
Current Trends and Controversies in the Management of Warthin Tumor of the Parotid Gland †

 , , ,
, , , 
 , , ,
, , ,  , , , , , ,
, , , , , , 
Abstract
:1. Introduction
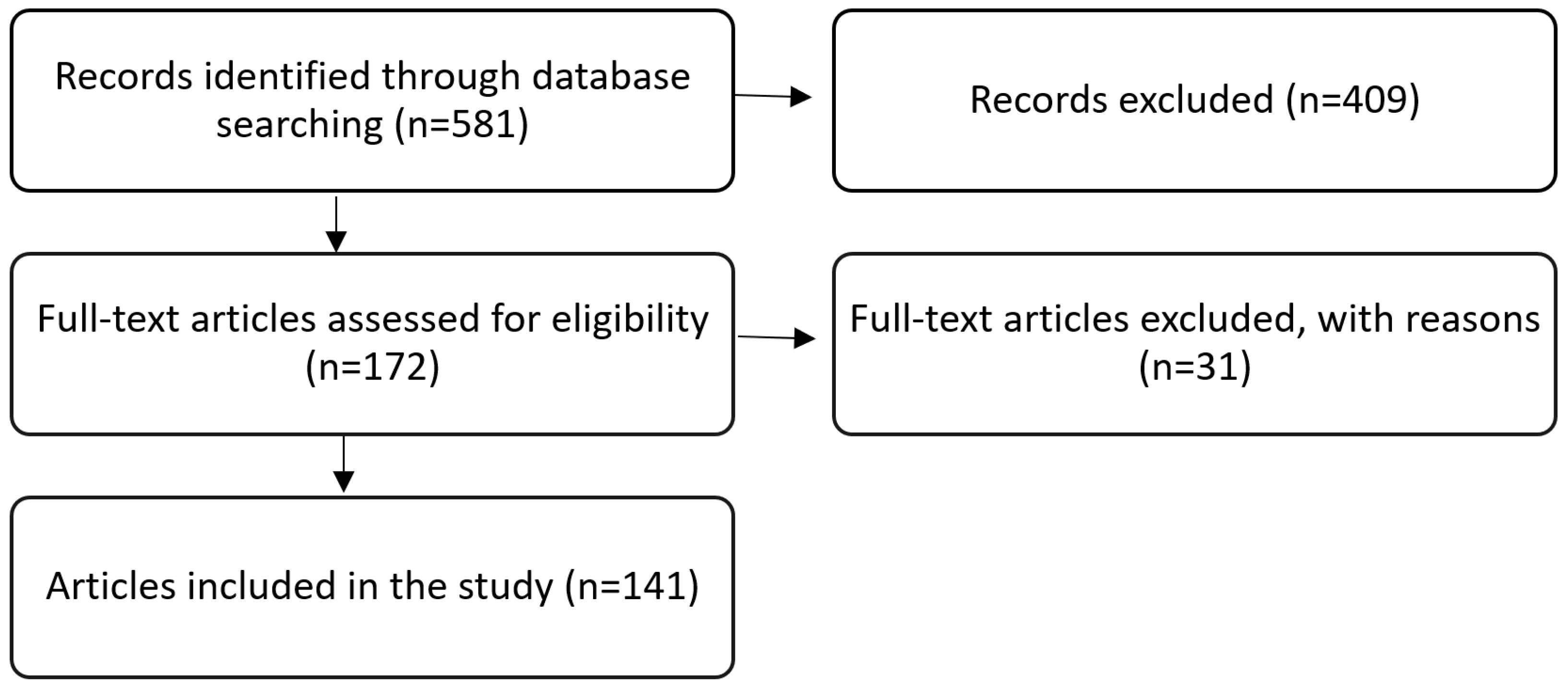
2. Methods
3. Epidemiology
4. Diagnosis of Warthin Tumors (WT)
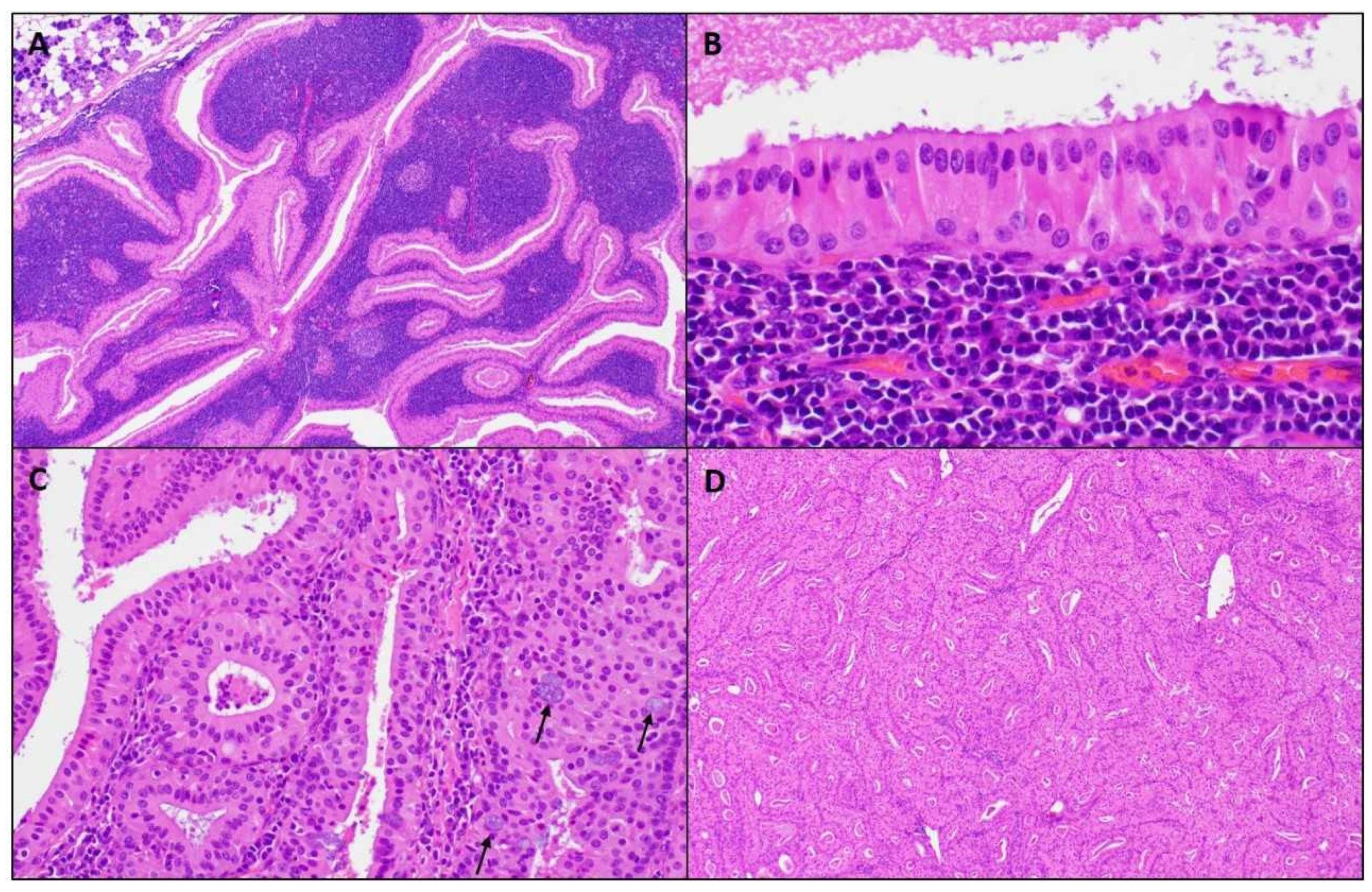
5. Diagnostic Pathology
6. Primary Surgical Excision
7. Extent of Surgery
7.1. Parotidectomy I–IV (Total Parotidectomy)
7.2. Parotidectomy I–II (Lateral Parotidectomy)
7.3. Parotidectomy II (Partial Lateral Parotidectomy)
7.4. Extracapsular Dissection (ECD)
7.5. Capsular Dissection (CD)
8. Active Surveillance (AS)
9. Alternatives to Surgery and AS
9.1. Microwave Ablation (MWA)
9.2. Radiofrequency Ablation (RFA)
9.3. Ultrasound-Guided Ethanol Sclerotherapy (UGES)
10. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- El-Naggar, A.K.; Takata, J.K.C.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Quer, M.; Guntinas-Lichius, O.; Marchal, F.; Poorten, V.V.; Chevalier, D.; León, X.; Eisele, D.; Dulguerov, P. Classification of parotidectomies: A proposal of the European Salivary Gland Society. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3307–3312. [Google Scholar] [CrossRef] [PubMed]
- Franzen, A.M.; Coordes, A.; Franzen, C.K.; Guenzel, T. Are Multiple Tumors of the Parotid Gland Uncommon or Underestimated? Anticancer. Res. 2018, 37, 5263–5267. [Google Scholar] [CrossRef] [Green Version]
- Zaccarini, D.J.; Khurana, K.K. Incidence of Non-Salivary Gland Neoplasms in Patients with Warthin Tumor: A Study of 73 Cases. Head Neck Pathol. 2019, 14, 412–418. [Google Scholar] [CrossRef]
