
CT-Based Radiomics Helps to Predict Residual Lung Lesions in COVID-19 Patients at Three Months after Discharge

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
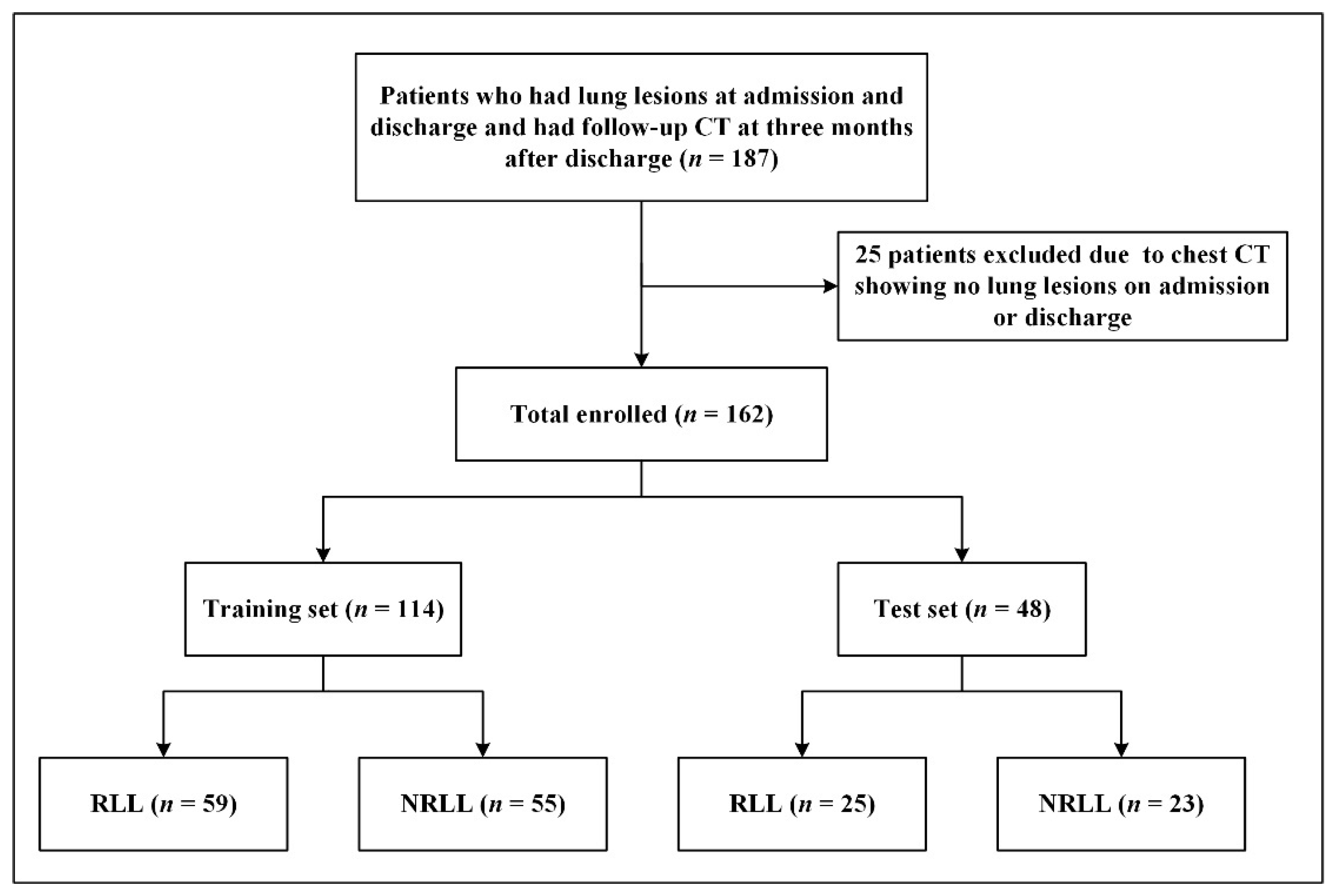
2.1. Patients
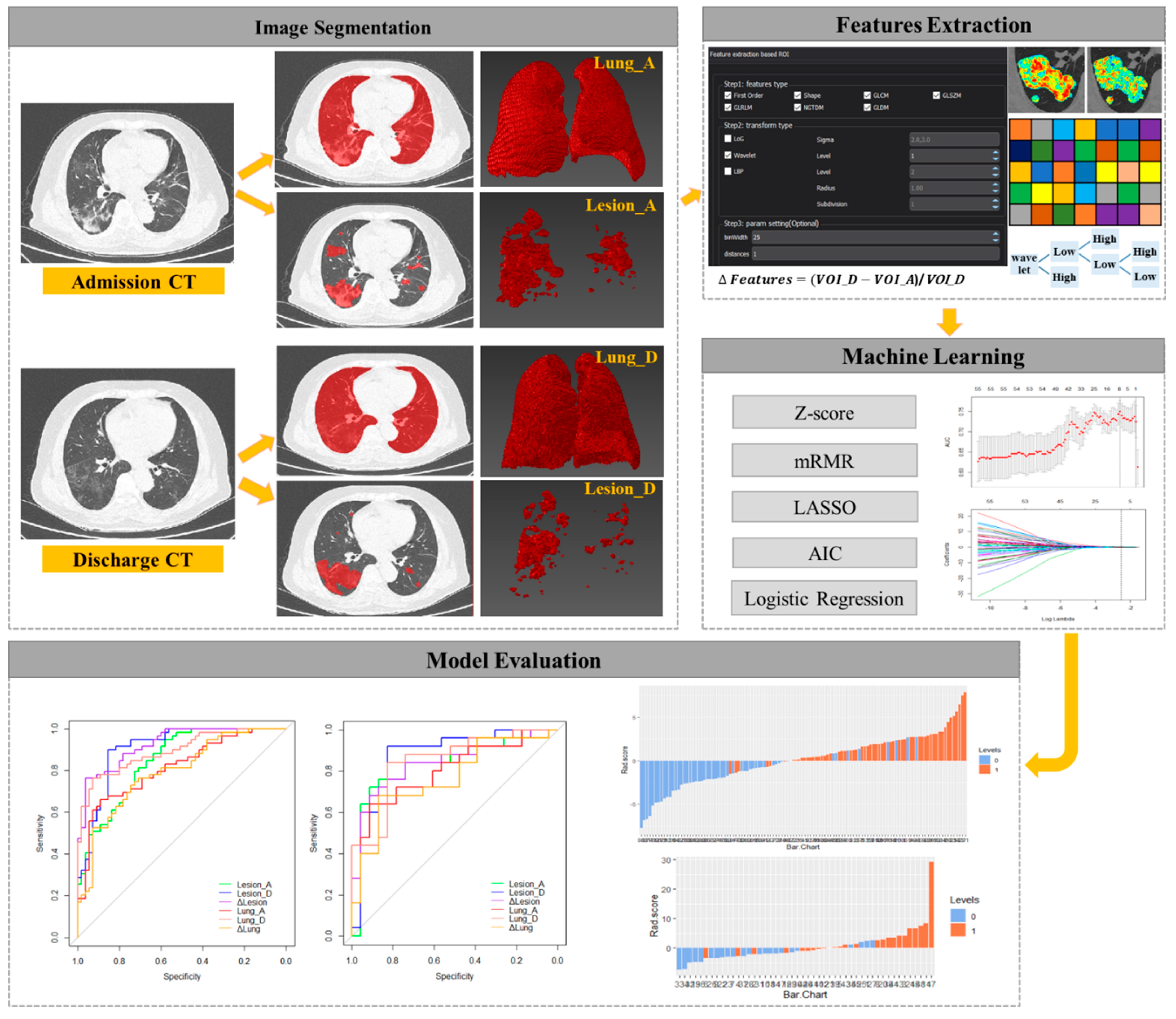
2.2. CT Image Acquisition and Segmentation
2.3. Subjective Assessment of Follow-Up CTs
2.4. Radiomic Feature Extraction
2.5. Radiomic Feature Selection and Model Construction
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Establishment of Radiomic Signature
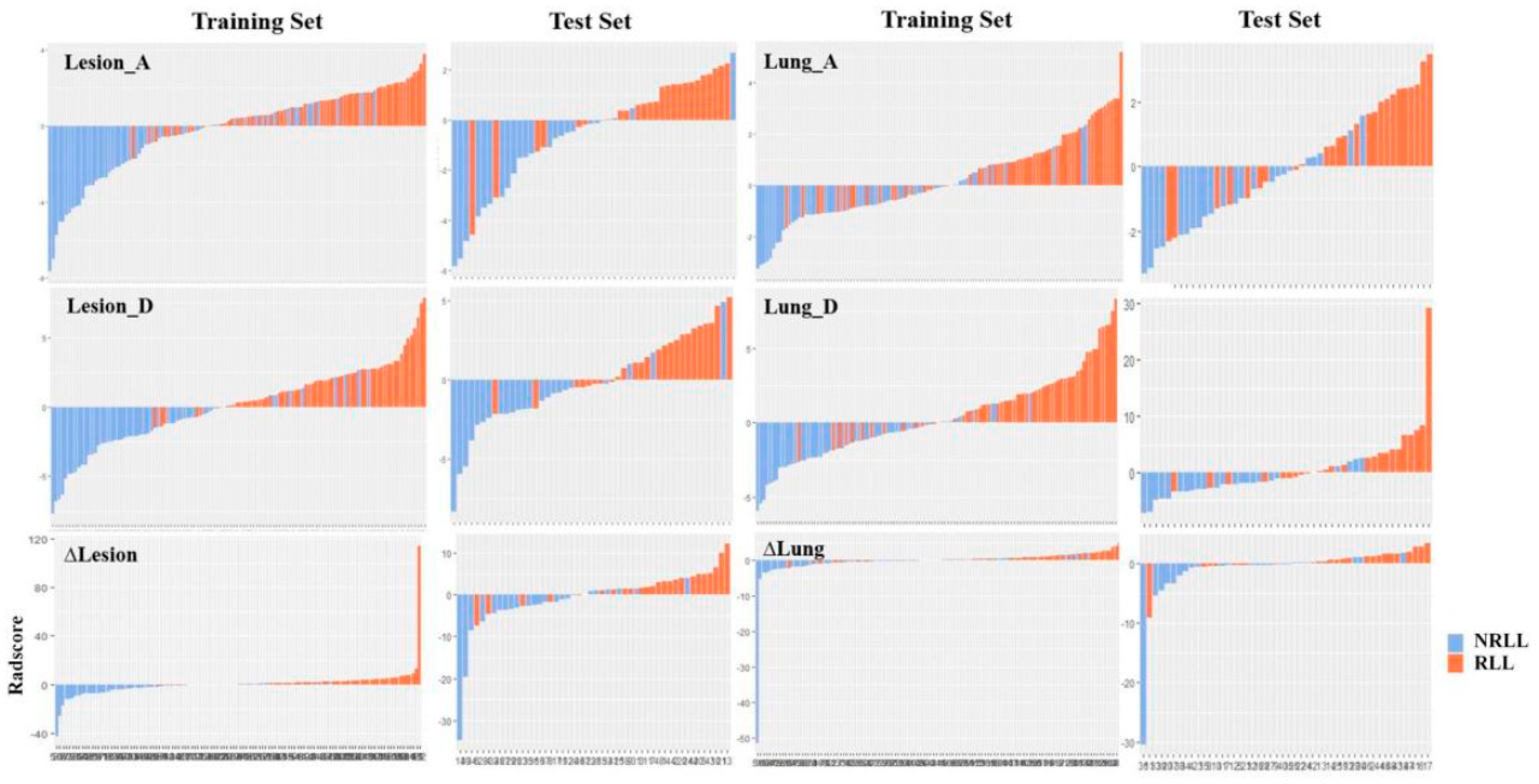
3.3. Evaluation of Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, Transmission, and Pathogenesis of SARS-CoV-2. BMJ 2020, m3862. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-J.; Dong, X.; Cao, Y.-Y.; Yuan, Y.-D.; Yang, Y.-B.; Yan, Y.-Q.; Akdis, C.A.; Gao, Y.-D. Clinical Characteristics of 140 Patients Infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Qin, W.; Chen, S.; Zhang, Y.; Dong, F.; Zhang, Z.; Hu, B.; Zhu, Z.; Li, F.; Wang, X.; Wang, Y.; et al. Diffusion Capacity Abnormalities for Carbon Monoxide in Patients with COVID-19 at Three-Month Follow-Up. Eur. Respir. J. 2021, 2003677. [Google Scholar] [CrossRef]
- Blomberg, B.; Mohn, K.G.-I.; Brokstad, K.A.; Zhou, F.; Linchausen, D.W.; Hansen, B.-A.; Lartey, S.; Onyango, T.B.; Kuwelker, K.; Sævik, M.; et al. Long COVID in a Prospective Cohort of Home-Isolated Patients. Nat. Med. 2021. