
Thoracic Aortic Calcification and Pre-Clinical Hypertension by New 2017 ACC/AHA Hypertension Guidelines

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Anthropometric Measures and Biochemical Data
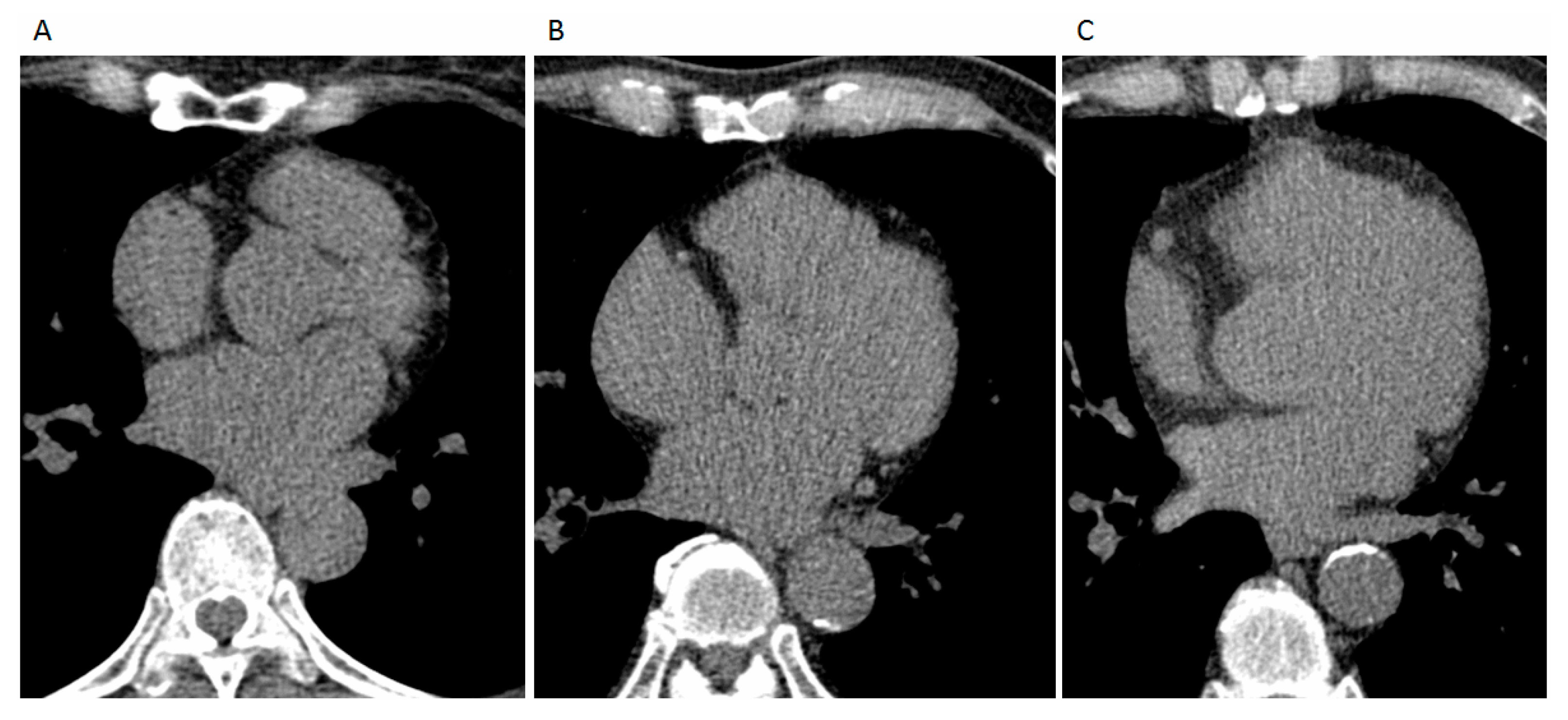
2.3. Semi-Automatic Quantification of Three-Dimensional (3D) Thoracic Aortic Calcification
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographics
3.2. Coronary and Thoracic Aortic Calcification across Four Categories by ACC/AHA Hypertension Guidelines
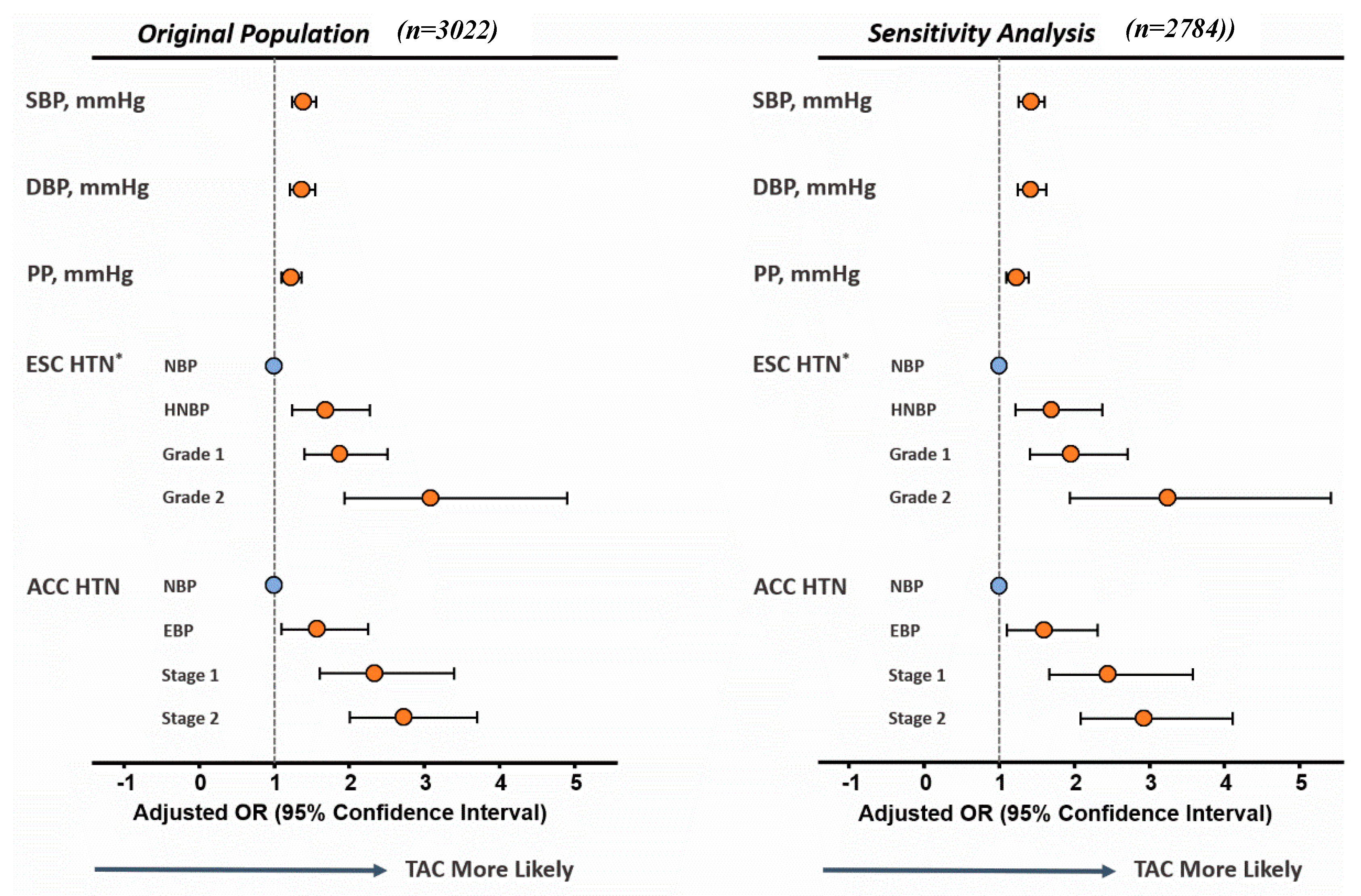
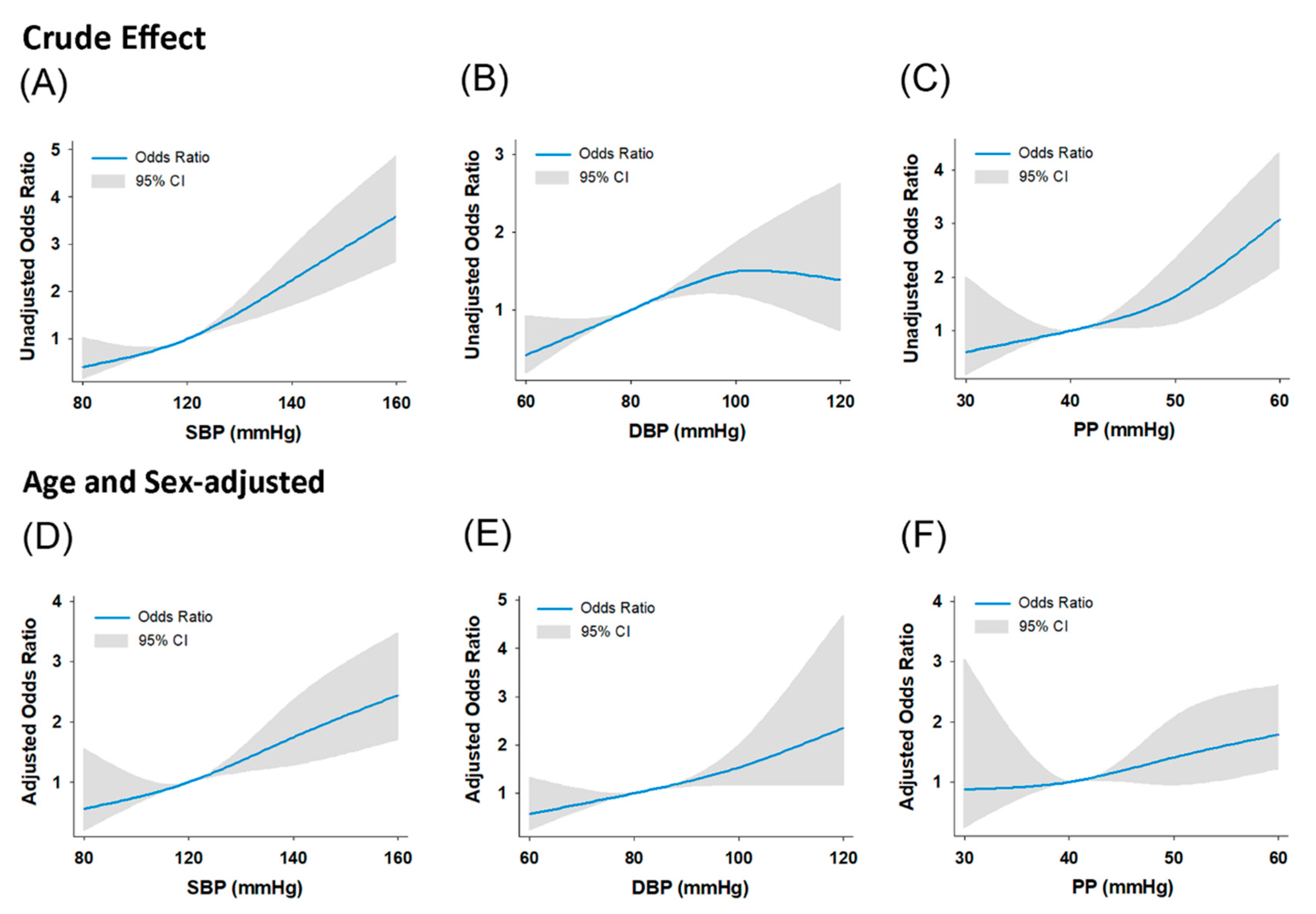
3.3. Associations of Blood Pressure Components with Coronary and Thoracic Aortic Calcification
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BP | blood pressure |
| CT | computed tomography |
| CAC | coronary artery calcification |
| CVD | cardiovascular diseases |
| DBP | diastolic blood pressure |
| HF | heart failure |
| HFpEF | heart failure with preserved ejection fraction |
| HTN | hypertension |
| MDCT | multi-detector computed tomography |
| PP | pulse pressure |
| SBP | systolic blood pressure |
| TAC | systolic blood pressure |
References
- Lawes, C.M.; Hoorn, S.V.; Rodgers, A.; International Society of Hypertension. Global burden of blood-pressure-related disease, 2001. Lancet 2008, 371, 1513–1518. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, N.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- Dzau, V.J.; Antman, E.M.; Black, H.R.; Hayes, D.L.; Manson, J.E.; Plutzky, J.; Popma, J.J.; Stevenson, W. The cardiovascular disease continuum validated: Clinical evidence of improved patient outcomes: Part I: Pathophysiology and clinical trial evidence (risk factors through stable coronary artery disease). Circulation 2006, 114, 2850–2870. [Google Scholar] [CrossRef]
- Kälsch, H.; Lehmann, N.; Möhlenkamp, S.; Hammer, C.; Mahabadi, A.A.; Moebus, S.; Schmermund, A.; Stang, A.; Bauer, M.; Jöckel, K.; et al. Prevalence of thoracic aortic calcification and its relationshipto cardiovascular risk factors and coronary calcification in an unselected population-based cohort: The Heinz Nixdorf Recall Study. Int. J. Cardiovasc. Imaging 2013, 29, 207–216. [Google Scholar] [CrossRef]
