
Deep Learning for Diagnosis of Paranasal Sinusitis Using Multi-View Radiographs

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
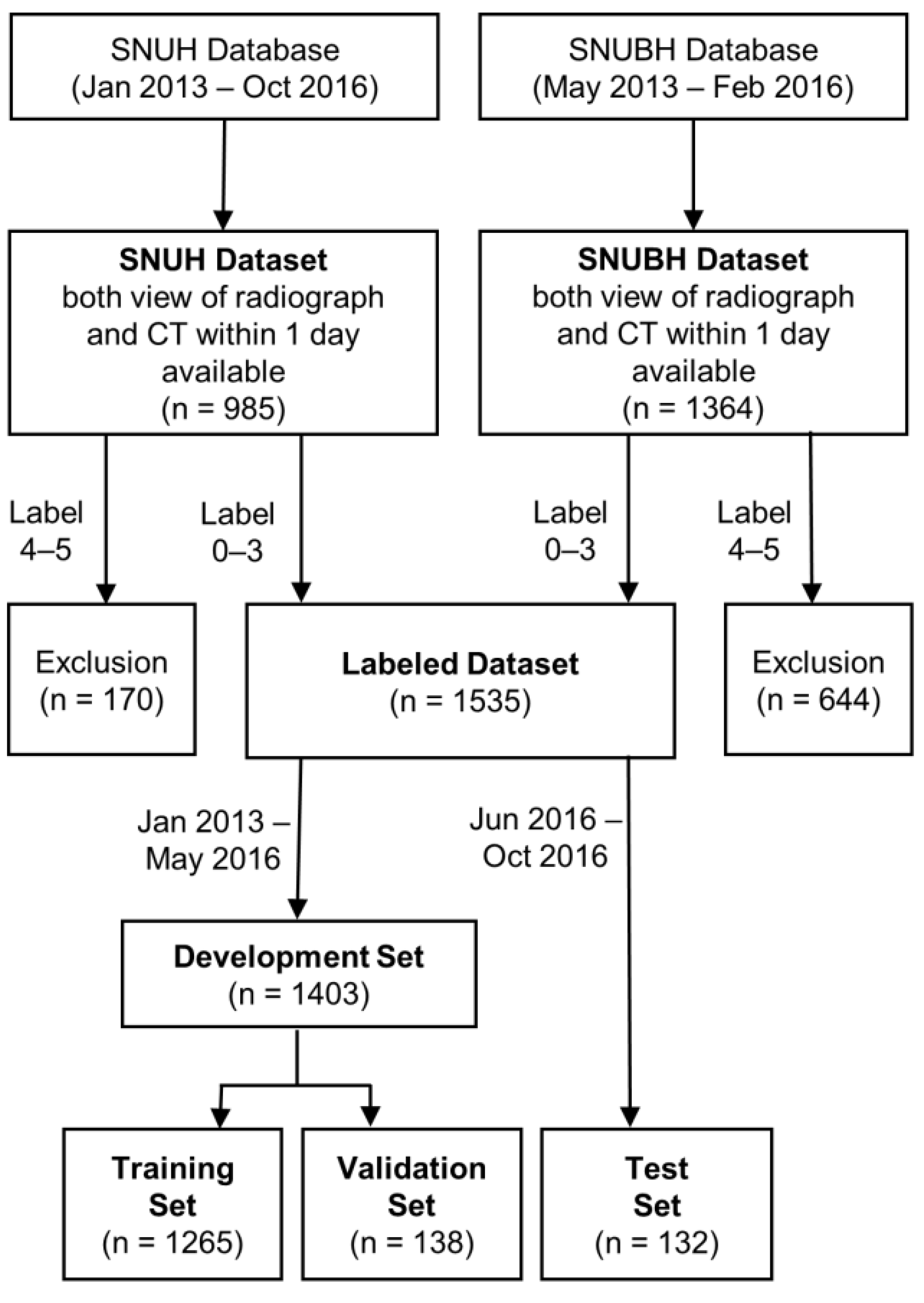
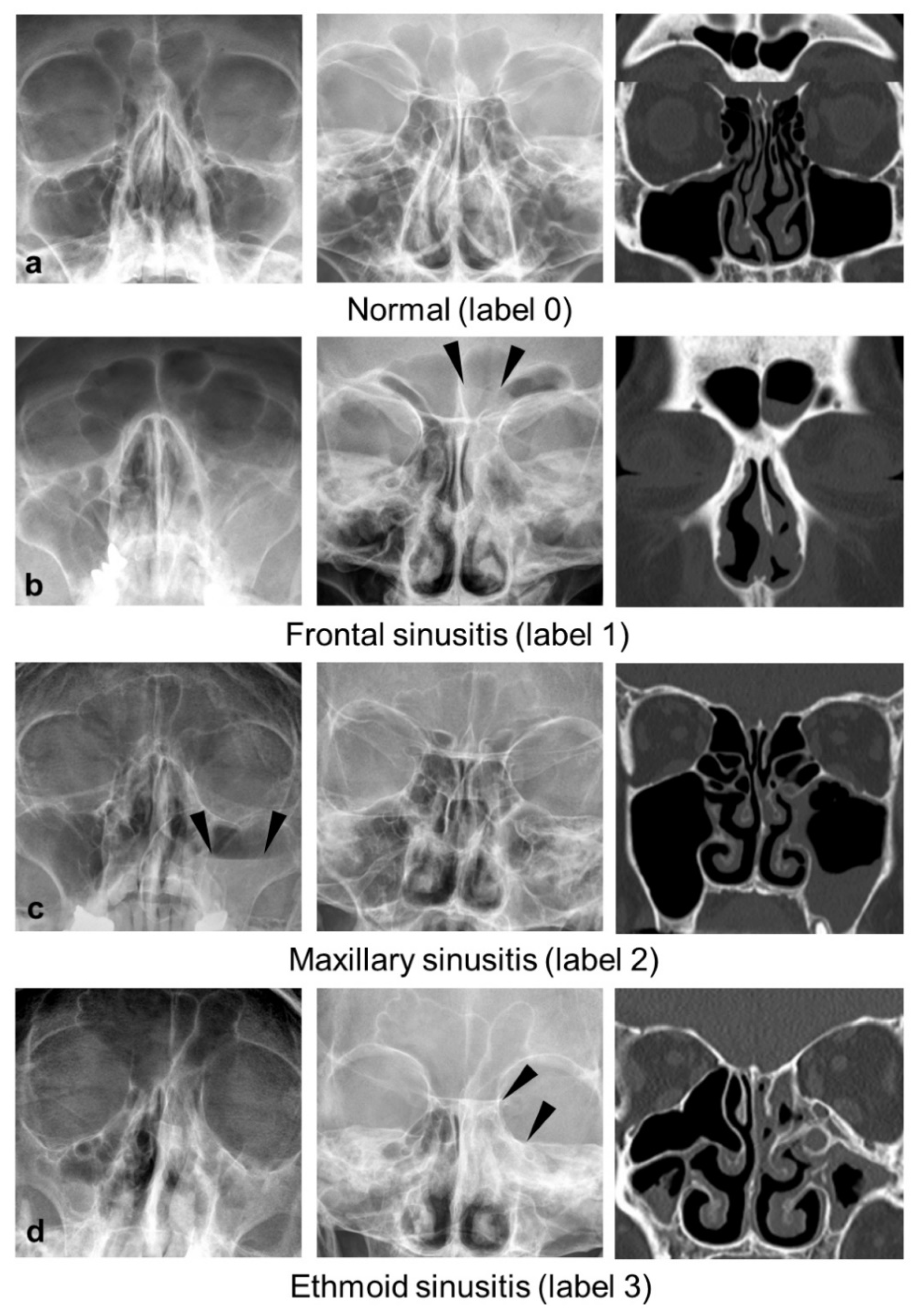
2.1. Dataset and Labeling
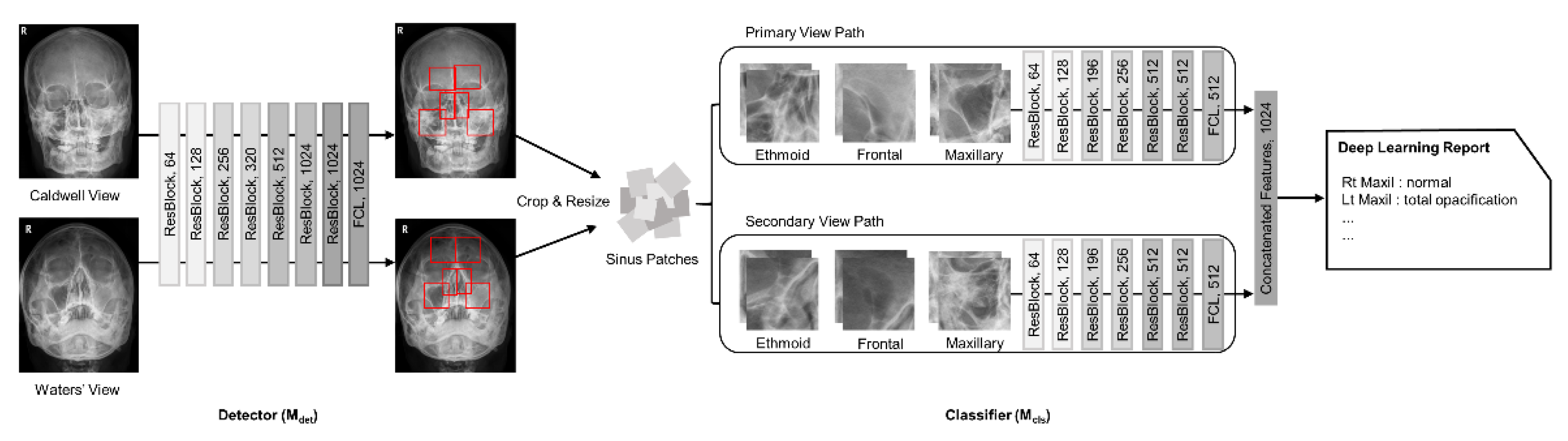
2.2. Network Architecture
2.3. Data Preprocessing
2.4. Training Settings
2.5. Observer Study
2.6. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Performance Comparison of Deep Learning Models
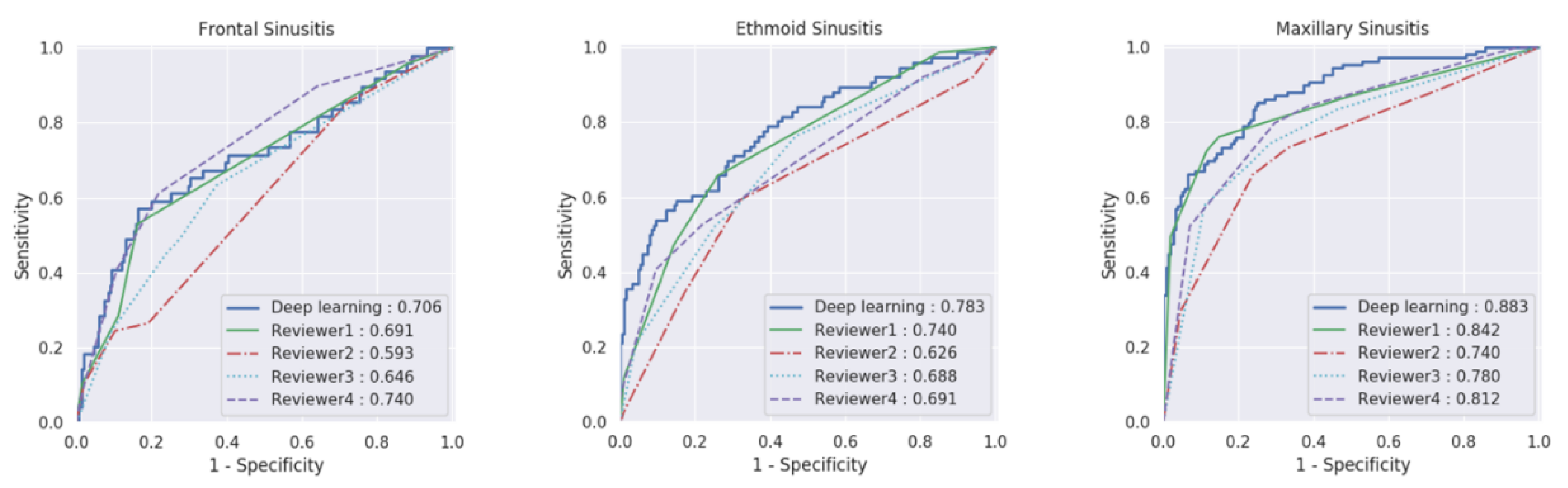
3.3. Performance Comparison of Multi-View Model with Radiologists
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anand, V.K. Epidemiology and economic impact of rhinosinusitis. Ann. Otol. Rhinol. Laryngol. Suppl. 2004, 193, 3–5. [Google Scholar] [CrossRef]
- Meltzer, E.O.; Hamilos, D.L. Rhinosinusitis diagnosis and management for the clinician: A synopsis of recent consensus guidelines. Mayo Clin. Proc. 2011, 86, 427–443. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Ashok Kumar, K.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical practice guideline (update): Adult sinusitis. Otolaryngol. Head Neck Surg. 2015, 152, S1–S39. [Google Scholar] [CrossRef] [Green Version]
- Aaløkken, T.M.; Hagtvedt, T.; Dalen, I.; Kolbenstvedt, A. Conventional sinus radiography compared with CT in the diagnosis of acute sinusitis. Dentomaxillofac. Radiol. 2003, 32, 60–62. [Google Scholar] [CrossRef]
- David, M. Imaging in sinus diseases. In Diseases of the Sinuses: Diagnosis and Management; Kennedy, D.W., Bolger, W.E., Zinreich, S.J., Eds.; B.C. Decker: Hamilton, ON, Canada, 2001; pp. 132–133. [Google Scholar]
