
A Comparison of Lung Ultrasound and Computed Tomography in the Diagnosis of Patients with COVID-19: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,
Abstract
:1. Background
2. Methods
2.1. Inclusion and Exclusion Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Search Strategy
2.3. Article Selection and Data Extraction
2.4. Assessment of Risk of Bias and Quality of Evidence
2.5. Statistical Analysis
3. Results
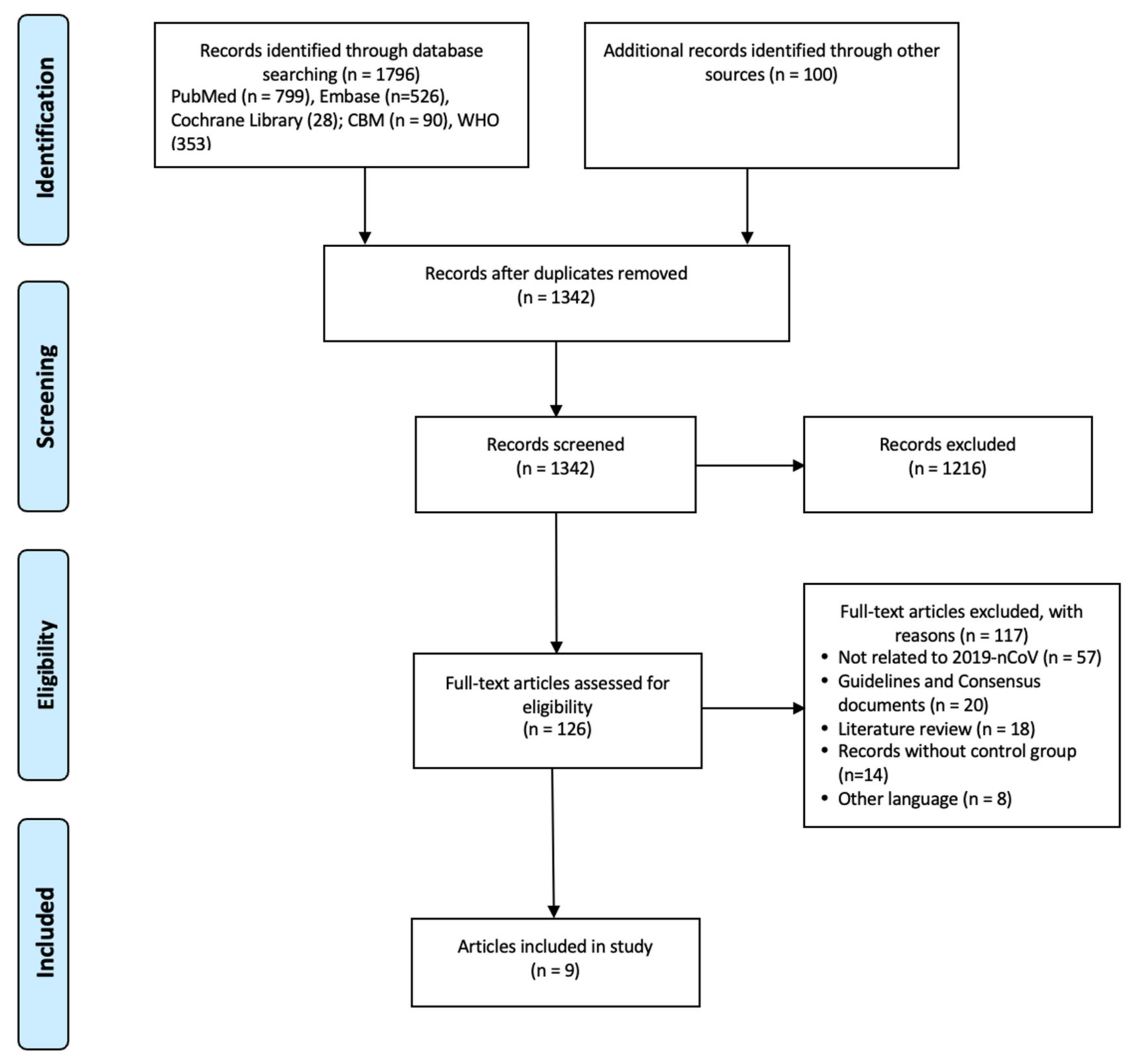
3.1. Literature Selection Process
3.2. Characteristics of the Included Studies
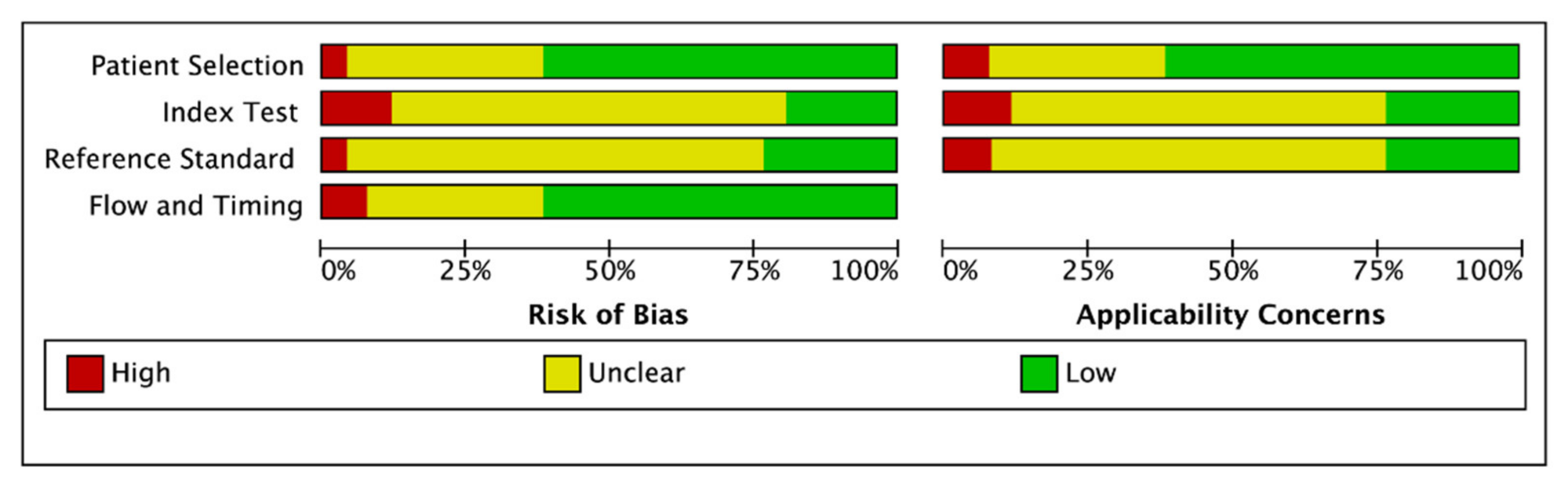
3.3. Risk of Bias in the Included Studies
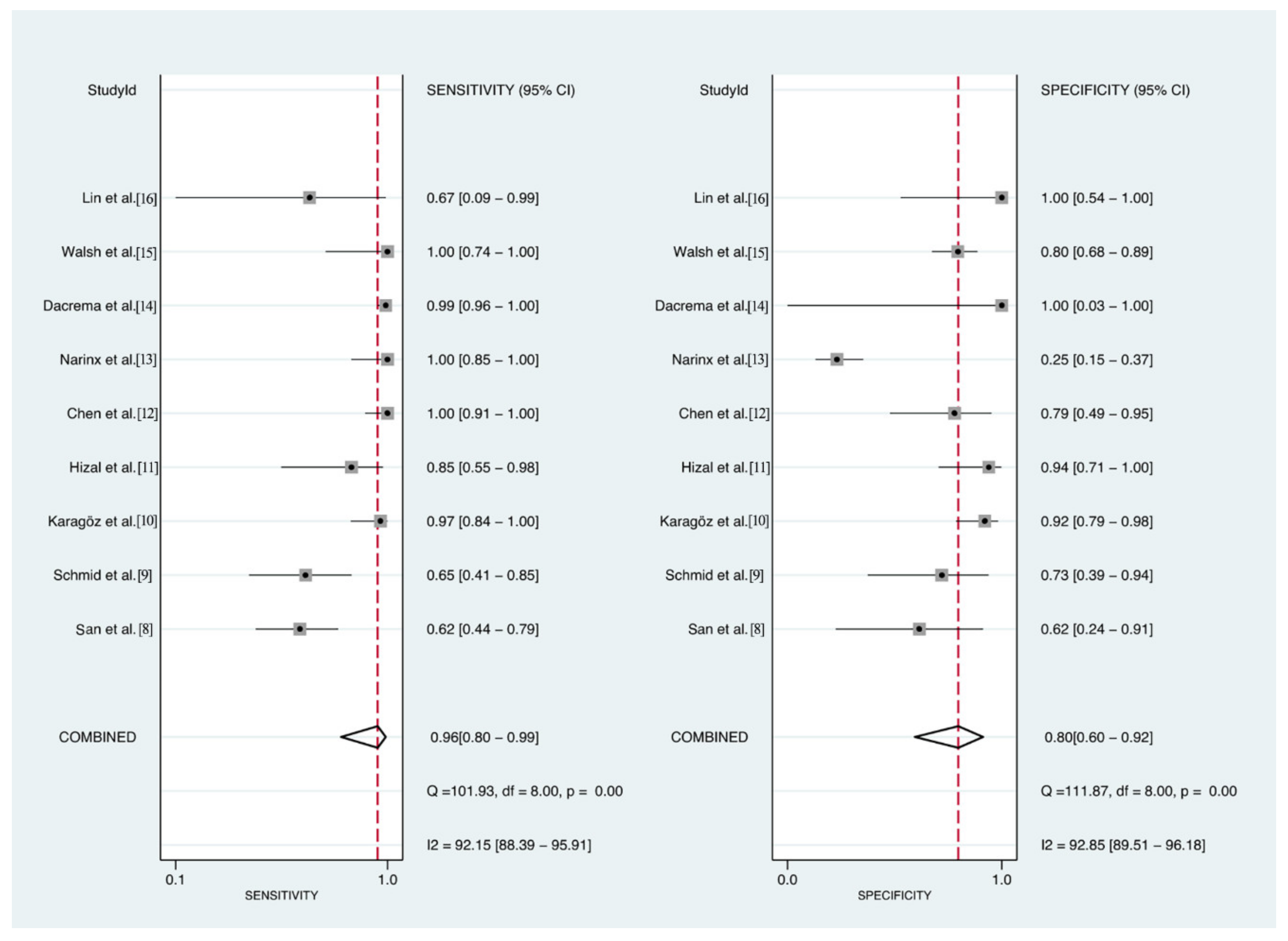
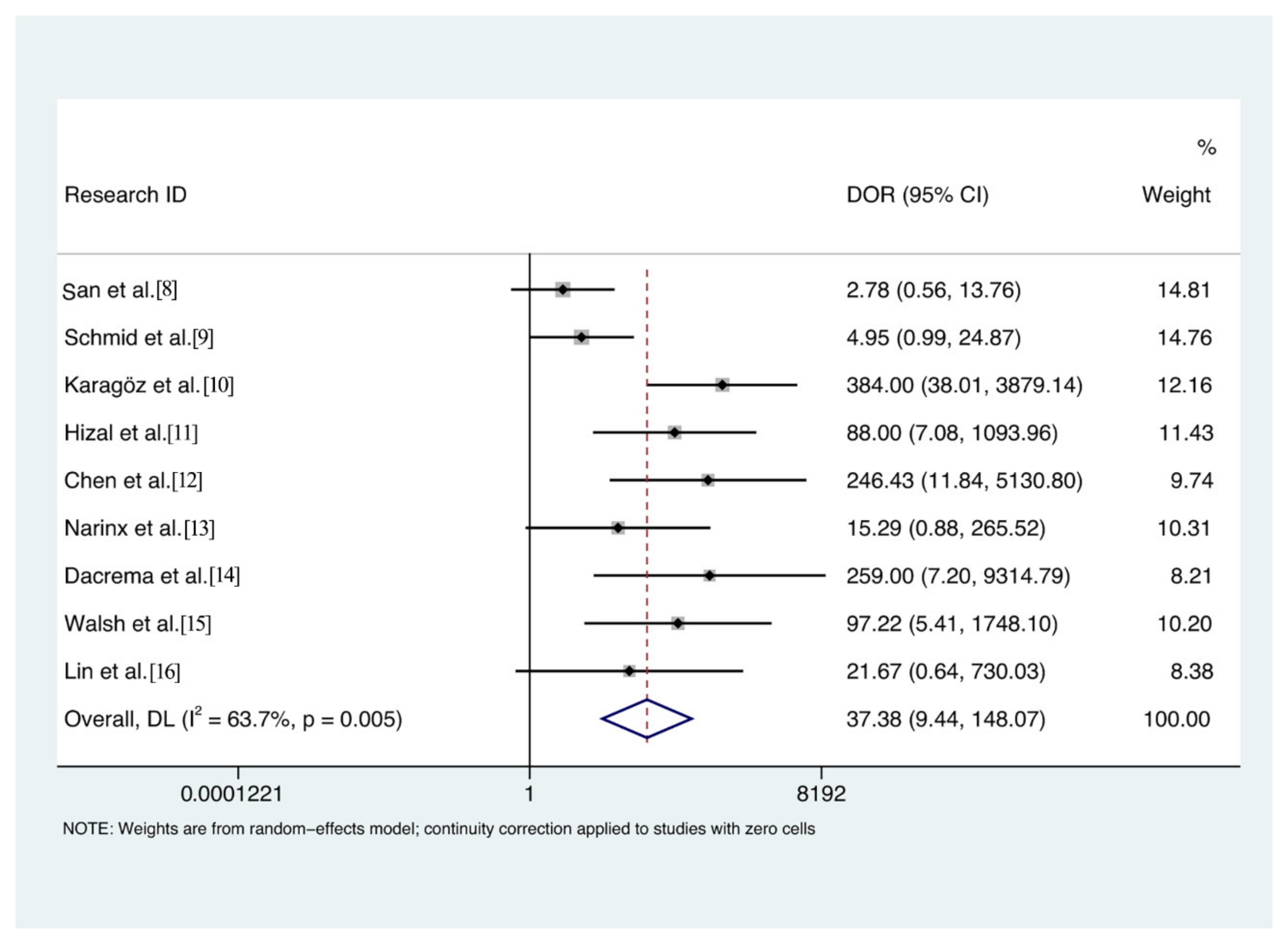
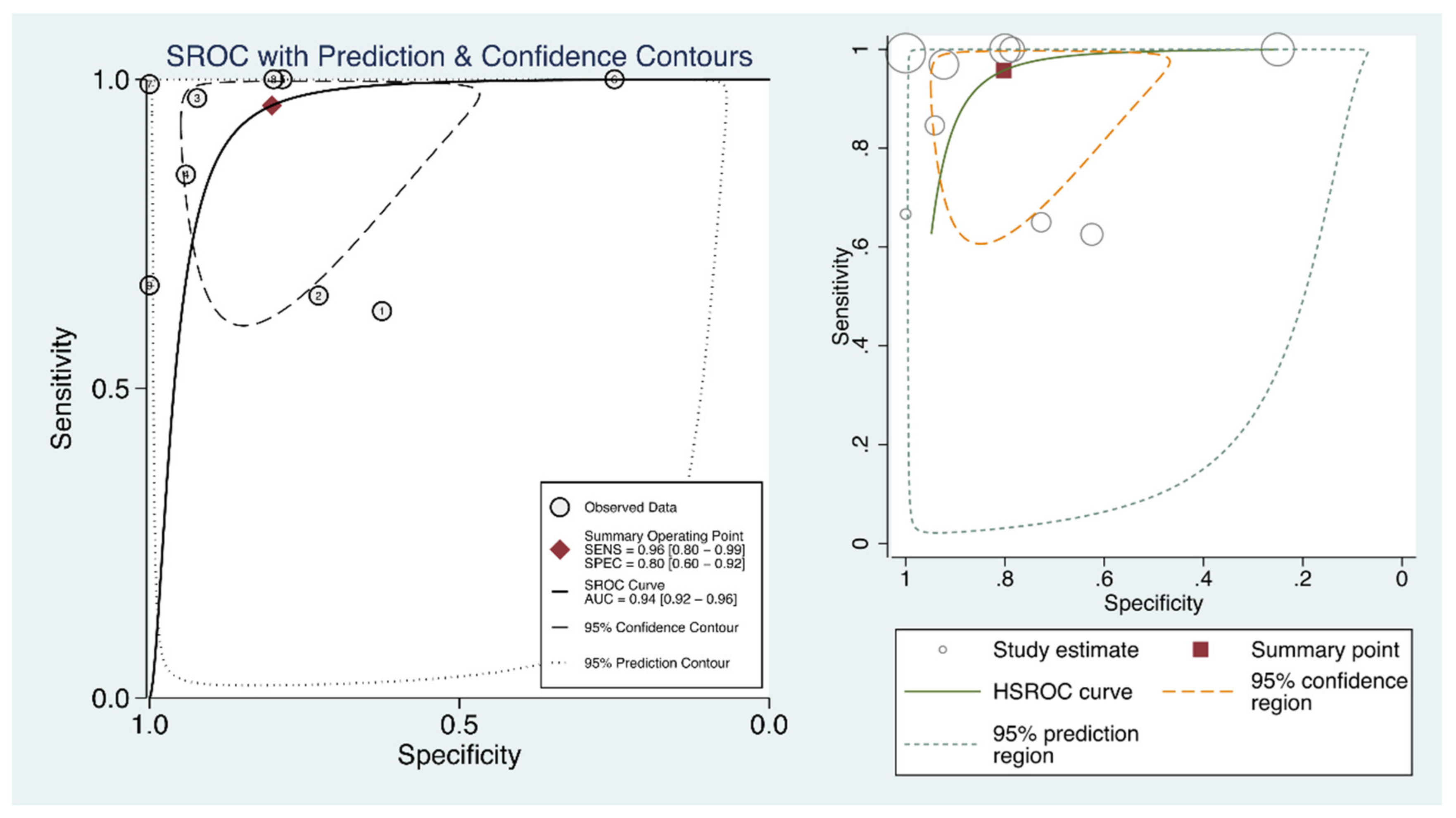
3.4. Agreement of LUS for the Diagnosis of COVID-19
4. Discussion
4.1. Principal Findings
4.2. Strengths and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Goudouris, E.S. Laboratory diagnosis of COVID-19. J. Pediatr. 2021, 97, 7–12. [Google Scholar] [CrossRef]
- Duarte, M.L.; Dos Santos, L.R.; Contenças, A.C.D.S.; Iared, W.; Peccin, M.S.; Atallah, N. Reverse-transcriptase polymerase chain reaction versus chest computed tomography for detecting early symptoms of COVID-19. A diagnostic accuracy systematic review and meta-analysis. Sao Paulo Med. J. 2020, 138, 422–432. [Google Scholar] [CrossRef]
- Soni, N.J.; Franco, R.; Velez, M.I.; Schnobrich, D.; Dancel, R.; Restrepo, M.I.; Mayo, P.H. Ultrasound in the diagnosis and management of pleural effusions. J. Hosp. Med. 2015, 10, 811–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitar, Z.I.; Maadarani, O.S.; El-Shably, A.M.; Al-Ajmi, M.J. Diagnostic accuracy of chest ultrasound in patients with pneumonia in the intensive care unit: A single-hospital study. Heal. Sci. Rep. 2018, 2, e102. [Google Scholar] [CrossRef] [PubMed]