- Budoff, M.J.; Nasir, K.; Katz, R.; Takasu, J.; Carr, J.J.; Wong, N.D.; Allison, M.; Lima, J.A.C.; Detrano, R.; Blumenthal, R.S.; et al. Thoracic aortic calcification and coronary heart disease events: The multi-ethnic study of atherosclerosis (MESA). Atherosclerosis 2011, 215, 196–202. [Google Scholar] [CrossRef] [Green Version]
- Eisen, A.; Tenenbaum, A.; Koren-Morag, N.; Tanne, D.; Shemesh, J.; Imazio, M.; Fisman, E.Z.; Motro, M.; Schwammenthal, E.; Adler, Y. Calcification of the thoracic aorta as detected by spiral computed tomography among stable angina pectoris patients: Association withcardiovascular events and death. Circulation 2008, 118, 1328–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, R.D.; Rumberger, J.A.; Budoff, M.J.; Shaw, L.J.; Orakzai, S.H.; Berman, D.; Raggi, P.; Blumenthal, R.S.; Nasir, K. Thoracic aorta calcification detected by electron beam tomography predicts all-cause mortality. Atherosclerosis 2010, 209, 131–135. [Google Scholar] [CrossRef]
- Thomas, I.C.; Thompson, C.A.; Yang, M.; Allison, M.A.; Forbang, N.I.; Michos, E.D.; McClelland, R.L.; Budoff, M.J.; Criqui, M.H. Thoracic Aorta Calcification and Noncardiovascular Disease-Related Mortality. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 1926–1932. [Google Scholar] [CrossRef] [Green Version]
- Takasu, J.; Katz, R.; Nasir, K.; Carr, J.J.; Wong, N.; Detrano, R.; Budoff, M.J. Relationships of thoracic aortic wall calcification to cardiovascular risk factors: The Multi-Ethnic Study of Atherosclerosis (MESA). Am. Heart J. 2008, 155, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Youssef, G.; Guo, M.; McClelland, R.L.; Shavelle, D.M.; Nasir, K.; Rivera, J.; Carr, J.J.; Wong, N.D.; Budoff, M.J. Risk Factors for the Development and Progression of Thoracic Aorta Calcification: The Multi-Ethnic Study of Atherosclerosis. Acad. Radiol. 2015, 22, 1536–1545. [Google Scholar] [CrossRef] [Green Version]
