
Radiomics Analysis of Multi-Phase DCE-MRI in Predicting Tumor Response to Neoadjuvant Therapy in Breast Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. MR Examination
2.3. Assessment Response to Treatment
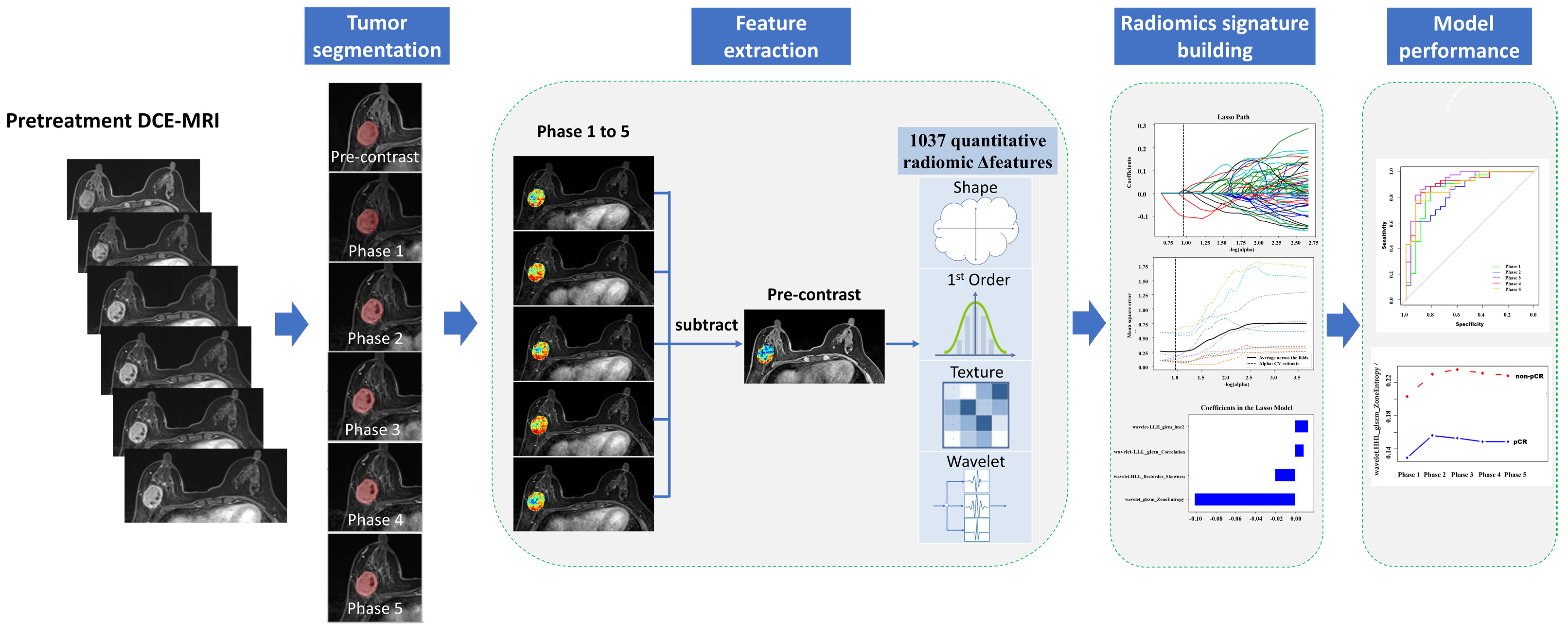
2.4. Radiomic Analysis
2.4.1. Tumor Segmentation
2.4.2. Feature Extraction
2.4.3. Feature Selection
2.4.4. Model Evaluation and Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Radiomics Signature Building
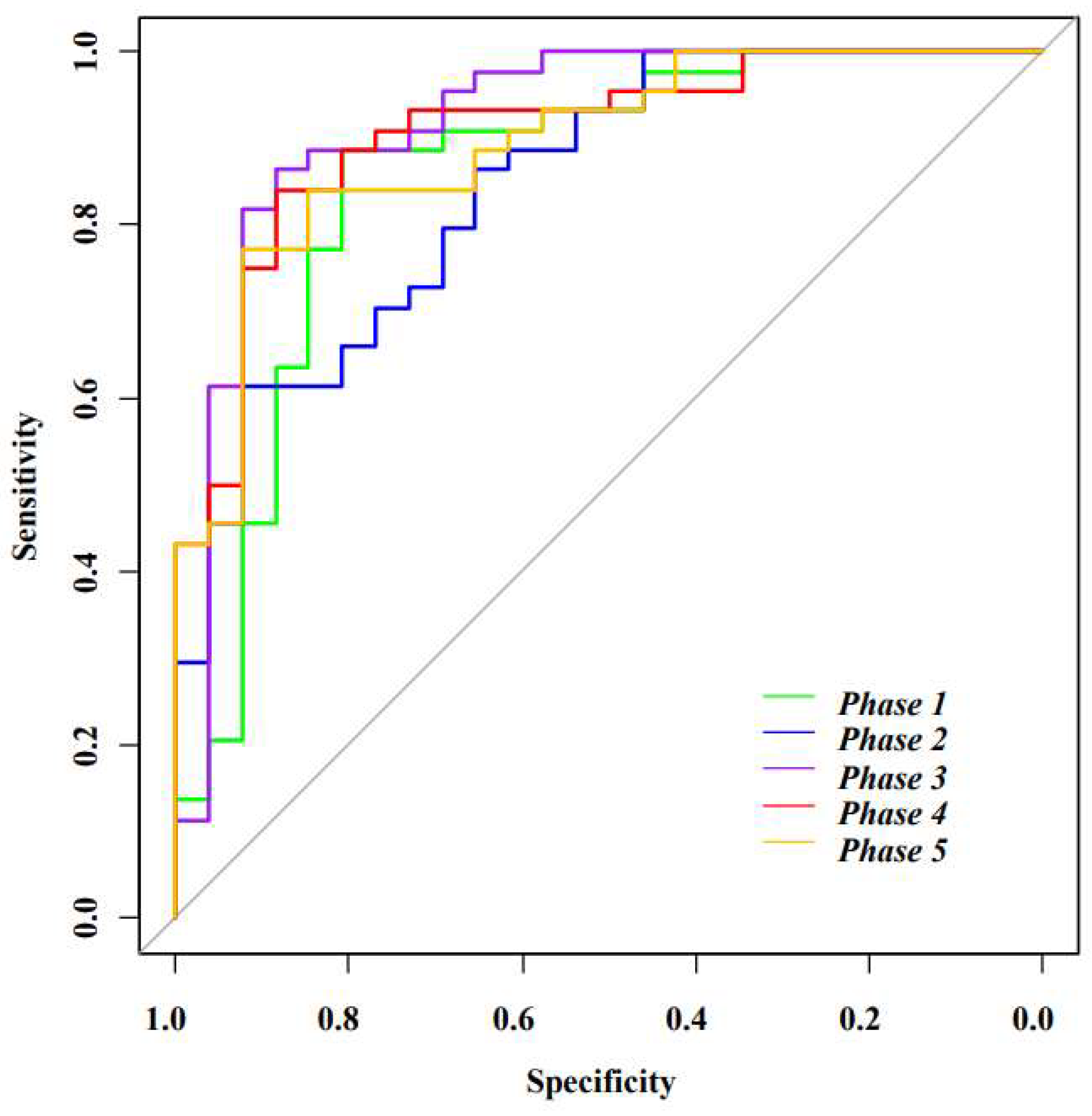
3.3. Model Performance Evaluation
3.4. Analysis of Features in Different Phases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loibl, S.; Denkert, C.; von Minckwitz, G. Neoadjuvant treatment of breast cancer—Clinical and research perspective. Breast 2015, 24 (Suppl. S2), S73–S77. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, M.; von Minckwitz, G.; Mamounas, E.P.; Cameron, D.; Carey, L.A.; Cristofanilli, M.; Denkert, C.; Eiermann, W.; Gnant, M.; Harris, J.R.; et al. Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann. Surg. Oncol. 2012, 19, 1508–1516. [Google Scholar] [CrossRef] [PubMed]
- Mieog, J.S.; van der Hage, J.A.; van de Velde, C.J. Neoadjuvant chemotherapy for operable breast cancer. Br. J. Surg. 2007, 94, 1189–1200. [Google Scholar] [CrossRef]
- Minarikova, L.; Bogner, W.; Pinker, K.; Valkovič, L.; Zaric, O.; Bago-Horvath, Z.; Bartsch, R.; Helbich, T.H.; Trattnig, S.; Gruber, S. Investigating the prediction value of multiparametric magnetic resonance imaging at 3 T in response to neoadjuvant chemotherapy in breast cancer. Eur. Radiol. 2017, 27, 1901–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hylton, N.M.; Blume, J.D.; Bernreuter, W.K.; Pisano, E.D.; Rosen, M.A.; Morris, E.A.; Weatherall, P.T.; Lehman, C.D.; Newstead, G.M.; Polin, S.; et al. Locally advanced breast cancer: MR imaging for prediction of response to neoadjuvant chemotherapy—results from ACRIN 6657/I-SPY TRIAL. Radiology 2012, 263, 663–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, W.J.; Kim, W.K.; Shin, H.J.; Cha, J.H.; Chae, E.Y.; Kim, H.H. Evaluation of the Tumor Response after Neoadjuvant Chemotherapy in Breast Cancer Patients: Correlation between Dynamic Contrast-enhanced Magnetic Resonance Imaging and Pathologic Tumor Cellularity. Clin. Breast Cancer 2018, 18, e115–e121. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Abramson, R.G.; Arlinghaus, L.R.; Kang, H.; Chakravarthy, A.B.; Abramson, V.G.; Farley, J.; Mayer, I.A.; Kelley, M.C.; Meszoely, I.M.; et al. Multiparametric Magnetic Resonance Imaging for Predicting Pathological Response after the First Cycle of Neoadjuvant Chemotherapy in Breast Cancer. Invest. Radiol 2015, 50, 195–204. [Google Scholar] [CrossRef]
- Smith, I.C.; Heys, S.D.; Hutcheon, A.W.; Miller, I.D.; Payne, S.; Gilbert, F.J.; Ah-See, A.K.; Eremin, O.; Walker, L.G.; Sarkar, T.K.; et al. Neoadjuvant chemotherapy in breast cancer: Significantly enhanced response with docetaxel. J. Clin. Oncol. 2002, 20, 1456–1466. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Angulo, A.M.; Morales-Vasquez, F.; Hortobagyi, G.N. Overview of resistance to systemic therapy in patients with breast cancer. Adv. Exp. Med. Biol. 2007, 608, 1–22. [Google Scholar]
- Berg, W.A.; Gutierrez, L.; NessAiver, M.S.; Carter, W.B.; Bhargavan, M.; Lewis, R.S.; Ioffe, O.B. Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 2004, 233, 830–849. [Google Scholar] [CrossRef]
- Park, J.S.; Moon, W.K.; Lyou, C.Y.; Cho, N.; Kang, K.W.; Chung, J.K. The assessment of breast cancer response to neoadjuvant chemotherapy: Comparison of magnetic resonance imaging and 18F-fluorodeoxyglucose positron emission tomography. Acta. Radiol. 2011, 52, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.; Rosen, M. Breast MR imaging: Current indications and advanced imaging techniques. Radiol. Clin. North Am. 2010, 48, 1013–1042. [Google Scholar] [CrossRef] [PubMed]
- Fowler, A.M.; Mankoff, D.A.; Joe, B.N. Imaging Neoadjuvant Therapy Response in Breast Cancer. Radiology 2017, 285, 358–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Forgia, D.; Vestito, A.; Lasciarrea, M.; Comes, M.C.; Diotaiuti, S.; Giotta, F.; Latorre, A.; Lorusso, V.; Massafra, R.; Palmiotti, G.; et al. Response Predictivity to Neoadjuvant Therapies in Breast Cancer: A Qualitative Analysis of Background Parenchymal Enhancement in DCE-MRI. J. Pers. Med. 2021, 11, 256. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.; Deist, T.M.; Peerlings, J.; de Jong, E.