17, 671–680. [Google Scholar] [CrossRef]
- Acem, I.; Verhoef, C.; Rueten-Budde, A.J.; Grunhagen, D.J.; van Houdt, W.J.; van de Sande, M.A.; Aston, W.; Bonenkamp, H.; Desar, I.M.; Ferguson, P.C.; et al. Age-related differences of oncological outcomes in primary extremity soft tissue sarcoma: A multistate model including 6260 patients. Eur. J. Cancer 2020, 141, 128–136. [Google Scholar] [CrossRef]
- Lochner, J.; Menge, F.; Vassos, N.; Hohenberger, P.; Kasper, B. Prognosis of Patients with Metastatic Soft Tissue Sarcoma: Advances in Recent Years. Oncol. Res. Treat. 2020, 43, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Mathoulin-Pelissier, S.; Cesne, A.L.; Terrier, P.; Bonvalot, S.; Collin, F.; Michels, J.J.; Blay, J.Y.; Coindre, J.M.; Bui, B. Trends in survival for patients with metastatic soft-tissue sarcoma. Cancer 2011, 117, 1049–1054. [Google Scholar] [CrossRef] [PubMed]
- Billingsley, K.G.; Lewis, J.J.; Leung, D.H.; Casper, E.S.; Woodruff, J.M.; Brennan, M.F. Multifactorial analysis of the survival of patients with distant metastasis arising from primary extremity sarcoma. Cancer 1999, 85, 389–395. [Google Scholar] [CrossRef]
- Gronchi, A.; Miah, A.B.; Dei Tos, A.P.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up ☆. Ann. Oncol. 2021, 32, 1348–1365. [Google Scholar] [CrossRef]
- Van Glabbeke, M.; van Oosterom, A.T.; Oosterhuis, J.W.; Mouridsen, H.; Crowther, D.; Somers, R.; Verweij, J.; Santoro, A.; Buesa, J.; Tursz, T. Prognostic factors for the outcome of chemotherapy in advanced soft tissue sarcoma: An analysis of 2,185 patients treated with anthracycline-containing first-line regimens—A European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group Study. J. Clin. Oncol. 1999, 17, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Rueten-Budde, A.J.; van Praag, V.M.; van de Sande, M.A.; Fiocco, M.; Group, P.S. External validation and adaptation of a dynamic prediction model for patients with high-grade extremity soft tissue sarcoma. J. Surg. Oncol. 2021, 123, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Rueten-Budde, A.J.; Van Praag, V.M.; Jeys, L.M.; Laitinen, M.K.; Pollock, R.; Aston, W.; van der Hage, J.A.; Dijkstra, P.S.; Ferguson, P.C.; Griffin, A.M.; et al. Dynamic prediction of overall survival for patients with high-grade extremity soft tissue sarcoma. Surg. Oncol. 2018, 27, 695–701. [Google Scholar] [CrossRef]
- Kalisvaart, G.M.; Bloem, J.L.; Bovee, J.; van de Sande, M.A.; Gelderblom, H.; van der Hage, J.A.; Hartgrink, H.H.; Krol, A.D.; de Geus-Oei, L.F.; Grootjans, W. Personalising sarcoma care using quantitative multimodality imaging for response assessment. Clin. Radiol. 2021, 76, 313.e1–313.e13. [Google Scholar] [CrossRef]
- Annovazzi, A.; Rea, S.; Zoccali, C.; Sciuto, R.; Baldi, J.; Anelli, V.; Petrongari, M.G.; Pescarmona, E.; Biagini, R.; Ferraresi, V. Diagnostic and Clinical Impact of 18F-FDG PET/CT in Staging and Restaging Soft-Tissue Sarcomas of the Extremities and Trunk: Mono-Institutional Retrospective Study of a Sarcoma Referral Center. J. Clin. Med. 2020, 9, 2549. [Google Scholar] [CrossRef] [PubMed]