- Kälsch, H.; Lehmann, N.; Moebus, S.; Hoffmann, B.; Stang, A.; Jöckel, K.; Erbel, R.; Mahabadi, A.A. Aortic Calcification Onset and Progression: Association With the Development of Coronary Atherosclerosis. J. Am. Heart Assoc. 2017, 6, e005093. [Google Scholar] [CrossRef] [Green Version]
- Park, J.B.; Kario, K.; Wang, J.G. Systolic hypertension: An increasing clinicalchallenge in Asia. Hypertens Res. 2015, 38, 227–236. [Google Scholar] [CrossRef] [Green Version]
- Arima, H.; Murakami, Y.; Lam, T.H.; Kim, H.C.; Ueshima, H.; Woo, J.; Suh, I.; Fang, X.; Woodward, M.; Asia Pacific Cohort Studies Collaboration. Effects of prehypertension and hypertension subtype on cardiovascular disease in the Asia-Pacific Region. Hypertension 2012, 59, 1118–1123. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Tsai, J.; Kuo, R.; Sun, J.; Yun, C.; Sung, K.; Liu, C.; Kuo, J.; Hung, C.; Wu, T.; Lin, J.; et al. Thoracic aortic calcification across the clinical dysglycemic continuum in a large Asian population free of cardiovascular symptoms. PLoS ONE 2019, 14, e0207089. [Google Scholar]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Desai, M.Y.; Cremer, P.C.; Schoenhagen, P. Thoracic Aortic Calcification: Diagnostic, Prognostic, and Management Considerations. JACC Cardiovasc. Imaging 2018, 11, 1012–1026. [Google Scholar] [CrossRef] [PubMed]
- Zalghout, S.; Kaplan, A.; Abidi, E.; El-Achkar, G.A.; Nour-Eldine, W.; Khalil, A.A.; Kobeissy, F.; Husari, A.; Habib, A.; Zouein, F.A.; et al. Tobacco cigarette smoking exacerbates aortic calcification in an early stage of myocardial infarction in a female mouse model. J. Cell. Physiol. 2020, 235, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.S.; Cheng, S.L.; Sadhu, J.; Towler, D.A. Inflammation and the osteogenic regulation of vascular calcification: A review and perspective. Hypertension 2010, 55, 579–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, C.W.; Pencina, K.M.; Massaro, J.M.; Benjamin, E.J.; Levy, D.; Vasan, R.S.; Hoffmann, U.; O’Donnell, C.J.; Mitchell, G.F. Cross-sectional relations of arterial stiffness, pressure pulsatility, wave reflection, and arterial calcification. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2495–2500. [Google Scholar] [CrossRef] [Green Version]