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Avanzo, M.; Stancanello, J.; El Naqa, I. Beyond imaging: The promise of radiomics. Physica. Medica. 2017, 38, 122–139. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More Than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Chamming’S, F.; Ueno, Y.; Ferre, R.; Kao, E.; Jannot, A.S.; Chong, J.; Omeroglu, A.; Mesurolle, B.; Reinhold, C.; Gallix, B. Features from Computerized Texture Analysis of Breast Cancers at Pretreatment MR Imaging Are Associated with Response to Neoadjuvant Chemotherapy. Radiology 2018, 286, 412–420. [Google Scholar] [CrossRef] [Green Version]
- Parikh, J.; Selmi, M.; Charles-Edwards, G.; Cameron, D. Changes in primary breast cancer heterogeneity may augment midtreatment MR imaging assessment of response to neoadjuvant chemotherapy. Radiology 2014, 272, 100–112. [Google Scholar] [CrossRef]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.J.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef] [Green Version]
- La Forgia, D.; Fanizzi, A.; Campobasso, F.; Bellotti, R.; Didonna, V.; Lorusso, V.; Moschetta, M.; Massafra, R.; Tamborra, P.; Tangaro, S.; et al. Radiomic Analysis in Contrast-Enhanced Spectral Mammography for Predicting Breast Cancer Histological Outcome. Diagnostics 2020, 10, 708. [Google Scholar] [CrossRef]
- Fan, M.; Wu, G.; Cheng, H.; Zhang, J.; Shao, G.; Li, L. Radiomic analysis of DCE-MRI for prediction of response to neoadjuvant chemotherapy in breast cancer patients. Eur. J. Radiol. 2017, 94, 140–147. [Google Scholar] [CrossRef]
- Braman, N.M.; Etesami, M.; Prasanna, P.; Dubchuk, C.; Gilmore, H.; Tiwari, P.; Plecha, D.; Madabhushi, A. Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Res. 2017, 19, 1–14. [Google Scholar]
- Comes, M.C.; Fanizzi, A.; Bove, S.; Didonna, V.; Diotaiuti, S.; La Forgia, D.; Latorre, A.; Martinelli, E.; Mencattini, A.; Nardone, A.; et al. Early prediction of neoadjuvant chemotherapy response by exploiting a transfer learning approach on breast DCE-MRIs. Sci. Rep. 2021, 11, 14123. [Google Scholar] [CrossRef] [PubMed]