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, W.; Pan, F.; Li, L.; Yang, L.; Zheng, D.; Wang, J.; Liang, B. The Pulmonary Sequalae in Discharged Patients with COVID-19: A Short-Term Observational Study. Respir. Res. 2020, 21, 125. [Google Scholar] [CrossRef]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and High-Resolution CT Features of the COVID-19 Infection: Comparison of the Initial and Follow-up Changes. Investig. Radiol. 2020, 55, 332–339. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The National Health Commision of the People’s Republic of China. Diagnosis and Treatment Protocol for COVID-19 in China (Trial Fifth Edition). 8 February 2020. [Google Scholar]
- Zhang, H.; Zhang, J.; Zhang, H.; Nan, Y.; Zhao, Y.; Fu, E.; Xie, Y.; Liu, W.; Li, W.; Zhang, H.; et al. Automated Detection and Quantification of COVID-19 Pneumonia: CT Imaging Analysis by a Deep Learning-Based Software. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2525–2532. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The Bridge between Medical Imaging and Personalized Medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Wan, L.; Peng, W.; Zou, S.; Ye, F.; Geng, Y.; Ouyang, H.; Zhao, X.; Zhang, H. MRI-Based Delta-Radiomics Are Predictive of Pathological Complete Response after Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer. Acad. Radiol. 2020, in press. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-Month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [Green Version]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; De Dominicis, C.; Laghi, A. Chest CT Features of COVID-19 in Rome, Italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-Month, 6-Month, 9-Month, and 12-Month Respiratory Outcomes in Patients Following COVID-19-Related Hospitalisation: A Prospective Study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Zhang, X.; Jia, X.; Zheng, Y.; Shi, H. Fibrotic Interstitial Lung Abnormalities at 1-Year Follow-up CT after Severe COVID-19. Radiology 2021, 210972. [Google Scholar] [CrossRef]
