
Coronary Computer Tomography Angiography in 2021—Acquisition Protocols, Tips and Tricks and Heading beyond the Possible


Abstract
:1. Introduction
2. Population Selection
Who Should Get a CCTA Scan?
3. Technical Aspects
3.1. What Do We Need?
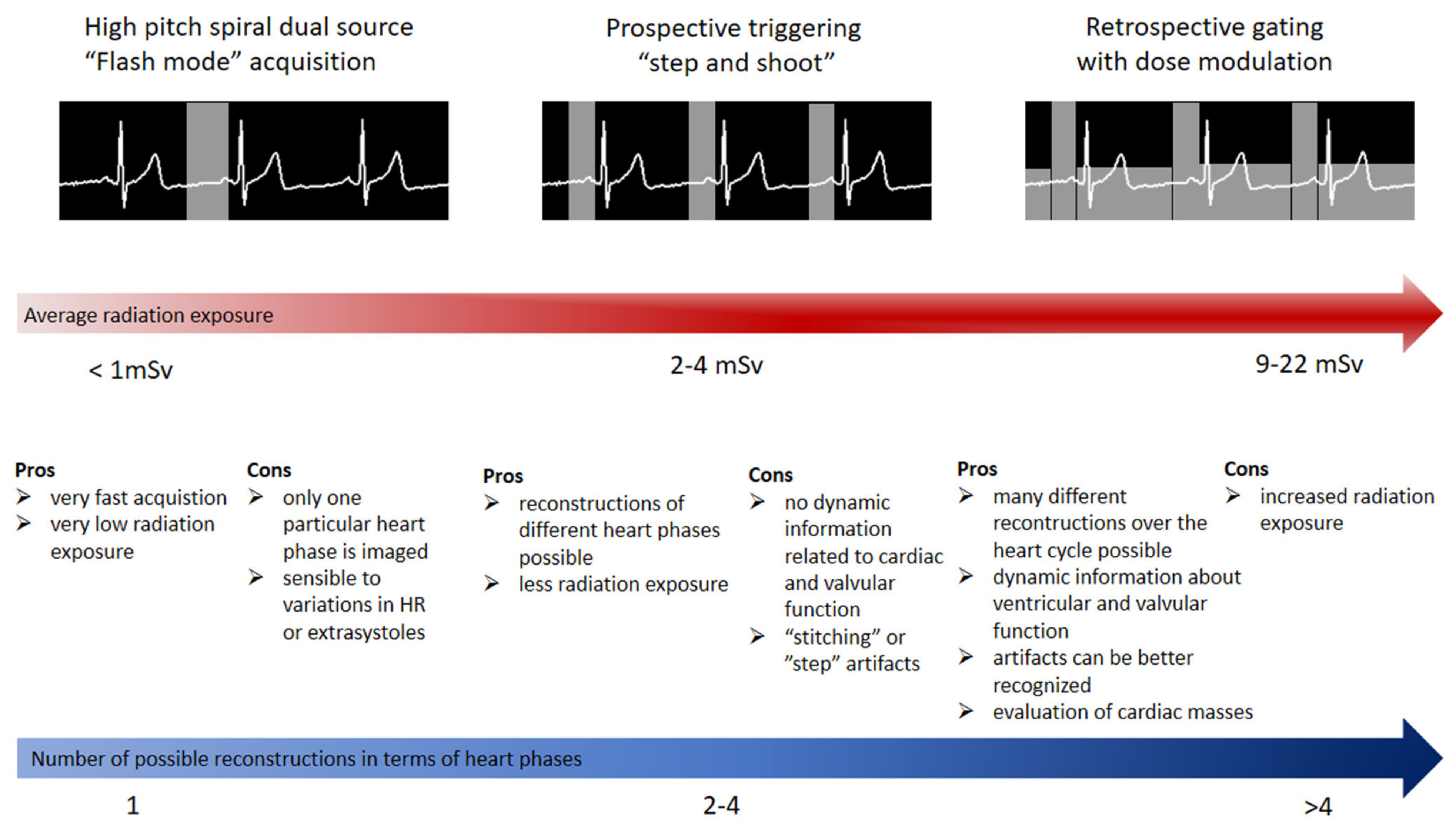
3.2. Which Protocol Needs to Be Chosen?
3.3. How Much Can We Reduce Radiation and Contrast Agent Exposure?
4. Diagnosis
4.1. Do We Still Need Calcium Scoring?
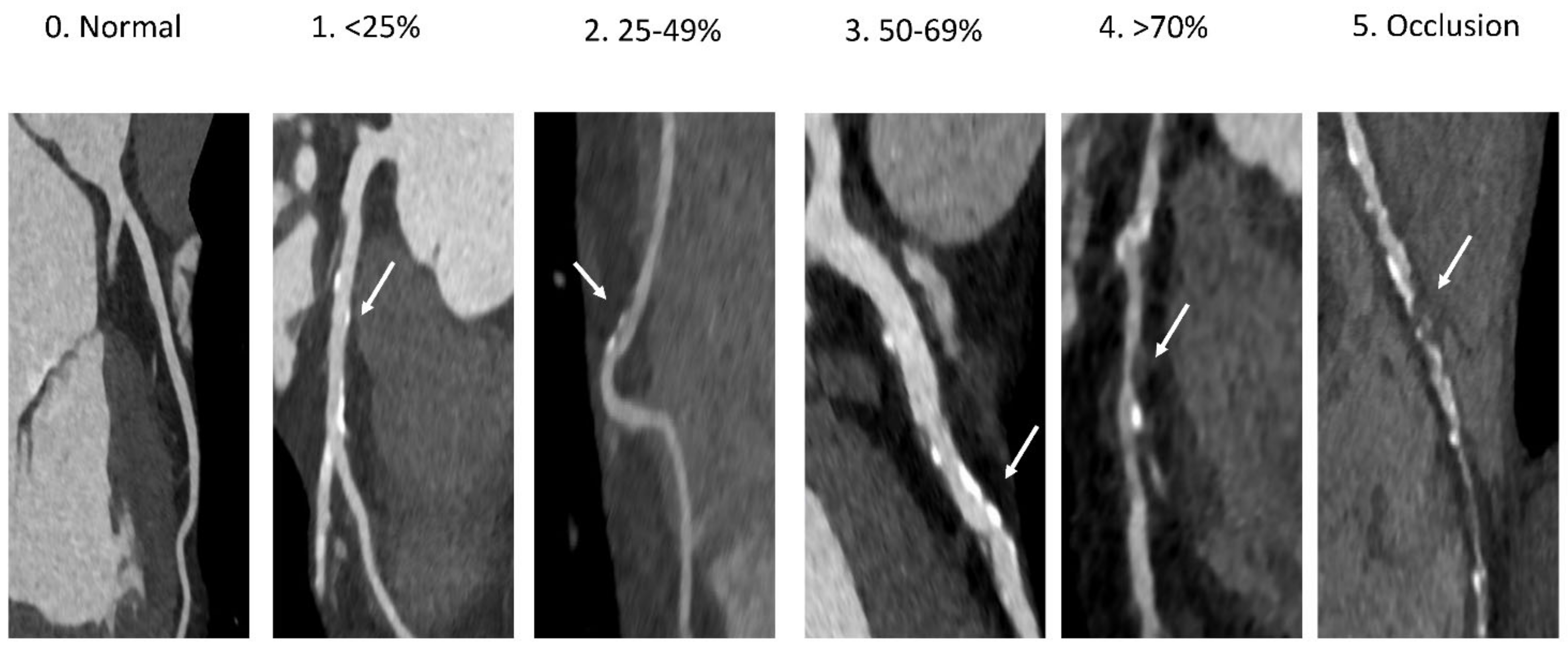
4.2. Stenosis Visualization and Quantification: The “Heart” of the Problem
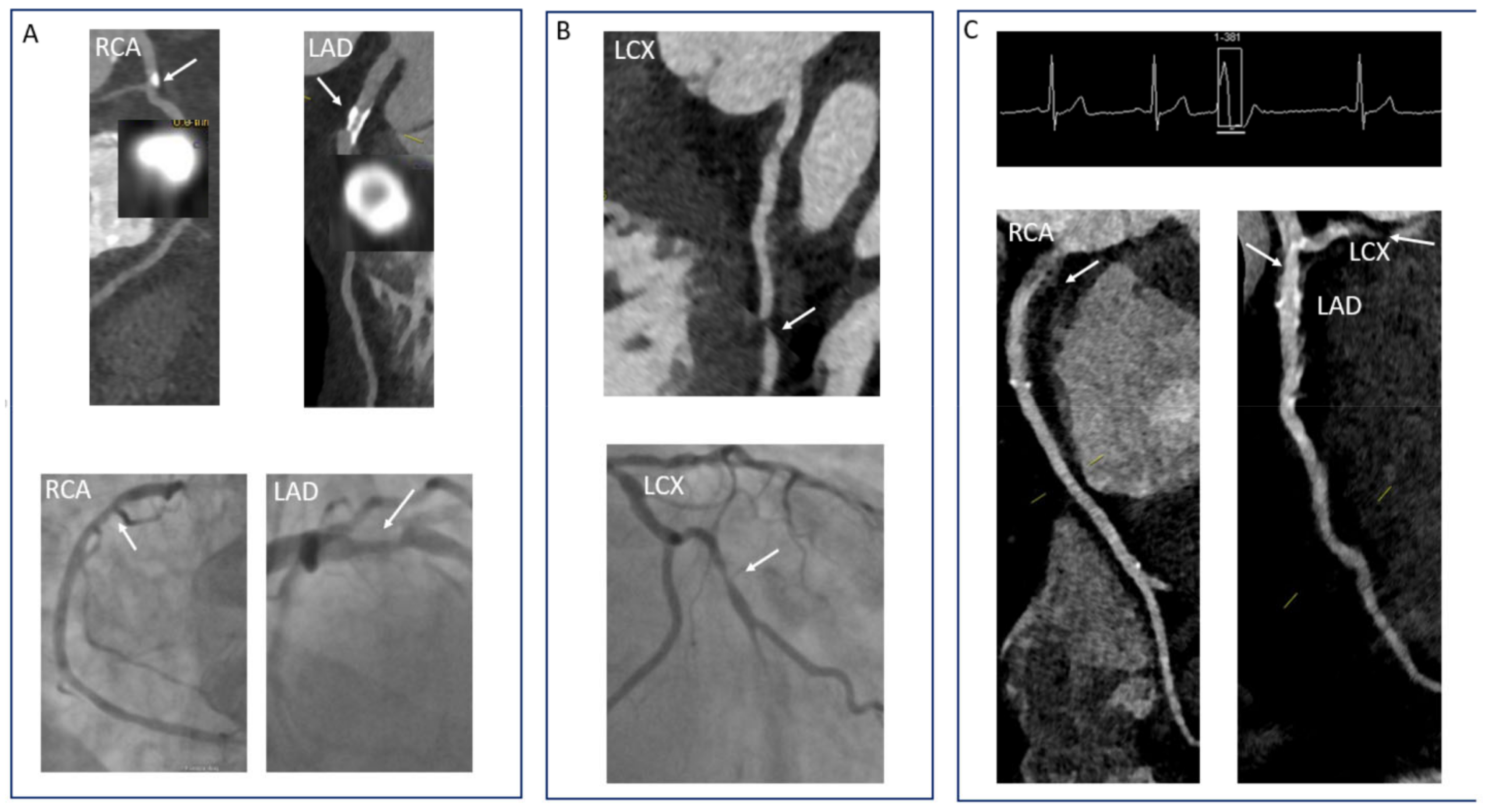
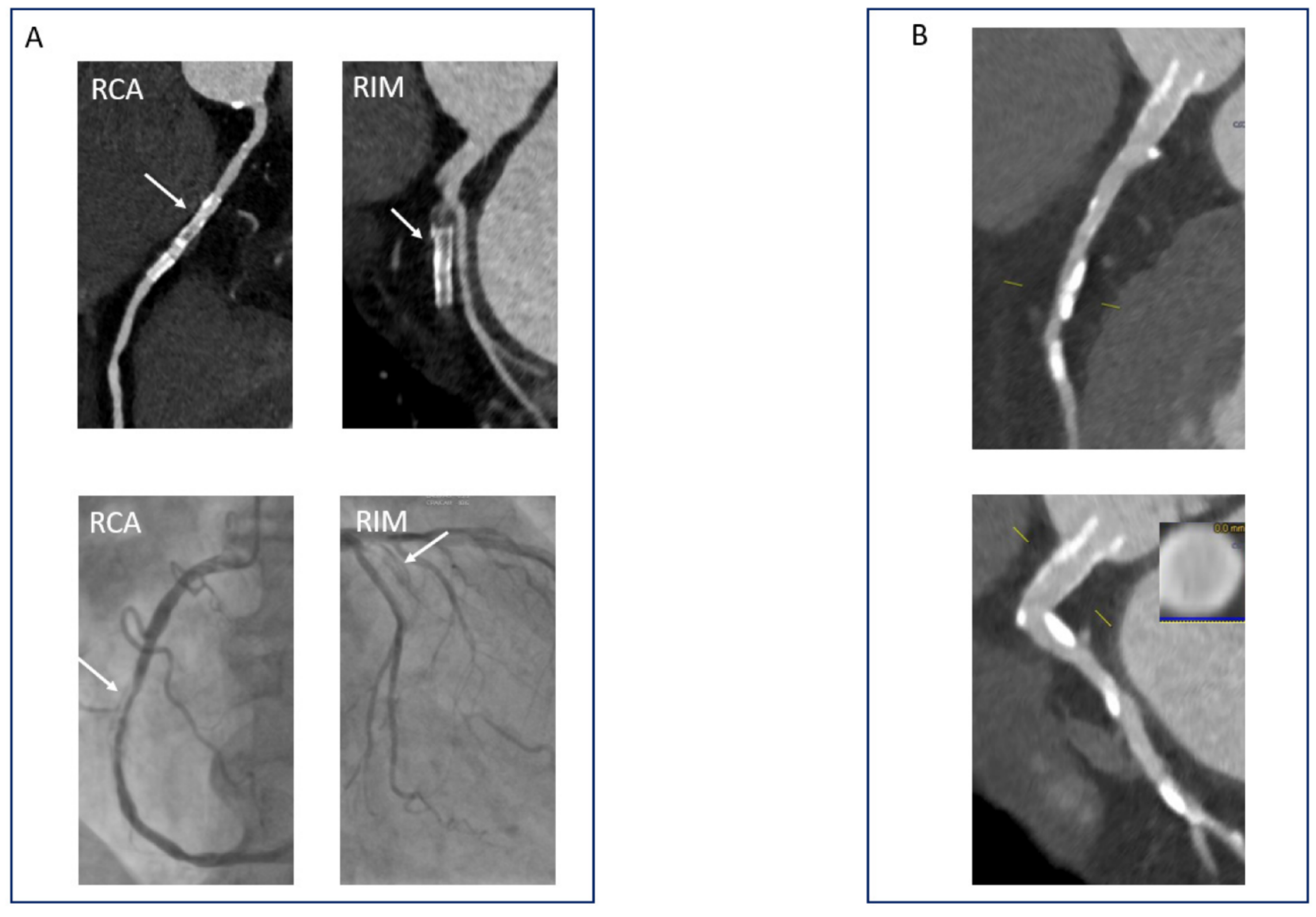
4.2.1. Pitfalls in the Evaluation of Coronary Stenoses: What Should We Look Out for?
4.2.2. CCTA versus Other Diagnostic Modalities: Which One to Choose?
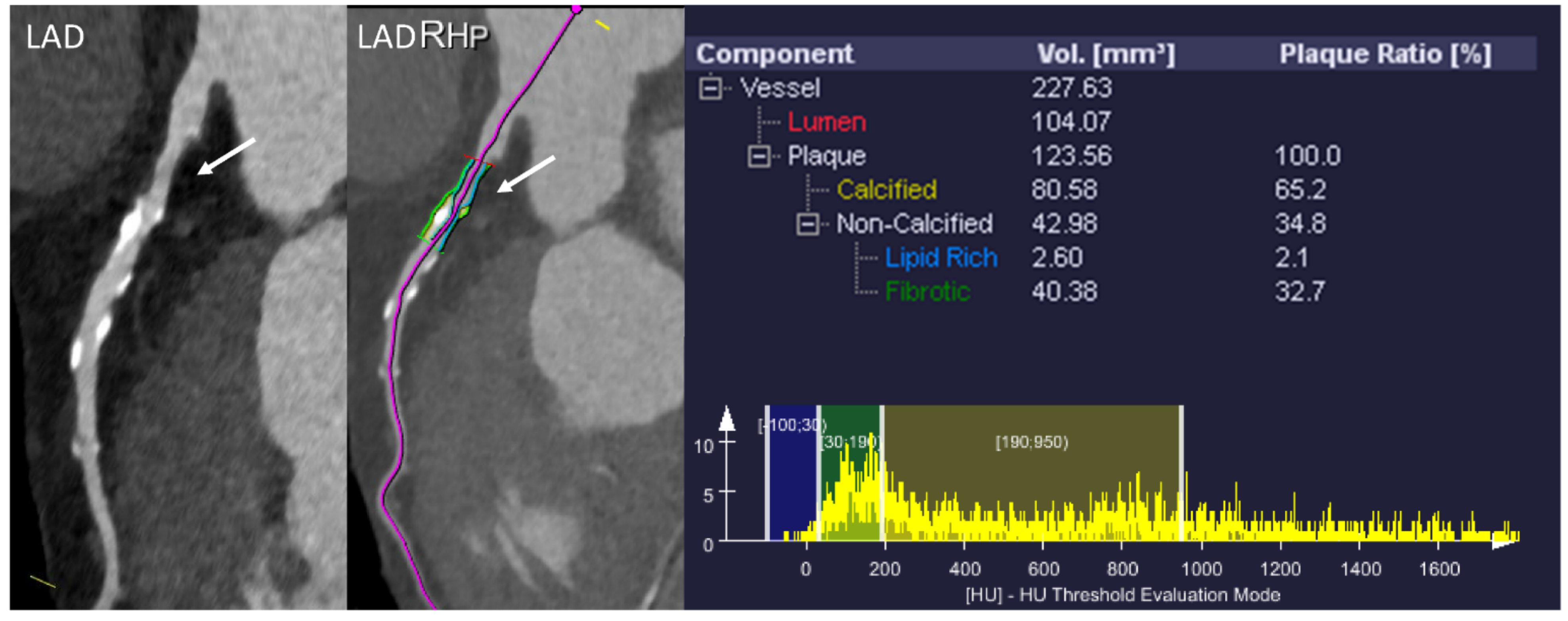
4.3. Plaque Characteristics: Are All Plaques Created Equally?
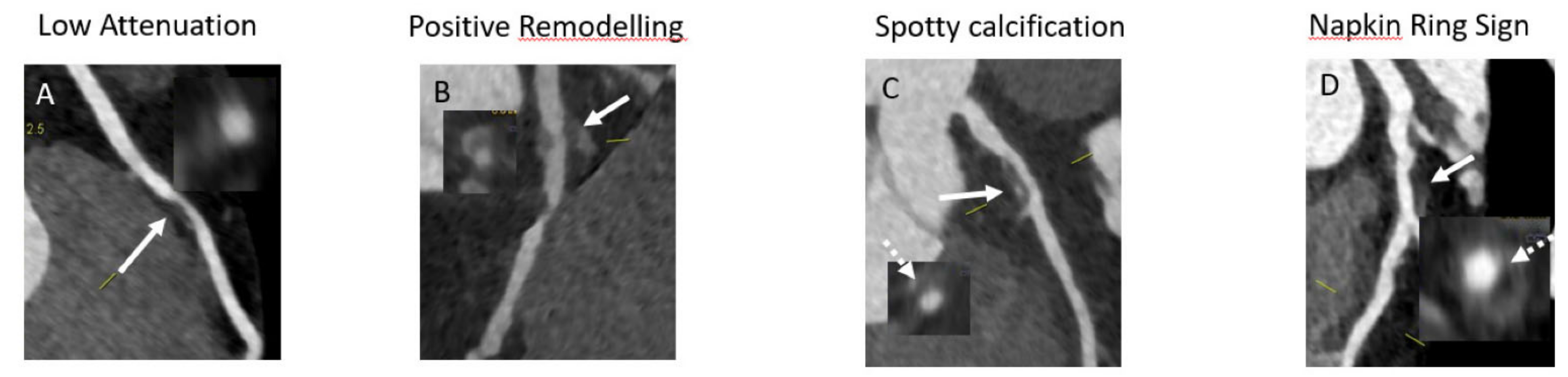
- Low attenuation plaques are considered to mirror the vulnerable plaques characterized by necrotic lipid rich core. As CCTA can distinguish between lipid and fibrotic tissue in terms of HU, it is conceivable that analyzing plaques in terms of HU can identify those with a predominant lipid composition. In this regard, several studies used intravascular ultrasound (IVUS) as reference standard for the characterization of low attenuation plaques [95,96]. Although significant overlap was seen, a value of <30 HU provided identification of vulnerable lipid-rich plaques with good sensitivity and specificity [97,98].
- Positive remodeling is a process that occurs in the early stages of atherosclerosis and is considered as a compensatory mechanism of the vessel to maintain a sufficient non-stenotic area in the context of atherosclerotic plaque progression [99]. The presence of positive remodeling is associated with a lipid-rich plaque and accumulation of macrophages and necrotic tissue [100]. A 10% increase in the diameter at the level of the stenosis in comparison to the reference diameter outside the stenosis is considered to indicate positive remodeling [101]. Similar to all other features of high-risk plaque, positive remodeling is seen more often in patients with ACS compared to patients with CCS [102].
- The napkin-ring sign is a form of low attenuation plaque that exhibits a heterogenous pattern of attenuation. Thus, the core shows low attenuation pattern indicative of lipid rich necrosis and the cap displays high attenuation indicative of the fibrotic cap [105]. This type of pattern is highly suggestive of vulnerable plaque and is considered as a precursor of plaque rupture [106]. The high predictive value of the napkin-ring sign for future ACS is quite consistent across studies [107,108,109].