- Cain, E.H.; Saha, A.; Harowicz, M.R.; Marks, J.R.; Marcom, P.K.; Mazurowski, M.A. Multivariate machine learning models for prediction of pathologic response to neoadjuvant therapy in breast cancer using MRI features: A study using an independent validation set. Breast Cancer Res. Treat. 2019, 173, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Chen, H.; You, C.; Liu, L.; Gu, Y.; Peng, W.; Gao, X.; Li, L. Radiomics of Tumor Heterogeneity in Longitudinal Dynamic Contrast-Enhanced Magnetic Resonance Imaging for Predicting Response to Neoadjuvant Chemotherapy in Breast Cancer. Front Mol. Biosci. 2021, 8, 622219. [Google Scholar] [CrossRef] [PubMed]
- Mahrooghy, M.; Ashraf, A.B.; Daye, D.; McDonald, E.S.; Rosen, M.; Mies, C.; Feldman, M.; Kontos, D. Pharmacokinetic Tumor Heterogeneity as a Prognostic Biomarker for Classifying Breast Cancer Recurrence Risk. IEEE Trans. Biomed. Eng. 2015, 62, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lu, J.; Gao, C.; Zeng, J.; Zhou, C.; Lai, X.; Cai, W.; Xu, M. Predicting the response to neoadjuvant chemotherapy for breast cancer: Wavelet transforming radiomics in MRI. BMC Cancer 2020, 20, 100. [Google Scholar] [CrossRef]
- Haralick, R.; Dinstein, I.; Shanmugan, K. Textural features for image classification. IEEE Trans. Syst. Man. Cybern. 1973, 3, 10–21. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Ko, E.S.; Lim, Y.; Lee, K.S.; Han, B.K.; Ko, E.Y.; Hahn, S.Y.; Nam, S.J. Breast Cancer Heterogeneity: MR Imaging Texture Analysis and Survival Outcomes. Radiology 2017, 282, 665–675. [Google Scholar] [CrossRef]
- Henderson, S.; Purdie, C.; Michie, C.; Evans, A.; Lerski, R.; Johnston, M.; Vinnicombe, S.; Thompson, A.M. Interim heterogeneity changes measured using entropy texture features on T2-weighted MRI at 3.0 T are associated with pathological response to neoadjuvant chemotherapy in primary breast cancer. Eur. Radiol. 2017, 27, 4602–4611. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | pCR (n = 26) | non-pCR (n = 44) | p-Value |
|---|---|---|---|
| Age (Mean years ± SD) | 47.55 ± 10.29 | 46.92 ± 9.36 | 0.801 |
| Menstrual status | 0.939 | ||
| Postmenopausal | 13 (50.0) | 21 (49.0) | |
| Premenopausal | 13 (50.0) | 23 (51.0) | |
| Histological type | 1.000 | ||
| IDC | 26 (100) | 43 (98.0) | |
| ILC | 0 (0.0) | 1 (2.0) | |
| Histologic grade | 0.097 | ||
| 2 | 9 (34.6) | 16 (36.4) | |
