
Risk Stratification Using 18F-FDG PET/CT and Artificial Neural Networks in Head and Neck Cancer Patients Undergoing Radiotherapy

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. 2-[18F]FDG PET/CT Imaging Protocol
2.3. Feature Extraction
2.4. Data Preprocessing
2.5. Feature Selection
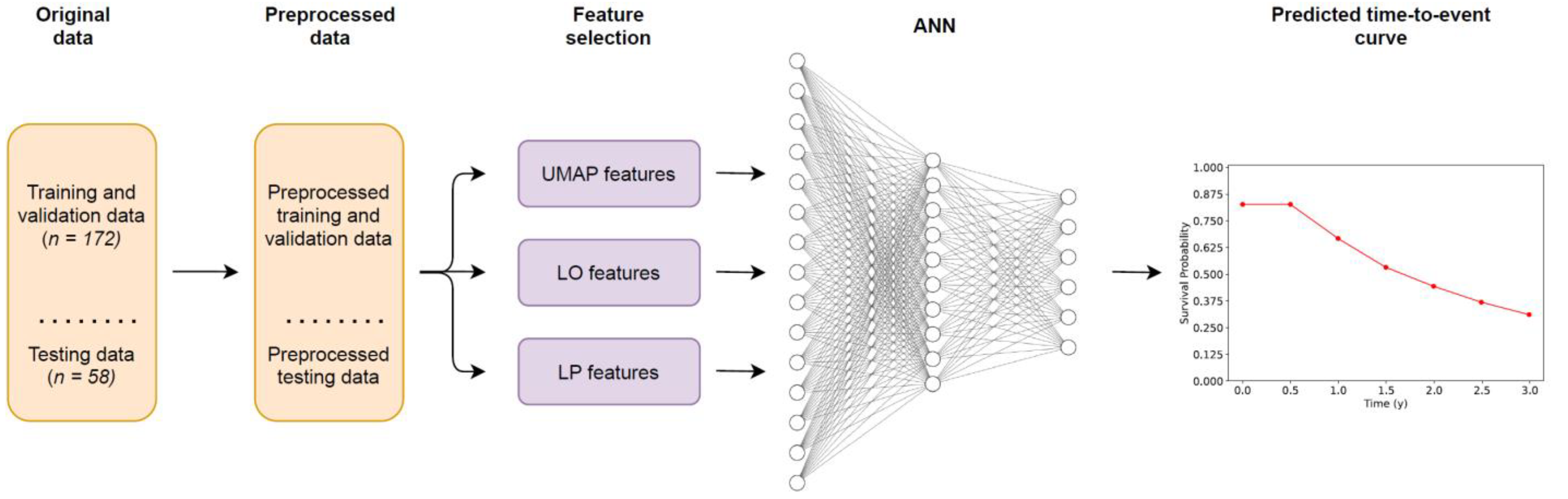
2.6. Artificial Neural Network
2.7. Model Optimization and Details
2.8. Statistical Analysis
3. Results
3.1. Patients
3.2. Feature Extraction
3.3. Data Preprocessing
3.4. Feature Selection
3.5. Model Optimization and Details
3.6. HCI Comparisons
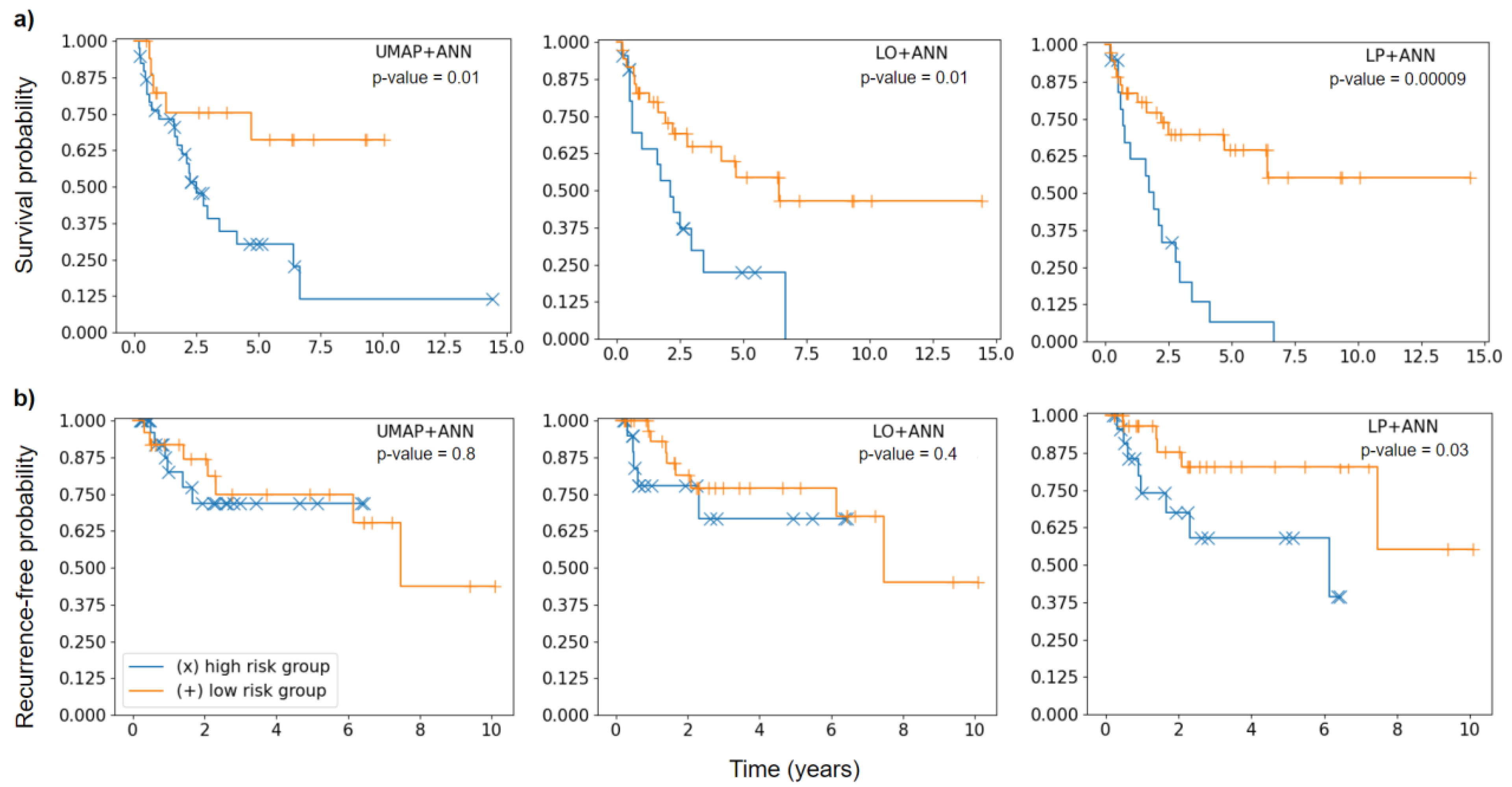
3.7. Risk Group Stratification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

Appendix B

{kind=link}
{kind=link}
| Training Cohort | Testing Cohort | Proportion of Training and Testing Cohort | |||||
|---|---|---|---|---|---|---|---|
| Patients | Percentage [%] | Patients | Percentage [%] | Training Cohort [%] | Testing Cohort [%] | ||
| Age at Diagnosis * | <45 | 9 | 5.20 | 4 | 7.00 | 69.2 | 30.8 |
| 45–65 | 90 | 52.00 | 28 | 49.10 | 76.3 | 23.7 | |
| >65 | 74 | 42.80 | 25 | 43.90 | 74.7 | 25.3 | |
| Gender * | male | 127 | 73.4 | 40 | 70.2 | 76.0 | 24.0 |
| female | 46 | 26.6 | 17 | 29.8 | 73.0 | 27.0 | |
| Tumor localization | Nasopharynx | 11 | 6.4 | 4 | 7.0 | 73.3 | 26.7 |
| Oropharynx | 58 | 33.5 | 22 | 38.6 | 72.5 | 27.5 | |
| Oral Cavity | 52 | 30.1 | 21 | 36.8 | 71.2 | 28.8 | |
| Hypopharynx | 27 | 15.6 | 4 | 7.0 | 87.1 | 12.9 | |
| Larynx | 25 | 14.5 | 6 | 10.5 | 80.6 | 19.4 | |
| UICC Stage | I | 5 | 2.9 | 0 | 0.0 | 100.0 | 0.0 |
| II | 17 | 9.8 | 8 | 14.0 | 68.0 | 32.0 | |
| III | 35 | 20.2 | 10 | 17.5 | 77.8 | 22.2 | |
| IV | 116 | 67.1 | 39 | 68.4 | 74.8 | 25.2 | |
| T Stage * | T1 | 17 | 9.8 | 5 | 8.8 | 77.3 | 22.7 |
| T2 | 41 | 23.7 | 16 | 28.1 | 71.9 | 28.1 | |
| T3 | 57 | 32.9 | 9 | 15.8 | 86.4 | 13.6 | |
| T4 | 58 | 33.5 | 27 | 47.4 | 68.2 | 31.8 | |
| N Stage * | N0 | 40 | 23.1 | 10 | 17.5 | 80.0 | 20.0 |
| N1 | 24 | 13.9 | 12 | 21.1 | 66.7 | 33.3 | |
| N2 | 97 | 56.1 | 30 | 52.6 | 76.4 | 23.6 | |
| N3 | 12 | 6.9 | 5 | 8.8 | 70.6 | 29.4 | |
| M Stage | M0 | 161 | 93.1 | 51 | 89.5 | 75.9 | 24.1 |
| M1 | 8 | 4.6 | 4 | 7.0 | 66.7 | 33.3 | |
| Mx | 4 | 2.3 | 2 | 3.5 | 66.7 | 33.3 | |
| Resection status | R0 | 17 | 9.8 | 8 | 14.0 | 68.0 | 32.0 |
| R0 (CM) | 15 | 8.7 | 6 | 10.5 | 71.4 | 28.6 | |
| R1 | 14 | 8.1 | 3 | 5.3 | 82.4 | 17.6 | |
| R2 | 5 | 2.9 | 2 | 3.5 | 71.4 | 28.6 | |
