
Neurofilaments as Emerging Biomarkers of Neuroaxonal Damage to Differentiate Behavioral Frontotemporal Dementia from Primary Psychiatric Disorders: A Systematic Review

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
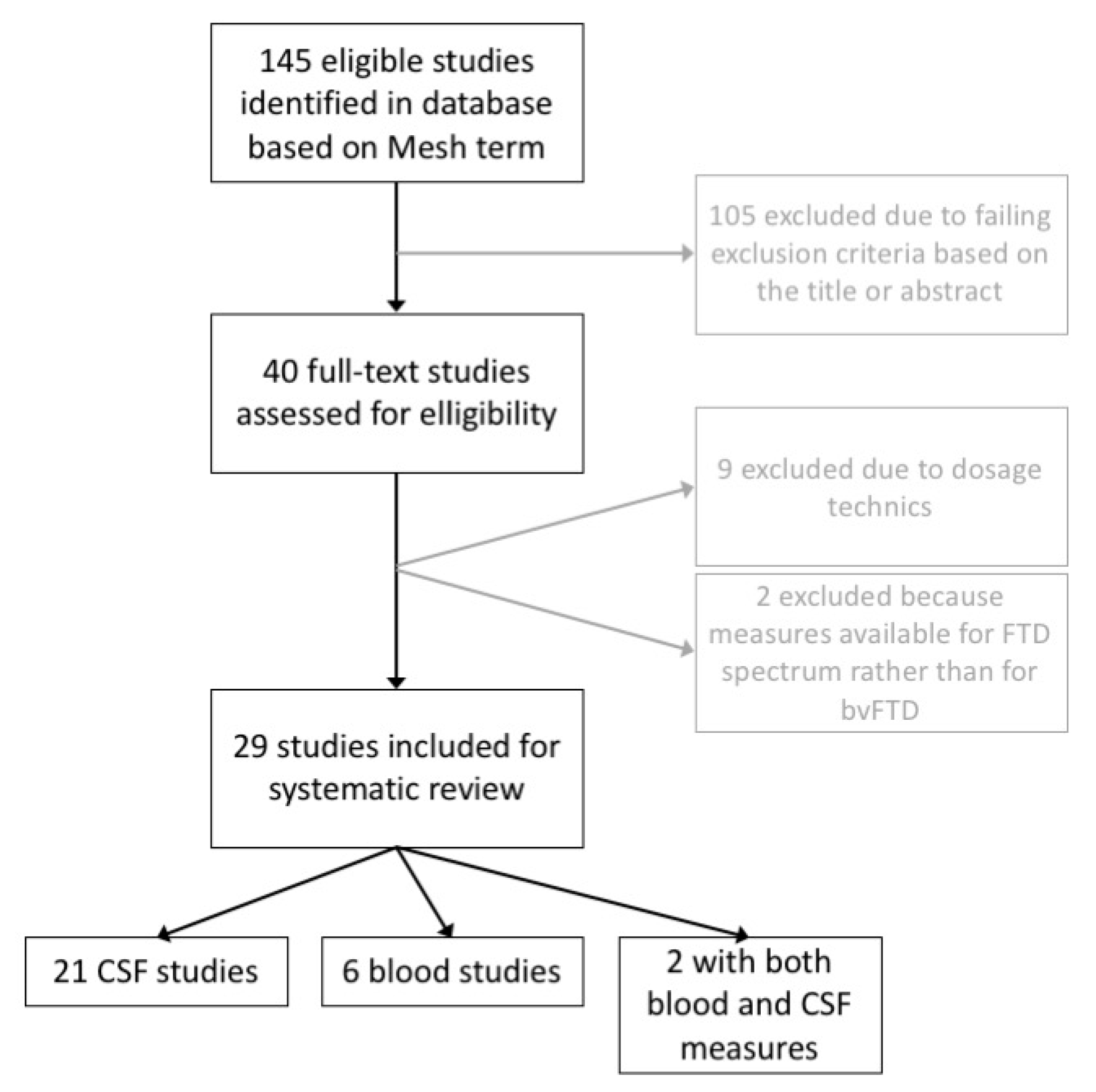
2. Methods
3. The Clinical Overlap between bvFTD and PPD
4. Biomarkers to Support the Diagnosis
5. Neurofilaments as Emerging Biomarkers in Neurological Disorders
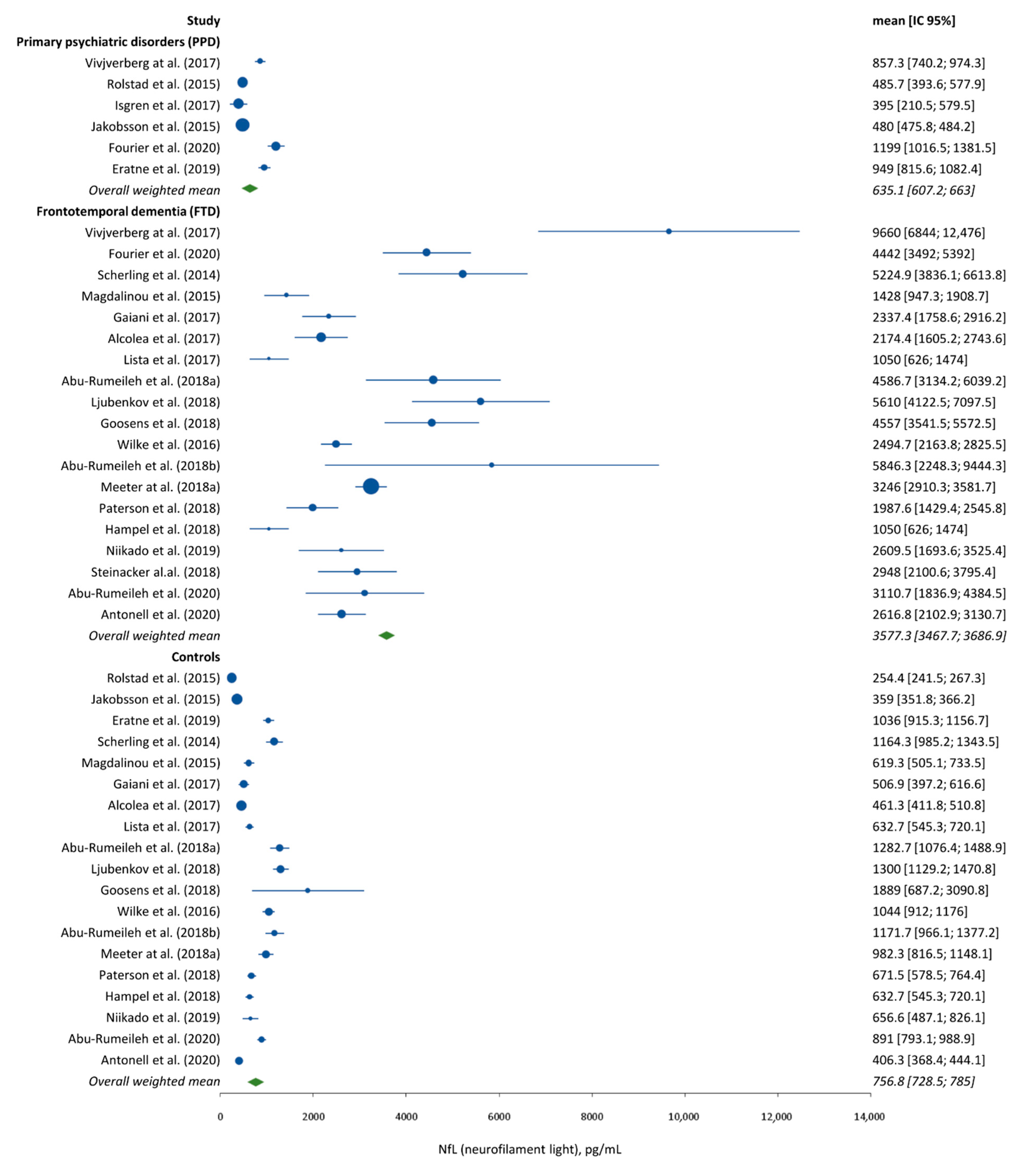
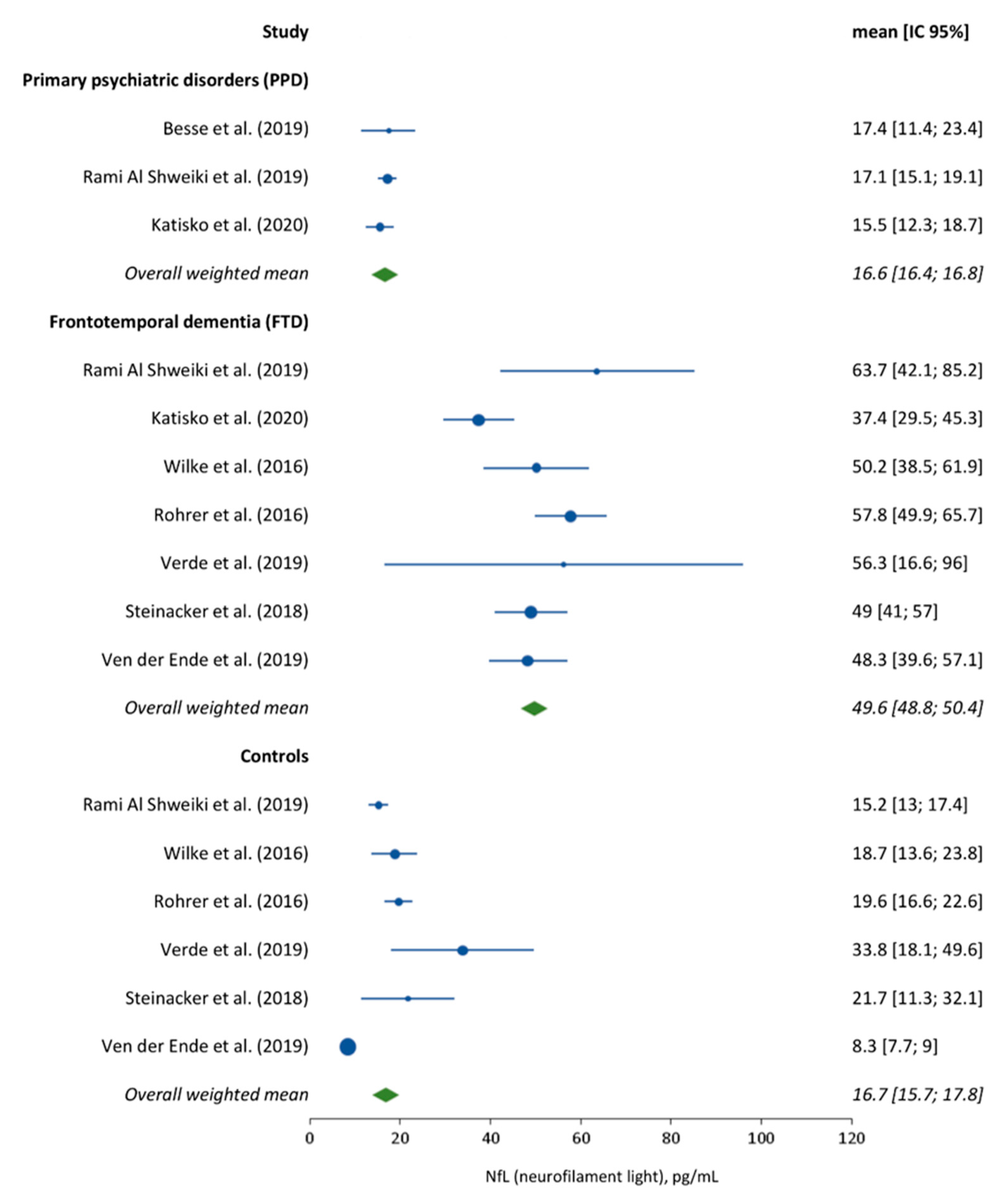
6. Neurofilaments Used to Differentiate PPD from bvFTD
7. Unsolved Questions
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mackenzie, I.R.A.; Neumann, M.; Bigio, E.H.; Cairns, N.J.; Alafuzoff, I.; Kril, J.; Kovacs, G.G.; Ghetti, B.; Halliday, G.; Holm, I.E.; et al. Nomenclature for Neuropathologic Subtypes of Frontotemporal Lobar Degeneration: Consensus Recommendations. Acta Neuropathol. 2009, 117, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of Revised Diagnostic Criteria for the Behavioural Variant of Frontotemporal Dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of Primary Progressive Aphasia and Its Variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Woolley, J.D.; Khan, B.K.; Murthy, N.K.; Miller, B.L.; Rankin, K.P. The Diagnostic Challenge of Psychiatric Symptoms in Neurodegenerative Disease: Rates of and Risk Factors for Prior Psychiatric Diagnosis in Patients With Early Neurodegenerative Disease. J. Clin. Psychiatry 2011, 72, 126–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducharme, S.; Dols, A.; Laforce, R.; Devenney, E.; Kumfor, F.; van den Stock, J.; Dallaire-Théroux, C.; Seelaar, H.; Gossink, F.; Vijverberg, E.; et al. Recommendations to Distinguish Behavioural Variant Frontotemporal Dementia from Psychiatric Disorders. Brain 2020, 142, 18. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as Biomarkers in Neurological Disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Andreasson, U.; Blennow, K.; Zetterberg, H. Update on Ultrasensitive Technologies to Facilitate Research on Blood Biomarkers for Central Nervous System Disorders. Alzheimer Dement. Diagn. Assess. Dis. Monit. 