- Jensky, N.E.; Criqui, M.H.; Wright, M.C.; Wassel, C.L.; Brody, S.A.; Allison, M.A. Blood Pressure and Vascular Calcification. Hypertension 2010, 55, 990–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEniery, C.M.; McDonnell, B.J.; So, A.; Aitken, S.; Bolton, C.E.; Munnery, M.; Hickson, S.S.; Yasmin; Maki-Petaja, K.M.; Cockcroft, J.R.; et al. Aortic calcification is associated with aortic stiffness and isolated systolic hypertension in healthy individuals. Hypertension 2009, 53, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Sekikawa, A.; Shin, C.; Curb, J.D.; Barinas-Mitchell, E.; Masaki, K.; El-Saed, A.; Seto, T.B.; Mackey, R.H.; Choo, J.; Fujiyoshi, A.; et al. Aortic stiffness and calcification in men in a population-based international study. Atherosclerosis 2012, 222, 473–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cecelja, M.; Hussain, T.; Greil, G.; Botnar, R.; Preston, R.; Moayyeri, A.; Spector, T.D.; Chowienczyk, P. Multimodality imaging of subclinical aortic atherosclerosis: Relation of aortic stiffness to calcification and plaque in female twins. Hypertension 2013, 61, 609–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ata Korkmaz, A.; Akyuz, A.R. Aortic knob calcification and cardioankle vascular index in asymptomatic hypertensive patients. Blood Press Monit. 2017, 22, 8–11. [Google Scholar] [CrossRef]
- Guo, J.; Fujiyoshi, A.; Willcox, B.; Choo, J.; Vishnu, A.; Hisamatsu, T.; Ahuja, V.; Takashima, N.; Barinas-Mitchell, E.; Kadota, A.; et al. Increased Aortic Calcification Is Associated With Arterial Stiffness Progression in Multiethnic Middle-Aged Men. Hypertension 2017, 69, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Cecelja, M.; Jiang, B.; Bevan, L.; Frost, M.L.; Spector, T.D.; Chowienczyk, P.J. Arterial Stiffening Relates to Arterial Calcification But Not to Noncalcified Atheroma in Women. J. Am. Coll. Cardiol. 2011, 57, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Amann, K. Media calcification and intima. calcification are distinct entities in chronic kidney disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1599–1605. [Google Scholar] [CrossRef] [Green Version]