| No surgery/unknwon | 122 | 70.5 | 38 | 66.7 | 76.3 | 23.8 | |
| Lymphovascular invasion | L0 | 29 | 16.8 | 15 | 26.3 | 65.9 | 34.1 |
| L1 | 18 | 10.4 | 1 | 1.8 | 94.7 | 5.3 | |
| No surgery/unknwon | 126 | 72.8 | 41 | 71.9 | 75.4 | 24.6 | |
| Venous tumor invasion | V0 | 38 | 22.0 | 16 | 28.1 | 70.4 | 29.6 |
| V1 | 7 | 4.0 | 1 | 1.8 | 87.5 | 12.5 | |
| No surgery/unknwon | 128 | 74.0 | 40 | 70.2 | 76.2 | 23.8 | |
| Perineural invasion | Pn0 | 26 | 15.0 | 11 | 19.3 | 70.3 | 29.7 |
| Pn1 | 9 | 5.2 | 3 | 5.3 | 75.0 | 25.0 | |
| No surgery/unknwon | 138 | 79.8 | 43 | 75.4 | 76.2 | 23.8 | |
| Tumor grading * | G1 | 8 | 4.6 | 0 | 0.0 | 100.0 | 0.0 |
| G2 | 77 | 44.5 | 25 | 43.9 | 75.5 | 24.5 | |
| G3 | 67 | 38.7 | 21 | 36.8 | 76.1 | 23.9 | |
| No surgery/unknwon | 21 | 12.1 | 11 | 19.3 | 65.6 | 34.4 | |
| Extracapsular enhancement | ECE neg | 44 | 25.4 | 19 | 33.3 | 69.8 | 30.2 |
| ECE pos. | 16 | 9.2 | 3 | 5.3 | 84.2 | 15.8 | |
| No surgery/unknwon | 113 | 65.3 | 35 | 61.4 | 76.4 | 23.6 | |
| HPV-P16 status * | HPV neg | 73 | 42.2 | 17 | 29.8 | 81.1 | 18.9 |
| HPV pos | 26 | 15.0 | 19 | 33.3 | 57.8 | 42.2 | |
| unknown/ not applicable | 74 | 42.8 | 21 | 36.8 | 77.9 | 22.1 | |
| Smoking status * | Nonsmoker | 0 | 0.0 | 0 | 0.0 | 0.0 | 0.0 |
| Smoker | 158 | 91.3 | 52 | 91.2 | 75.2 | 24.8 | |
| unknown | 15 | 8.7 | 5 | 8.8 | 75.0 | 25.0 | |
| Therapy regime | OP + RT | 27 | 15.6 | 14 | 24.6 | 65.9 | 34.1 |
| OP + RCT | 25 | 14.5 | 7 | 12.3 | 78.1 | 21.9 | |
| RCT | 121 | 69.9 | 36 | 63.2 | 77.1 | 22.9 | |
| Death | No | 79 | 45.7 | 28 | 49.1 | 73.8 | 26.2 |
| Yes | 94 | 54.3 | 29 | 50.9 | 76.4 | 23.6 | |
| SUV Values Tumor | SUV Ratio (SUR) | SUV Values Organ | |||
|---|---|---|---|---|---|
| SUV40 | mean | SUV40 | SURmax Liver * | Spine | SUVmean * |
| min | SURmean Liver | SUVmin | |||
| max * | SURTLG Liver | SUVmax | |||
| median | SURmax Spine * | SUVmedian | |||
| peak * | SURmean Spine | MTV | |||
| MTV | SURTLG Spine | TLG | |||
| TLG * | SURmax Aorta * | Aorta | SUVmean * | ||
| SUV50 | mean | SURmean Aorta | SUVmin | ||
| min | SURTLG Aorta | SUVmax | |||
| max | SUV50 | SURmax Liver | SUVmedian | ||
| median | SURmean Liver | MTV | |||
| peak | SURTLG Liver | TLG | |||
| MTV | SURmax Spine | Liver | SUVmean * | ||
| TLG | SURmean Spine | SUVmin | |||
| SUV75 | mean | SURTLG Spine | SUVmax | ||
| min | SURmax Aorta | SUVmedian | |||
| max | SURmean Aorta | MTV | |||
| median | SURTLG Aorta | TLG | |||
| peak | SUV75 | SURmax Liver | |||