4.4. Plaque Stabilization and Regression: Can We Turn Back the Time?
4.5. Perivascular Fat: Identifying the Problems before They Even Start?
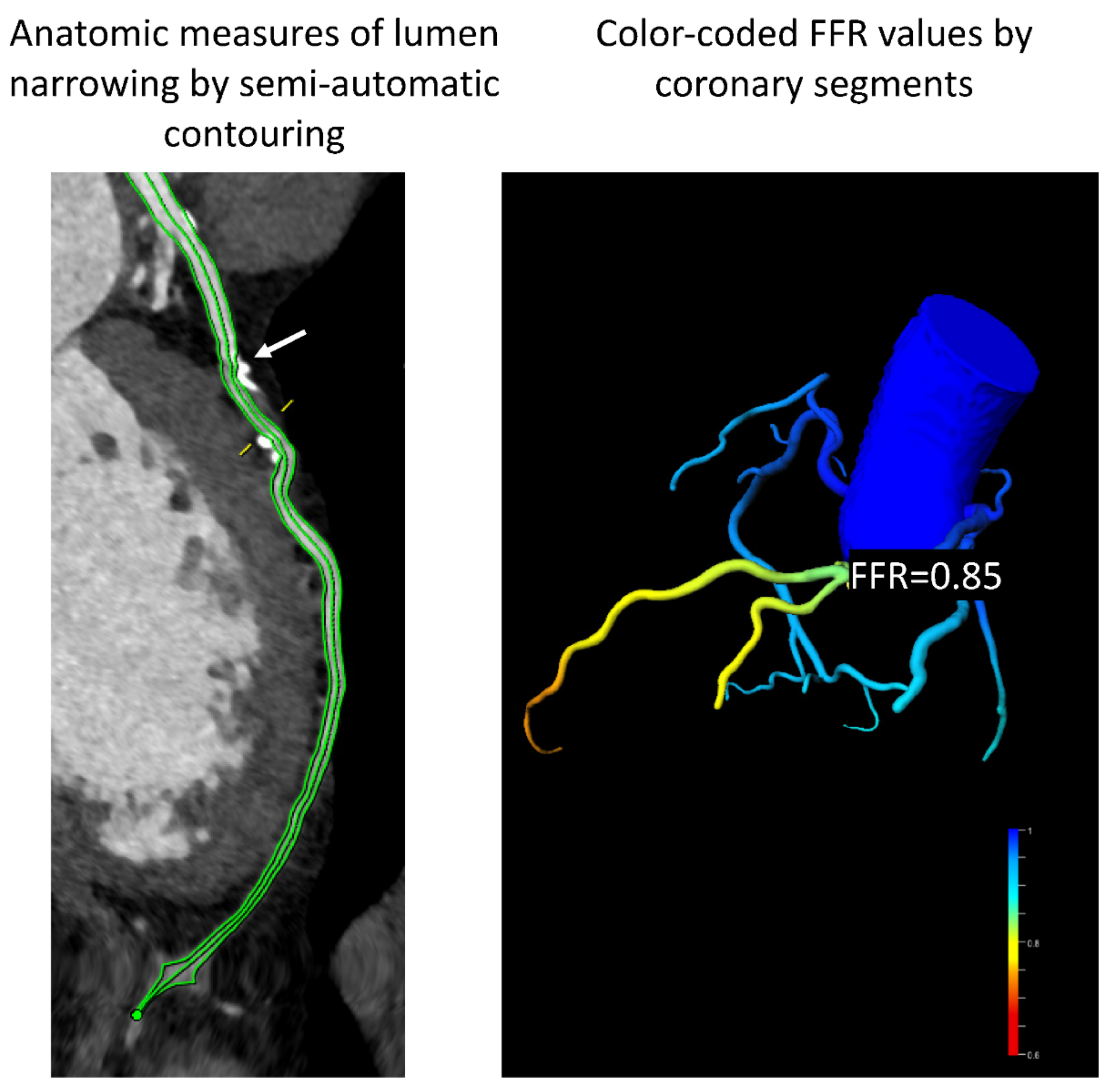
4.6. Computational Fluid Dynamics and Fractional Flow Reserve CT: Moving from Anatomy to Hemodynamic Significance
4.7. Perfusion Imaging in CCTA: Not Just the Coronaries
5. Prognosis: Can We See into the Future?
6. Special Scenarios
6.1. Evaluation of Stents: Can We See through Metal?
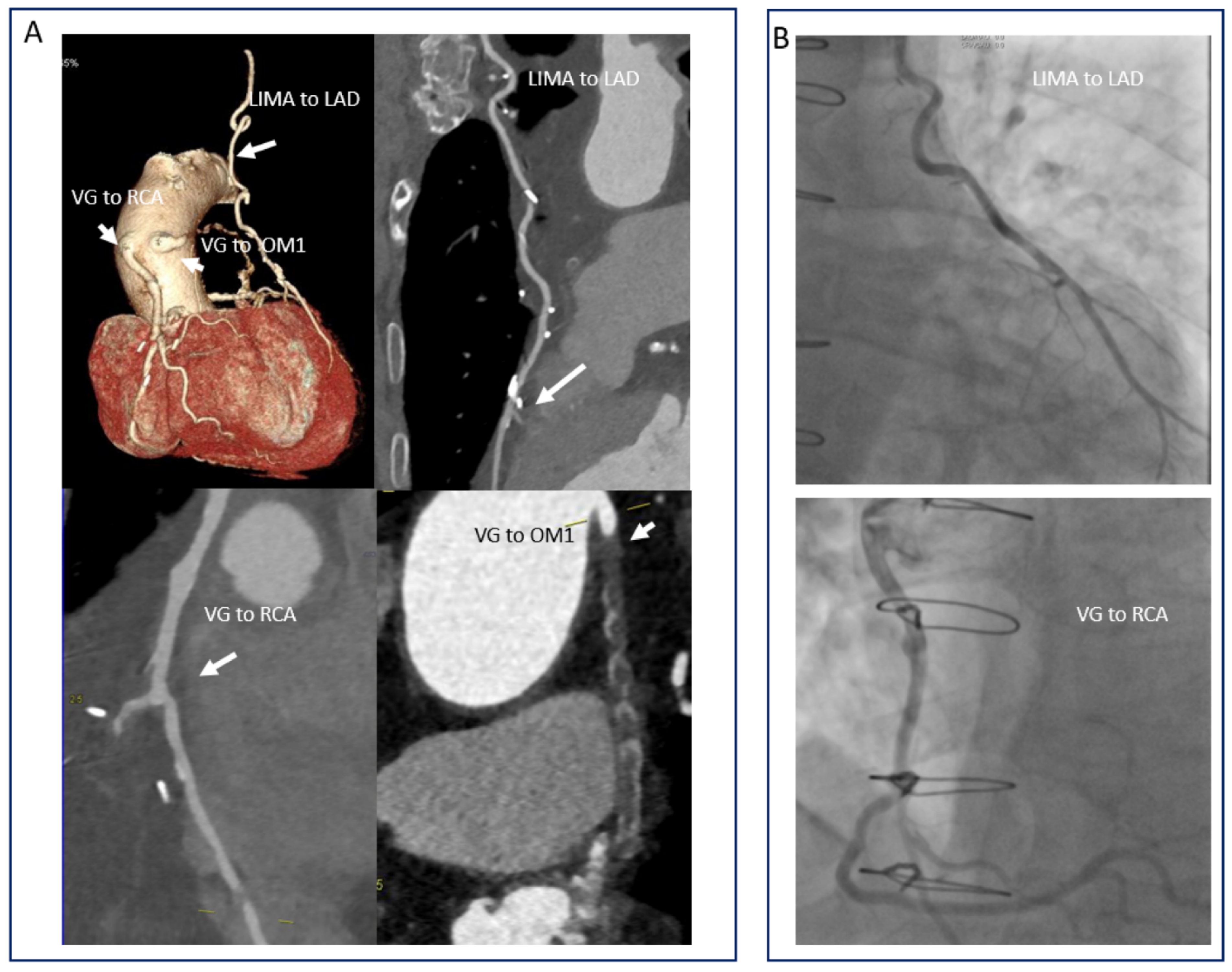
6.2. Evaluation of Bypass Grafts: Looking at the Surgeon’s Work
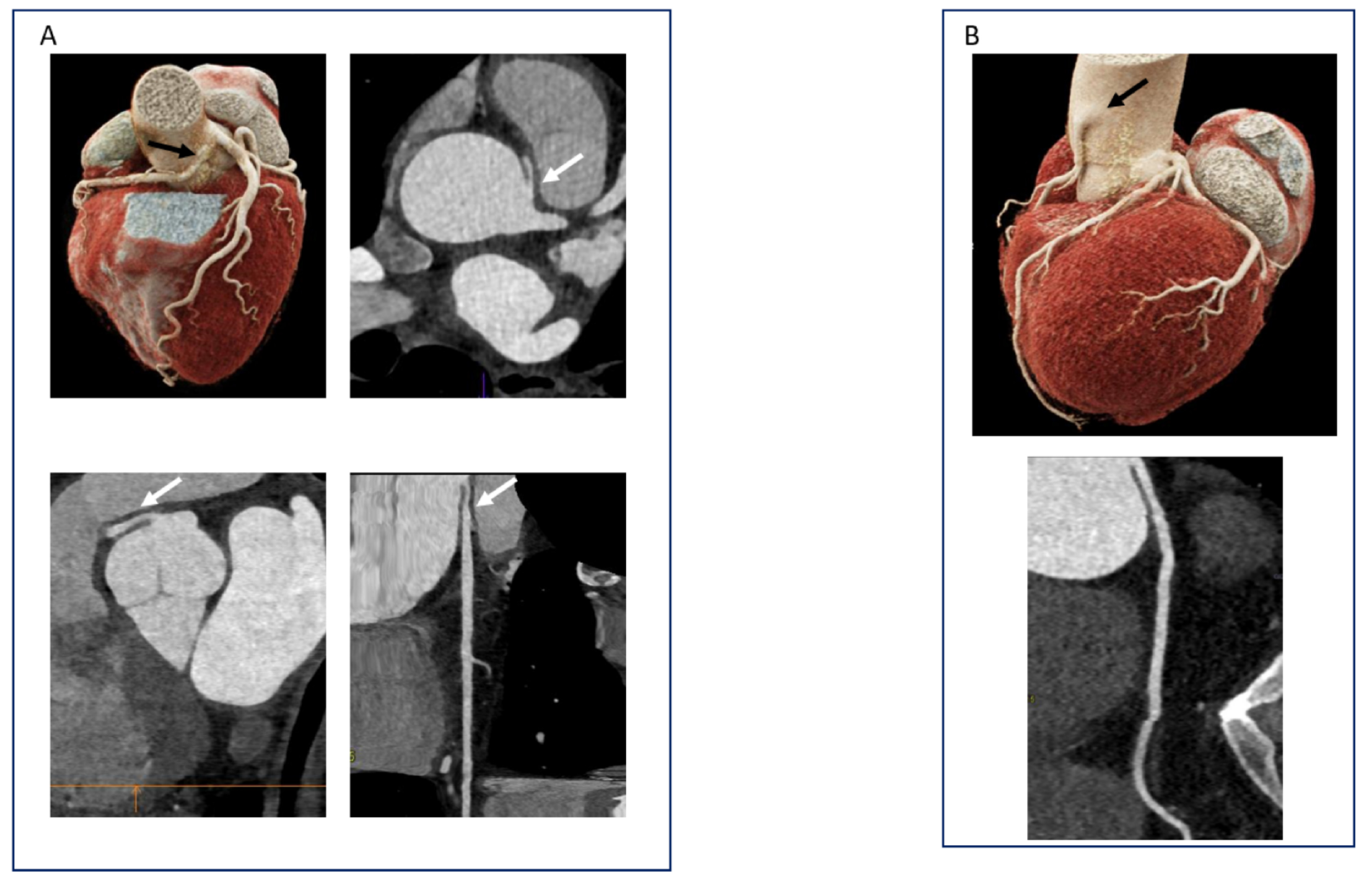
6.3. Coronary Anomalies and Muscle Bridges: Not So Rare
6.4. Cardiac CT in Other Clinical Scenarios: Valvular Heart Diseases and Atrial Fibrillation
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2021 Update: A Report From the American Heart Association. Circulation 2021, 137, 67. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Korosoglou, G.; Giusca, S.; Gitsioudis, G.; Erbel, C.; Katus, H.A. Cardiac magnetic resonance and computed tomography angiography for clinical imaging of stable coronary artery disease. Diagnostic classification and risk stratification. Front. Physiol. 2014, 5, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knuuti, J.; Ballo, H.; Juarez-Orozco, L.E.; Saraste, A.; Kolh, P.; Rutjes, A.W.S.; Jüni, P.; Windecker, S.; Bax, J.J.; Wijns, W. The performance of non-invasive tests to rule-in and rule-out significant coronary artery stenosis in patients with stable angina: A meta-analysis focused on post-test disease probability. Eur. Hear. J. 2018, 39, 3322–3330. [Google Scholar] [CrossRef]
- Baessato, F.; Guglielmo, M.; Muscogiuri, G.; Baggiano, A.; Fusini, L.; Scafuri, S.; Babbaro, M.; Mollace, R.; Collevecchio, A.; Guaricci, A.I.; et al. The Incremental Role of Coronary Computed Tomography in Chronic Coronary Syndromes. J. Clin. Med. 2020, 9, 3925. [Google Scholar] [CrossRef]
- Abdelrahman, K.M.; Chen, M.Y.; Dey, A.K.; Virmani, R.; Finn, A.V.; Khamis, R.Y.; Choi, A.D.; Min, J.K.; Williams, M.C.; Buckler, A.J.; et al. Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies. J. Am. Coll. Cardiol. 2020, 76, 1226–1243. [Google Scholar] [CrossRef]
- Stehli, J.; Fuchs, T.A.; Bull, S.; Clerc, O.F.; Possner, M.; Buechel, R.R.; Gaemperli, O.; Kaufmann, P.A. Accuracy of Coronary CT Angiography Using a Submillisievert Fraction of Radiation Exposure: Comparison With Invasive Coronary Angiography. J. Am. Coll. Cardiol. 2014, 64, 772–780. [Google Scholar] [CrossRef] [Green Version]
- Al-Lamee, R.; Thompson, D.; Dehbi, H.-M.; Sen, S.; Tang, K.; Davies, J.; Keeble, T.; Mielewczik, M.; Kaprielian, R.; Malik, I.S.; et al. Percutaneous coronary intervention in stable angina (ORBITA): A double-blind, randomised controlled trial. Lancet 2018, 391, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; López-Sendón, J.; Alexander, K.P.; et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef]
- Overview | Recent-Onset Chest Pain of Suspected Cardiac Origin: Assessment and Diagnosis | Guidance | NICE. NICE. Available online: https://www.nice.org.uk/guidance/cg95 (accessed on 30 November 2016).
- Narula, J.; Chandrashekhar, Y.; Ahmadi, A.; Abbara, S.; Berman, D.S.; Blankstein, R.; Leipsic, J.; Newby, D.; Nicol, E.D.; Nieman, K.; et al. SCCT 2021 Expert Consensus Document on Coronary Computed Tomographic Angiography: A Report of the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2021, 15, 192–217. [Google Scholar] [CrossRef]
- Recommendations | HeartFlow FFRCT for Estimating Fractional Flow Reserve from Coronary CT Angiography | Guidance | NICE. NICE. Available online: https://www.nice.org.uk/guidance/mtg32/chapter/1-recommendations (accessed on 1 January 2021).