- Kaess, B.M.; Rong, J.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S.; Mitchell, G.F. Aortic Stiffness, Blood Pressure Progression, and Incident Hypertension. JAMA 2012, 308, 875–881. [Google Scholar] [CrossRef] [Green Version]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.M.; Wang, J.J.; Chen, C.H. The Role of Vascular Calcification in Heart Failure and Cognitive Decline. Pulse 2017, 5, 144–153. [Google Scholar] [CrossRef]
- Heinzel, F.R.; Hohendanner, F.; Jin, G.; Sedej, S.; Edelmann, F. Myocardial hypertrophy and its role in heart failure with preserved ejection fraction. J. Appl. Physiol. 2015, 119, 1233–1242. [Google Scholar] [CrossRef]
- Cho, I.J.; Chang, H.J.; Lee, S.E.; Shim, C.Y.; Hong, G.R.; Chung, N. Prognostic Application of Thoracic Aortic Calcium Scoring for Adverse Clinical Outcome Risk in Elderly Patients with Left Ventricular Hypertrophy. Korean Circ. J. 2017, 47, 918–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonini-Canterin, F.; Poli, S.; Vriz, O.; Pavan, D.; di Bello, V.; Nicolosi, G.L. The Ventricular-Arterial Coupling: From Basic Pathophysiology to Clinical Application in the Echocardiography Laboratory. J. Cardiovasc. Echogr. 2013, 23, 91–95. [Google Scholar] [CrossRef] [PubMed]
- SPRINT Research Group; Wright, J.T., Jr.; Williamson, J.D.; Whelton, P.K.; Snyder, J.K.; Sink, K.M.; Rocco, M.V.; Reboussin, D.M.; Rahman, M.; Oparil, S.; et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [PubMed]
- Cushman, W.C.; Whelton, P.K.; Fine, L.J.; Wright, J.T., Jr.; Reboussin, D.M.; Johnson, K.C.; Oparil, S.; SPRINT Study Research Group. SPRINT Trial Results: Latest News in Hypertension Management. Hypertension 2016, 67, 263–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craiem, D.; Casciaro, M.; Pascaner, A.; Soulat, G.; Guilenea, F.; Sirieix, M.E.; Simon, A.; Mousseaux, E. Association of calcium density in the thoracic aorta with risk factors and clinical events. Eur. Radiol. 2020, 30, 3960–3967. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Study Participants | NBP | EBP | S1 HTN | S2 HTN) | p-Value (Trend) | |
