
Musculoskeletal Soft-Tissue Sarcoma: Quality Assessment of Initial MRI Reports Shows Frequent Deviation from ESSR Guidelines

 , , ,
, , ,
Abstract
:1. Introduction
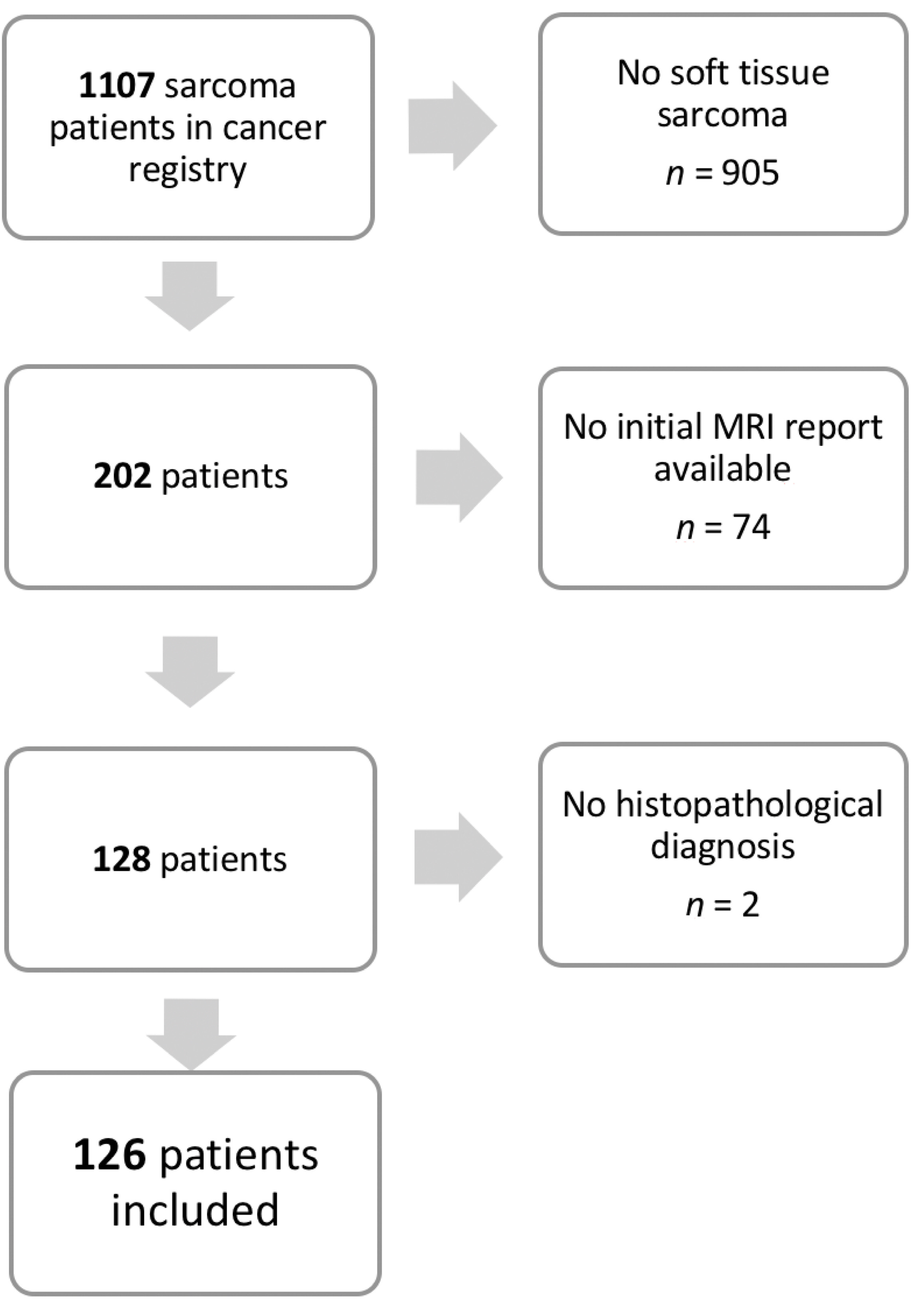
2. Materials and Methods
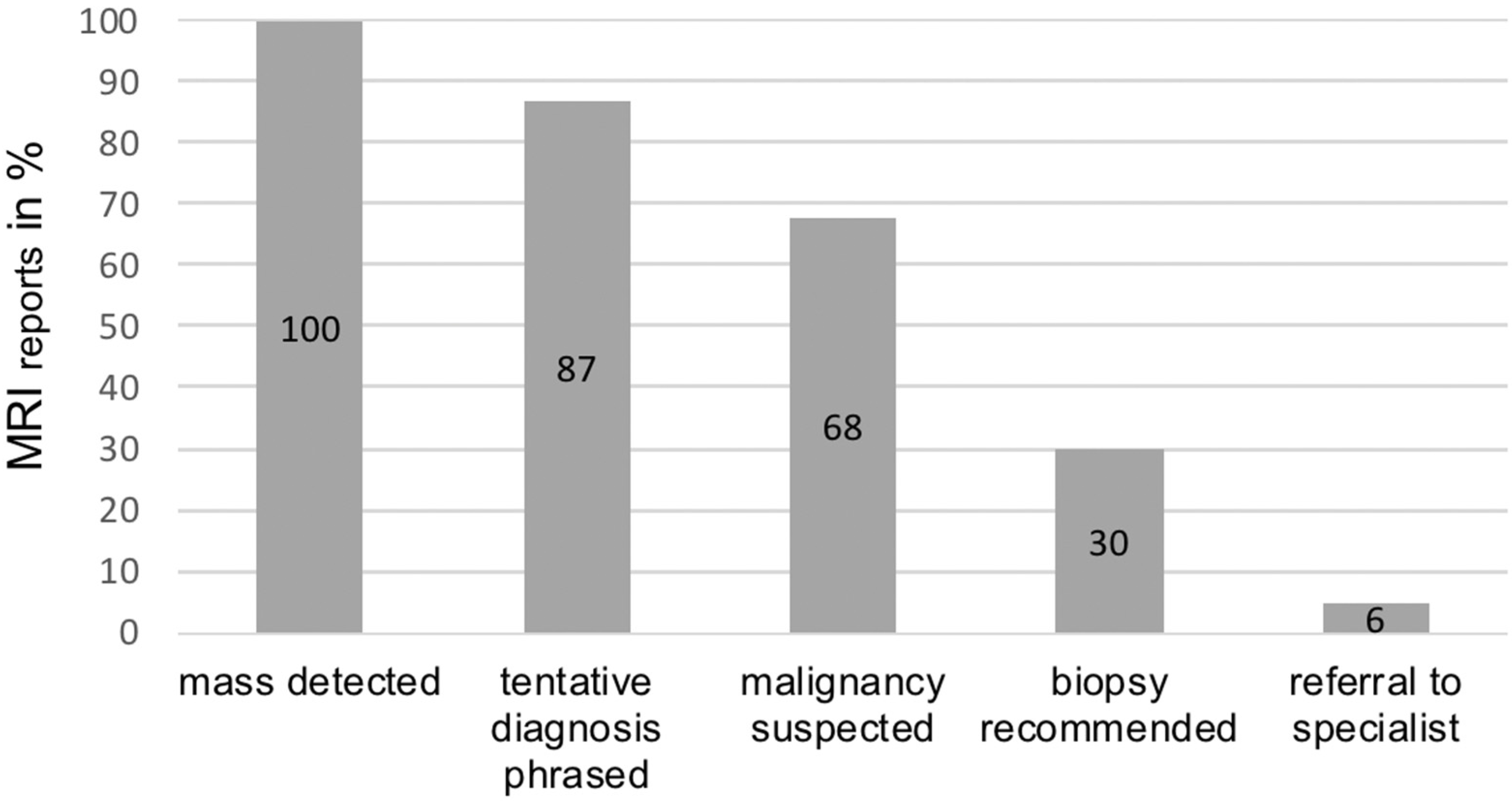
- Was the soft-tissue mass detected and described as anomalous?