| 3 | 17 (65.4) | 28 (63.6) | |
| Molecular subtype | 0.016 * | ||
| Luminal A | 2 (7.7) | 7 (15.9) | |
| Luminal B | 7 (26.9) | 28 (63.7) | |
| HER-2 enriched | 8 (30.8) | 3 (6.8) | |
| TNBC | 9 (34.6) | 6 (13.6) | |
| ER | 0.004 * | ||
| Positive | 9 (34.6) | 31 (70.5) | |
| Negative | 17 (65.4) | 13 (29.5) | |
| PR | 0.001 * | ||
| Positive | 5 (19.2) | 29 (65.9) | |
| Negative | 21 (80.8) | 15 (34.1) | |
| HER-2 | 0.734 | ||
| Positive | 12 (46.2) | 18 (40.9) | |
| Negative | 14 (53.8) | 26 (59.1) | |
| Ki 67 | 0.092 | ||
| <14% | 5 (19.2) | 12 (27.3) | |
| ≥14% | 21 (80.8) | 32 (72.7) |
| Phase 1 | wavelet.LLH_glszm_ZoneEntropy |
| log.sigma.3.0.mm.3D_gldm_SmallDependenceEmphasis | |
| wavelet.HHL_glszm_ZoneEntropy | |
| log.sigma.3.0.mm.3D_glszm_GrayLevelNonUniformity | |
| wavelet.LHL_gldm_SmallDependenceLowGrayLevelEmphasis | |
| original_gldm_LargeDependenceHighGrayLevelEmphasis | |
| Phase 2 | wavelet.HHL_glszm_ZoneEntropy |
| log.sigma.3.0.mm.3D_gldm_SmallDependenceEmphasis | |
| original_glszm_GrayLevelNonUniformity | |
| wavelet.HLL_glrlm_LongRunHighGrayLevelEmphasis | |
| Phase 3 | original_shape_Maximum2DDiameterSlice |
| wavelet.LLH_glszm_ZoneEntropy | |
| wavelet.HHL_glszm_ZoneEntropy | |
| original_glszm_GrayLevelNonUniformity | |
| log.sigma.2.0.mm.3D_glcm_ClusterShade | |
| original_gldm_LargeDependenceHighGrayLevelEmphasis | |
| log.sigma.3.0.mm.3D_gldm_SmallDependenceEmphasis | |
| wavelet.HLL_glrlm_LongRunHighGrayLevelEmphasis | |
| log.sigma.2.0.mm.3D_glrlm_LongRunHighGrayLevelEmphasis | |
| wavelet.LLH_firstorder_Median | |
| Phase 4 | wavelet.LLH_glszm_ZoneEntropy |
| original_glszm_GrayLevelNonUniformity | |
| wavelet.HLH_glszm_ZoneEntropy | |
| wavelet.HHL_glszm_ZoneEntropy | |
| log.sigma.2.0.mm.3D_glcm_ClusterShade | |
| wavelet.LLL_glcm_Correlation | |
| log.sigma.3.0.mm.3D_glszm_GrayLevelNonUniformity | |
| wavelet.LLH_gldm_SmallDependenceLowGrayLevelEmphasis | |
| original_gldm_LargeDependenceHighGrayLevelEmphasis | |
| Phase 5 | wavelet.LLH_glszm_ZoneEntropy |
| original_glszm_GrayLevelNonUniformity | |
| wavelet.HHL_glszm_ZoneEntropy | |
| wavelet.LLL_glcm_Correlation | |
| wavelet.HLH_glszm_ZoneEntropy | |
| log.sigma.2.0.mm.3D_glcm_ClusterShade | |