- Son, M.; Yoo, S.; Lee, D.; Lee, H.; Song, I.; Chun, E.; White, C. Current Role of Computed Tomography in the Evaluation of Acute Coronary Syndrome. Diagnostics 2021, 11, 266. [Google Scholar] [CrossRef]
- Hoffmann, U.; Truong, Q.A.; Schoenfeld, D.A.; Chou, E.T.; Woodard, P.K.; Nagurney, J.T.; Pope, J.H.; Hauser, T.H.; White, C.S.; Weiner, S.; et al. Coronary CT Angiography versus Standard Evaluation in Acute Chest Pain. N. Engl. J. Med. 2012, 367, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Litt, H.I.; Gatsonis, C.; Snyder, B.; Singh, H.; Miller, C.D.; Entrikin, D.W.; Leaming, J.M.; Gavin, L.J.; Pacella, C.B.; Hollander, J.E. CT Angiography for Safe Discharge of Patients with Possible Acute Coronary Syndromes. N. Engl. J. Med. 2012, 366, 1393–1403. [Google Scholar] [CrossRef] [Green Version]
- Linde, J.J.; Hove, J.D.; Sørgaard, M.; Kelbæk, H.; Jensen, G.B.; Kühl, J.T.; Hindsø, L.; Køber, L.; Nielsen, W.B.; Kofoed, K.F. Long-Term Clinical Impact of Coronary CT Angiography in Patients With Recent Acute-Onset Chest Pain: The Randomized Controlled CATCH Trial. JACC Cardiovasc. Imaging 2015, 8, 1404–1413. [Google Scholar]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Linde, J.J.; Kelbæk, H.; Hansen, T.F.; Sigvardsen, P.E.; Torp-Pedersen, C.; Bech, J.; Heitmann, M.; Nielsen, O.W.; Høfsten, D.; Kühl, J.T.; et al. Coronary CT Angiography in Patients With Non-ST-Segment Elevation Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 75, 453–463. [Google Scholar] [CrossRef]
- Lee, H.Y.; Yoo, S.M.; White, C.S. Coronary CT angiography in emergency department patients with acute chest pain: Triple rule-out protocol versus dedicated coronary CT angiography. Int. J. Cardiovasc. Imaging 2008, 25, 319–326. [Google Scholar] [CrossRef]
- De Isla, L.P.; Alonso, R.; de Diego, J.J.G.; Muñiz-Grijalvo, O.; Díaz-Díaz, J.L.; Zambón, D.; Miramontes, J.P.; Fuentes, F.; Andrés, R.D.; Werenitzky, J. Coronary plaque burden, plaque characterization and their prognostic implications in familial hypercholesterolemia: A computed tomographic angiography study. Atherosclerosis 2021, 317, 52–58. [Google Scholar] [CrossRef]
- Korosoglou, G.; Chatzizisis, Y.S.; Raggi, P. Coronary computed tomography angiography in asymptomatic patients: Still a taboo or precision medicine? Atherosclerosis 2021, 317, 47–49. [Google Scholar] [CrossRef]
- Lewis, M.A.; Pascoal, A.; Keevil, S.F.; Lewis, C.A. Selecting a CT scanner for cardiac imaging: The heart of the matter. Br. J. Radiol. 2016, 89, 20160376. [Google Scholar] [CrossRef] [Green Version]
- Lawler, L.P.; Pannu, H.K.; Fishman, E.K. MDCT Evaluation of the Coronary Arteries, 2004: How We Do It—Data Acquisition, Postprocessing, Display, and Interpretation. Am. J. Roentgenol. 2005, 184, 1402–1412. [Google Scholar] [CrossRef]
- Otero, H.J.; Steigner, M.L.; Rybicki, F.J. The “Post-64” Era of Coronary CT Angiography: Understanding New Technology from Physical Principles. Radiol. Clin. North Am. 2009, 47, 79–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naoum, C.; Blanke, P.; Leipsic, J. Iterative reconstruction in cardiac CT. J. Cardiovasc. Comput. Tomogr. 2015, 9, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Halliburton, S.S.; Tanabe, Y.; Partovi, S.; Rajiah, P. The role of advanced reconstruction algorithms in cardiac CT. Cardiovasc. Diagn. Ther. 2017, 7, 527–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toia, P.; La Grutta, L.; Sollami, G.; Clemente, A.; Gagliardo, C.; Galia, M.; Maffei, E.; Midiri, M.; Cademartiri, F. Technical development in cardiac CT: current standards and future improvements—a narrative review. Cardiovasc. Diagn. Ther. 2020, 10, 2018–2035. [Google Scholar] [CrossRef] [PubMed]
- Halliburton, S.; Arbab-Zadeh, A.; Dey, D.; Einstein, A.J.; Gentry, R.; George, R.T.; Gerber, T.; Mahesh, M.; Weigold, W.G. State-of-the-art in CT hardware and scan modes for cardiovascular CT. J. Cardiovasc. Comput. Tomogr. 2012, 6, 154–163. [Google Scholar] [CrossRef] [Green Version]
- Stephan, A.; Stefan, U.; Ulrich, B.; Marc, K.; Dieter, R.; Tom, G.; Daniel, W.G.; Kalender, W.A.; Moshage, W. Noninvasive Coronary Angiography by Retrospectively ECG-Gated Multislice Spiral CT. Circulation 2000, 102, 2823–2828. [Google Scholar]
- Husmann, L.; Leschka, S.; Desbiolles, L.; Schepis, T.; Gaemperli, O.; Seifert, B.; Cattin, P.; Frauenfelder, T.; Flohr, T.G.; Marincek, B.; et al. Coronary Artery Motion and Cardiac Phases: Dependency on Heart Rate—Implications for CT Image Reconstruction. Radiology 2007, 245, 567–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliburton, S.S.; Abbara, S.; Chen, M.Y.; Gentry, R.; Mahesh, M.; Raff, G.L.; Shaw, L.J.; Hausleiter, J. SCCT guidelines on radiation dose and dose-optimization strategies in cardiovascular CT. J. Cardiovasc. Comput. Tomogr. 2011, 5, 198–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bischoff, B.; Hein, F.; Meyer, T.; Krebs, M.; Hadamitzky, M.; Martinoff, S.; Schömig, A.; Hausleiter, J. Comparison of Sequential and Helical Scanning for Radiation Dose and Image Quality: Results of the Prospective Multicenter Study on Radiation Dose Estimates of Cardiac CT Angiography (PROTECTION) I Study. Am. J. Roentgenol. 2010, 194, 1495–1499. [Google Scholar] [CrossRef]
- Husmann, L.; Valenta, I.; Gaemperli, O.; Adda, O.; Treyer, V.; Wyss, C.A.; Veit-Haibach, P.; Tatsugami, F.; Von Schulthess, G.K.; Kaufmann, P.A. Feasibility of low-dose coronary CT angiography: First experience with prospective ECG-gating. Eur. Hear. J. 2007, 29, 191–197. [Google Scholar] [CrossRef] [Green Version]
- Korosoglou, G.; Marwan, M.; Schmermund, A.; Schneider, S.; Giusca, S.; Gitsioudis, G.; Bruder, O.; Hausleiter, J.; Schroeder, S.; Leber, A.; et al. 2179Influence of irregular heart rhythm on radiation exposure, image quality and diagnostic impact of cardiac computed tomography angiography in 4,767 patients. Eur. Hear. J. 2017, 38, 34–41. [Google Scholar] [CrossRef]
- Rybicki, F.J.; Otero, H.J.; Steigner, M.L.; Vorobiof, G.; Nallamshetty, L.; Mitsouras, D.; Ersoy, H.; Mather, R.T.; Judy, P.F.; Cai, T.; et al. Initial evaluation of coronary images from 320-detector row computed tomography. Int. J. Cardiovasc. Imaging 2008, 24, 535–546. [Google Scholar] [CrossRef]
- Khan, A.; Nasir, K.; Khosa, F.; Saghir, A.; Sarwar, S.; Clouse, M.E. Prospective Gating With 320-MDCT Angiography: Effect of Volume Scan Length on Radiation Dose. Am. J. Roentgenol. 2011, 196, 407–411. [Google Scholar] [CrossRef] [Green Version]
- Hausleiter, J.; Bischoff, B.; Hein, F.; Meyer, T.; Hadamitzky, M.; Thierfelder, C.; Allmendinger, T.; Flohr, T.G.; Schömig, A.; Martinoff, S. Feasibility of dual-source cardiac CT angiography with high-pitch scan protocols. J. Cardiovasc. Comput. Tomogr. 2009, 3, 236–242. [Google Scholar] [CrossRef]
- Achenbach, S.; Marwan, M.; Schepis, T.; Pflederer, T.; Bruder, H.; Allmendinger, T.; Petersilka, M.; Anders, K.; Lell, M.; Kuettner, A.; et al. High-pitch spiral acquisition: A new scan mode for coronary CT angiography. J. Cardiovasc. Comput. Tomogr. 2009, 3, 117–121. [Google Scholar] [CrossRef]
- Achenbach, S.; Marwan, M.; Ropers, D.; Schepis, T.; Pflederer, T.; Anders, K.; Kuettner, A.; Daniel, W.G.; Uder, M.; Lell, M.M. Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur. Hear. J. 2009, 31, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Earls, J.P.; Berman, E.L.; Urban, B.A.; Curry, C.A.; Lane, J.L.; Jennings, R.S.; McCulloch, C.C.; Hsieh, J.; Londt, J.H. Prospectively Gated Transverse Coronary CT Angiography versus Retrospectively Gated Helical Technique: Improved Image Quality and Reduced Radiation Dose. Radiology 2008, 246, 742–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Defrance, T.; Dubois, E.; Gebow, D.; Ramirez, A.; Wolf, F.; Feuchtner, G.M. Helical prospective ECG-gating in cardiac computed tomography: Radiation dose and image quality. Int. J. Cardiovasc. Imaging 2009, 26, 99–107. [Google Scholar] [CrossRef]
- Stolzmann, P.; Leschka, S.; Scheffel, H.; Krauss, T.; Desbiolles, L.; Plass, A.; Genoni, M.; Flohr, T.G.; Wildermuth, S.; Marincek, B.; et al. Dual-Source CT in Step-and-Shoot Mode: Noninvasive Coronary Angiography with Low Radiation Dose1. Radiology 2008, 249, 71–80. [Google Scholar] [CrossRef] [Green Version]
- Menke, J.; Unterberg-Buchwald, C.; Staab, W.; Sohns, J.M.; Hosseini, A.S.A.; Schwarz, A. Head-to-head comparison of prospectively triggered vs retrospectively gated coronary computed tomography angiography: Meta-analysis of diagnostic accuracy, image quality, and radiation dose. Am. Hear. J. 2013, 165, 154–163.e3. [Google Scholar] [CrossRef] [PubMed]
- Hausleiter, J.; Meyer, T. Tips to minimize radiation exposure. J. Cardiovasc. Comput. Tomogr. 2008, 2, 325–327. [Google Scholar] [CrossRef]
- Kim, J.S.; Choo, K.S.; Jeong, D.W.; Chun, K.J.; Park, Y.H.; Song, S.G.; Park, J.H.; Kim, J.H.; Kim, J.; Han, D.; et al. Step-and-shoot prospectively ECG-gated vs. retrospectively ECG-gated with tube current modulation coronary CT angiography using 128-slice MDCT patients with chest pain: Diagnostic performance and radiation dose. Acta Radiol. 2011, 52, 860–865. [Google Scholar] [CrossRef]
- Hausleiter, J.; Meyer, T.; Hadamitzky, M.; Huber, E.; Zankl, M.; Martinoff, S.; Kastrati, A.; Schömig, A. Radiation dose estimates from cardiac multislice computed tomography in daily practice: Impact of different scanning protocols on effective dose estimates. Circulation 2006, 113, 1305–1310. [Google Scholar] [CrossRef] [Green Version]
- Meyer, M.; Haubenreisser, H.; Schoepf, U.J.; Vliegenthart, R.; Leidecker, C.; Allmendinger, T.; Lehmann, R.; Sudarski, S.; Borggrefe, M.; Schoenberg, S.O.; et al. Closing in on the K edge: Coronary CT angiography at 100, 80, and 70 kV-initial comparison of a second- versus a third-generation dual-source CT system. Radiology 2014, 273, 373–382. [Google Scholar] [CrossRef] [Green Version]
- Katzberg, R.W.; Lamba, R. Contrast-induced nephropathy after intravenous administration: Fact or fiction? Radiol. Clin. 2009, 47, 789–800. [Google Scholar] [CrossRef]
- Nakaura, T.; Awai, K.; Yauaga, Y.; Nakayama, Y.; Oda, S.; Hatemura, M.; Nagayoshi, Y.; Ogawa, H.; Yamashita, Y. Contrast Injection Protocols for Coronary Computed Tomography Angiography Using a 64-Detector Scanner: Comparison Between Patient Weight-Adjusted- and Fixed Iodine-Dose Protocols. Investig. Radiol. 2008, 43, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Yamamuro, M.; Tadamura, E.; Kanao, S.; Wu, Y.-W.; Tambara, K.; Komeda, M.; Toma, M.; Kimura, T.; Kita, T.; Togashi, T. Coronary angiography by 64-detector row computed tomography using low dose of contrast material with saline chaser: Influence of total injection volume on vessel attenuation. J. Comput. Assist. Tomogr. 2007, 31, 272–280. [Google Scholar] [CrossRef]