- McInnes, M.D.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388396. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Şan, İ.; Bekgöz, B.; Usul, E.; Yıldırım, Ç.; Gemcioğlu, E.; Kahraman, A.F.; Ay, A.E. Role of lung ultrasonography in the diagnosis of COVID-19 patients admitted to the emergency department. Notf. Rett. 2020, 2, 1–6. [Google Scholar]
- Schmid, B.; Feuerstein, D.; Lang, C.N.; Fink, K.; Steger, R.; Rieder, M.; Duerschmied, D.; Busch, H.J.; Damjanovic, D. Lung ultrasound in the emergency department-a valuable tool in the management of patients presenting with respiratory symptoms during the SARS-CoV-2 pandemic. BMC Emerg. Med. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Karagöz, A.; Sağlam, C.; Demirbaş, H.B.; Korkut, S.; Ünlüer, E.E. Accuracy of Bedside Lung Ultrasound as a Rapid Triage Tool for Suspected Covid-19 Cases. Ultrasound Q. 2020, 36, 339–344. [Google Scholar] [CrossRef]
- Hizal, M.; Aykac, K.; Yayla, B.C.C.; Yilmaz, A.; Altun, D.; Akkaya, H.E.; Bayhan, G.I.; Kurt, A.N.C.; Karakaya, J.; Ozsurekci, Y.; et al. Diagnostic value of lung ultrasonography in children with COVID-19. Pediatr. Pulmonol. 2020, 56, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Tung-Chen, Y.; de Gracia, M.M.; Díez-Tascón, A.; Alonso-González, R.; Agudo-Fernández, S.; Parra, M.; Ossaba-Vélez, S.; Rodríguez-Fuertes, P.; Llamas-Fuentes, R. Correlation between Chest Computed Tomography and Lung Ultrasonography in Patients with Coronavirus Disease 2019 (COVID-19). Ultrasound Med. Biol. 2020, 46, 2918–2926. [Google Scholar] [CrossRef]