- Merrell, R.A.; Yanagisawa, E. Radiographic anatomy of the paranasal sinuses. I. Waters’ view. Arch. Otolaryngol. 1968, 87, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, E.; Smith, H.M. Radiographic anatomy of the paranasal sinuses. IV. Caldwell view. Arch. Otolaryngol. 1968, 87, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Burke, T.F.; Guertler, A.T.; Timmons, J.H. Comparison of sinus x-rays with computed tomography scans in acute sinusitis. Acad. Emerg. Med. 1994, 1, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Davidson, T.M.; Brahme, F.J.; Gallagher, M.E. Radiographic evaluation for nasal dysfunction: Computed tomography versus plain films. Head Neck 1989, 11, 405–409. [Google Scholar] [CrossRef]
- Byun, J.E.; Shim, S.S.; Kim, Y.K.; Kong, K.A. Assessment of maxillary sinus wall thickness with paranasal sinus digital tomosynthesis and CT. J. Korean Soc. Radiol. 2017, 76, 314–321. [Google Scholar] [CrossRef]
- Christ, P.F.; Elshaer, M.E.A.; Ettlinger, F.; Tatavarty, S.; Bickel, M.; Bilic, P.; Rempfler, M.; Armbruster, M.; Hofmann, F.; D’Anastasi, M.; et al. Automatic Liver and Lesion Segmentation in CT Using Cascaded Fully Convolutional Neural Networks and 3D Conditional Random Fields. MICCAI 2016, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, P.; Sundaram, B. Deep Learning at Chest Radiography: Automated Classification of Pulmonary Tuberculosis by Using Convolutional Neural Networks. Radiology 2017, 284, 574–582. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Abe, O.; Kiryu, S. Deep Learning with Convolutional Neural Network for Differentiation of Liver Masses at Dynamic Contrast-enhanced CT: A Preliminary Study. Radiology 2018, 286, 887–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Jang, H.; Kijowski, R.; Bradshaw, T.; McMillan, A.B. Deep Learning MR Imaging-based Attenuation Correction for PET/MR Imaging. Radiology 2018, 286, 676–684. [Google Scholar] [CrossRef]