|---|---|---|---|---|---|---|
| (n = 3022) | (n = 1204) | (n = 591) | (n = 383) | (n = 844) | ||
| Clinical feature | ||||||
| Age (years) | 49.4 ± 9.5 | 47.0 ± 8.6 | 48.4 ± 9.4 * | 50.3 ± 9.8 *a | 53.6 ± 9.6 *bc | <0.01 |
| Male gender | 2161 (71.5%) | 779 (64.7%) | 426 (72.1%) | 296 (77.3%) | 660 (78.2%) | <0.01 |
| BMI (kg/m2) | 24.69 ± 3.51 | 23.39 ± 2.97 | 24.67 ± 3.15 * | 25.50 ± 3.62 *a | 26.18 ± 3.72 *bc | <0.01 |
| WHR | 0.88 ± 0.07 | 0.86 ± 0.07 | 0.89 ± 0.06 * | 0.90 ± 0.65 *a | 0.91 ± 0.06 *bc | <0.01 |
| Body fat (%) | 26.08 ± 6.59 | 24.87 ± 6.04 | 25.98 ± 6.32 * | 26.50 ± 6.90 * | 27.74 ± 7.05 *bc | <0.01 |
| Biochemistry data | ||||||
| Hemoglobin A1c (%) | 5.86 ± 0.88 | 5.66 ± 0.60 | 5.79 ± 0.77 * | 5.98 ± 1.05 *a | 6.13 ± 1.09 *b | <0.01 |
| Total cholesterol (mg/dL) | 201.96 ± 36.61 | 198.20 ± 35.62 | 203.93 ± 36.27 * | 203.85 ± 34.93 * | 205.09 ± 38.56 *b | <0.01 |
| Triglyceride (mg/dL) | 141.81 ± 116.10 | 122.51 ± 79.88 | 139.72 ± 81.96 * | 153.97 ± 100.34 * | 165.34 ± 169.71 *b | <0.01 |
| LDL cholesterol (mg/dL) | 130.48 ± 32.48 | 127.72 ± 32.31 | 133.54 ± 32.58 * | 131.99 ± 31.75 | 131.61 ± 32.02* | NS |
| HDL cholesterol (mg/dL) | 52.35 ± 14.09 | 54.68 ± 15.05 | 52.20 ± 13.93 * | 50.88 ± 13.60 *a | 49.78 ± 12.41 * | <0.01 |
| Uric acid (mg/dL) | 6.03 ± 1.44 | 5.73 ± 1.42 | 6.11 ± 1.41 * | 6.15 ± 1.42 * | 6.35 ± 1.44 *b | <0.01 |
| eGFR (ml/min/1.73 m2) | 82.81 ± 15.16 | 85.26 ± 15.72 | 83.73 ± 14.90 | 82.69 ± 15.74 *a | 79.57 ± 16.49 *bc | <0.01 |
| hs-CRP (mg/dL) | 0.20 ± 0.41 | 0.16 ± 0.34 | 0.19 ± 0.35 | 0.20 ± 0.33 | 0.27 ± 0.56 * | <0.01 |
| Homocysteine (µmol/L) | 9.31 ± 4.04 | 8.86 ± 3.69 | 9.32 ± 3.93 | 10.00 ± 5.32 | 9.67 ± 3.96 * | <0.01 |
| Medical History | ||||||