- Narinx, N.; Smismans, A.; Symons, R.; Frans, J.; Demeyere, A.; Gillis, M. Feasibility of using point-of-care lung ultrasound for early triage of COVID-19 patients in the emergency room. Emerg. Radiol. 2020, 27, 663–670. [Google Scholar] [CrossRef] [PubMed]
- DaCrema, A.; Silva, M.; Rovero, L.; Vertemati, V.; Losi, G.; Piepoli, M.F.; Sacchi, R.; Mangiacotti, M.; Nazerian, P.; Pagani, L.; et al. A simple lung ultrasound protocol for the screening of COVID-19 pneumonia in the emergency department. Intern. Emerg. Med. 2021, 19, 1–9. [Google Scholar] [CrossRef]
- Walsh, P.; Hankins, A.; Bang, H. Point-of-care Lung Ultrasound Is Useful to Evaluate Emergency Department Patients for COVID-19. West. J. Emerg. Med. 2020, 21, 24–31. [Google Scholar] [CrossRef]
- Lin, H.; Zhang, B.; Kou, H.; Zhao, Y.; Li, K.; Wu, D.; Ren, L.; Chen, Z.; Shan, X.; Huang, Y.; et al. Application Value of Lung Ultrasound in Asymptomatic Patients with Confirmed COVID-19. Adv. Ultrasound Diagn. Ther. 2020, 4, 67–72. [Google Scholar] [CrossRef]
- Testa, A.; Soldati, G.; Copetti, R.; Giannuzzi, R.; Portale, G.; Gentiloni-Silveri, N. Early recognition of the 2009 pandemic influenza A (H1N1) pneumonia by chest ultrasound. Crit. Care 2012, 16, R30. [Google Scholar] [CrossRef] [Green Version]
- Baston, C.; West, T.E. Lung ultrasound in acute respiratory distress syndrome and beyond. J. Thorac. Dis. 2016, 8, E1763–E1766. [Google Scholar] [CrossRef] [Green Version]
- See, K.C.; Ong, V.; Tan, Y.L.; Sahagun, J.; Taculod, J. Chest radiography versus lung ultrasound for identification of acute respiratory distress syndrome: A retrospective observational study. Crit. Care 2018, 22, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ramsingh, D.; Bronshteyn, Y.S.; Haskins, S.; Zimmerman, J. Perioperative Point-of-Care Ultrasound: From Concept to Application. Anesthesiology 2020, 132, 908. [Google Scholar] [CrossRef] [PubMed]