- Chen, M.C.; Ball, R.L.; Yang, L.; Moradzadeh, N.; Chapman, B.E.; Larson, D.B.; Langlotz, C.P.; Amrhein, T.J.; Lungren, M.P. Deep Learning to Classify Radiology Free-Text Reports. Radiology 2018, 286, 845–852. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, K.J.; Sunwoo, L.; Choi, D.; Nam, C.M.; Cho, J.; Kim, J.; Bae, Y.J.; Yoo, R.E.; Choi, B.S.; et al. Deep Learning in Diagnosis of Maxillary Sinusitis Using Conventional Radiography. Invest. Radiol. 2019, 54, 7–15. [Google Scholar] [CrossRef]
- Kim, H.G.; Lee, K.M.; Kim, E.J.; Lee, J.S. Improvement diagnostic accuracy of sinusitis recognition in paranasal sinus X-ray using multiple deep learning models. Quant. Imaging Med. Surg. 2019, 9, 942–951. [Google Scholar] [CrossRef]
- Lee, C.H.; Rhee, C.S.; Oh, S.J.; Jun, Y.H.; Min, Y.G.; Kim, I.O. Development of the Paranasal Sinuses in Children: A MRI Study. Korean J. Otorhinolaryngol. Head Neck Surg. 2000, 43, 507–513. [Google Scholar]
- Kozak, F.K.; Ospina, J.C.; Fandiño, M.C. Characteristics of Normal and Abnormal Postnatal Craniofacial Growth and Development. In Cummings Otolaryngology—Head and Neck Surgery, 6th ed.; Flint, P.W., Haughey, B.H., Niparko, J.K., Richardson, M.A., Lund, V.J., Robbins, K.T., Eds.; Elsevier Health Sciences: Philadelpia, PA, USA, 2014; Volume 3, pp. 2871–2874. [Google Scholar]