| log.sigma.3.0.mm.3D_glszm_GrayLevelNonUniformity | |
| log.sigma.2.0.mm.3D_glrlm_LongRunHighGrayLevelEmphasis |
| Model | AUC (95%CI) | Sensitivity | Specificity | Accuracy | Youden Index |
|---|---|---|---|---|---|
| Phase 1 | 0.858(0.757–0.959) | 0.886 | 0.808 | 0.786 | 0.694 |
| Phase 2 | 0.845 (0.753–0.938) | 0.614 | 0.923 | 0.771 | 0.537 |
| Phase 3 | 0.919 (0.842–0.996) | 0.864 | 0.885 | 0.857 | 0.748 |
| Phase 4 | 0.906 (0.835–0.978) | 0.841 | 0.885 | 0.843 | 0.726 |
| Phase 5 | 0.892 (0.815–0.968) | 0.773 | 0.923 | 0.786 | 0.696 |
| Time Point | non-pCR (n = 26) | pCR (n = 44) | Statistics | p-Value |
|---|---|---|---|---|
| wavelet.LLH_glszm_ZoneEntropy | ||||
| Phase 1 | 0.19 (0.13, 0.24) | 0.13 (0.08, 0.16) | 3.257 | 0.001 * |
| Phase 2 | 0.19 (0.17, 0.26) | 0.14 (0.10, 0.21) | 3.124 | 0.002 * |
| Phase 3 | 0.20(0.17, 0.27) | 0.13(0.10, 0.20) | 3.343 | 0.001 * |
| Phase 4 | 0.19(0.17, 0.26) | 0.13(0.09, 0.21) | 3.367 | 0.001 * |
| Phase 5 | 0.20(0.16, 0.26) | 0.13(0.10, 0.20) | 3.379 | 0.001 * |
| original_glszm_GrayLevelNonUniformity | ||||
| Phase 1 | 1.41(0.71, 2.55) | 0.87(0.53, 1.69) | 2.018 | 0.044 * |
| Phase 2 | 2.32 ± 1.20 | 1.60 ± 0.91 | 2.837 | 0.006 * |
| Phase 3 | 2.41 ± 1.09 | 1.64 ± 0.83 | 3.096 | 0.003 * |
| Phase 4 | 2.26 ± 0.99 | 1.60 ± 0.79 | 3.071 | 0.003 * |
| Phase 5 | 2.23 ± 0.91 | 1.55 ± 0.76 | 3.358 | 0.001 * |
| log.sigma.3.0.mm.3D_gldm_ SmallDependenceEmphasis | ||||
| Phase 1 | 2.08 ± 1.19 | 1.44 ± 0.90 | 2.578 | 0.012 * |
| Phase 2 | 3.01(2.54, 3.62) | 2.59(1.77, 2.84) | 2.723 | 0.006 * |
| Phase 3 | 3.14(2.35, 3.57) | 2.54(1.99, 2.93) | 2.443 | 0.015 * |
| Phase 4 | 2.93(2.17, 3.58) | 2.39(1.88, 2.90) | 2.261 | 0.024 * |
| Phase 5 | 2.88 ± 1.02 | 2.31 ± 0.88 | 2.502 | 0.015 * |
| wavelet.LLL_glcm_Correlation | ||||
| Phase 1 | 0.03 ± 0.07 | 0.05 ± 0.08 | −1.033 | 0.305 |
| Phase 2 | 0.01 ± 0.08 | 0.03 ± 0.08 | −1.342 | 0.184 |
| Phase 3 | −0.02 ± 0.08 | 0.02 ± 0.09 | −1.997 | 0.05 * |
| Phase 4 | −0.01(−0.09, 0.05) | 0.01(−0.01, 0.07) | −1.92 | 0.055 |
| Phase 5 | −0.02(−0.09, 0.03) | 0.02(−0.01, 0.05) | −2.601 | 0.009 * |
| wavelet.HHL_glszm_ZoneEntropy | ||||
| Phase 1 | 0.42(0.11, 0.71) | 0.18(0.06, 0.33) | 2.686 | 0.007 * |