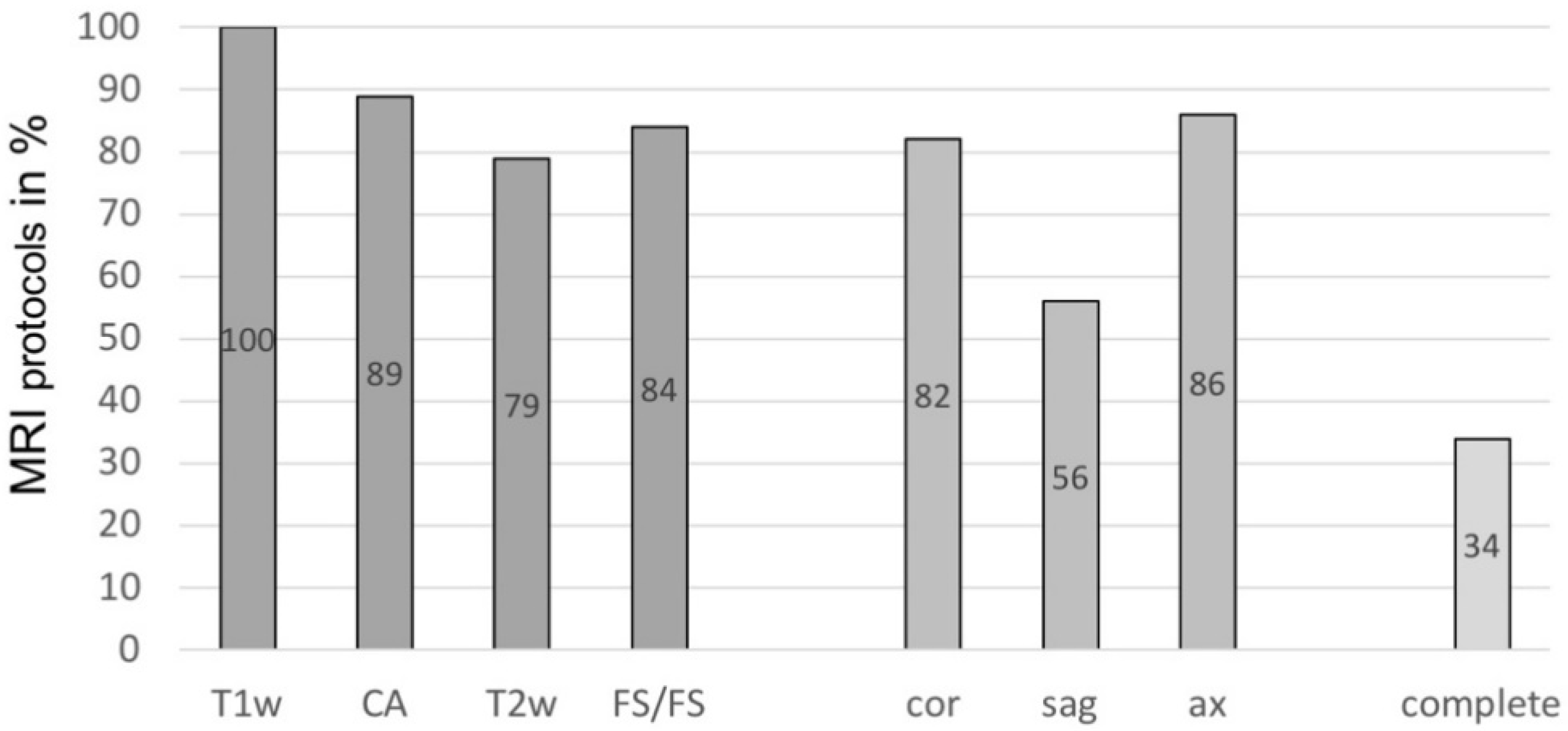
- Which sequences (T1-weighted, T2-weighted, fluid-sensitive/fat-saturated) were performed, which planes (coronal, sagittal, axial) were included, and was a contrast agent used?