- Chicco, D.; Jurman, G. The advantages of the Matthews correlation coefficient (MCC) over F1 score and accuracy in binary classification evaluation. BMC Genom. 2020, 21, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Unal, I. Defining an Optimal Cut-Point Value in ROC Analysis: An Alternative Approach. Comput. Math. Methods Med. 2017, 2017, 1–14. [Google Scholar] [CrossRef]
- Obuchowski, N.A.; Rockette, H.E. Hypothesis testing of diagnostic accuracy for multiple readers and multiple tests an anova approach with dependent observations. Commun. Stat-Simul. C 1995, 24, 285–308. [Google Scholar] [CrossRef]
- Gisev, N.; Bell, J.S.; Chen, T.F. Interrater agreement and interrater reliability: Key concepts, approaches, and applications. Res. Soc. Adm. Pharm. 2013, 9, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.A. When to use the Bonferroni correction. Opthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef]
- Fagnan, L.J. Acute sinusitis: A cost-effective approach to diagnosis and treatment. Am. Fam. Physician. 1998, 58, 1795–1802. [Google Scholar]
- Stammberger, H. Endoscopic endonasal surgery--concepts in treatment of recurring rhinosinusitis. Part I. Anatomic and pathophysiologic considerations. Otolaryngol. Head Neck Surg. 1986, 94, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.N.; Oroszlan, G.; Anderson, T.D. Complications of frontal sinusitis and their management. Otolaryngol. Clin. N. Am. 2001, 34, 211–225. [Google Scholar] [CrossRef]
- Kim, Y.; Choi, D.; Lee, K.J.; Kang, Y.; Ahn, J.M.; Lee, E.; Lee, J.W.; Kang, H.S. Ruling out rotator cuff tear in shoulder radiograph series using deep learning: Redefining the role of conventional radiograph. Eur. Radiol. 2020, 30, 2843–2852. [Google Scholar] [CrossRef] [PubMed]