2016, 3, 98–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Ying, M.; Xie, L.; Chandrasekar, E.K.; Lu, H.; Wang, T.; Li, C. Late-Life Depression and Cognitive Function among Older Adults in the U.S.: The National Health and Nutrition Examination Survey, 2011–2014. J. Psychiatr. Res. 2019, 111, 30–35. [Google Scholar] [CrossRef]
- Blazer, D. Depression in Late Life: Review and Commentary. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, 249–265. [Google Scholar] [CrossRef] [Green Version]
- Lewandowski, K.E.; Cohen, B.M.; Öngur, D. Evolution of Neuropsychological Dysfunction during the Course of Schizophrenia and Bipolar Disorder. Psychol. Med. 2011, 41, 225–241. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.S.; Rollinson, S.; Thompson, J.C.; Harris, J.M.; Stopford, C.L.; Richardson, A.M.T.; Jones, M.; Gerhard, A.; Davidson, Y.S.; Robinson, A.; et al. Distinct Clinical and Pathological Characteristics of Frontotemporal Dementia Associated with C9ORF72 Mutations. Brain 2012, 135, 693–708. [Google Scholar] [CrossRef] [PubMed]
- Galimberti, D.; Fenoglio, C.; Serpente, M.; Villa, C.; Bonsi, R.; Arighi, A.; Fumagalli, G.G.; Del Bo, R.; Bruni, A.C.; Anfossi, M.; et al. Autosomal Dominant Frontotemporal Lobar Degeneration Due to the C9ORF72 Hexanucleotide Repeat Expansion: Late-Onset Psychotic Clinical Presentation. Biol. Psychiatry 2013, 74, 384–391. [Google Scholar] [CrossRef]
- Mendez, M.F.; Perryman, K.M.; Miller, B.L.; Swartz, J.R.; Cummings, J.L. Compulsive Behaviors as Presenting Symptoms of Frontotemporal Dementia. J. Geriatr. Psychiatry Neurol. 1997, 10, 154–157. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9780890425558. [Google Scholar]
- Hallam, B.J.; Silverberg, N.D.; LaMarre, A.K.; Mackenzie, I.R.A.; Feldman, H.H. Clinical Presentation of Prodromal Frontotemporal Dementia. Am. J. Alzheimers Dis. Demen. 2008, 22, 456–467. [Google Scholar] [CrossRef]