| MTV | SURmean Liver | ||||
| TLG | SURTLG Liver | ||||
| SUV90 | mean | SURmax Spine | |||
| min | SURmean Spine | ||||
| max | SURTLG Spine | ||||
| median | SURmax Aorta | ||||
| peak | SURmean Aorta | ||||
| MTV | SURTLG Aorta | ||||
| TLG | SUV90 | SURmax Liver | |||
| SURmean Liver | |||||
| SURTLG Liver | |||||
| SURmax Spine | |||||
| SURmean Spine | |||||
| SURTLG Spine | |||||
| SURmax Aorta | |||||
| SURmean Aorta | |||||
| SURTLG Aorta | |||||
References
- Rogowski, P.; von Bestenbostel, R.; Walter, F.; Straub, K.; Nierer, L.; Kurz, C.; Landry, G.; Reiner, M.; Auernhammer, C.J.; Belka, C.; et al. Feasibility and early clinical experience of online adaptive mr-guided radiotherapy of liver tumors. Cancers 2021, 13, 1523. [Google Scholar] [CrossRef] [PubMed]
- Corradini, S.; Alongi, F.; Andratschke, N.; Belka, C.; Boldrini, L.; Cellini, F.; Debus, J.; Guckenberger, M.; Hörner-Rieber, J.; Lagerwaard, F.J.; et al. MR-guidance in clinical reality: Current treatment challenges and future perspectives. Radiat. Oncol. 2019, 14, 92. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.W.L.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraud, P.; Giraud, P.; Gasnier, A.; El Ayachy, R.; Kreps, S.; Foy, J.P.; Durdux, C.; Huguet, F.; Burgun, A.; Bibault, J.-E. Radiomics and machine learning for radiotherapy in head and neck cancers. Front. Oncol. 2019, 9, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peeken, J.C.; Nüsslin, F.; Combs, S.E. “Radio-oncomics”: The potential of radiomics in radiation oncology. Strahlenther. Onkol. 2017, 193, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Diamant, A.; Chatterjee, A.; Vallières, M.; Shenouda, G.; Seuntjens, J. Deep learning in head & neck cancer outcome prediction. Sci. Rep. 2019, 9, 2764. [Google Scholar] [CrossRef] [Green Version]
- Starke, S.; Leger, S.; Zwanenburg, A.; Leger, K.; Lohaus, F.; Linge, A.; Schreiber, A.; Kalinauskaite, G.; Tinhofer, I.; Guberina, N.; et al. 2D and 3D convolutional neural networks for outcome modelling of locally advanced head and neck squamous cell carcinoma. Sci. Rep. 2020, 10, 15625. [Google Scholar] [CrossRef]
- Lombardo, E.; Kurz, C.; Marschner, S.; Avanzo, M.; Gagliardi, V.; Fanetti, G.; Franchin, G.; Stancanello, J.; Corradini, S.; Niyazi, M.; et al. Distant metastasis time to event analysis with CNNs in independent head and neck cancer cohorts. Sci. Rep. 2021, 11, 6418. [Google Scholar] [CrossRef]