- Was a conclusion drawn regarding the specific suspected diagnosis?
- Did the report mention a suspected malignancy or signs thereof? In cases of suspected “sarcoma” (see question 3), this question was answered with “yes”.
- Did the report include a recommendation for biopsy and histopathological analysis of the described tissue?
- Was a referral to a specialized sarcoma center recommended?
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Manaster, B.J. Soft-tissue masses: Optimal imaging protocol and reporting. AJR Am. J. Roentgenol. 2013, 201, 505–514. [Google Scholar] [CrossRef]
- Gatta, G.; van der Zwan, J.M.; Casali, P.G.; Siesling, S.; Dei Tos, A.P.; Kunkler, I.; Otter, R.; Licitra, L.; Mallone, S.; Tavilla, A.; et al. Rare cancers are not so rare: The rare cancer burden in Europe. Eur. J. Cancer 2011, 47, 2493–2511. [Google Scholar] [CrossRef]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.; Brodowicz, T.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv268–iv269. [Google Scholar] [CrossRef] [Green Version]
- Ducimetiere, F.; Lurkin, A.; Ranchere-Vince, D.; Decouvelaere, A.V.; Peoc’h, M.; Istier, L.; Chalabreysse, P.; Muller, C.; Alberti, L.; Bringuier, P.P.; et al. Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing. PLoS ONE 2011, 6, e20294. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Eilber, F.R. The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J. Clin. Oncol. 1985, 3, 1344–1348. [Google Scholar] [CrossRef]
- Gielen, J.L.; De Schepper, A.M.; Vanhoenacker, F.; Parizel, P.M.; Wang, X.L.; Sciot, R.; Weyler, J. Accuracy of MRI in characterization of soft tissue tumors and tumor-like lesions. A prospective study in 548 patients. Eur. Radiol. 2004, 14, 2320–2330. [Google Scholar] [CrossRef]
- Pretell-Mazzini, J.; Barton, M.D., Jr.; Conway, S.A.; Temple, H.T. Unplanned excision of soft-tissue sarcomas: Current concepts for management and prognosis. J. Bone Jt. Surg. Am. 2015, 97, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.C.; Perez, E.A.; Moffat, F.L.; Livingstone, A.S.; Franceschi, D.; Koniaris, L.G. Should soft tissue sarcomas be treated at high-volume centers? An analysis of 4205 patients. Ann. Surg. 2007, 245, 952–958. [Google Scholar] [CrossRef]
- Paszat, L.; O’Sullivan, B.; Bell, R.; Bramwell, V.; Groome, P.; Mackillop, W.; Bartfay, E.; Holowaty, E. Processes and outcomes of care for soft tissue sarcoma of the extremities. Sarcoma 2002, 6, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clasby, R.; Tilling, K.; Smith, M.A.; Fletcher, C.D. Variable management of soft tissue sarcoma: Regional audit with implications for specialist care. Br. J. Surg. 1997, 84, 1692–1696. [Google Scholar] [CrossRef] [PubMed]
- Jakob, J.; Henzler, T.; Kasper, B.; Marx, A.; Hohenberger, P. Interdisciplinary treatment of soft tissue sarcoma of the extremities. Chirurg 2014, 85, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.Y.; Honore, C.; Stoeckle, E.; Meeus, P.; Jafari, M.; Gouin, F.; Anract, P.; Ferron, G.; Rochwerger, A.; Ropars, M.; et al. Surgery in reference centers improves survival of sarcoma patients: A nationwide study. Ann. Oncol. 2019, 30, 1407. [Google Scholar] [CrossRef]