- Gordovez, F.J.A.; McMahon, F.J. The Genetics of Bipolar Disorder. Mol. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Chou, I.-J.; Kuo, C.-F.; Huang, Y.-S.; Grainge, M.J.; Valdes, A.M.; See, L.-C.; Yu, K.-H.; Luo, S.-F.; Huang, L.-S.; Tseng, W.-Y.; et al. Familial Aggregation and Heritability of Schizophrenia and Co-Aggregation of Psychiatric Illnesses in Affected Families. Schizophr. Bull. 2017, 43, 1070–1078. [Google Scholar] [CrossRef] [Green Version]
- Devenney, E.; Hornberger, M.; Irish, M.; Mioshi, E.; Burrell, J.; Tan, R.; Kiernan, M.C.; Hodges, J.R. Frontotemporal Dementia Associated with the C9ORF72 Mutation: A Unique Clinical Profile. JAMA Neurol. 2014, 71, 331. [Google Scholar] [CrossRef] [Green Version]
- Kipps, C.M.; Hodges, J.R.; Hornberger, M. Nonprogressive Behavioural Frontotemporal Dementia: Recent Developments and Clinical Implications of the ‘BvFTD Phenocopy Syndrome. Curr. Opin. Neurol. 2010, 23, 628–632. [Google Scholar] [CrossRef]
- Khan, B.K.; Yokoyama, J.S.; Takada, L.T.; Sha, S.J.; Rutherford, N.J.; Fong, J.C.; Karydas, A.M.; Wu, T.; Ketelle, R.S.; Baker, M.C.; et al. Atypical, Slowly Progressive Behavioural Variant Frontotemporal Dementia Associated with C9ORF72 Hexanucleotide Expansion. J. Neurol. Neurosurg. Psychiatry 2012, 83, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Mendez, M.F.; Shapira, J.S.; McMurtray, A.; Licht, E.; Miller, B.L. Accuracy of the Clinical Evaluation for Frontotemporal Dementia. Arch. Neurol. 2007, 64, 830. [Google Scholar] [CrossRef] [Green Version]
- Simrén, J.; Ashton, N.J.; Blennow, K.; Zetterberg, H. An Update on Fluid Biomarkers for Neurodegenerative Diseases: Recent Success and Challenges Ahead. Curr. Opin. Neurobiol. 2020, 61, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Knopman, D.S.; Boeve, B.F.; Parisi, J.E.; Dickson, D.W.; Smith, G.E.; Ivnik, R.J.; Josephs, K.A.; Petersen, R.C. Antemortem Diagnosis of Frontotemporal Lobar Degeneration. Ann. Neurol. 2005, 57, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Kerklaan, B.J.; van Berckel, B.N.M.; Herholz, K.; Dols, A.; van der Flier, W.M.; Scheltens, P.; Pijnenburg, Y.A.L. The Added Value of 18-Fluorodeoxyglucose-Positron Emission Tomography in the Diagnosis of the Behavioral Variant of Frontotemporal Dementia. Am. J. Alzheimers Dis. Demen. 