- Oda, S.; Utsunomiya, D.; Nakaura, T.; Kidoh, M.; Funama, Y.; Tsujita, K.; Yamashita, Y. Basic Concepts of Contrast Injection Protocols for Coronary Computed Tomography Angiography. Curr. Cardiol. Rev. 2018, 15, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Bae, K.T. Intravenous Contrast Medium Administration and Scan Timing at CT: Considerations and Approaches. Radiology 2010, 256, 32–61. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.T.; Pannu, H.K.; Fishman, E.K. IV Contrast Infusion for Coronary Artery CT Angiography: Literature Review and Results of a Nationwide Survey. Am. J. Roentgenol. 2009, 192, 214. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.H.; Palmer, F.J. Incidence and significance of coronary artery calcification. Heart 1974, 36, 499–506. [Google Scholar] [CrossRef] [Green Version]
- Schmermund, A.; Baumgart, D.; Görge, G.; Seibel, R.; Grönemeyer, D.; Ge, J.; Haude, M.; Rumberger, J.; Erbel, R. Coronary artery calcium in acute coronary syndromes: A comparative study of electron-beam computed tomography, coronary angiography, and intracoronary ultrasound in survivors of acute myocardial infarction and unstable angina. Circulation 1997, 96, 1461–1469. [Google Scholar] [CrossRef]
- Mintz, G.S.; Pichard, A.D.; Popma, J.J.; Kent, K.M.; Satler, L.F.; A Bucher, T.; Leon, M.B. Determinants and Correlates of Target Lesion Calcium in Coronary Artery Disease: A Clinical, Angiographic and Intravascular Ultrasound Study. J. Am. Coll. Cardiol. 1997, 29, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Nasir, K.; Clouse, M. Role of Nonenhanced Multidetector CT Coronary Artery Calcium Testing in Asymptomatic and Symptomatic Individuals. Radiology 2012, 264, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Neves, P.O.; Andrade, J.; Monção, H. Coronary artery calcium score: current status. Radiol. Bras. 2017, 50, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Greenland, P.; Bonow, R.O.; Brundage, B.H.; Budoff, M.J.; Eisenberg, M.J.; Grundy, S.M.; Lauer, M.S.; Post, W.S.; Raggi, P.; Redberg, R.F.; et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: A report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J. Am. Coll. Cardiol. 2007, 49, 378–402. [Google Scholar]
- Budoff, M.J.; Shaw, L.J.; Liu, S.T.; Weinstein, S.R.; Mosler, T.P.; Tseng, P.H.; Flores, F.R.; Callister, T.Q.; Raggi, P.; Berman, D.S. Long-term prognosis associated with coronary calcification: Observations from a registry of 25,253 patients. J. Am. Coll. Cardiol. 2007, 49, 1860–1870. [Google Scholar] [CrossRef] [Green Version]
- Nasir, K.; Rubin, J.; Blaha, M.J.; Shaw, L.J.; Blankstein, R.; Rivera, J.J.; Khan, A.N.; Berman, D.; Raggi, P.; Callister, T.; et al. Interplay of Coronary Artery Calcification and Traditional Risk Factors for the Prediction of All-Cause Mortality in Asymptomatic Individuals. Circ. Cardiovasc. Imaging 2012, 5, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Erbel, R.; Möhlenkamp, S.; Moebus, S.; Schmermund, A.; Lehmann, N.; Stang, A.; Dragano, D.; Grönemeyer, D.; Seibel, R.; Kälsch, H.; et al. Coronary risk stratification, discrimination, and reclassification improvement based on quantification of subclinical coronary atherosclerosis: The Heinz Nixdorf Recall study. J. Am. Coll. Cardiol. 2010, 56, 1397–1406. [Google Scholar] [CrossRef] [Green Version]
- Elias-Smale, S.E.; Proença, R.V.; Koller, M.T.; Kavousi, M.; van Rooij, F.J.A.; Hunink, M.G.; Steyerberg, E.W.; Hofman, A.; Oudkerk, M.; Witteman, J.C.M. Coronary calcium score improves classification of coronary heart disease risk in the elderly: The Rotterdam study. J. Am. Coll. Cardiol. 2010, 56, 1407–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- Stein, P.D.; Yaekoub, A.Y.; Matta, F.; Sostman, H.D. 64-Slice CT for Diagnosis of Coronary Artery Disease: A Systematic Review. Am. J. Med. 2008, 121, 715–725. [Google Scholar] [CrossRef]
- Sun, Z.; Lin, C.; Davidson, R.; Dong, C.; Liao, Y. Diagnostic value of 64-slice CT angiography in coronary artery disease: A systematic review. Eur. J. Radiol. 2008, 67, 78–84. [Google Scholar] [CrossRef]
- Miller, J.M.; Rochitte, C.E.; Dewey, M.; Arbab-Zadeh, A.; Niinuma, H.; Gottlieb, I.; Paul, N.; Clouse, M.E.; Shapiro, E.P.; Hoe, J.; et al. Diagnostic Performance of Coronary Angiography by 64-Row CT. N. Engl. J. Med. 2008, 359, 2324–2336. [Google Scholar] [CrossRef] [Green Version]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar]
- Meijboom, W.B.; van Mieghem, C.A.; Mollet, N.R.; Pugliese, F.; Weustink, A.C.; van Pelt, N.; Cademartiri, F.; Nieman, K.; Boersma, E.; de Jaegere, P.; et al. 64-Slice Computed Tomography Coronary Angiography in Patients With High, Intermediate, or Low Pretest Probability of Significant Coronary Artery Disease. J. Am. Coll. Cardiol. 2007, 50, 1469–1475. [Google Scholar] [CrossRef] [Green Version]
- De Graaf, F.R.; Schuijf, J.D.; van Velzen, J.E.; Kroft, L.J.; de Roos, A.; Reiber, J.H.C.; Boersma, E.; Schalij, M.J.; Spanó, F.; Jukema, J.W.; et al. Diagnostic accuracy of 320-row multidetector computed tomography coronary angiography in the non-invasive evaluation of significant coronary artery disease. Eur. Heart J. 2010, 31, 1908–1915. [Google Scholar] [CrossRef] [Green Version]
- Leber, A.W.; Johnson, T.; Becker, A.; Von Ziegler, F.; Tittus, J.; Nikolaou, K.; Reiser, M.; Steinbeck, G.; Becker, C.R.; Knez, A. Diagnostic accuracy of dual-source multi-slice CT-coronary angiography in patients with an intermediate pretest likelihood for coronary artery disease. Eur. Hear. J. 2007, 28, 2354–2360. [Google Scholar] [CrossRef]
- Leipsic, J.; Abbara, S.; Achenbach, S.; Cury, R.; Earls, J.P.; Mancini, G.J.; Nieman, K.; Pontone, G.; Raff, G.L. SCCT guidelines for the interpretation and reporting of coronary CT angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J. Cardiovasc. Comput. Tomogr. 2014, 8, 342–358. [Google Scholar] [CrossRef] [PubMed]
- Cury, R.C.; Abbara, S.; Achenbach, S.; Agatston, A.; Berman, D.S.; Budoff, M.J.; Dill, K.E.; Jacobs, J.E.; Maroules, C.D.; Rubin, G.D.; et al. CAD-RADSTM Coronary Artery Disease – Reporting and Data System. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. J. Cardiovasc. Comput. Tomogr. 2016, 10, 269–281. [Google Scholar] [CrossRef] [Green Version]
- Kroft, L.J.M.; De Roos, A.; Geleijns, J. Artifacts in ECG-Synchronized MDCT Coronary Angiography. Am. J. Roentgenol. 2007, 189, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.; Tang, L.-J.; Xu, Y.; Zhu, X.-M.; Zhang, Y.-D.; Shi, H.-B.; Yu, R.-B. The Diagnostic Performance of Coronary CT Angiography for the Assessment of Coronary Stenosis in Calcified Plaque. PLoS ONE 2016, 11, e0154852. [Google Scholar] [CrossRef] [PubMed]
- Karlo, C.A.; Leschka, S.; Stolzmann, P.; Glaser-Gallion, N.; Wildermuth, S.; Alkadhi, H. A systematic approach for analysis, interpretation, and reporting of coronary CTA studies. Insights Imaging 2012, 3, 215–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Levin, D.C.; Halpern, E.J.; Fischman, D.; Savage, M.; Walinsky, P. Accuracy of MDCT in Assessing the Degree of Stenosis Caused by Calcified Coronary Artery Plaques. Am. J. Roentgenol. 2008, 191, 1676–1683. [Google Scholar] [CrossRef] [Green Version]
- Mangold, S.; Wichmann, J.L.; Schoepf, U.J.; Litwin, S.E.; Canstein, C.; Varga-Szemes, A.; Muscogiuri, G.; Fuller, S.R.; Stubenrauch, A.C.; Nikolaou, K.; et al. Coronary CT angiography in obese patients using 3rd generation dual-source CT: Effect of body mass index on image quality. Eur. Radiol. 2016, 26, 2937–2946. [Google Scholar] [CrossRef] [PubMed]
- Neglia, D.; Rovai, D.; Caselli, C.; Pietila, M.; Teresinska, A.; Aguadé-Bruix, S.; Pizzi, M.N.; Todiere, G.; Gimelli, A.; Schroeder, S.; et al. Detection of Significant Coronary Artery Disease by Noninvasive Anatomical and Functional Imaging. Circ. Cardiovasc. Imaging 2015, 8, 002179. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, L.H.; Ortner, N.; Nørgaard, B.; Achenbach, S.; Leipsic, J.; Abdulla, J. The diagnostic accuracy and outcomes after coronary computed tomography angiography vs. conventional functional testing in patients with stable angina pectoris: a systematic review and meta-analysis. Eur. Hear. J. Cardiovasc. Imaging 2014, 15, 961–971. [Google Scholar] [CrossRef]
- Arbab-Zadeh, A.; Di Carli, M.F.; Cerci, R.J.; George, R.T.; Chen, M.Y.; Dewey, M.; Niinuma, H.; Vavere, A.L.; Betoko, A.; Plotkin, M.; et al. Accuracy of Computed Tomographic Angiography and Single-Photon Emission Computed Tomography–Acquired Myocardial Perfusion Imaging for the Diagnosis of Coronary Artery Disease. Circ. Cardiovasc. Imaging 2015, 8, e003533. [Google Scholar] [CrossRef] [Green Version]
- Mark, D.B.; Federspiel, J.J.; Cowper, P.A.; Anstrom, K.J.; Hoffmann, U.; Patel, M.R.; Davidson-Ray, L.; Daniels, M.R.; Cooper, L.S.; Knight, J.D.; et al. Economic Outcomes With Anatomical Versus Functional Diagnostic Testing for Coronary Artery Disease. Ann. Intern. Med. 2016, 165, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.C.; Hunter, A.; Shah, A.; Assi, V.; Lewis, S.; Smith, J.; Berry, C.; Boon, N.A.; Clark, E.; Flather, M.; et al. Use of Coronary Computed Tomographic Angiography to Guide Management of Patients With Coronary Disease. J. Am. Coll. Cardiol. 2016, 67, 1759–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubbers, M.; Dedic, A.; Coenen, A.; Galema, T.; Akkerhuis, J.; Bruning, T.; Krenning, B.; Musters, P.; Ouhlous, M.; Liem, A.; et al. Calcium imaging and selective computed tomography angiography in comparison to functional testing for suspected coronary artery disease: The multicentre, randomized CRESCENT trial. Eur. Hear. J. 2016, 37, 1232–1243. [Google Scholar] [CrossRef] [Green Version]
- Lusis, A.J. Atherosclerosis. Nature 2000, 407, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Burke, A.P.; Farb, A.; Kolodgie, F.D. Pathology of the vulnerable plaque. J. Am. Coll. Cardiol. 2006, 47 (Suppl. 8), C13–C18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolossváry, M.; Szilveszter, B.; Merkely, B.; Maurovich-Horvat, P. Plaque imaging with CT—a comprehensive review on coronary CT angiography based risk assessment. Cardiovasc. Diagn. Ther. 2017, 7, 489–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadamitzky, M.; Achenbach, S.; Al-Mallah, M.; Berman, D.; Budoff, M.; Cademartiri, F.; Callister, T.; Chang, H.J.; Cheng, V.; Chinnaiyan, K.; et al. Optimized Prognostic Score for Coronary Computed Tomographic Angiography: Results From the CONFIRM Registry (COronary CT Angiography EvaluatioN For Clinical Outcomes: An InteRnational Multicenter Registry). J. Am. Coll. Cardiol. 2013, 62, 468–476. [Google Scholar] [CrossRef] [Green Version]