- Zompatori, M.; Ciccarese, F.; Fasano, L. Overview of current lung imaging in acute respiratory distress syndrome. Eur. Respir. Rev. 2014, 23, 519–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahrani, S.A.; Al-Salamah, M.A.; Al-Madani, W.H.; Elbarbary, M.A. Systematic review and meta-analysis for the use of ultrasound versus radiology in diagnosing of pneumonia. Crit. Ultrasound J. 2017, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leopold, S.J.; Ghose, A.; Plewes, K.A.; Mazumder, S.; Pisani, L.; Kingston, H.W.; Paul, S.; Barua, A.; Sattar, M.A.; Huson, M.A.; et al. Point-of-care lung ultrasound for the detection of pulmonary manifestations of malaria and sepsis: An observational study. PLoS ONE 2018, 13, e0204832. [Google Scholar] [CrossRef] [Green Version]
- Bainbridge, D.; McConnell, B.; Royse, C. A review of diagnostic accuracy and clinical impact from the focused use of perioperative ultrasound. Can. J. Anesth. 2018, 65, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.J.; Ha, Y.R.; Oh, J.H.; Cho, Y.S.; Lee, W.W.; Sohn, Y.D.; Cho, G.C.; Koh, C.Y.; Do, H.H.; Jeong, W.J.; et al. Clinical guidance for point-of-care ultrasound in the emergency and critical care areas after implementing insurance coverage in Korea. J. Korean Med. Sci. 2020, 35, 7. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Piano, A.; Raffaelli, F.; Bonadia, N.; Donati, K.D.G.; Franceschi, F. Point-of-Care Lung Ultrasound findings in novel coronavirus disease-19 pnemoniae: A case report and potential applications during COVID-19 outbreak. J. Ultrasound Med. 2020, 24, 2776–2780. [Google Scholar]