- Vlenterie, M.; Oyen, W.J.; Steeghs, N.; Desar, I.M.; Verheijen, R.B.; Koenen, A.M.; Grootjans, W.; De Geus-Oei, L.F.; Van Erp, N.P.; Van Der Graaf, W.T. Early Metabolic Response as a Predictor of Treatment Outcome in Patients with Metastatic Soft Tissue Sarcomas. Anticancer Res. 2019, 39, 1309–1316. [Google Scholar] [CrossRef]
- Reyes Marles, R.H.; Navarro Fernandez, J.L.; Puertas Garcia-Sandoval, J.P.; Santonja Medina, F.; Mohamed Salem, L.; Frutos Esteban, L.; Contreras Gutierrez, J.F.; Castellon Sanchez, M.I.; Ruiz Merino, G.; Claver Valderas, M.A. Clinical value of baseline 18F-FDG PET/CT in soft tissue sarcomas. Eur. J. Hybrid Imaging 2021, 5, 16. [Google Scholar] [CrossRef]
- Chen, L.; Wu, X.; Ma, X.; Guo, L.; Zhu, C.; Li, Q. Prognostic value of 18F-FDG PET-CT-based functional parameters in patients with soft tissue sarcoma: A meta-analysis. Medicine 2017, 96, e5913. [Google Scholar] [CrossRef]
- De Geus-Oei, L.F.; Wiering, B.; Krabbe, P.F.; Ruers, T.J.; Punt, C.J.; Oyen, W.J. FDG-PET for prediction of survival of patients with metastatic colorectal carcinoma. Ann. Oncol. 2006, 17, 1650–1655. [Google Scholar] [CrossRef] [PubMed]
- Trojani, M.; Contesso, G.; Coindre, J.M.; Rouesse, J.; Bui, N.B.; de Mascarel, A.; Goussot, J.F.; David, M.; Bonichon, F.; Lagarde, C. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int. J. Cancer 1984, 33, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Frings, V.; van Velden, F.H.; Velasquez, L.M.; Hayes, W.; van de Ven, P.M.; Hoekstra, O.S.; Boellaard, R. Repeatability of metabolically active tumor volume measurements with FDG PET/CT in advanced gastrointestinal malignancies: A multicenter study. Radiology 2014, 273, 539–548. [Google Scholar] [CrossRef]
- Singh, T.P.; Sharma, A.; Sharma, A.; Bakhshi, S.; Patel, C.; Pandey, A.K.; Dhamija, E.; Batra, A.; Kumar, R. Utility of 18F-FDG-PET/CT in management and prognostication of treatment naive late-stage soft tissue sarcomas. Nucl. Med. Commun. 2021, 42, 818–825. [Google Scholar] [CrossRef]
- Fuglø, H.M.; Jørgensen, S.M.; Loft, A.; Hovgaard, D.; Petersen, M.M. The diagnostic and prognostic value of ¹⁸F-FDG PET/CT in the initial assessment of high-grade bone and soft tissue sarcoma. A retrospective study of 89 patients. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Heo, E.J.; Moon, S.H.; Lee, H.; Cheon, G.J.; Lee, M.; Kim, H.S.; Chung, H.H. Prognostic value of total lesion glycolysis on preoperative 18F-FDG PET/CT in patients with uterine carcinosarcoma. Eur. Radiol. 2016, 26, 4148–4154. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.J.; Lim, I.; Park, J.Y.; Jo, A.R.; Kong, C.B.; Song, W.S.; Jo, W.H.; Lee, S.Y.; Koh, J.S.; Kim, B.I.; et al. The Role of 18F-FDG PET/CT as a Prognostic Factor in Patients with Synovial Sarcoma. Nucl. Med. Mol. Imaging 2015, 49, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Lisle, J.W.; Eary, J.F.; O’Sullivan, J.; Conrad, E.U. Risk assessment based on FDG-PET imaging in patients with synovial sarcoma. Clin. Orthop. Relat. Res. 2009, 467, 1605–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, E.S.; Ha, S.G.; Kim, H.S.; Ha, J.H.; Paeng, J.C.; Han, I. Total lesion glycolysis by 18F-FDG PET/CT is a reliable predictor of prognosis in soft-tissue sarcoma. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1836–1842. [Google Scholar] [CrossRef] [PubMed]