- Dedic, A.; Kurata, A.; Lübbers, M.; Meijboom, W.B.; Van Dalen, B.; Snelder, S.; Korbee, R.; Moelker, A.; Ouhlous, M.; Van Domburg, R.; et al. Prognostic implications of non-culprit plaques in acute coronary syndrome: Non-invasive assessment with coronary CT angiography. Eur. Hear. J. Cardiovasc. Imaging 2014, 15, 1231–1237. [Google Scholar] [CrossRef] [Green Version]
- Puchner, S.B.; Mayrhofer, T.; Park, J.; Lu, M.T.; Liu, T.; Maurovich-Horvat, P.; Ghemigian, K.; Bittner, D.O.; Fleg, J.L.; Udelson, J.E.; et al. Differences in the association of total versus local coronary artery calcium with acute coronary syndrome and culprit lesions in patients with acute chest pain: The coronary calcium paradox. Atherosclerosis 2018, 274, 251–257. [Google Scholar] [CrossRef]
- Korosoglou, G.; Giusca, S.; Katus, H.A. The coronary calcium paradox: Yet another step towards the differentiation between stable and rupture-prone coronary plaques? Atherosclerosis 2018, 274, 232–234. [Google Scholar] [CrossRef]
- Schaar, J.A.; Muller, J.E.; Falk, E.; Virmani, R.; Fuster, V.; Serruys, P.W.; Colombo, A.; Stefanadis, C.; Casscells, S.W.; Moreno, P.R.; et al. Terminology for high-risk and vulnerable coronary artery plaques. Eur. Hear. J. 2004, 25, 1077–1082. [Google Scholar] [CrossRef]
- Maurovich-Horvat, P.; Ferencik, M.; Voros, S.; Merkely, B.; Hoffmann, U. Comprehensive plaque assessment by coronary CT angiography. Nat. Rev. Cardiol. 2014, 11, 390–402. [Google Scholar] [CrossRef]
- Pohle, K.; Achenbach, S.; MacNeill, B.; Ropers, D.; Ferencik, M.; Moselewski, F.; Hoffmann, U.; Brady, T.J.; Jang, I.-K.; Daniel, W.G. Characterization of non-calcified coronary atherosclerotic plaque by multi-detector row CT: Comparison to IVUS. Atherosclerosis 2007, 190, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Zhang, Z.; Lu, B.; Yu, W.; Yang, Y.; Zhou, Y.; Wang, Y.; Fan, Z. Identification and Quantification of Coronary Atherosclerotic Plaques: A Comparison of 64-MDCT and Intravascular Ultrasound. Am. J. Roentgenol. 2008, 190, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, S.; Kondo, T.; Anno, H.; Sugiura, A.; Ito, Y.; Mori, K.; Ishii, J.; Sato, T.; Inoue, K.; Sarai, M.; et al. Atherosclerotic Plaque Characterization by 0.5-mm-Slice Multislice Computed Tomographic Imaging Comparison With Intravascular Ultrasound. Circ. J. 2007, 71, 363–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marwan, M.; Taher, M.A.; El Meniawy, K.; Awadallah, H.; Pflederer, T.; Schuhbäck, A.; Ropers, D.; Daniel, W.G.; Achenbach, S. In vivo CT detection of lipid-rich coronary artery atherosclerotic plaques using quantitative histogram analysis: A head to head comparison with IVUS. Atherosclerosis 2011, 215, 110–115. [Google Scholar] [CrossRef]
- Glagov, S.; Weisenberg, E.; Zarins, C.K.; Stankunavicius, R.; Kolettis, G.J. Compensatory Enlargement of Human Atherosclerotic Coronary Arteries. N. Engl. J. Med. 1987, 316, 1371–1375. [Google Scholar] [CrossRef] [PubMed]
- Varnava, A.M.; Mills, P.G.; Davies, M.J. Relationship Between Coronary Artery Remodeling and Plaque Vulnerability. Circulation 2002, 105, 939–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauss, S.; Achenbach, S.; Pflederer, T.; Schuhbäck, A.; Daniel, W.G.; Marwan, M. Assessment of coronary artery remodelling by dual-source CT: a head-to-head comparison with intravascular ultrasound. Heart 2011, 97, 991–997. [Google Scholar] [CrossRef]
- Hoffmann, U.; Moselewski, F.; Nieman, K.; Jang, I.-K.; Ferencik, M.; Rahman, A.M.; Cury, R.C.; Abbara, S.; Joneidi-Jafari, H.; Achenbach, S.; et al. Noninvasive Assessment of Plaque Morphology and Composition in Culprit and Stable Lesions in Acute Coronary Syndrome and Stable Lesions in Stable Angina by Multidetector Computed Tomography. J. Am. Coll. Cardiol. 2006, 47, 1655–1662. [Google Scholar] [CrossRef] [Green Version]
- Van Velzen, J.E.; de Graaf, F.R.; de Graaf, M.A.; Schuijf, J.D.; Kroft, L.J.; de Roos, A.; Reiber, J.H.C.; Bax, J.J.; Jukema, J.W.; Boersma, E.; et al. Comprehensive assessment of spotty calcifications on computed tomography angiography: Comparison to plaque characteristics on intravascular ultrasound with radiofrequency backscatter analysis. J. Nucl. Cardiol. 2011, 18, 893–903. [Google Scholar] [CrossRef] [Green Version]
- Pflederer, T.; Marwan, M.; Schepis, T.; Ropers, D.; Seltmann, M.; Muschiol, G.; Daniel, W.G.; Achenbach, S. Characterization of culprit lesions in acute coronary syndromes using coronary dual-source CT angiography. Atherosclerosis 2010, 211, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Maurovich-Horvat, P.; Hoffmann, U.; Vorpahl, M.; Nakano, M.; Virmani, R.; Alkadhi, H. The Napkin-Ring Sign: CT Signature of High-Risk Coronary Plaques? JACC: Cardiovasc. Imaging 2010, 3, 440–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifarth, H.; Schlett, C.L.; Nakano, M.; Otsuka, F.; Károlyi, M.; Liew, G.; Maurovich-Horvat, P.; Alkadhi, H.; Virmani, R.; Hoffmann, U. Histopathological correlates of the napkin-ring sign plaque in coronary CT angiography. Atherosclerosis 2012, 224, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Puchner, S.B.; Liu, T.; Mayrhofer, T.; Truong, Q.A.; Lee, H.; Fleg, J.L.; Nagurney, J.T.; Udelson, J.E.; Hoffmann, U.; Ferencik, M. High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: Results from the ROMICAT-II trial. J. Am. Coll. Cardiol. 2014, 64, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashiwagi, M.; Tanaka, A.; Shimada, K.; Kitabata, H.; Komukai, K.; Nishiguchi, T.; Ozaki, Y.; Tanimoto, T.; Kubo, T.; Hirata, K.; et al. Distribution, frequency and clinical implications of napkin-ring sign assessed by multidetector computed tomography. J. Cardiol. 2013, 61, 399–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feuchtner, G.; Kerber, J.; Burghard, P.; Dichtl, W.; Friedrich, G.; Bonaros, N.; Plank, F. The high-risk criteria low-attenuation plaque < 60 HU and the napkin-ring sign are the most powerful predictors of MACE: A long-term follow-up study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 772–779. [Google Scholar] [CrossRef] [Green Version]
- Ferencik, M.; Mayrhofer, T.; Bittner, D.O.; Emami, H.; Puchner, S.B.; Lu, M.T.; Meyersohn, N.M.; Ivanov, A.V.; Adami, E.C.; Patel, M.R.; et al. Use of High-Risk Coronary Atherosclerotic Plaque Detection for Risk Stratification of Patients With Stable Chest Pain: A Secondary Analysis of the PROMISE Randomized Clinical Trial. JAMA Cardiol. 2018, 3, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.C.; Kwiecinski, J.; Doris, M.; McElhinney, P.; D’Souza, M.S.; Cadet, S.; Adamson, P.D.; Moss, A.J.; Alam, S.; Hunter, A.; et al. Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction. Circulation 2020, 141, 1452–1462. [Google Scholar] [CrossRef] [Green Version]
- Korosoglou, G.; Lehrke, S.; Mueller, D.; Hosch, W.; Kauczor, H.-U.; Humpert, P.M.; Giannitsis, E.; A Katus, H. Determinants of troponin release in patients with stable coronary artery disease: Insights from CT angiography characteristics of atherosclerotic plaque. Heart 2010, 97, 823–831. [Google Scholar] [CrossRef]
- Gitsioudis, G.; Schüssler, A.; Nagy, E.; Maurovich-Horvat, P.; Buss, S.J.; Voss, A.; Hosch, W.; Hofmann, N.; Kauczor, H.-U.; Giannitsis, E.; et al. Combined Assessment of High-Sensitivity Troponin T and Noninvasive Coronary Plaque Composition for the Prediction of Cardiac Outcomes. Radiology 2015, 276, 141110-81. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, M.B.; Nordestgaard, B.G. Statin Use in Primary Prevention of Atherosclerotic Cardiovascular Disease According to 5 Major Guidelines for Sensitivity, Specificity, and Number Needed to Treat. JAMA Cardiol. 2019, 4, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Nicholls, S.J.; Sipahi, I.; Libby, P.; Raichlen, J.S.; Ballantyne, C.M.; Davignon, J.; Erbel, R.; Fruchart, J.C.; Tardif, J.C.; et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: The ASTEROID trial. JAMA 2006, 295, 1556–1565. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Ballantyne, C.M.; Barter, P.J.; Chapman, M.J.; Erbel, R.M.; Libby, P.; Raichlen, J.S.; Uno, K.; Borgman, M.; Wolski, K.; et al. Effect of Two Intensive Statin Regimens on Progression of Coronary Disease. N. Engl. J. Med. 2011, 365, 2078–2087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissen, S.E.; Tuzcu, E.M.; Schoenhagen, P.; Brown, B.G.; Ganz, P.; Vogel, R.A.; Crowe, T.; Howard, G.; Cooper, C.J.; Brodie, B.; et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: A randomized controlled trial. JAMA 2004, 291, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Agostoni, P.; Abbate, A.; Castagno, D.; Lipinski, M.J.; Vetrovec, G.W.; Frati, G.; Presutti, D.G.; Quadri, G.; Moretti, C.; et al. Atherosclerotic coronary plaque regression and the risk of adverse cardiovascular events: A meta-regression of randomized clinical trials. Atherosclerosis 2013, 226, 178–185. [Google Scholar] [CrossRef]
- Sandfort, V.; Lima, J.A.; Bluemke, D.A. Noninvasive Imaging of Atherosclerotic Plaque Progression. Circ. Cardiovasc. Imaging 2015, 8, e003316. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Park, H.-B.; Chang, H.-J.; Arsanjani, R.; Min, J.K.; Kim, Y.-J.; Lee, B.K.; Choi, J.-H.; Hong, G.-R.; Chung, N. Impact of Intensive LDL Cholesterol Lowering on Coronary Artery Atherosclerosis Progression: A Serial CT Angiography Study. JACC Cardiovasc. Imaging 2017, 10, 437–446. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Goeller, M.; Achenbach, S.; Cadet, S.; Kwan, A.C.; Commandeur, F.; Slomka, P.J.; Gransar, H.; Albrecht, M.H.; Tamarappoo, B.K.; Berman, D.S.; et al. Pericoronary Adipose Tissue Computed Tomography Attenuation and High-Risk Plaque Characteristics in Acute Coronary Syndrome Compared With Stable Coronary Artery Disease. JAMA Cardiol. 2018, 3, 858–863. [Google Scholar] [CrossRef] [Green Version]