- Ferlito, A.; Bertino, G.; Rinaldo, A.; Mannarà, G.M.; Devaney, K.O. A review of heterotopia and associated salivary gland neoplasms of the head and neck. J. Laryngol. Otol. 1999, 113, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Ethunandan, M.; Pratt, C.; Higgins, B.; Morrison, A.; Umar, T.; MacPherson, D.; Wilson, A. Factors influencing the occurrence of multicentric and ‘recurrent’ Warthin’s tumour: A cross sectional study. Int. J. Oral Maxillofac. Surg. 2008, 37, 831–834. [Google Scholar] [CrossRef] [PubMed]
- Borsetto, D.; Fussey, J.M.; Cazzador, D.; Smith, J.; Ciorba, A.; Pelucchi, S.; Donà, S.; Boscolo-Rizzo, P.; Tomasoni, M.; Lombardi, D.; et al. The diagnostic value of cytology in parotid Warthin’s tumors: International multicenter series. Head Neck 2019, 42, 522–529. [Google Scholar] [CrossRef]
- Warthin, A.S. Papillary Cystadenoma Lymphomatosum. A Rare Teratoid of the Parotid Region. J. Cancer Res. 1929, 13, 116–125. [Google Scholar]
- Patel, D.K.; Morton, R.P. Demographics of benign parotid tumours: Warthin’s tumour versus other benign salivary tumours. Acta Oto-Laryngol. 2015, 136, 83–86. [Google Scholar] [CrossRef]
- Luers, J.; Guntinas-Lichius, O.; Klussmann, J.; Küsgen, C.; Beutner, D.; Grosheva, M. The incidence of Warthin tumours and pleomorphic adenomas in the parotid gland over a 25-year period. Clin. Otolaryngol. 2016, 41, 793–797. [Google Scholar] [CrossRef]
- Franzen, A.M.; Franzen, C.K.; Guenzel, T.; Lieder, A. Increased incidence of Warthin tumours of the parotid gland: A 42-year evaluation. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 2593–2598. [Google Scholar] [CrossRef]
- Psychogios, G.; Vlastos, I.; Thölken, R.; Zenk, J. Warthin’s tumour seems to be the most common benign neoplasm of the parotid gland in Germany. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2081–2084. [Google Scholar] [CrossRef]