- Akl, E.A.; Blažić, I.; Yaacoub, S.; Frija, G.; Chou, R.; Appiah, J.A.; Fatehi, M.; Flor, N.; Hitti, E.; Jafri, H.; et al. Use of chest imaging in the diagnosis and management of COVID-19: A WHO rapid advice guide. Radiology 2020, 298, E63–E69. [Google Scholar] [CrossRef]
- Buerke, M.; Gasser, A.; Suhai, T. Medizinische Klinik–Intensivmedizin und Notfallmedizin. Med. Klin. Intensivmed. Notf. 2011, 106, 5. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.J.; Hayward, S.A.; Innes, S.M.; Miller, A.S. Point-of-care lung ultrasound in patients with COVID-19–a narrative review. Anaesthesia 2020, 75, 1096–1104. [Google Scholar] [CrossRef] [Green Version]
- Convissar, D.L.; Gibson, L.E.; Berra, L.; Bittner, E.A.; Chang, M.G. Narrative Review Article: Application of Lung Ultrasound During the COVID-19 Pandemic: A Narrative Review. Anesth. Analg. 2020, 131, 345. [Google Scholar] [CrossRef]
- Gutiérrez, V.F.; Azcárate, J.A.; Torres, D.P.; Zapata, L.; Yakushev, A.R.; Calvo, A.O. Ultrasound in the management of the critically ill patient with SARS-CoV-2 infection (COVID-19): Narrative review. Med. Intensiva 2020, 2, 11. [Google Scholar]
- Vetrugno, L.; Baciarello, M.; Bignami, E.; Bonetti, A.; Saturno, F.; Orso, D.; Girometti, R.; Cereser, L.; Bove, T. The “pandemic” increase in lung ultrasound use in response to Covid-19: Can we complement computed tomography findings? A narrative review. Ultrasound J. 2020, 12, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Youssef, A.; Cavalera, M.; Azzarone, C.; Serra, C.; Brunelli, E.; Casadio, P.; Pilu, G. The use of lung ultrasound during the COVID-19 pandemic: A narrative review with specific focus on its role in pregnancy. J. Popul. Ther. Clin. Pharmacol. 2020, 27, e64–e75. [Google Scholar] [CrossRef]