| Phase 2 | 0.47(0.20, 0.80) | 0.22(0.08, 0.39) | 3.051 | 0.002 * |
| Phase 3 | 0.50(0.20, 0.87) | 0.20(0.09, 0.36) | 3.33 | 0.001 * |
| Phase 4 | 0.49(0.17, 0.70) | 0.23(0.09, 0.35) | 2.662 | 0.008 * |
| Phase 5 | 0.46(0.20, 0.78) | 0.23(0.10, 0.33) | 3.257 | 0.001 * |
| log.sigma.2.0.mm.3D_glcm_ ClusterShade | ||||
| Phase 1 | −5.36(−31.94, 0.52) | 1.98(−2.03, 26.89) | −3.233 | 0.001 * |
| Phase 2 | −4.11(−33.18, 6.39) | 3.39(−7.09, 60.64) | −2.127 | 0.033 * |
| Phase 3 | −5.72(−30.67, 7.14) | 3.97(−6.00, 55.44) | −2.37 | 0.018 * |
| Phase 4 | 0.25(−31.26, 9.41) | 3.71(−5.23, 61.37) | −1.993 | 0.046 * |
| Phase 5 | 0.02(−29.43, 11.50) | 6.43(−3.48, 56.29) | −1.872 | 0.061 |
| log.sigma.2.0.mm.3D_glrlm_ LongRunHighGrayLevelEmphasis | ||||
| Phase 1 | 0.20(−0.12, 0.45) | −0.02(−0.23, 0.26) | 1.155 | 0.248 |
| Phase 2 | 0.27 ± 0.57 | 0.10 ± 0.44 | 1.378 | 0.173 |
| Phase 3 | 0.33 ± 0.58 | 0.08 ± 0.43 | 2.102 | 0.039 * |
| Phase 4 | 0.34 ± 0.61 | 0.08 ± 0.42 | 1.935 | 0.06 |
| Phase 5 | 0.28(−0.20, 0.68) | 0.00(−0.30, 0.31) | 1.69 | 0.091 |
| wavelet.HLH_glszm_ZoneEntropy | ||||
| Phase 1 | 0.37(0.19, 0.61) | 0.16(0.06, 0.35) | 2.565 | 0.01 * |
| Phase 2 | 0.39(0.26, 0.63) | 0.24(0.12, 0.39) | 2.82 | 0.005 * |
| Phase 3 | 0.41(0.25, 0.65) | 0.23(0.12, 0.39) | 2.929 | 0.003 * |
| Phase 4 | 0.43(0.23, 0.68) | 0.23(0.13, 0.34) | 2.808 | 0.005 * |
| Phase 5 | 0.42(0.22, 0.67) | 0.24(0.11, 0.37) | 2.893 | 0.004 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, S.; Chen, L.; Tao, J.; Liu, J.; Zhu, W.; Liu, H.; Yang, F. Radiomics Analysis of Multi-Phase DCE-MRI in Predicting Tumor Response to Neoadjuvant Therapy in Breast Cancer. Diagnostics 2021, 11, 2086. https://doi.org/10.3390/diagnostics11112086
Peng S, Chen L, Tao J, Liu J, Zhu W, Liu H, Yang F. Radiomics Analysis of Multi-Phase DCE-MRI in Predicting Tumor Response to Neoadjuvant Therapy in Breast Cancer. Diagnostics. 2021; 11(11):2086. https://doi.org/10.3390/diagnostics11112086
Chicago/Turabian StylePeng, Shuyi, Leqing Chen, Juan Tao, Jie Liu, Wenying Zhu, Huan Liu, and Fan Yang. 2021. "Radiomics Analysis of Multi-Phase DCE-MRI in Predicting Tumor Response to Neoadjuvant Therapy in Breast Cancer" Diagnostics 11, no. 11: 2086. https://doi.org/10.3390/diagnostics11112086