2014, 29, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Krudop, W.A.; Dols, A.; Kerssens, C.J.; Prins, N.D.; Möller, C.; Schouws, S.; Barkhof, F.; van Berckel, B.N.M.; Teunissen, C.E.; van der Flier, W.M.; et al. Impact of Imaging and Cerebrospinal Fluid Biomarkers on Behavioral Variant Frontotemporal Dementia Diagnosis within a Late-Onset Frontal Lobe Syndrome Cohort. Dement. Geriatr. Cogn. Disord. 2016, 41, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Petzold, A. Neurofilament Phosphoforms: Surrogate Markers for Axonal Injury, Degeneration and Loss. J. Neurol. Sci. 2005, 233, 183–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhle, J.; Barro, C.; Andreasson, U.; Derfuss, T.; Lindberg, R.; Sandelius, Å.; Liman, V.; Norgren, N.; Blennow, K.; Zetterberg, H. Comparison of Three Analytical Platforms for Quantification of the Neurofilament Light Chain in Blood Samples: ELISA, Electrochemiluminescence Immunoassay and Simoa. Clin. Chem. Lab. Med. (CCLM) 2016, 54, 1655–1661. [Google Scholar] [CrossRef]
- Malmeström, C.; Haghighi, S.; Rosengren, L.; Andersen, O.; Lycke, J. Neurofilament Light Protein and Glial Fibrillary Acidic Protein as Biological Markers in MS. Neurology 2003, 61, 1720–1725. [Google Scholar] [CrossRef]
- Gunnarsson, M.; Malmeström, C.; Axelsson, M.; Sundström, P.; Dahle, C.; Vrethem, M.; Olsson, T.; Piehl, F.; Norgren, N.; Rosengren, L.; et al. Axonal Damage in Relapsing Multiple Sclerosis Is Markedly Reduced by Natalizumab. Ann. Neurol. 2011, 69, 83–89. [Google Scholar] [CrossRef]
- Magdalinou, N.K.; Paterson, R.W.; Schott, J.M.; Fox, N.C.; Mummery, C.; Blennow, K.; Bhatia, K.; Morris, H.R.; Giunti, P.; Warner, T.T.; et al. A Panel of Nine Cerebrospinal Fluid Biomarkers May Identify Patients with Atypical Parkinsonian Syndromes. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1240–1247. [Google Scholar] [CrossRef]
- Hall, S.; Öhrfelt, A.; Constantinescu, R.; Andreasson, U.; Surova, Y.; Bostrom, F.; Nilsson, C.; Widner, H.; Decraemer, H.; Nägga, K.; et al. Accuracy of a Panel of 5 Cerebrospinal Fluid Biomarkers in the Differential Diagnosis of Patients With Dementia and/or Parkinsonian Disorders. Arch. Neurol. 2012, 69, 1445. [Google Scholar] [CrossRef]