- Wu, Q.; Zhong, L.; Li, H.; Guo, J.; Li, Y.; Hou, X.; Yang, F.; Xie, Y.; Li, L.; Xing, Z. A Follow-Up Study of Lung Function and Chest Computed Tomography at 6 Months after Discharge in Patients with Coronavirus Disease 2019. Can. Respir. J. 2021, 2021, 6692409. [Google Scholar] [CrossRef]
- Li, L.; Wang, L.; Zeng, F.; Peng, G.; Ke, Z.; Liu, H.; Zha, Y. Development and Multicenter Validation of a CT-Based Radiomics Signature for Predicting Severe COVID-19 Pneumonia. Eur. Radiol. 2021, 31, 7901–7912. [Google Scholar] [CrossRef]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A Deep Look into Radiomics. Radiol. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.W.L.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The Process and the Challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, X.; Li, X.; Bian, Y.; Ji, X.; Lu, J. Radiomics Nomogram for the Prediction of 2019 Novel Coronavirus Pneumonia Caused by SARS-CoV-2. Eur. Radiol. 2020, 30, 6888–6901. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Dong, D.; Li, L.; Gong, W.; Li, X.; Bai, Y.; Wang, M.; Hu, Z.; Zha, Y.; Tian, J. Classification of Severe and Critical Covid-19 Using Deep Learning and Radiomics. IEEE J. Biomed. Health Inform. 2020, 24, 3585–3594. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, S.; Li, L.; Wu, Q.; Qian, W.; Hu, Y.; Li, L.; Zhou, X.; Ma, H.; Li, H.; et al. Radiomics Analysis of Computed Tomography Helps Predict Poor Prognostic Outcome in COVID-19. Theranostics 2020, 10, 7231–7244. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training Set (n = 114) | Test Set (n = 48) | ||||