- Antoniades, C.; Kotanidis, C.; Berman, D.S. State-of-the-art review article. Atherosclerosis affecting fat: What can we learn by imaging perivascular adipose tissue? J. Cardiovasc. Comput. Tomogr. 2019, 13, 288–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonopoulos, A.; Sanna, F.; Sabharwal, N.; Thomas, S.; Oikonomou, E.K.; Herdman, L.; Margaritis, M.; Shirodaria, C.; Kampoli, A.-M.; Akoumianakis, I.; et al. Detecting human coronary inflammation by imaging perivascular fat. Sci. Transl. Med. 2017, 9, eaal2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikonomou, E.K.; Marwan, M.; Desai, M.Y.; Mancio, J.; Alashi, A.; Centeno, E.H.; Thomas, S.; Herdman, L.; Kotanidis, C.; E Thomas, K.; et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. Lancet 2018, 392, 929–939. [Google Scholar] [CrossRef] [Green Version]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; Veer, M.V.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional Flow Reserve versus Angiography for Guiding Percutaneous Coronary Intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bruyne, B.; Pijls, N.H.; Kalesan, B.; Barbato, E.; Tonino, P.A.; Piroth, Z.; Jagic, N.; Mobius-Winckler, S.; Rioufol, G.; Witt, N.; et al. Fractional Flow Reserve–Guided PCI versus Medical Therapy in Stable Coronary Disease. N. Engl. J. Med. 2012, 367, 991–1001. [Google Scholar] [CrossRef] [Green Version]
- Pijls, N.H.; Sels, J.-W.E. Functional Measurement of Coronary Stenosis. J. Am. Coll. Cardiol. 2012, 59, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Toth, G.G.; Johnson, N.P.; Jeremias, A.; Pellicano, M.; Vranckx, P.; Fearon, W.F.; Barbato, E.; Kern, M.J.; Pijls, N.H.; De Bruyne, B. Standardization of Fractional Flow Reserve Measurements. J. Am. Coll. Cardiol. 2016, 68, 742–753. [Google Scholar] [CrossRef]
- Taylor, C.A.; Fonte, T.A.; Min, J.K. Computational Fluid Dynamics Applied to Cardiac Computed Tomography for Noninvasive Quantification of Fractional Flow Reserve: Scientific Basis. J. Am. Coll. Cardiol. 2013, 61, 2233–2241. [Google Scholar] [CrossRef] [Green Version]
- Koo, B.-K.; Erglis, A.; Doh, J.-H.; Daniels, D.V.; Jegere, S.; Kim, H.-S.; Dunning, A.; DeFrance, T.; Lansky, A.; Leipsic, J.; et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J. Am. Coll. Cardiol. 2011, 58, 1989–1997. [Google Scholar]
- Nørgaard, B.L.; Leipsic, J.; Gaur, S.; Seneviratne, S.; Ko, B.S.; Ito, H. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: The NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps). J. Am. Coll Cardiol. 2014, 63, 1145–1155. [Google Scholar] [CrossRef] [Green Version]
- Douglas, P.S.; De Bruyne, B.; Pontone, G.; Patel, M.R.; Norgaard, B.L.; Byrne, R.A.; Curzen, N.; Purcell, I.; Gutberlet, M.; Rioufol, G.; et al. 1-Year Outcomes of FFRCT-Guided Care in Patients With Suspected Coronary Disease: The PLATFORM Study. J. Am. Coll. Cardiol. 2016, 68, 435–445. [Google Scholar] [CrossRef]
- Driessen, R.S.; Danad, I.; Stuijfzand, W.J.; Raijmakers, P.G.; Schumacher, S.P.; van Diemen, P.A.; Leipsic, J.A.; Knuuti, J.; Underwood, S.R.; van de Ven, P.M.; et al. Comparison of Coronary Computed Tomography Angiography, Fractional Flow Reserve, and Perfusion Imaging for Ischemia Diagnosis. J. Am. Coll. Cardiol. 2019, 73, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Nørgaard, B.L.; Fairbairn, T.A.; Safian, R.D.; Rabbat, M.G.; Ko, B.; Jensen, J.M.; Nieman, K.; Chinnaiyan, K.M.; Sand, N.P.; Matsuo, H.; et al. Coronary CT Angiography-derived Fractional Flow Reserve Testing in Patients with Stable Coronary Artery Disease: Recommendations on Interpretation and Reporting. Radiol. Cardiothorac. Imaging 2019, 1, e190050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papafaklis, M.; Muramatsu, T.; Ishibashi, Y.; Lakkas, L.S.; Nakatani, S.; Bourantas, C.V.; Ligthart, J.; Onuma, Y.; Echavarria-Pinto, M.; Tsirka, G.; et al. Fast virtual functional assessment of intermediate coronary lesions using routine angiographic data and blood flow simulation in humans: Comparison with pressure wire – fractional flow reserve. EuroIntervention 2014, 10, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Siogkas, P.K.; Anagnostopoulos, C.D.; Liga, R.; Exarchos, T.P.; Sakellarios, A.I.; Rigas, G.; Scholte, A.J.H.A.; Papafaklis, M.I.; Loggitsi, D.; Pelosi, G.; et al. Noninvasive CT-based hemodynamic assessment of coronary lesions derived from fast computational analysis: a comparison against fractional flow reserve. Eur. Radiol. 2018, 29, 2117–2126. [Google Scholar] [CrossRef] [Green Version]
- Anagnostopoulos, C.D.; Siogkas, P.K.; Liga, R.; Benetos, G.; Maaniitty, T.; I Sakellarios, A.; Koutagiar, I.; Karakitsios, I.; I Papafaklis, M.; Berti, V.; et al. Characterization of functionally significant coronary artery disease by a coronary computed tomography angiography-based index: a comparison with positron emission tomography. Eur. Hear. J. Cardiovasc. Imaging 2019, 20, 897–905. [Google Scholar] [CrossRef]
- Sakellarios, A.I.; Rigas, G.; Kigka, V.; Siogkas, P.; Tsompou, P.; Karanasiou, G.; Exarchos, T.; Andrikos, I.; Tachos, N.; Pelosi, G.; et al. SMARTool: A tool for clinical decision support for the management of patients with coronary artery disease based on modeling of atherosclerotic plaque process. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, South Korea, 11–15 July 2017; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, SAD, 2017; Volume 2017, pp. 96–99. [Google Scholar]
- Sakellarios, A.I.; Pelosi, G.; Fotiadis, D.I.; Tsompou, P.; Siogkas, P.; Kigka, V.; Andrikos, I.; Tachos, N.; Georga, E.; Kyriakidis, S.; et al. Predictive Models of Coronary Artery Disease Based on Computational Modeling: The SMARTool System. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, SAD, 2019; Volume 2019, pp. 7002–7005. [Google Scholar]
- Sun, Z.; Xu, L. Computational fluid dynamics in coronary artery disease. Comput. Med Imaging Graph. 2014, 38, 651–663. [Google Scholar] [CrossRef]
- Carvalho, V.; Pinho, D.; Lima, R.A.; Teixeira, J.C.; Teixeira, S. Blood Flow Modeling in Coronary Arteries: A Review. Fluids 2021, 6, 53. [Google Scholar] [CrossRef]
- Gitsioudis, G.; Chatzizisis, Y.S.; Wolf, P.; Missiou, A.; Antoniadis, A.P.; Mitsouras, D.; Bartling, S.; Arica, Z.; Stuber, M.; Rybicki, F.J.; et al. Combined non-invasive assessment of endothelial shear stress and molecular imaging of inflammation for the prediction of inflamed plaque in hyperlipidaemic rabbit aortas. Eur. Hear. J. Cardiovasc. Imaging 2016, 18, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Samady, H.; Eshtehardi, P.; McDaniel, M.C.; Suo, J.; Dhawan, S.S.; Maynard, C.; Timmins, L.H.; Quyyumi, A.A.; Giddens, D.P. Coronary Artery Wall Shear Stress Is Associated With Progression and Transformation of Atherosclerotic Plaque and Arterial Remodeling in Patients With Coronary Artery Disease. Circulation 2011, 124, 779–788. [Google Scholar] [CrossRef] [Green Version]
- Stone, P.H.; Saito, S.; Takahashi, S.; Makita, Y.; Nakamura, S.; Kawasaki, T.; Takahashi, A.; Katsuki, T.; Nakamura, S.; Namiki, A.; et al. Response to Letter Regarding Article, “Prediction of Progression of Coronary Artery Disease and Clinical Outcomes Using Vascular Profiling of Endothelial Shear Stress and Arterial Plaque Characteristics: The PREDICTION Study. ” Circulation 2013, 127, e489–e490. [Google Scholar] [CrossRef] [Green Version]
- Hetterich, H.; Jaber, A.; Gehring, M.; Curta, A.; Bamberg, F.; Filipovic, N.; Rieber, J. Coronary Computed Tomography Angiography Based Assessment of Endothelial Shear Stress and Its Association with Atherosclerotic Plaque Distribution In-Vivo. PLoS ONE 2015, 10, e0115408. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Choi, G.; Koo, B.-K.; Hwang, D.; Park, J.; Zhang, J.; Kim, K.-J.; Tong, Y.; Kim, H.J.; Grady, L.; et al. Identification of High-Risk Plaques Destined to Cause Acute Coronary Syndrome Using Coronary Computed Tomographic Angiography and Computational Fluid Dynamics. JACC: Cardiovasc. Imaging 2019, 12, 1032–1043. [Google Scholar] [CrossRef]
- Salerno, M.; Beller, G.A. Noninvasive Assessment of Myocardial Perfusion. Circ. Cardiovasc. Imaging 2009, 2, 412–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, D.H.; Kim, Y.-H. CT myocardial perfusion imaging: Current status and future perspectives. Int. J. Cardiovasc. Imaging 2017, 52, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Techasith, T.; Cury, R.C. Stress myocardial CT perfusion: An update and future perspective. JACC Cardiovasc. Imaging 2011, 4, 905–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochitte, C.E.; George, R.T.; Chen, M.Y.; Arbab-Zadeh, A.; Dewey, M.; Miller, J.M.; Niinuma, H.; Yoshioka, K.; Kitagawa, K.; Nakamori, S.; et al. Computed tomography angiography and perfusion to assess coronary artery stenosis causing perfusion defects by single photon emission computed tomography: the CORE320 study. Eur. Hear. J. 2014, 35, 1120–1130. [Google Scholar] [CrossRef] [PubMed]
- Pontone, G.; Baggiano, A.; Andreini, D.; Guaricci, A.I.; Guglielmo, M.; Muscogiuri, G.; Fusini, L.; Fazzari, F.; Mushtaq, S.; Conte, E.; et al. Stress Computed Tomography Perfusion Versus Fractional Flow Reserve CT Derived in Suspected Coronary Artery Disease: The Perfection Study. JACC Cardiovasc Imaging 2019, 12, 1487–1497. [Google Scholar] [CrossRef]
- Andreini, D.; Mushtaq, S.; Pontone, G.; Conte, E.; Collet, C.; Sonck, J.; D’Errico, A.; Di Odoardo, L.; Guglielmo, M.; Baggiano, A.; et al. CT Perfusion Versus Coronary CT Angiography in Patients With Suspected In-Stent Restenosis or CAD Progression. JACC: Cardiovasc. Imaging 2020, 13, 732–742. [Google Scholar] [CrossRef] [PubMed]
- SCOT-HEART Investigators. Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. N. Engl. J. Med. 2018, 379, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Douglas, P.S.; Hoffmann, U.; Patel, M.R.; Mark, D.B.; Al-Khalidi, H.R.; Cavanaugh, B.; Cole, J.; Dolor, R.J.; Fordyce, C.B.; Huang, M.; et al. Outcomes of Anatomical versus Functional Testing for Coronary Artery Disease. N. Engl. J. Med. 2015, 372, 1291–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, U.; Ferencik, M.; Udelson, J.E.; Picard, M.H.; Truong, Q.A.; Patel, M.R.; Huang, M.; Pencina, M.; Mark, D.B.; Heitner, J.F.; et al. Prognostic Value of Noninvasive Cardiovascular Testing in Patients with Stable Chest Pain: Insights from the PROMISE Trial. Circulation 2017, 135, 2320–2332. [Google Scholar] [CrossRef]
- Chow, B.J.W.; Wells, G.A.; Chen, L.; Yam, Y.; Galiwango, P.; Abraham, A.; Sheth, T.; Dennie, C.; Beanlands, R.S.; Ruddy, T.A. Prognostic value of 64-slice cardiac computed tomography severity of coronary artery disease, coronary atherosclerosis, and left ventricular ejection fraction. J. Am. Coll. Cardiol. 2010, 55, 1017–1028. [Google Scholar] [CrossRef] [Green Version]
- Hadamitzky, M.; Täubert, S.; Deseive, S.; Byrne, R.; Martinoff, S.; Schömig, A.; Hausleiter, J. Prognostic value of coronary computed tomography angiography during 5 years of follow-up in patients with suspected coronary artery disease. Eur. Hear. J. 2013, 34, 3277–3285. [Google Scholar] [CrossRef] [Green Version]