- Weydt, P.; Oeckl, P.; Huss, A.; Müller, K.; Volk, A.E.; Kuhle, J.; Knehr, A.; Andersen, P.M.; Prudlo, J.; Steinacker, P.; et al. Neurofilament Levels as Biomarkers in Asymptomatic and Symptomatic Familial Amyotrophic Lateral Sclerosis: Biomarkers in ALS. Ann. Neurol. 2016, 79, 152–158. [Google Scholar] [CrossRef]
- Poesen, K.; De Schaepdryver, M.; Stubendorff, B.; Gille, B.; Muckova, P.; Wendler, S.; Prell, T.; Ringer, T.M.; Rhode, H.; Stevens, O.; et al. Neurofilament Markers for ALS Correlate with Extent of Upper and Lower Motor Neuron Disease. Neurology 2017, 88, 2302–2309. [Google Scholar] [CrossRef]
- Lu, C.-H.; Petzold, A.; Topping, J.; Allen, K.; Macdonald-Wallis, C.; Clarke, J.; Pearce, N.; Kuhle, J.; Giovannoni, G.; Fratta, P.; et al. Plasma Neurofilament Heavy Chain Levels and Disease Progression in Amyotrophic Lateral Sclerosis: Insights from a Longitudinal Study. J. Neurol. Neurosurg. Psychiatry 2015, 86, 565–573. [Google Scholar] [CrossRef]
- Mattsson, N.; Insel, P.S.; Palmqvist, S.; Portelius, E.; Zetterberg, H.; Weiner, M.; Blennow, K.; Hansson, O.; the Alzheimer’s Disease Neuroimaging Initiative. Cerebrospinal Fluid Tau, Neurogranin, and Neurofilament Light in Alzheimer’s Disease. EMBO Mol. Med. 2016, 8, 1184–1196. [Google Scholar] [CrossRef] [PubMed]
- Meeter, L.H.; Dopper, E.G.; Jiskoot, L.C.; Sanchez-Valle, R.; Graff, C.; Benussi, L.; Ghidoni, R.; Pijnenburg, Y.A.; Borroni, B.; Galimberti, D.; et al. Neurofilament Light Chain: A Biomarker for Genetic Frontotemporal Dementia. Ann. Clin. Transl. Neurol. 2016, 3, 623–636. [Google Scholar] [CrossRef]
- Pijnenburg, Y.A.L.; Verwey, N.A.; van der Flier, W.M.; Scheltens, P.; Teunissen, C.E. Discriminative and Prognostic Potential of Cerebrospinal Fluid PhosphoTau/Tau Ratio and Neurofilaments for Frontotemporal Dementia Subtypes. Alzheimer Dement. Diagn. Assess. Dis. Monit. 2015, 1, 505–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rohrer, J.D.; Woollacott, I.O.C.; Dick, K.M.; Brotherhood, E.; Gordon, E.; Fellows, A.; Toombs, J.; Druyeh, R.; Cardoso, M.J.; Ourselin, S.; et al. Serum Neurofilament Light Chain Protein Is a Measure of Disease Intensity in Frontotemporal Dementia. Neurology 2016, 87, 1329–1336. [Google Scholar] [CrossRef] [Green Version]