- Kharasch, S.; Duggan, N.M.; Cohen, A.R.; Shokoohi, H. Lung Ultrasound in Children with Respiratory Tract Infections: Viral, Bacterial or COVID-19? A Narrative Review. Open Access Emerg. Med. 2020, 12, 275. [Google Scholar] [CrossRef]
- Gandhi, D.; Jain, N.; Khanna, K.; Li, S.; Patel, L.; Gupta, N. Current role of imaging in COVID-19 infection with recent recommendations of point of care ultrasound in the contagion: A narrative review. Ann. Transl. Med. 2020, 8, 1094. [Google Scholar] [CrossRef]
- Gandhi, D.; Ahuja, K.; Grover, H.; Sharma, P.; Solanki, S.; Gupta, N.; Patel, L. Review of X-ray and computed tomography scan findings with a promising role of point of care ultrasound in COVID-19 pandemic. World J. Radiol. 2020, 12, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Szabó, I.A.; Ágoston, G.; Varga, A.; Cotoi, O.S.; Frigy, A. Pathophysiological background and clinical practice of lung ultrasound in COVID-19 patients: A short review. Anatol. J. Cardiol. 2020, 24, 76. [Google Scholar]
- Pata, D.; Valentini, P.; De Rose, C.; De Santis, R.; Morello, R.; Buonsenso, D. Chest Computed Tomography and Lung Ultrasound Findings in COVID-19 Pneumonia: A Pocket Review for Non-radiologists. Front. Med. 2020, 7, 375. [Google Scholar] [CrossRef] [PubMed]
- Buda, N.; Segura-Grau, E.; Cylwik, J.; Wełnicki, M. Lung ultrasound in the diagnosis of COVID-19 infection-A case series and review of the literature. Adv. Med. Sci. 2020, 65, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Sultan, L.R.; Sehgal, C.M. A review of early experience in lung ultrasound in the diagnosis and management of COVID-19. Ultrasound Med. Biol. 2020, 46, 2530–2545. [Google Scholar] [CrossRef]