- Lisowska, A.; Beveridge, E.; Muir, K.; Poole, I. Thrombus detection in CT brain scans using a convolutional neural network. In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2017), Porto, Portugal, 21–23 February 2017; pp. 24–33. [Google Scholar]
- Oh, D.Y.; Kim, J.; Lee, K.J. Longitudinal Change Detection on Chest X-rays Using Geometric Correlation Maps. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2019, Shenzhen, China, 13–17 October 2019; Springer: Cham, Switzerland, 2019; pp. 748–756. [Google Scholar]
- Hwang, P.H.; Irwin, S.B.; Griest, S.E.; Caro, J.E.; Nesbit, G.M. Radiologic Correlates of Symptom-Based Diagnostic Criteria for Chronic Rhinosinusitis. Otolaryngol. Head Neck Surg. 2003, 128, 489–496. [Google Scholar] [CrossRef]
- Lau, J.; Zucker, D.; Engels, E.A.; Balk, E.; Barza, M.; Terrin, N.; Devine, D.; Chew, P.; Lang, T.; Liu, D. Diagnosis and Treatment of Acute Bacterial Rhinosinusitis. Evid. Rep. Technol. Assess. 1999, 9, 1–5. [Google Scholar]
- Engels, E.A.; Terrin, N.; Barza, M.; Lau, J. Meta-analysis of diagnostic tests for acute sinusitis. J. Clin. Epidemiol. 2000, 53, 852–862. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and Validation of a Deep Learning Algorithm for Detection of Diabetic Retinopathy in Retinal Fundus Photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Hoxworth, J.M.; Lal, D.; Fletcher, G.P.; Patel, A.C.; He, M.; Paden, R.G.; Hara, A.K. Radiation dose reduction in paranasal sinus CT using model-based iterative reconstruction. AJNR Am. J. Neuroradiol. 