|---|---|---|---|---|---|---|
| RLL (n = 59) | NRLL (n = 55) | p-Value | RLL (n = 25) | NRLL (n = 23) | p-Value | |
| Age (years) | 57 (48, 66) | 51 (39, 59) | 0.005 | 63 (56, 69) | 44 (35, 57) | <0.001 |
| Sex, n (%) | - | - | 0.071 | - | - | 0.036 |
| Male | 28 (47.5%) | 17 (30.9%) | - | 14 (56.0%) | 6 (26.1%) | - |
| Female | 31 (52.5%) | 38 (69.1%) | - | 11 (44.0%) | 17 (73.9%) | - |
| Length of hospital stay (days) | 20 (16, 27) | 18 (11, 28) | 0.213 | 28 (18.5, 36.5) | 17 (10, 25) | 0.037 |
| Days from discharge to follow-up CT | 103 (86, 122) | 107 (72, 127) | 0.869 | 94 (79.5, 114.5) | 110 (88, 129) | 0.137 |
| Model | Features | Coefficients |
|---|---|---|
| Lesion_A (n = 6) | log.sigma.3.0.mm.3D_glcm_InverseVariance | 27.3963 |
| wavelet.HLH_firstorder_Mean | −2.6492 | |
| log.sigma.3.0.mm.3D_firstorder_Skewness | −2.8087 | |
| wavelet.LHH_glcm_Correlation | 39.5595 | |
| original_glszm_SmallAreaLowGrayLevelEmphasis | −653.335 | |
| original_shape_Sphericity | −7.1196 | |
| Lesion_D (n = 8) | log.sigma.3.0.mm.3D_glcm_InverseVariance | 40.8774 |
| wavelet.HLL_glcm_ClusterShade | −0.002 | |
| wavelet.HLL_firstorder_Median | 0.2507 | |
| wavelet.HLL_gldm_LargeDependenceLowGrayLevelEmphasis | 250.846 | |
| wavelet.LLL_gldm_LargeDependenceHighGrayLevelEmphasis | 7.11 × 10−5 | |
| original_shape_Maximum2DDiameterRow | 0.0153 | |
| log.sigma.4.0.mm.3D_glrlm_LongRunHighGrayLevelEmphasis | 0.001 | |