- Mohamed, M.F.; Al-Shokri, S.; Yousaf, Z.; Danjuma, M.; Parambil, J.; Mohamed, S.; Mubasher, M.; Dauleh, M.M.; Hasanain, B.; AlKahlout, M.A.; et al. Frequency of abnormalities detected by point-of-care lung ultrasound in symptomatic COVID-19 patients: Systematic review and meta-analysis. Am. J. Trop. Med. Hyg. 2020, 103, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhang, D.; Zhou, C.; Huang, H.; Wang, R. Value of lung ultrasound for the diagnosis of COVID-19 pneumonia: A protocol for a systematic review and meta-analysis. BMJ Open 2020, 10, e039180. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research ID | Journals | Country/Area | Publication Date | Patients | Female, N (%) | Age (year) | Patients Enrolled Time | Setting | Sample Size | Ultrasound | CT | TP | FP | FN | TN |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Şan et al. [8] | Notfall and Rettungsmedizin | Turkey | 2 December 2020 | Confirmed COVID-19 | 20 (50.0%) | Mean ± SD 43.8 ± 16.6 | 1–30 April 2020 | ED | 40 | LUS | CT | 20 | 3 | 12 | 5 |
| Schmid et al. [9] | BMC Emergency Medicine | Germany | 7 December 2020 | Suspected COVID-19 | NA | NA | 1–25 April 2020 | ED | 31 | LUS | CT | 13 | 3 | 7 | 8 |
| Karagöz et al. [10] | Ultrasound Quarterly | Turkey | 1 December 2020 | Suspected COVID-19 | 31 (43.0%) | Mean 51 (range 20–96) | 1–15 April 2020 | ED | 72 | BLUS | CT | 32 | 3 | 1 | 36 |
| Hizal et al. [11] | Pediatr Pulmonol | Turkey | 21 October 2020 | Confirmed COVID-19 | NA | Children | April–May 2020 | Hospital | 30 | LUS | CT | 11 | 1 | 2 | 16 |
| Chen et al. [12] | Ultrasound Med Biol | Spain | 13 July 2020 | Confirmed COVID-19 | 23 (45.1%) | Mean ± SD 61.4 ± 17.7 | March–April 2020 | ED | 51 | LUS | CT | 37 | 3 | 0 | 11 |