2014, 35, 644–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.; Tashiro, S. Estimation of the effects of medical diagnostic radiation exposure based on DNA damage. J. Radiat. Res. 2018, 59, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Preston, D.L.; Shimizu, Y.; Pierce, D.A.; Suyama, A.; Mabuchi, K. Studies of mortality of atomic bomb survivors. Report 13: Solid cancer and noncancer disease mortality: 1950–1997. Radiat. Res. 2003, 160, 381–407. [Google Scholar] [CrossRef]
- Williams, J.W., Jr.; Roberts, L., Jr.; Distell, B.; Simel, D.L. Diagnosing sinusitis by X-ray: Is a single Waters view adequate? J. Gen. Intern. Med. 1992, 7, 481–485. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Training Set | Validation Set | Temporal Test Set | Total |
|---|---|---|---|---|
| Number of Patients | 1265 | 138 | 132 | 1535 |
| Age (y) † | 50 ± 19 | 49 ± 18 | 54 ± 17 | 51 ± 19 |
| Sex | ||||
| Men | 659 (52.1) | 76 (55.1) | 57 (43.2) | 792 (51.6) |
| Women | 606 (47.9) | 62 (44.9) | 75 (56.8) | 743 (48.4) |
| Frontal Sinusitis ‡ | ||||
| 0—normal | 2029 (80.2) | 212 (76.8) | 215 (81.4) | 2456 (80.0) |
| 1—mucosal thickening > 2 mm | 286 (11.3) | 38 (13.8) | 37 (14.0) | 361 (11.8) |
| 2—air-fluid level | 3 (0.1) | 1 (0.4) | 0 (0.0) | 4 (0.1) |
| 3—total opacification | 212 (8.4) | 25 (9.1) | 12 (4.5) | 249 (8.1) |
| Ethmoid Sinusitis ‡ | ||||
| 0—normal | 1589 (62.8) | 178 (64.5) | 188 (71.2) | 1955 (63.7) |
| 1—mucosal thickening > 2 mm | 171 (6.8) | 14 (5.1) | 20 (7.6) | 205 (6.7) |
| 2—air-fluid level | 184 (7.3) | 18 (6.5) | 21 (8.0) | 223 (7.3) |
| 3—total opacification | 586 (23.2) | 66 (23.9) | 35 (13.3) | 687 (22.4) |
| Maxillary Sinusitis ‡ | ||||
| 0—normal | 1375 (54.3) | 149 (54.0) | 155 (58.7) | 1679 (54.7) |
| 1—mucosal thickening > 4 mm | 738 (29.2) | 77 (27.9) | 87 (33.0) | 902 (29.4) |