- Baum, S.H.; Frühwald, M.; Rahbar, K.; Wessling, J.; Schober, O.; Weckesser, M. Contribution of PET/CT to prediction of outcome in children and young adults with rhabdomyosarcoma. J. Nucl. Med. 2011, 52, 1535–1540. [Google Scholar] [CrossRef] [Green Version]
- Satoh, Y.; Nambu, A.; Ichikawa, T.; Onishi, H. Whole-body total lesion glycolysis measured on fluorodeoxyglucose positron emission tomography/computed tomography as a prognostic variable in metastatic breast cancer. BMC Cancer 2014, 14, 525. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.; Bang, J.I.; Han, S.W.; Paeng, J.C.; Lee, K.H.; Kim, J.H.; Kang, G.H.; Jeong, S.Y.; Park, K.J.; Kim, T.Y. Total lesion glycolysis (TLG) as an imaging biomarker in metastatic colorectal cancer patients treated with regorafenib. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 757–764. [Google Scholar] [CrossRef]
- Macpherson, R.E.; Pratap, S.; Tyrrell, H.; Khonsari, M.; Wilson, S.; Gibbons, M.; Whitwell, D.; Giele, H.; Critchley, P.; Cogswell, L.; et al. Retrospective audit of 957 consecutive 18F-FDG PET-CT scans compared to CT and MRI in 493 patients with different histological subtypes of bone and soft tissue sarcoma. Clin. Sarcoma Res. 2018, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Charest, M.; Hickeson, M.; Lisbona, R.; Novales-Diaz, J.A.; Derbekyan, V.; Turcotte, R.E. FDG PET/CT imaging in primary osseous and soft tissue sarcomas: A retrospective review of 212 cases. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1944–1951. [Google Scholar] [CrossRef]
- Spinnato, P.; Kind, M.; Le Loarer, F.; Bianchi, G.; Colangeli, M.; Sambri, A.; Ponti, F.; van Langevelde, K.; Crombe, A. Soft Tissue Sarcomas: The Role of Quantitative MRI in Treatment Response Evaluation. Acad. Radiol. 2021. [Google Scholar] [CrossRef]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.; Brodowicz, T.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv268–iv269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chodyla, M.; Demircioglu, A.; Schaarschmidt, B.M.; Bertram, S.; Morawitz, J.; Bauer, S.; Podleska, L.; Rischpler, C.; Forsting, M.; Herrmann, K.; et al. Evaluation of the Predictive Potential of 18F-FDG PET and DWI Data Sets for Relevant Prognostic Parameters of Primary Soft-Tissue Sarcomas. Cancers 2021, 13, 2753. [Google Scholar] [CrossRef]
- Chodyla, M.; Demircioglu, A.; Schaarschmidt, B.M.; Bertram, S.; Bruckmann, N.M.; Haferkamp, J.; Li, Y.; Bauer, S.; Podleska, L.; Rischpler, C.; et al. Evaluation of 18F-FDG PET and DWI Datasets for Predicting Therapy Response of Soft-Tissue Sarcomas Under Neoadjuvant Isolated Limb Perfusion. J. Nucl. Med. 2021, 62, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Dangoor, A.; Seddon, B.; Gerrand, C.; Grimer, R.; Whelan, J.; Judson, I. UK guidelines for the management of soft tissue sarcomas. Clin. Sarcoma Res. 2016, 6, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics, n = 31 | |||