| Dyslipidemia | 158 (5.2%) | 31 (2.5%) | 22 (3.7%) | 12 (3.1%) | 93 (11.0%) *bc | <0.01 |
| CVD | 133 (4.4%) | 26 (2.1%) | 9 (1.5%) | 9 (2.3 %) | 89 (10.5%) *bc | <0.01 |
| Stroke | 13 (0.43%) | 1 (0.08%) | 1 (0.16%) | 0 (0%) | 11 (1.3%) * | <0.01 |
| Diabetes | 174 (5.7%) | 21 (1.7%) | 23 (3.9%) * | 18 (4.7%) * | 112 (13.3%) *bc | <0.01 |
| Smoking | 363 (12%) | 153 (12.7%) | 72 (12.2%) | 40 (10.4%) | 98 (11.6%) | NS |
| ACC/AHA 2017 HTN Guideline [2] | ||||||
|---|---|---|---|---|---|---|
| (Original Population, n = 3022) | ||||||
| BP Category (mmHg) | SBP | DBP | TAC Score | TAC Volume (mm3) | TAC Density (HU) | CAC Score |
| Normal (NBP) | <120 | and <80 | 35.3 ± 13.6 | 32.4 ± 11.1 | 35.2 ± 2.20 | 36.0 ± 5.4 |
| Elevated (EBP) | 120–129 | and <80 | 63.4 ± 25.5 * | 52.5 ± 20.9 * | 51.1 ± 4.12 * | 41.6 ± 7.4 |
| Stage 1 HTN | 130–139 | or 80–89 | 157.5 ± 25.2 *# | 130.2 ± 20.6 *# | 57.6 ± 4.08 *# | 40.5 ± 9.2 |
| Stage 2 HTN | ≥140 | or ≥90 | 194.6 ± 46.2 *#† | 160.3 ± 37.8 *#† | 68.9 ± 7.48 *#† | 50.9 ± 6.6 |
| ESC/ESH 2018 HTN Guideline [14] | ||||||
| (Original Population, n = 3022) | ||||||
| BP Category (mmHg) | SBP | DBP | TAC Score | TAC Volume (mm3) | TAC Density (HU) | CAC Score |
| Normal (NBP) | <130 | and <85 | 31.7 ± 16.8 | 29.4 ± 13.7 | 29.2 ± 2.71 | 39.7 ± 4.2 |
| High Normal (HNBP) | 130–139 | and/or 85–89 | 41.2 ± 23.0 * | 35.0 ± 18.9 * | 39.4 ± 3.71 * | 55.6 ± 8.2 |
| Grade 1 HTN | 140–159 | and/or 90–99 | 38.0 ± 28.5 * | 32.0 ± 23.3 * | 47.9 ± 4.60 *# | 40.7 ± 8.1 |
| Grade 2 HTN | ≥160 | and/or ≥100 | 152.2 ± 20.5 *#† | 127.6 ± 16.8 *#† | 64.5 ± 3.31 *#† | 62.7 ± 15.1 |
| Logistic Regression (Total n = 3022) | Uni-Variate | Multi-Variate | ||
|---|---|---|---|---|
| ACC/AHA 2017 HTN Guideline [2] | Odds Ratio | Odds Ratio | ||
| Thoracic aortic calcium | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age (>50 years) | 8.62 (6.64–11.20) | <0.001 | 7.01 (5.31–9.24) | <0.001 |
| Sex (male) | 0.86 (0.69–1.06) | 0.15 | — | NS |
| BMI (>25 kg/m2) | 1.22 (1.01–1.48) | 0.042 | — | NS |
| Body fat (M > 23%, F > 25%) [12] | 1.22 (0.99–1.50) | NS | — | NS |