- Stryjewska-Makuch, G.; Kolebacz, B.; Janik, M.A.; Wolnik, A. Increase in the incidence of parotid gland tumors in the years 2005–2014. Otolaryngol. Polska 2017, 71, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Tunç, O.; Gönüldaş, B.; Arslanhan, Y.; Kanlıkama, M. Change in Warthin’s tumor incidence: A 20-year joinpoint trend analysis. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 3431–3434. [Google Scholar] [CrossRef] [PubMed]
- Kadletz, L.; Grasl, S.; Perisanidis, C.; Grasl, M.C.; Erovic, B.M. Rising incidences of Warthin’s tumors may be linked to obesity: A single-institutional experience. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 1191–1196. [Google Scholar] [CrossRef]
- Bothe, C.; Fernandez, A.; Quer, M.; Lop, J. Parotid Incidentaloma Identified by Positron Emission/Computed Tomography: When to Consider Diagnoses Other than Warthin Tumor. Int. Arch. Otorhinolaryngol. 2015, 19, 112–115. [Google Scholar]
- Sagiv, D.; Witt, R.L.; Glikson, E.; Mansour, J.; Shalmon, B.; Yakirevitch, A.; Wolf, M.; Alon, E.E.; Slonimsky, G.; Talmi, Y.P. Warthin tumor within the superficial lobe of the parotid gland: A suggested criterion for diagnosis. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1993–1996. [Google Scholar] [CrossRef]
- Klijanienko, J.; Vielh, P. Fine-needle sampling of salivary gland lesions. II. Cytology and histology correlation of 71 cases of Warthin’s tumor (adenolymphoma). Diagn Cytopathol. 1997, 16, 221–225. [Google Scholar] [CrossRef]
- Ballo, M.S.; Shin, H.J.C.; Sneige, N. Sources of diagnostic error in the fine-needle aspiration diagnosis of Warthin’s tumor and clues to a correct diagnosis. Diagn. Cytopathol. 1997, 17, 230–234. [Google Scholar] [CrossRef]
- Faquin, W.C.; Rossi, E.D.; Baloch, Z.; Barkan, G.A.; Foschini, M.; Kurtycz, D.F.I.; Pusztaszeri, M.; Vielh, P. The Milan System for Reporting Salivary Gland Cytopathology; Springer International Publishing: Berlin, Germany, 2018. [Google Scholar]