- Jakobsson, J.; Bjerke, M.; Ekman, C.J.; Sellgren, C.; Johansson, A.G.; Zetterberg, H.; Blennow, K.; Landén, M. Elevated Concentrations of Neurofilament Light Chain in the Cerebrospinal Fluid of Bipolar Disorder Patients. Neuropsychopharmacology 2014, 39, 2349–2356. [Google Scholar] [CrossRef] [PubMed]
- Eratne, D.; Loi, S.M.; Walia, N.; Farrand, S.; Li, Q.-X.; Varghese, S.; Walterfang, M.; Evans, A.; Mocellin, R.; Dhiman, K.; et al. A Pilot Study of the Utility of Cerebrospinal Fluid Neurofilament Light Chain in Differentiating Neurodegenerative from Psychiatric Disorders: A ‘C-Reactive Protein’ for Psychiatrists and Neurologists? Aust. NZJ. Psychiatry 2020, 54, 57–67. [Google Scholar] [CrossRef]
- Besse, M.; Belz, M.; Folsche, T.; Vogelgsang, J.; Methfessel, I.; Steinacker, P.; Otto, M.; Wiltfang, J.; Zilles, D. Serum Neurofilament Light Chain (NFL) Remains Unchanged during Electroconvulsive Therapy. World J. Biol. Psychiatry 2020, 21, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Vijverberg, E.G.B.; Dols, A.; Krudop, W.A.; Del Campo Milan, M.; Kerssens, C.J.; Gossink, F.; Prins, N.D.; Stek, M.L.; Scheltens, P.; Teunissen, C.E.; et al. Cerebrospinal Fluid Biomarker Examination as a Tool to Discriminate Behavioral Variant Frontotemporal Dementia from Primary Psychiatric Disorders. Alzheimer Dement. Diagn. Assess. Dis. Monit. 2017, 7, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Fourier, A.; Formaglio, M.; Kaczorowski, F.; Mollion, H.; Perret-Liaudet, A.; Sauvee, M.; Quadrio, I. A Combination of Total Tau and Neurofilaments Discriminates between Neurodegenerative and Primary Psychiatric Disorders. Eur. J. Neurol. 2020, 27, 14247. [Google Scholar] [CrossRef] [PubMed]