- Gilbert, N.F.; Cannon, C.P.; Lin, P.P.; Lewis, V.O. Soft-tissue sarcoma. J. Am. Acad. Orthop. Surg. 2009, 17, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.H.; Ro, J.Y. Retroperitoneal Sarcomas: An Update on the Diagnostic Pathology Approach. Diagnostics 2020, 10, 642. [Google Scholar] [CrossRef]
- Potter, B.K.; Adams, S.C.; Pitcher, J.D., Jr.; Temple, H.T. Local recurrence of disease after unplanned excisions of high-grade soft tissue sarcomas. Clin. Orthop. Relat. Res. 2008, 466, 3093–3100. [Google Scholar] [CrossRef] [Green Version]
- Noebauer-Huhmann, I.M.; Weber, M.A.; Lalam, R.K.; Trattnig, S.; Bohndorf, K.; Vanhoenacker, F.; Tagliafico, A.; van Rijswijk, C.; Vilanova, J.C.; Afonso, P.D.; et al. Soft Tissue Tumors in Adults: ESSR-Approved Guidelines for Diagnostic Imaging. Semin. Musculoskelet. Radiol. 2015, 19, e1. [Google Scholar] [CrossRef]
- Mayerson, J.L.; Scharschmidt, T.J.; Lewis, V.O.; Morris, C.D. Diagnosis and Management of Soft-tissue Masses. Instr. Course Lect. 2015, 64, 95–103. [Google Scholar] [CrossRef]
- George, A.; Grimer, R. Early symptoms of bone and soft tissue sarcomas: Could they be diagnosed earlier? Ann. R Coll. Surg. Engl. 2012, 94, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Damron, T.A.; Beauchamp, C.P.; Rougraff, B.T.; Ward, W.G. Soft-tissue lumps and bumps. Instr. Course Lect. 2004, 53, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat, S.; Ravesh, M.S.; Sedaghat, M.; Both, M.; Jansen, O. Configuration of soft-tissue sarcoma on MRI correlates with grade of malignancy. Radiol. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Hao, D.; Li, J.; Liu, J.; Hou, F.; Chen, H.; Duan, L.; Huang, C.; Wang, H.; Yu, T. Magnetic Resonance Imaging-Based Radiomics Nomogram for Prediction of the Histopathological Grade of Soft Tissue Sarcomas: A Two-Center Study. J. Magn. Reson. Imaging 2021. [Google Scholar] [CrossRef]
- Wu, J.S.; Hochman, M.G. Soft-tissue tumors and tumorlike lesions: A systematic imaging approach. Radiology 2009, 253, 297–316. [Google Scholar] [CrossRef] [Green Version]
- Ulaner, G.; Hwang, S.; Landa, J.; Lefkowitz, R.A.; Panicek, D.M. Musculoskeletal tumours and tumour-like conditions: Common and avoidable pitfalls at imaging in patients with known or suspected cancer: Part B: Malignant mimics of benign tumours. Int. Orthop. 2013, 37, 877–882. [Google Scholar] [CrossRef] [Green Version]
- Gingrich, A.A.; Elias, A.; Michael Lee, C.Y.; Nakache, Y.N.; Li, C.S.; Shah, D.R.; Boutin, R.D.; Canter, R.J. Predictors of residual disease after unplanned excision of soft tissue sarcomas. J. Surg. Res. 2017, 208, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Brisson, M.; Kashima, T.; Delaney, D.; Tirabosco, R.; Clarke, A.; Cro, S.; Flanagan, A.M.; O’Donnell, P. MRI characteristics of lipoma and atypical lipomatous tumor/well-differentiated liposarcoma: Retrospective comparison with histology and MDM2 gene amplification. Skeletal. Radiol. 2013, 42, 635–647. [Google Scholar] [CrossRef]
- Sato, D.; Suga, H.; Takushima, A. Liposarcoma Preoperatively Diagnosed as Lipoma: 10-Year Experience at a Single Institution. Dermatol. Surg. 2018, 44, 1065–1069. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, R.E.; Golfam, M.; Sheikh, A.; Cron, G.O.; White, E.A.; Werier, J.; Schweitzer, M.E.; Di Primio, G. Differentiation of lipoma from liposarcoma on MRI using texture and shape analysis. Acad. Radiol. 2014, 21, 1185–1194. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.Y.; Jost, E.; Mack, L.; Bouchard-Fortier, A. Surgical management of truncal and extremities atypical lipomatous tumors/well-differentiated liposarcoma: A systematic review of the literature. Am. J. Surg. 2020, 219, 823–827. [Google Scholar] [CrossRef] [PubMed]