| eGFR (<60 mL/min/1.732) | 4.18 (2.84–6.15) | <0.001 | 2.15 (1.39–3.33) | 0.001 |
| HTN (Stages 1 + 2) | 3.60 (2.95–4.41) | <0.001 | 2.49 1.98–3.12) | <0.001 |
| Diabetes | 3.93 (2.86–5.40) | <0.001 | 1.83 (1.28–2.63) | 0.001 |
| CVD | 3.33 (2.31–4.79) | <0.001 | — | NS |
| Dyslipidemia | 1.94 (1.35–2.79) | <0.001 | — | NS |
| Smoking | 1.20 (1.05–1.37) | 0.008 | — | NS |
| Coronary artery calcium | ||||
| Age (>50 y/o) | 4.22 (3.57–4.99) | <0.001 | 4.17 (3.46–5.03) | <0.001 |
| Sex (male) | 2.37 (1.95–2.87) | <0.001 | 2.58 (2.08–3.21) | <0.001 |
| BMI (>25 kg/m2) | 1.95 (1.67–2.28) | <0.001 | 1.61 (1.34–1.93) | <0.001 |
| Body fat (M > 23%, F > 25%) | 1.18 (1.00–1.40) | 0.048 | — | NS |
| eGFR (<60 mL/min/1.732) | 1.99 (1.36–2.92) | <0.001 | — | NS |
| HTN (Stages 1 + 2) | 2.98 (2.54–3.49) | <0.001 | 2.03 (1.69–2.44) | <0.001 |
| Diabetes | 3.33 (2.43–4.55) | <0.001 | 1.74 (1.22–2.48) | 0.002 |
| CVD | 2.54 (1.79–3.61) | <0.001 | — | NS |
| Dyslipidemia | 1.60 (1.16–2.22) | 0.004 | — | NS |
| Smoking | 1.12 (0.88–1.41) | 0.34 | — | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jan, Y.-T.; Tsai, P.-S.; Longenecker, C.T.; Lin, D.-C.; Yun, C.-H.; Sung, K.-T.; Liu, C.-C.; Kuo, J.-Y.; Hung, C.-L.; Wu, T.-H.; et al. Thoracic Aortic Calcification and Pre-Clinical Hypertension by New 2017 ACC/AHA Hypertension Guidelines. Diagnostics 2021, 11, 1027. https://doi.org/10.3390/diagnostics11061027
Jan Y-T, Tsai P-S, Longenecker CT, Lin D-C, Yun C-H, Sung K-T, Liu C-C, Kuo J-Y, Hung C-L, Wu T-H, et al. Thoracic Aortic Calcification and Pre-Clinical Hypertension by New 2017 ACC/AHA Hypertension Guidelines. Diagnostics. 2021; 11(6):1027. https://doi.org/10.3390/diagnostics11061027
Chicago/Turabian StyleJan, Ya-Ting, Pei-Shan Tsai, Chris T. Longenecker, Dao-Chen Lin, Chun-Ho Yun, Kuo-Tzu Sung, Chuan-Chuan Liu, Jen-Yuan Kuo, Chung-Lieh Hung, Tung-Hsin Wu, and et al. 2021. "Thoracic Aortic Calcification and Pre-Clinical Hypertension by New 2017 ACC/AHA Hypertension Guidelines" Diagnostics 11, no. 6: 1027. https://doi.org/10.3390/diagnostics11061027