- Al Shweiki, M.R.; Steinacker, P.; Oeckl, P.; Hengerer, B.; Danek, A.; Fassbender, K.; Diehl-Schmid, J.; Jahn, H.; Anderl-Straub, S.; Ludolph, A.C.; et al. Neurofilament Light Chain as a Blood Biomarker to Differentiate Psychiatric Disorders from Behavioural Variant Frontotemporal Dementia. J. Psychiatr. Res. 2019, 113, 137–140. [Google Scholar] [CrossRef]
- Katisko, K.; Cajanus, A.; Jääskeläinen, O.; Kontkanen, A.; Hartikainen, P.; Korhonen, V.E.; Helisalmi, S.; Haapasalo, A.; Koivumaa-Honkanen, H.; Herukka, S.-K.; et al. Serum Neurofilament Light Chain Is a Discriminative Biomarker between Frontotemporal Lobar Degeneration and Primary Psychiatric Disorders. J. Neurol. 2020, 267, 162–167. [Google Scholar] [CrossRef] [Green Version]
- Steinacker, P.; Anderl-Straub, S.; Diehl-Schmid, J.; Semler, E.; Uttner, I.; von Arnim, C.A.F.; Barthel, H.; Danek, A.; Fassbender, K.; Fliessbach, K.; et al. Serum Neurofilament Light Chain in Behavioral Variant Frontotemporal Dementia. Neurology 2018, 91, 1390–1401. [Google Scholar] [CrossRef]
- Passant, U.; Elfgren, C.; Englund, E.; Gustafson, L. Psychiatric Symptoms and Their Psychosocial Consequences in Frontotemporal Dementia. Alzheimer Dis. Assoc. Disord. 2005, 19, 15–18. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davy, V.; Dumurgier, J.; Fayosse, A.; Paquet, C.; Cognat, E. Neurofilaments as Emerging Biomarkers of Neuroaxonal Damage to Differentiate Behavioral Frontotemporal Dementia from Primary Psychiatric Disorders: A Systematic Review. Diagnostics 2021, 11, 754. https://doi.org/10.3390/diagnostics11050754
Davy V, Dumurgier J, Fayosse A, Paquet C, Cognat E. Neurofilaments as Emerging Biomarkers of Neuroaxonal Damage to Differentiate Behavioral Frontotemporal Dementia from Primary Psychiatric Disorders: A Systematic Review. Diagnostics. 2021; 11(5):754. https://doi.org/10.3390/diagnostics11050754
Chicago/Turabian StyleDavy, Vincent, Julien Dumurgier, Aurore Fayosse, Claire Paquet, and Emmanuel Cognat. 2021. "Neurofilaments as Emerging Biomarkers of Neuroaxonal Damage to Differentiate Behavioral Frontotemporal Dementia from Primary Psychiatric Disorders: A Systematic Review" Diagnostics 11, no. 5: 754. https://doi.org/10.3390/diagnostics11050754