- Allison, D.B.; Smith, A.P.; An, D.; Miller, J.A.; Shafique, K.; Song, S.; Viswanathan, K.; Eykman, E.; Rao, R.A.; Wiles, A.; et al. Assessing the diagnostic accuracy for pleomorphic adenoma and Warthin tumor by employing the Milan System for Reporting Salivary Gland Cytopathology: An international, multi-institutional study. Cancer Cytopathol. 2021, 129, 43–52. [Google Scholar] [CrossRef]
- Di Palma, S.; Simpson, R.H.; Skálová, A.; Michal, M. Metaplastic (infarcted) Warthin’s tumour of the parotid gland: A possible consequence of fine needle aspiration biopsy. Histopathology 1999, 35, 432–438. [Google Scholar] [CrossRef] [Green Version]
- Skálová, A.; Vanecek, T.; Simpson, R.H.W.; Vazmitsel, M.A.; Majewska, H.; Mukensnabl, P.; Hauer, L.; Andrle, P.; Hosticka, L.; Grossmann, P.; et al. CRTC1-MAML2 and CRTC3-MAML2 Fusions Were Not Detected in Metaplastic Warthin Tumor and Metaplastic Pleomorphic Adenoma of Salivary Glands. Am. J. Surg. Pathol. 2013, 37, 1743–1750. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, K.; Ito, Y.; Masaki, A.; Fujii, K.; Beppu, S.; Sakakibara, T.; Takino, H.; Takase, H.; Ijichi, K.; Shimozato, K.; et al. Warthin-like Mucoepidermoid Carcinoma. Am. J. Surg. Pathol. 2015, 39, 1479–1487. [Google Scholar] [CrossRef]
- Bieńkowski, M.; Kunc, M.; Iliszko, M.; Kuźniacka, A.; Studniarek, M.; Biernat, W. MAML2 rearrangement as a useful diagnostic marker discriminating between Warthin tumour and Warthin-like mucoepidermoid carcinoma. Virchows Arch. 2020, 477, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Palmer, T.; Gleeson, M.; Eveson, J.; Cawson, R. Oncocytic adenomas and oncocytic hyperplasia of salivary glands: A clinicopathological study of 26 cases. Histopathology 2007, 16, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Thompson, L.; Wenig, B.M.; Ellis, G.L. Oncocytomas of the submandibular gland: A series of 22 cases and a review of the literature. Cancer 1996, 78, 2281–2287. [Google Scholar] [CrossRef]