- De La Hoz Polo, M.; Dick, E.; Bhumbra, R.; Pollock, R.; Sandhu, R.; Saifuddin, A. Surgical considerations when reporting MRI studies of soft tissue sarcoma of the limbs. Skeletal. Radiol. 2017, 46, 1667–1678. [Google Scholar] [CrossRef]
- Dangoor, A.; Seddon, B.; Gerrand, C.; Grimer, R.; Whelan, J.; Judson, I. UK guidelines for the management of soft tissue sarcomas. Clin. Sarcoma Res. 2016, 6, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traina, F.; Errani, C.; Toscano, A.; Pungetti, C.; Fabbri, D.; Mazzotti, A.; Donati, D.; Faldini, C. Current concepts in the biopsy of musculoskeletal tumors. J. Bone Jt. Surg. Am. 2015, 97, e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honore, C.; Meeus, P.; Stoeckle, E.; Bonvalot, S. Soft tissue sarcoma in France in 2015: Epidemiology, classification and organization of clinical care. J. Visc. Surg. 2015, 152, 223–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subtype of Soft-Tissue Sarcoma | Number of Cases |
|---|---|
| Atypical lipomatous tumor/liposarcoma grade I | 24 |
| Myxofibrosarcoma | 16 |
| Myxoid liposarcoma | 15 |
| Dedifferentiated liposarcoma | 9 |
| Synovial sarcoma | 8 |
| Fibromyxoid sarcoma | 6 |
| Pleomorphic undifferentiated sarcoma | 7 |
| Leiomyosarcoma | 5 |
| Malignant peripheral nerve sheath tumor(MPNST) | 5 |
| Pleomorphic spindle cell sarcoma (PSCS) | 4 |
| Undifferentiated pleophormic sarcoma | 4 |
| Epithelioid sarcoma | 4 |
| Undifferentiated sarcoma NOS | 3 |
| Angiosarcoma | 2 |
| Desmoplastic small-round-cell tumor | 2 |
| Spindle cell sarcoma NOS | 2 |
| Alveolar rhabdomyosarcoma | 1 |
| Extraskelettal osteosarcoma | 1 |
| Glomus tumor | 1 |
| High-grade myxoid liposarcoma | 1 |
| Clear-cell sarcoma | 1 |
| Myofibroblastic sarcoma | 1 |
| Pleomorphic liposarcoma | 1 |
| Pleomorphic rhabdomyosarcoma | 1 |
| Peripheral primitive neuroectodermal tumor (pPNET) | 1 |
| Sclerosing epithelioid fibrosarcom | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiss, S.; Korthaus, A.; Baumann, N.; Yamamura, J.; Spiro, A.S.; Lübke, A.M.; Frosch, K.-H.; Schlickewei, C.; Priemel, M. Musculoskeletal Soft-Tissue Sarcoma: Quality Assessment of Initial MRI Reports Shows Frequent Deviation from ESSR Guidelines. Diagnostics 2021, 11, 695. https://doi.org/10.3390/diagnostics11040695
Weiss S, Korthaus A, Baumann N, Yamamura J, Spiro AS, Lübke AM, Frosch K-H, Schlickewei C, Priemel M. Musculoskeletal Soft-Tissue Sarcoma: Quality Assessment of Initial MRI Reports Shows Frequent Deviation from ESSR Guidelines. Diagnostics. 2021; 11(4):695. https://doi.org/10.3390/diagnostics11040695
Chicago/Turabian StyleWeiss, Sebastian, Alexander Korthaus, Nora Baumann, Jin Yamamura, Alexander S. Spiro, Andreas M. Lübke, Karl-Heinz Frosch, Carsten Schlickewei, and Matthias Priemel. 2021. "Musculoskeletal Soft-Tissue Sarcoma: Quality Assessment of Initial MRI Reports Shows Frequent Deviation from ESSR Guidelines" Diagnostics 11, no. 4: 695. https://doi.org/10.3390/diagnostics11040695