- Unterrainer, M.; Eze, C.; Ilhan, H.; Marschner, S.; Roengvoraphoj, O.; Schmidt-Hegemann, N.S.; Walter, F.; Kunz, W.G.; af Rosenschöld, P.M.; Jeraj, R.; et al. Recent advances of PET imaging in clinical radiation oncology. Radiat. Oncol. 2020, 15, 88. [Google Scholar] [CrossRef] [Green Version]
- Birk Christensen, C.; Loft-Jakobsen, A.; Munck af Rosenschöld, P.; Højgaard, L.; Roed, H.; Berthelsen, A.K. 18F-FDG PET/CT for planning external beam radiotherapy alters therapy in 11% of 581 patients. Clin. Physiol. Funct. Imaging 2018, 38, 278–284. [Google Scholar] [CrossRef]
- Goel, R.; Moore, W.; Sumer, B.; Khan, S.; Sher, D.; Subramaniam, R.M. Clinical practice in PET/CT for the management of head and neck squamous cell cancer. Am. J. Roentgenol. 2017, 209, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Pedraza, S.; Ruiz-Alonso, A.; Hernández-Martínez, A.C.; Cabello, E.; Lora, D.; Pérez-Regadera, J.F. 18F-FDG PET/CT in staging and delineation of radiotherapy volume for head and neck cancer. Rev. Esp. Med. Nucl. Imagen Mol. 2019, 38, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Cacicedo, J.; Fernandez, I.; del Hoyo, O.; Navarro, A.; Gomez-Iturriaga, A.; Pijoan, J.I.; Martinez-Indart, L.; Escudero, J.; Gomez-Suarez, J.; Zarate, R.O.; et al. Prognostic value of maximum standardized uptake value measured by pretreatment 18F-FDG PET/CT in locally advanced head and neck squamous cell carcinoma. Clin. Transl. Oncol. 2017, 19, 1337–1349. [Google Scholar] [CrossRef]
- Martens, R.M.; Noij, D.P.; Koopman, T.; Zwezerijnen, B.; Heymans, M.; de Jong, M.C.; Hoekstra, O.S.; Vergeer, M.R.; de Bree, R.; Leemans, C.R.; et al. Predictive value of quantitative diffusion-weighted imaging and 18-F-FDG-PET in head and neck squamous cell carcinoma treated by (chemo)radiotherapy. Eur. J. Radiol. 2019, 113, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Cheng, N.M.; Hsieh, C.E.; Liao, C.T.; Ng, S.H.; Wang, H.M.; Fang, Y.H.D.; Chou, W.C.; Lin, C.Y.; Yen, T.C. Prognostic Value of Tumor Heterogeneity and SUVmax of Pretreatment 18F-FDG PET/CT for Salivary Gland Carcinoma with High-Risk Histology. Clin. Nucl. Med. 2019, 44, 351–358. [Google Scholar] [CrossRef]