- Quer, M.; Poorten, V.V.; Takes, R.P.; Silver, C.E.; Boedeker, C.C.; De Bree, R.; Rinaldo, A.; Sanabria, A.; Shaha, A.R.; Pujol, A.; et al. Surgical options in benign parotid tumors: A proposal for classification. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 3825–3836. [Google Scholar] [CrossRef]
- Psychogios, G.; Bohr, C.; Constantinidis, J.; Canis, M.; Poorten, V.V.; Plzak, J.; Knopf, A.; Betz, C.; Guntinas-Lichius, O.; Zenk, J. Review of surgical techniques and guide for decision making in the treatment of benign parotid tumors. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 15–29. [Google Scholar] [CrossRef]
- Hung, C.-J.; Kang, B.-H.; Wang, J.-S.; Lin, Y.-S. Ulcerative Warthin Tumor: A Case Report and Review of the Literature. Ear Nose Throat J. 2020, 386, 1–4. [Google Scholar] [CrossRef]
- Witt, R.L.; Iacocca, M.; Gerges, F. Contemporary diagnosis and management of Warthin’s tumor. Del. Med. J. 2015, 87, 13–16. [Google Scholar]
- Gant, T.D.; Hovey, L.M.; Williams, C. Surgical Management of Parotid Gland Tumors. Ann. Plast. Surg. 1981, 6, 389–392. [Google Scholar] [CrossRef]
- Lee, D.H.; Yoon, T.M.; Lee, J.K.; Lim, S.C. Surgical treatment strategy in Warthin tumor of the parotid gland. Braz. J. Otorhinolaryngol. 2019, 85, 546–550. [Google Scholar] [CrossRef]
- Maiorano, E.; Muzio, L.L.; Favia, G.; Piattelli, A. Warthin’ s tumour: A study of 78 cases with emphasis on bilaterality, multifocality and association with other malignancies. Oral Oncol. 2002, 38, 35–40. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Koch, M.; Goncalves, M.; Iro, H. Investigation of the surgical strategies for unilateral multifocal cystadenolymphomas of the parotid gland. Oral Oncol. 2018, 82, 176–180. [Google Scholar] [CrossRef]