- Chow, B.J.W.; Yam, Y.; Small, G.; A Wells, G.; Crean, A.M.; Ruddy, T.D.; Hossain, A. Prognostic durability of coronary computed tomography angiography. Eur. Hear. J. Cardiovasc. Imaging 2021, 22, 331–338. [Google Scholar] [CrossRef]
- Park, K.W.; Kim, C.-H.; Lee, H.-Y.; Kang, H.-J.; Koo, B.-K.; Oh, B.-H.; Park, Y.-B.; Kim, H.-S. Does “late catch-up” exist in drug-eluting stents: Insights from a serial quantitative coronary angiography analysis of sirolimus versus paclitaxel-eluting stents. Am. Hear. J. 2010, 159, 446–453.e3. [Google Scholar] [CrossRef]
- Mahnken, A.H. CT Imaging of Coronary Stents: Past, Present, and Future. ISRN Cardiol. 2012, 2012, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Sun, Z.; Almutairi, A.M.D. Diagnostic accuracy of 64 multislice CT angiography in the assessment of coronary in-stent restenosis: A meta-analysis. Eur. J. Radiol. 2010, 73, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Carrabba, N.; Schuijf, J.D.; De Graaf, F.R.; Parodi, G.; Maffei, E.; Valenti, R.; Palumbo, A.; Weustink, A.C.; Mollet, N.R.; Accetta, G.; et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography for the detection of in-stent restenosis: A meta-analysis. J. Nucl. Cardiol. 2010, 17, 470–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumbhani, D.J.; Ingelmo, C.P.; Schoenhagen, P.; Curtin, R.J.; Flamm, S.D.; Desai, M.Y. Meta-Analysis of Diagnostic Efficacy of 64-Slice Computed Tomography in the Evaluation of Coronary In-Stent Restenosis. Am. J. Cardiol. 2009, 103, 1675–1681. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, F.; Weustink, A.C.; Van Mieghem, C.; Alberghina, F.; Otsuka, M.; Meijboom, W.B.; Van Pelt, N.; Mollet, N.R.; Cademartiri, F.; Krestin, G.P.; et al. Dual source coronary computed tomography angiography for detecting in-stent restenosis. Heart 2008, 94, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Carbone, I.; Francone, M.; Algeri, E.; Granatelli, A.; Napoli, A.; Kirchin, M.A.; Catalano, C.; Passariello, R. Non-invasive evaluation of coronary artery stent patency with retrospectively ECG-gated 64-slice CT angiography. Eur. Radiol. 2007, 18, 234–243. [Google Scholar] [CrossRef]
- Pflederer, T.; Marwan, M.; Renz, A.; Bachmann, S.; Ropers, D.; Kuettner, A.; Anders, K.; Bamberg, F.; Werner, G.D.; Achenbach, S. Noninvasive assessment of coronary in-stent restenosis by dual-source computed tomography. Am. J. Cardiol. 2009, 103, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Van Mieghem, C.A.G.; Cademartiri, F.; Mollet, N.R.; Malagutti, P.; Valgimigli, M.; Meijboom, W.B. Multislice spiral computed tomography for the evaluation of stent patency after left main coronary artery stenting: A comparison with conventional coronary angiography and intravascular ultrasound. Circulation 2006, 114, 645–653. [Google Scholar] [CrossRef]
- Öncel, D.; Oncel, G.; Taştan, A.; Tamci, B. Evaluation of Coronary Stent Patency and In-Stent Restenosis with Dual-Source CT Coronary Angiography Without Heart Rate Control. Am. J. Roentgenol. 2008, 191, 56–63. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; A Byrne, R.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Hear. J. 2018, 40, 87–165. [Google Scholar] [CrossRef]
- Goldman, S.; Zadina, K.; Moritz, T.; Ovitt, T.; Sethi, G.; Copeland, J.G.; Thottapurathu, L.; Krasnicka, B.; Ellis, N.; Anderson, R.J.; et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: Results from a Department of Veterans Affairs Cooperative Study. J. Am. Coll. Cardiol. 2004, 44, 2149–2156. [Google Scholar] [CrossRef]
- Di Lazzaro, D.; Crusco, F. CT angio for the evaluation of graft patency. J. Thorac. Dis. 2017, 9, S283–S288. [Google Scholar] [CrossRef] [Green Version]
- Barbero, U.; Iannaccone, M.; D’Ascenzo, F.; Barbero, C.; Mohamed, A.; Annone, U.; Benedetto, S.; Celentani, D.; Gagliardi, M.; Moretti, C.; et al. 64 slice-coronary computed tomography sensitivity and specificity in the evaluation of coronary artery bypass graft stenosis: A meta-analysis. Int. J. Cardiol. 2016, 216, 52–57. [Google Scholar] [CrossRef]
- Chan, M.; Ridley, L.; Dunn, D.J.; Tian, D.H.; Liou, K.; Ozdirik, J.; Cheruvu, C.; Cao, C. A systematic review and meta-analysis of multidetector computed tomography in the assessment of coronary artery bypass grafts. Int. J. Cardiol. 2016, 221, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Collet, C.; Onuma, Y.; Andreini, D.; Sonck, J.; Pompilio, G.; Mushtaq, S.; La Meir, M.; Miyazaki, Y.; De Mey, J.; Gaemperli, O.; et al. Coronary computed tomography angiography for heart team decision-making in multivessel coronary artery disease. Eur. Hear. J. 2018, 39, 3689–3698. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Seo, J.B.; Do, K.-H.; Heo, J.-N.; Lee, J.S.; Song, J.-W.; Choe, Y.H.; Kim, T.H.; Yong, H.S.; Choi, S.I.; et al. Coronary Artery Anomalies: Classification and ECG-gated Multi–Detector Row CT Findings with Angiographic Correlation. Radiographics 2006, 26, 317–333. [Google Scholar] [CrossRef]
- Salehi, S.; Suri, K.; Najafi, M.H.; Assadi, M.; Toudeshki, E.A.H.; Alizadeh, N.S.; Gholamrezanezhad, A. Computed Tomography Angiographic Features of Anomalous Origination of the Coronary Arteries in Adult Patients: A Literature Review and Coronary Computed Tomography Angiographic Illustrations. Curr. Probl. Diagn. Radiol. 2021. [Google Scholar] [CrossRef]
- Gräni, C.; Buechel, R.R.; Kaufmann, P.A.; Kwong, R.Y. Multimodality Imaging in Individuals With Anomalous Coronary Arteries. JACC: Cardiovasc. Imaging 2017, 10, 471–481. [Google Scholar] [CrossRef]
- Angelini, P. Coronary artery anomalies: An entity in search of an identity. Circulation 2007, 115, 1296–1305. [Google Scholar] [CrossRef]
- Ferreira, A.G.; E Trotter, S.; Konig, B.; Decourt, L.V.; Fox, K.; Olsen, E.G. Myocardial bridges: Morphological and functional aspects. Heart 1991, 66, 364–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zenooz, N.A.; Habibi, R.; Mammen, L.; Finn, J.P.; Gilkeson, R.C. Coronary Artery Fistulas: CT Findings. Radiographics 2009, 29, 781–789. [Google Scholar] [CrossRef]
- Blanke, P.; Weir-McCall, J.R.; Achenbach, S.; Delgado, V.; Hausleiter, J.; Jilaihawi, H.; Marwan, M.; Nørgaard, B.; Piazza, N.; Schoenhagen, P.; et al. Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI) / transcatheter aortic valve replacement (TAVR): An expert consensus document of the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2019, 13, 1–20. [Google Scholar] [CrossRef]
- Ge, Y.; Gupta, S.; Fentanes, E.; Aghayev, A.; Steigner, M.; Sobieszczyk, P.; Kaneko, T.; Di Carli, M.F.; Bhatt, D.L.; Shah, P.; et al. Role of Cardiac CT in Pre-Procedure Planning for Transcatheter Mitral Valve Replacement. JACC: Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Storz, C.; Mangold, S.; Mueller, K.A.; Lausberg, H.; Gatidis, S.; Heber, S.D.; Schlett, C.L.; Nikolaou, K.; Bamberg, F. Cardiac CT for Guiding Mitral Valve Interventions. Curr. Cardiovasc. Imaging Rep. 2017, 10, 31. [Google Scholar] [CrossRef]
- Van Rosendael, P.J.; Kamperidis, V.; Kong, W.K.F.; van Rosendael, A.R.; van der Kley, F.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Computed tomography for planning transcatheter tricuspid valve therapy. Eur. Heart J. 2017, 38, 665–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liddy, S.; Buckley, U.; Kok, H.K.; Loo, B.; Glover, B.; Dhillon, G.R.; Buckley, O. Applications of cardiac computed tomography in electrophysiology intervention. Eur. Hear. J. Cardiovasc. Imaging 2017, 19, 253–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Kanaji, Y.; Miyazaki, S.; Iwasawa, J.; Ichihara, N.; Takagi, T.; Kuroi, A.; Nakamura, H.; Taniguchi, H.; Hachiya, H.; Iesaka, Y. Pre-procedural evaluation of the left atrial anatomy in patients referred for catheter ablation of atrial fibrillation. J. Cardiol. 2016, 67, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Velthuis, B.O.; Molenaar, M.; Dorman, H.G.R.; Stevenhagen, J.Y.; Scholten, M.F.; Van Der Palen, J.; Van Opstal, J.M. Use of three-dimensional computed tomography overlay for real-time cryoballoon ablation in atrial fibrillation reduces radiation dose and contrast dye. Neth. Hear. J. 2017, 25, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Marques, H.; Gonçalves, P.D.A.; Ferreira, A.M.; Cruz, R.; Lopes, J.; Dos Santos, R.; Radu, L.; Costa, F.; Mesquita, J.; Carmo, P.; et al. Cardiac computed tomography prior to atrial fibrillation ablation: Effects of technological advances and protocol optimization. Rev. Port. Cardiol. Engl. Ed. 2018, 37, 873–883. [Google Scholar] [CrossRef]
- Romero, J.; Husain, S.A.; Kelesidis, I.; Sanz, J.; Medina, H.M.; Garcia, M.J. Detection of Left Atrial Appendage Thrombus by Cardiac Computed Tomography in Patients With Atrial Fibrillation. Circ. Cardiovasc. Imaging 2013, 6, 185–194. [Google Scholar] [CrossRef] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maximal Coronary Artery Stenosis Severity (Per Patient) | Interpretation | Further Recommendations | |
|---|---|---|---|
| CAD-RADS 0 | 0% | “no plaque or stenosis” | None |
| CAD-RADS 1 | 1–24% | “plaque without stenosis” | None |
| CAD-RADS 2 | 25–49% | “mild stenosis” | None |
| CAD-RADS 3 | 50–69% | “moderate stenosis” | Consider functional testing |
| CAD-RADS 4A | 70–99% | “severe stenosis” | Consider functional testing or ICA |
| CAD-RADS 4B | Left main > 50% or 3-vessel disease ≥70% | “severe stenosis” | ICA is recommended |
| CAD-RADS 5 | 100% | Total coronary occlusion | ICA and/or test for viability |
| CAD—RADS N | Non diagnostic | CAD cannot be excluded | Consider alternative tests |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giusca, S.; Schütz, M.; Kronbach, F.; Wolf, D.; Nunninger, P.; Korosoglou, G. Coronary Computer Tomography Angiography in 2021—Acquisition Protocols, Tips and Tricks and Heading beyond the Possible. Diagnostics 2021, 11, 1072. https://doi.org/10.3390/diagnostics11061072
Giusca S, Schütz M, Kronbach F, Wolf D, Nunninger P, Korosoglou G. Coronary Computer Tomography Angiography in 2021—Acquisition Protocols, Tips and Tricks and Heading beyond the Possible. Diagnostics. 2021; 11(6):1072. https://doi.org/10.3390/diagnostics11061072
Chicago/Turabian StyleGiusca, Sorin, Moritz Schütz, Florian Kronbach, David Wolf, Peter Nunninger, and Grigorios Korosoglou. 2021. "Coronary Computer Tomography Angiography in 2021—Acquisition Protocols, Tips and Tricks and Heading beyond the Possible" Diagnostics 11, no. 6: 1072. https://doi.org/10.3390/diagnostics11061072