- Maihoefer, C.; Schüttrumpf, L.; Macht, C.; Pflugradt, U.; Hess, J.; Schneider, L.; Woischke, C.; Walch, A.; Baumeister, P.; Kirchner, T.; et al. Postoperative (chemo) radiation in patients with squamous cell cancers of the head and neck—clinical results from the cohort of the clinical cooperation group “Personalized Radiotherapy in Head and Neck Cancer”. Radiat. Oncol. 2018, 13, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Sullivan, B.; Huang, S.H.; Siu, L.L.; Waldron, J.; Zhao, H.; Perez-Ordonez, B.; Weinreb, I.; Kim, J.; Ringash, J.; Bayley, A.; et al. Deintensification candidate subgroups in human papillomavirus-related oropharyngeal cancer according to minimal risk of distant metastasis. J. Clin. Oncol. 2013, 31, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.; Unger, K.; Maihoefer, C.; Schüttrumpf, L.; Wintergerst, L.; Heider, T.; Weber, P.; Marschner, S.; Braselmann, H.; Samaga, D.; et al. A Five-MicroRNA Signature Predicts Survival and Disease Control of Patients with Head and Neck Cancer Negative for HPV-infection. Clin. Cancer Res. 2019, 25, 1505–1516. [Google Scholar] [CrossRef] [Green Version]
- Shen, C.; Nguyen, D.; Zhou, Z.; Jiang, S.B.; Dong, B.; Jia, X. An introduction to deep learning in medical physics: Advantages, potential, and challenges. Phys. Med. Biol. 2020, 65, 05TR01. [Google Scholar] [CrossRef]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; International Union Against Cancer: Geneva, Switzerland, 2011. [Google Scholar]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Ahmaddy, F.; Burgard, C.; Beyer, L.; Koehler, V.; Bartenstein, P.; Fabritius, M.P.; Geyer, T.; Wenter, V.; Ilhan, H.; Spitzweg, C.; et al. 18F-FDG-PET/CT in patients with advanced, radioiodine refractory thyroid cancer treated with lenvatinib. Cancers 2021, 13, 317. [Google Scholar] [CrossRef]
- Fendler, W.P.; Chalkidis, R.P.; Ilhan, H.; Knösel, T.; Herrmann, K.; Issels, R.D.; Bartenstein, P.; Cyran, C.C.; Lindner, L.H.; Hacker, M. Evaluation of several FDG PET parameters for prediction of soft tissue tumour grade at primary diagnosis and recurrence. Eur. Radiol. 2015, 25, 2214–2221. [Google Scholar] [CrossRef] [PubMed]
- Helsen, N.; Van den Wyngaert, T.; Carp, L.; De Bree, R.; VanderVeken, O.M.; De Geeter, F.; Maes, A.; Cambier, J.-P.; Spaepen, K.; Martens, M.; et al. Quantification of 18F-fluorodeoxyglucose uptake to detect residual nodal disease in locally advanced head and neck squamous cell carcinoma after chemoradiotherapy: Results from the ECLYPS study. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, S.; Dijkema, T.; Philippens, M.E.P.; Terhaard, C.H.J.; Hoebers, F.J.P.; Kaanders, J.H.A.M.; Oyen, W.J.G. Tumor to cervical spinal cord standardized uptake ratio (SUR) improves the reproducibility of 18F-FDG-PET based tumor segmentation in head and neck squamous cell carcinoma in a multicenter setting. Radiother. Oncol. 