| wavelet.HLH_gldm_SmallDependenceHighGrayLevelEmphasis | 0.01845 | |
| Δlesion (n = 13) | log.sigma.3.0.mm.3D_glcm_InverseVariance | 21.7079 |
| wavelet.HHL_glcm_ClusterShade | 0.0154 | |
| log.sigma.3.0.mm.3D_firstorder_Skewness | 0.0154 | |
| log.sigma.4.0.mm.3D_glszm_LargeAreaHighGrayLevelEmphasis | −1.7870 | |
| log.sigma.3.0.mm.3D_glszm_SmallAreaEmphasis | 10.7100 | |
| log.sigma.3.0.mm.3D_firstorder_Mean | −0.0573 | |
| wavelet.LHH_firstorder_Skewness | 0.1581 | |
| log.sigma.4.0.mm.3D_gldm_SmallDependenceLowGrayLevelEmphasis | −0.009 | |
| log.sigma.1.0.mm.3D_firstorder_Mean | 0.2537 | |
| log.sigma.1.0.mm.3D_glszm_GrayLevelVariance | 6.5212 | |
| wavelet.HHH_firstorder_RootMeanSquared | 1551.5109 | |
| log.sigma.1.0.mm.3D_gldm_LargeDependenceLowGrayLevelEmphasis | 1.0871 | |
| wavelet.LLL_firstorder_Maximum | −0.0932 | |
| Lung_A (n = 3) | wavelet.LHL_firstorder_Mean | −0.7123 |
| wavelet.HHH_glszm_SmallAreaEmphasis | 29.0881 | |
| wavelet.LLL_glszm_ZoneEntropy | 6.7584 | |
| Lung_D (n = 7) | wavelet.HHH_firstorder_Mean | 39.2045 |
| wavelet.HLH_firstorder_Skewness | −7.3873 | |
| log.sigma.2.0.mm.3D_glcm_Correlation | −134.446 | |
| wavelet.HHL_glszm_SmallAreaLowGrayLevelEmphasis | 7178.18 | |
| wavelet.LHH_firstorder_Median | −18.3834 | |
| wavelet.LLH_glrlm_RunEntropy | 9.1189 | |
| wavelet.LLL_glcm_Imc2 | 21.9867 | |
| Δlung (n = 5) | wavelet.HHL_firstorder_Mean | −0.1124 |
| wavelet.LHL_firstorder_Skewness | 0.6402 | |
| log.sigma.2.0.mm.3D_glszm_ZoneEntropy | −37.0901 | |
| log.sigma.5.0.mm.3D_gldm_DependenceNonUniformityNormalized | −10.0756 | |
| wavelet.HLH_glszm_LargeAreaHighGrayLevelEmphasis | −0.4602 |