- Chulam, T.C.; Francisco, A.L.N.; Filho, J.G.; Alves, C.A.P.; Kowalski, L.P. Warthin’ s tumour of the parotid gland: Our experience. Acta Otorhinolaryngol. Ital. 2013, 33, 393–397. [Google Scholar]
- Leverstein, H.; Van Der Wal, J.; Tiwari, R.; Van Der Waal, I.; Snow, G. Results of the surgical management and histopathological evaluation of 88 parotid gland Warthin’s tumours. Clin. Otolaryngol. 1997, 22, 500–503. [Google Scholar] [CrossRef]
- Lee, D.H.; Yoon, T.M.; Lee, J.K.; Lim, S.C. Extracapsular dissection for Warthin tumor in the tail of parotid gland. Acta Oto-Laryngol. 2017, 137, 1007–1009. [Google Scholar] [CrossRef] [PubMed]
- Iwai, H.; Yamashita, T. Local excision procedure for Warthin’s tumor of the parotid gland. Otolaryngol. Neck Surg. 2005, 132, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Mantsopoulos, K.; Goncalves, M.; Koch, M.; Iro, H. Extracapsular dissection for warthin tumors despite the risk of ipsilateral metachronous occurrence. Laryngoscope 2018, 128, 2521–2524. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Goncalves, M.; Koch, M.; Traxdorf, M.; Schapher, M.; Iro, H. Going beyond extracapsular dissection in cystadenolymphomas of the parotid gland. Oral Oncol. 2019, 88, 168–171. [Google Scholar] [CrossRef]
- McMullen, C.P.; Smith, R.V.; Ow, T.J.; Tassler, A.; Schiff, B.A. Minimal Margin Extracapsular Dissection. Ann. Otol. Rhinol. Laryngol. 2016, 125, 912–917. [Google Scholar] [CrossRef]
- Teymoortash, A.; Krasnewicz, Y.; Werner, J. Clinical features of cystadenolymphoma (Warthin’s tumor) of the parotid gland: A retrospective comparative study of 96 cases. Oral Oncol. 2006, 42, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Mantsopoulos, K.; Goncalves, M.; Koch, M.; Iro, H. Watchful waiting in carefully selected metachronous cystadenolymphomas of the parotid gland: A reliable option? Br. J. Oral Maxillofac. Surg. 2019, 57, 425–429. [Google Scholar] [CrossRef]