2019, 130, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.; Pak, K.; Kim, I.J.; Kim, B.S.; Kim, S.J. Prognostic Value of Tumor-to-Blood Standardized Uptake Ratio in Patients with Resectable Non-Small-Cell Lung Cancer. Nucl. Med. Mol. Imaging 2017, 51, 233–239. [Google Scholar] [CrossRef] [PubMed]
- McInnes, L.; Healy, J.; Melville, J. UMAP: Uniform Manifold Approximation and Projection for Dimension Reduction. arXiv 2018, arXiv:1802.03426. [Google Scholar]
- Gensheimer, M.F.; Narasimhan, B. A scalable discrete-time survival model for neural networks. PeerJ 2019, 2019, e6257. [Google Scholar] [CrossRef] [PubMed]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A Simple Way to Prevent Neural Networks from Overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar] [CrossRef] [Green Version]
- Clevert, D.A.; Unterthiner, T.; Hochreiter, S. Fast and accurate deep network learning by exponential linear units (ELUs). In Proceedings of the 4th International Conference on Learning Representations, ICLR 2016, San Juan, Puerto Rico, 2–4 May 2016; pp. 1–14. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Løberg, M.; Kalager, M.; Holme, Ø; Hoff, G.; Adami, H.-O.; Bretthauer, M. Long-Term Colorectal-Cancer Mortality after Adenoma Removal. N. Engl. J. Med. 2014, 371, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Bogowicz, M.; Riesterer, O.; Stark, L.S.; Studer, G.; Unkelbach, J.; Guckenberger, M.; Tanadini-Lang, S. Comparison of PET and CT radiomics for prediction of local tumor control in head and neck squamous cell carcinoma. Acta Oncol. 2017, 56, 1531–1536. [Google Scholar] [CrossRef] [Green Version]
- Ger, R.B.; Zhou, S.; Elgohari, B.; Elhalawani, H.; Mackin, D.M.; Meier, J.G.; Nguyen, C.M.; Anderson, B.M.; Gay, C.; Ning, J.; et al. Radiomics features of the primary tumor fail to improve prediction of overall survival in large cohorts of CT- and PET-imaged head and neck cancer patients. PLoS ONE 2019, 14, e0222509. [Google Scholar] [CrossRef] [PubMed]
- Parmar, C.; Leijenaar, R.T.H.; Grossmann, P.; Velazquez, E.R.; Bussink, J.; Rietveld, D.; Rietbergen, M.M.; Haibe-Kains, B.; Lambin, P.; Aerts, H.J.W.L. Radiomic feature clusters and Prognostic Signatures specific for Lung and Head &neck cancer. Sci. Rep. 2015, 5, 11044. [Google Scholar] [CrossRef]