|---|---|---|---|
| Age | 59 ± 18 | Histologic subtype | |
| Sex | Undifferentiated soft tissue sarcoma | 8 (26%) | |
| Male | 20 (65%) | Myxofibrosarcoma | 6 (19%) |
| Female | 11 (35%) | MPNST | 5 (16%) |
| WHO performance status | Leiomyosarcoma | 3 (10%) | |
| Unknown | 8 (26%) | Dedifferentiated liposarcoma | 2 (6%) |
| 0 | 10 (32%) | Synovial sarcoma | 2 (6%) |
| 1 | 11 (35%) | Myxoid liposarcoma † | 1 (3%) |
| 2 | 2 (7%) | Round cell sarcoma | 1 (3%) |
| Location of primary tumour | Rhabdomyosarcoma | 1 (3%) | |
| Lower extremity | 18 (58%) | Angiosarcoma | 1 (3%) |
| Upper extremity | 3 (10%) | Intima sarcoma | 1 (3%) |
| Trunk wall | 3 (10%) | FNCLCC Grade * | |
| Deep trunk | 6 (19%) | 1 | 1 (3%) |
| Head/neck | 1 (3%) | 2 | 15 (48%) |
| Disease free interval | 3 | 14 (45%) | |
| Synchronous | 7 (23%) | Not applicable | 1 (3%) |
| <14 months | 12 (39%) | Location of metastases | |
| >14 months | 12 (39%) | Lung | 7 (23%) |
| Number of lesions | 3.3 ± 2.8 | Lung and other | 11(35%) |
| Sum of lesion diameters per patient (cm) | 7.5 (6.0–17.5) | Soft tissue only | 9 (29%) |
| Bone only | 4 (13%) | ||
| Variable | Overall Survival | p-value | |
|---|---|---|---|
| Clinical variables | Hazard ratio | 95% CI | |
| Age (years) | 1.02 | 0.99–1.04 | 0.2 |
| Grade (3 versus 2) | 1.26 | 0.50–3.21 | 0.6 |
| Location (Deep trunk or upper extr. versus other) | 0.91 | 0.34–2.40 | 0.8 |
| Number of lesions WHO performance status (≥1 versus 0) | 1.28 2.72 | 1.07–1.52 0.73–10.07 | 0.006 0.1 |
| Disease free interval | 0.2 | ||
| Synchronous versus >14 months | 3.36 | 0.94–12.0 | |
| <14 months versus >14 months | 1.44 | 0.47–4.47 | |
| PET features | |||
| SUVmax | 1.16 | 1.05–1.29 | 0.004 |
| SUVpeak | 1.20 | 1.05–1.37 | 0.006 |
| SUVmean | 1.23 | 0.99–1.54 | 0.07 |
| MTV | 1.001 | 0.999–1.003 | 0.2 |
| TLG | 1.001 | 1.000–1.001 | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalisvaart, G.M.; Grootjans, W.; Bovée, J.V.M.G.; Gelderblom, H.; van der Hage, J.A.; van de Sande, M.A.J.; van Velden, F.H.P.; Bloem, J.L.; de Geus-Oei, L.-F. Prognostic Value of Quantitative [18F]FDG-PET Features in Patients with Metastases from Soft Tissue Sarcoma. Diagnostics 2021, 11, 2271. https://doi.org/10.3390/diagnostics11122271
Kalisvaart GM, Grootjans W, Bovée JVMG, Gelderblom H, van der Hage JA, van de Sande MAJ, van Velden FHP, Bloem JL, de Geus-Oei L-F. Prognostic Value of Quantitative [18F]FDG-PET Features in Patients with Metastases from Soft Tissue Sarcoma. Diagnostics. 2021; 11(12):2271. https://doi.org/10.3390/diagnostics11122271
Chicago/Turabian StyleKalisvaart, Gijsbert M., Willem Grootjans, Judith V. M. G. Bovée, Hans Gelderblom, Jos A. van der Hage, Michiel A. J. van de Sande, Floris H. P. van Velden, Johan L. Bloem, and Lioe-Fee de Geus-Oei. 2021. "Prognostic Value of Quantitative [18F]FDG-PET Features in Patients with Metastases from Soft Tissue Sarcoma" Diagnostics 11, no. 12: 2271. https://doi.org/10.3390/diagnostics11122271