- Mann, L.; Crosher, R.; Steel, C. Warthin’s tumour–Resolution following FNA. Int. J. Surg. Case Rep. 2014, 5, 471–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klussmann, J.P.; Wittekindt, C.; Preuss, S.F.; Al Attab, A.; Schroeder, U.; Guntinas-Lichius, O. High risk for bilateral Warthin tumor in heavy smokers–review of 185 cases. Acta Oto-Laryngol. 2006, 126, 1213–1217. [Google Scholar] [CrossRef]
- Schwalje, A.T.; Uzelac, A.; Ryan, W.R. Growth rate characteristics of Warthin’s tumours of the parotid gland. Int. J. Oral Maxillofac. Surg. 2015, 44, 1474–1479. [Google Scholar] [CrossRef]
- Jin, M.; Fu, J.; Lu, J.; Xu, W.; Chi, H.; Wang, X.; Cong, Z. Ultrasound-guided percutaneous microwave ablation of parotid gland adenolymphoma. Medicine 2019, 98, e16757. [Google Scholar] [CrossRef]
- Tung, Y.-C.; Luo, S.-D.; Su, Y.-Y.; Chen, W.-C.; Chen, H.-L.; Cheng, K.-L.; Lin, W.-C. Evaluation of Outcomes following Radiofrequency Ablation for Treatment of Parotid Tail Warthin Tumors. J. Vasc. Interv. Radiol. 2019, 30, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Mamidi, I.S.; Lee, E.; Benito, D.A.; Li, L.; Goodman, J.F.; Thakkar, P.G.; Joshi, A. Ultrasound-guided ethanol sclerotherapy for non-surgical treatment of Warthin’s tumor. Am. J. Otolaryngol. 2021, 42, 102813. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
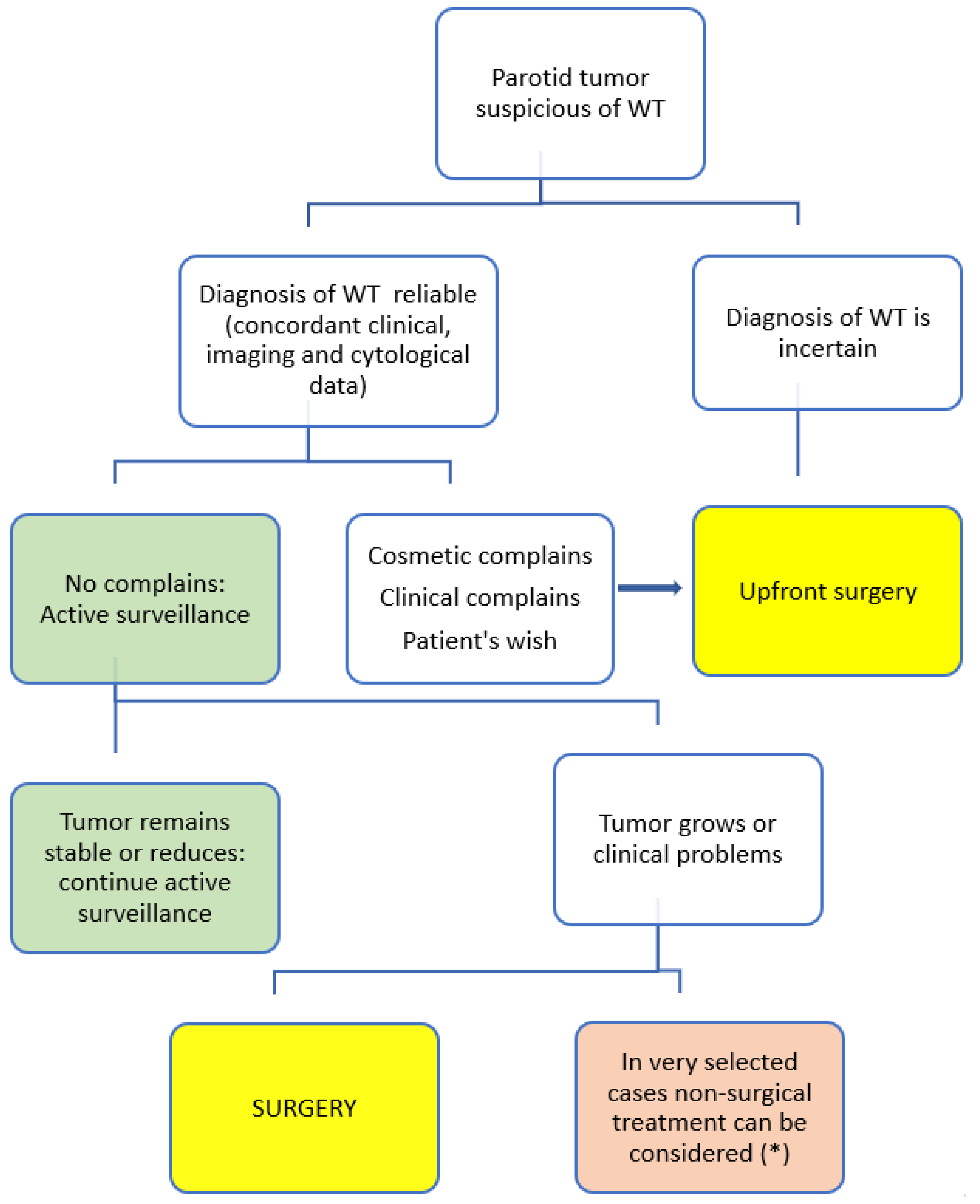
| Clinical Scenarios | Comments |
|---|---|
| 1. Diagnosis of WT is not reliable | A reliable diagnosis must be based on concordant clinical, image, and cytological data |
| 2. Cosmetic concerns | When the WT grows considerably causing cosmetic complaints, surgery is the best option |
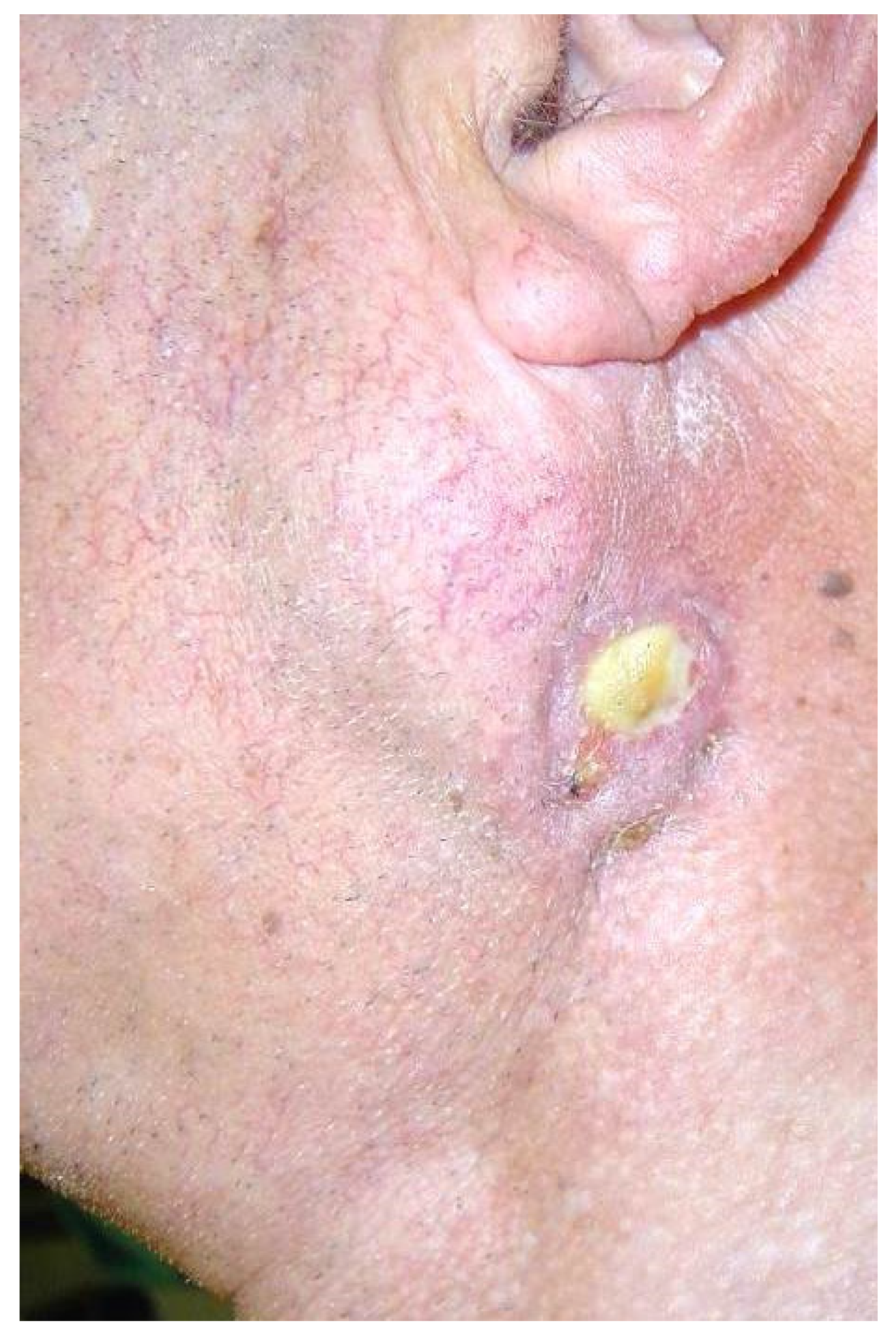