- Haury, A.C.; Gestraud, P.; Vert, J.P. The influence of feature selection methods on accuracy, stability and interpretability of molecular signatures. PLoS ONE 2011, 6, e28210. [Google Scholar] [CrossRef]
- Austin, P.C.; Hux, J.E. A brief note on overlapping confidence intervals. J. Vasc. Surg. 2002, 36, 194–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, H.; Healy, M.J.R. The Graphical Presentation of a Collection of Means. J. R. Stat. Soc. Ser. A 1995, 158, 175. [Google Scholar] [CrossRef]
- Morin, O.; Vallières, M.; Jochems, A.; Woodruff, H.C.; Valdes, G.; Braunstein, S.E.; Wildberger, J.E.; Villanueva-Meyer, J.E.; Kearney, V.; Yom, S.S.; et al. A Deep Look Into the Future of Quantitative Imaging in Oncology: A Statement of Working Principles and Proposal for Change. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1074–1082. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The image biomarker standardization initiative: Standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Avanzo, M.; Stancanello, J.; El Naqa, I. Beyond imaging: The promise of radiomics. Phys. Med. 2017, 38, 122–139. [Google Scholar] [CrossRef] [PubMed]
- Bottaci, L.; Drew, P.J.; Hartley, J.E.; Hadfield, M.B.; Farouk, R.; Lee, P.W.R.; Macintyre, I.M.; Duthie, G.S.; Monson, J.R. Artificial neural networks applied to outcome prediction for colorectal cancer patients in separate institutions. Lancet 1997, 350, 469–472. [Google Scholar] [CrossRef]
- Bostwick, D.G.; Burke, H.B. Prediction of individual patient outcome in cancer: Comparison of artificial neural networks and Kaplan-Meier methods. Cancer 2001, 91, 1643–1646. [Google Scholar] [CrossRef]
- Deist, T.M.; Dankers, F.J.W.M.; Valdes, G.; Wijsman, R.; Hsu, I.C.; Oberije, C.; Lustberg, T.; van Soest, J.; Hoebers, F.; Jochems, A.; et al. Machine learning algorithms for outcome prediction in (chemo)radiotherapy: An empirical comparison of classifiers. Med. Phys. 2018, 45, 3449–3459. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, Z.; Li, Y.; Chen, Z.; Lu, P.; Wang, W.; Liu, W.; Yu, L. Comparison of machine learning methods for classifying mediastinal lymph node metastasis of non-small cell lung cancer from 18F-FDG PET/CT images. EJNMMI Res. 2017, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.; Zhu, X.; Garmire, L.X. Cox-nnet: An artificial neural network method for prognosis prediction on high-throughput omics data. BioRxiv 2016, 093021. [Google Scholar] [CrossRef]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef]

| Literature Only (LO) | Literature + PET (LP) | |