| Model | Training Set | Test Set | p Value | ||||
|---|---|---|---|---|---|---|---|
| AUC (95% CI) | Sensitivity | Specificity | AUC (95% CI) | Sensitivity | Specificity | ||
| Lesion_A | 0.849 (0.780–0.917) | 0.949 | 0.582 | 0.837 (0.713–0.961) | 0.720 | 0.913 | 0.8670 |
| Lesion_D | 0.907 (0.851–0.962) | 0.898 | 0.855 | 0.875 (0.766–0.984) | 0.920 | 0.826 | 0.6115 |
| Δlesion | 0.927 (0.883–0.971) | 0.763 | 0.964 | 0.837 (0.718–0.955) | 0.680 | 0.913 | 0.1678 |
| Lung_A | 0.812 (0.734–0.891) | 0.661 | 0.891 | 0.809 (0.686–0.932) | 0.640 | 0.913 | 0.9612 |
| Lung_D | 0.893 (0.836–0.950) | 0.763 | 0.927 | 0.849 (0.738–0.960) | 0.840 | 0.826 | 0.4890 |
| Δlung | 0.791 (0.709–0.873) | 0.729 | 0.745 | 0.765 (0.628–0.903) | 0.680 | 0.870 | 0.7490 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.; Wu, F.; Chen, L.; Yu, J.; Sun, W.; Nie, Z.; Liu, H.; Yang, F.; Zheng, C. CT-Based Radiomics Helps to Predict Residual Lung Lesions in COVID-19 Patients at Three Months after Discharge. Diagnostics 2021, 11, 1814. https://doi.org/10.3390/diagnostics11101814
Huang J, Wu F, Chen L, Yu J, Sun W, Nie Z, Liu H, Yang F, Zheng C. CT-Based Radiomics Helps to Predict Residual Lung Lesions in COVID-19 Patients at Three Months after Discharge. Diagnostics. 2021; 11(10):1814. https://doi.org/10.3390/diagnostics11101814
Chicago/Turabian StyleHuang, Jia, Feihong Wu, Leqing Chen, Jie Yu, Wengang Sun, Zhuang Nie, Huan Liu, Fan Yang, and Chuansheng Zheng. 2021. "CT-Based Radiomics Helps to Predict Residual Lung Lesions in COVID-19 Patients at Three Months after Discharge" Diagnostics 11, no. 10: 1814. https://doi.org/10.3390/diagnostics11101814