| 3. Clinical complaints: pain, ulceration, or recurrent infection | When the WT is painful or ulcerates, surgery is advised. |
| 4. Patient’s wishes |
| WT | Resections Proposed |
|---|---|
| Only one lesion category I or II (*) | Parotidectomy II (partial parotidectomy) or ECD |
| Only one lesion category III or IV (*) intraparotid | Parotidectomy adapted to the extension of the lesions |
| Only one lesion of more than 3 cm in parotid tail, but extending mainly to the extraparotid | Parotidectomy II (partial lateral parotidectomy) or ECD |
| Multiple lesions affecting superficial parotid | Parotidectomy I and II (lateral or superficial parotidectomy) |
| Multiple lesions affecting superficial and deep lobe | Parotidectomy I–II–III–IV (total parotidectomy) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quer, M.; Hernandez-Prera, J.C.; Silver, C.E.; Casasayas, M.; Simo, R.; Vander Poorten, V.; Guntinas-Lichius, O.; Bradley, P.J.; Tong-Ng, W.; Rodrigo, J.P.; et al. Current Trends and Controversies in the Management of Warthin Tumor of the Parotid Gland. Diagnostics 2021, 11, 1467. https://doi.org/10.3390/diagnostics11081467
Quer M, Hernandez-Prera JC, Silver CE, Casasayas M, Simo R, Vander Poorten V, Guntinas-Lichius O, Bradley PJ, Tong-Ng W, Rodrigo JP, et al. Current Trends and Controversies in the Management of Warthin Tumor of the Parotid Gland. Diagnostics. 2021; 11(8):1467. https://doi.org/10.3390/diagnostics11081467
Chicago/Turabian StyleQuer, Miquel, Juan C. Hernandez-Prera, Carl E. Silver, Maria Casasayas, Ricard Simo, Vincent Vander Poorten, Orlando Guntinas-Lichius, Patrick J. Bradley, Wai Tong-Ng, Juan P. Rodrigo, and et al. 2021. "Current Trends and Controversies in the Management of Warthin Tumor of the Parotid Gland" Diagnostics 11, no. 8: 1467. https://doi.org/10.3390/diagnostics11081467