|---|---|---|
| Clinical values | Age at diagnosis | Age at diagnosis |
| Gender | Gender | |
| T-Stage | T-Stage | |
| N-Stage | N-Stage | |
| Tumor grading | Tumor grading | |
| HPV-status | HPV-status | |
| Smoking status | Smoking status | |
| PET values | none | SUV40max |
| SUV40peak | ||
| SUV40TLG | ||
| SURmax Liver | ||
| SURmax Spine | ||
| SURmax Aorta | ||
| SUVmean Liver | ||
| SUVmean Spine | ||
| SUVmean Aorta |
| Endpoint | Model | UMAP | ANN | |||
|---|---|---|---|---|---|---|
| Nearest Neighbors | Number of Features | Learning Rate | Number of Hidden Layers | Neurons per Hidden Layer | ||
| OS | UMAP + ANN | 5 | 50 | 1 × 10−3 | 2 | 10 |
| LO + ANN | - | - | 1 × 10−4 | 2 | 10 | |
| LP + ANN | - | - | 1 × 10−3 | 2 | 5 | |
| LRF | UMAP + ANN | 50 | 15 | 1 × 10−4 | 1 | 10 |
| LO + ANN | - | - | 5 × 10−4 | 2 | 10 | |
| LP + ANN | - | - | 1 × 10−4 | 2 | 15 | |
| Endpoint | Model | 3-Fold Cross-Validation HCI | Median Testing HCI (83% Confidence Interval) |
|---|---|---|---|
| OS | UMAP + ANN | 0.63; 0.59; 0.64 | 0.64 (0.56–0.72) |
| LO + ANN | 0.59; 0.65; 0.66 | 0.67 (0.58–0.75) | |
| LP + ANN | 0.58; 0.66; 0.59 | 0.71 (0.64–0.78) | |
| LRF | UMAP + ANN | 0.55; 0.76, 0.62 | 0.62 (0.50–0.75) |
| LO + ANN | 0.55; 0.59; 0.64 | 0.70 (0.56–0.80) | |
| LP + ANN | 0.56; 0.55; 0.64 | 0.65 (0.54–0.76) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marschner, S.N.; Lombardo, E.; Minibek, L.; Holzgreve, A.; Kaiser, L.; Albert, N.L.; Kurz, C.; Riboldi, M.; Späth, R.; Baumeister, P.; et al. Risk Stratification Using 18F-FDG PET/CT and Artificial Neural Networks in Head and Neck Cancer Patients Undergoing Radiotherapy. Diagnostics 2021, 11, 1581. https://doi.org/10.3390/diagnostics11091581
Marschner SN, Lombardo E, Minibek L, Holzgreve A, Kaiser L, Albert NL, Kurz C, Riboldi M, Späth R, Baumeister P, et al. Risk Stratification Using 18F-FDG PET/CT and Artificial Neural Networks in Head and Neck Cancer Patients Undergoing Radiotherapy. Diagnostics. 2021; 11(9):1581. https://doi.org/10.3390/diagnostics11091581
Chicago/Turabian StyleMarschner, Sebastian N., Elia Lombardo, Lena Minibek, Adrien Holzgreve, Lena Kaiser, Nathalie L. Albert, Christopher Kurz, Marco Riboldi, Richard Späth, Philipp Baumeister, and et al. 2021. "Risk Stratification Using 18F-FDG PET/CT and Artificial Neural Networks in Head and Neck Cancer Patients Undergoing Radiotherapy" Diagnostics 11, no. 9: 1581. https://doi.org/10.3390/diagnostics11091581