| Narinx et al. [13] | Emergency Radiology | Belgium | 10 September 2020 | Suspected COVID-19 | 49 (54.4%) | Mean ± SD 50.4 ± 16.3 | 28 March–20 April 2020 | ED | 90 | POCUS | CT | 22 | 51 | 0 | 17 |
| Dacrema et al. [14] | Internal and Emergency Medicine | Italy | 11 January 2021 | Suspected COVID-19 | 32 (24.4%) | Mean ± SD 64.3 ± 14.3 | 21 February–15 March 2020 | ED | 131 | LUS | HRCT | 129 | 0 | 1 | 1 |
| Walsh et al. [15] | Western Journal of Emergency Medicine | USA | 28 September 2020 | COVID-19 | NA | ≥14 | 4 March–19 May 2020 | ED | 77 | LUS | CT | 12 | 13 | 0 | 52 |
| Lin et al. [16] | Advanced Ultrasound in Diagnosis and Therapy | China | 6 September 2020 | Asymptomatic SARS-CoV-2 infected patients | 4 (44.4%) | Mean ± SD 34.0 ± 17.9 | 22–23 February 2020 | Hospital | 9 | LUS | CT | 2 | 0 | 1 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, M.; Luo, X.; Wang, L.; Estill, J.; Lv, M.; Zhu, Y.; Wang, Q.; Xiao, X.; Song, Y.; Lee, M.S.; et al. A Comparison of Lung Ultrasound and Computed Tomography in the Diagnosis of Patients with COVID-19: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 1351. https://doi.org/10.3390/diagnostics11081351
Wang M, Luo X, Wang L, Estill J, Lv M, Zhu Y, Wang Q, Xiao X, Song Y, Lee MS, et al. A Comparison of Lung Ultrasound and Computed Tomography in the Diagnosis of Patients with COVID-19: A Systematic Review and Meta-Analysis. Diagnostics. 2021; 11(8):1351. https://doi.org/10.3390/diagnostics11081351
Chicago/Turabian StyleWang, Mengshu, Xufei Luo, Ling Wang, Janne Estill, Meng Lv, Ying Zhu, Qi Wang, Xiaojuan Xiao, Yang Song, Myeong Soo Lee, and et al. 2021. "A Comparison of Lung Ultrasound and Computed Tomography in the Diagnosis of Patients with COVID-19: A Systematic Review and Meta-Analysis" Diagnostics 11, no. 8: 1351. https://doi.org/10.3390/diagnostics11081351