| 2—air-fluid level | 145 (5.7) | 22 (8.0) | 5 (1.9) | 172 (5.6) |
| 3—total opacification | 272 (10.8) | 28 (10.1) | 17 (6.4) | 317 (10.3) |
| Single Primary View | Single Secondary View | Multi-View | |
|---|---|---|---|
| Frontal Sinusitis | |||
| AUC | 0.72 (0.63–0.80) | 0.72 (0.65–0.80) | 0.71 (0.62–0.80) |
| p-Value * | 0.645 | 0.685 | |
| Ethmoid Sinusitis | |||
| AUC | 0.79 (0.73–0.85) | 0.70 (0.63–0.77) | 0.78 (0.72–0.85) |
| p-Value * | 0.566 | 0.004 | |
| Maxillary Sinusitis | |||
| AUC | 0.86 (0.81–0.90) | 0.76 (0.70–0.81) | 0.88 (0.84–0.92) |
| p-Value * | 0.038 | <0.001 |
| Frontal Sinusitis | Sensitivity | Specificity | PPV | MCC | AUC | p-Value † |
| Deep learning algorithm | 0.71 (0.62–0.80) | |||||
| Optimal Cutoff † | 57.1 (42.2–71.2) | 82.8 (77.1–87.6) | 43.1 (30.8–56.0) | 0.36 (0.25–0.46) | ||
| Cutoff for High Sensitivity | 71.4 (56.7–83.4) | 48.8 (42.0–55.7) | 24.1 (17.4–31.9) | 0.16 (0.04–0.27) | ||
| Cutoff for High Specificity | 40.8 (27.0–55.8) | 90.2 (85.5–93.9) | 48.8 (32.9–64.9) | 0.33 (0.22–0.44) | ||
| Radiologist | ||||||
| 1 | 49.0 (34.4–63.7) | 85.6 (80.2–90.0) | 43.6 (33.4–54.4) | 0.33 (0.22–0.43) | 0.69 (0.61–0.77) | 0.402 |
| 2 | 26.5 (14.9–41.1) | 85.1 (79.6–89.6) | 28.9 (18.8–41.7) | 0.12 (0.00–0.24) | 0.59 (0.51–0.67) | 0.032 |
| 3 | 46.9 (32.5–61.7) | 74.0 (67.5–79.7) | 29.1 (22.0–37.4) | 0.18 (0.06–0.29) | 0.64 (0.56–0.73) | 0.165 |
| 4 | 49.0 (34.4–63.7) | 84.7 (79.1–89.2) | 42.1 (32.2–52.6) | 0.32 (0.20–0.42) | 0.73 (0.66–0.82) | 0.711 |
| Overall ‡ | 42.9 | 82.4 | 0.66 (0.56–0.78) | 0.477 | ||
| Ethmoid Sinusitis | Sensitivity | Specificity | PPV | MCC | AUC | p-Value † |
| Deep learning algorithm | 0.78 (0.72–0.85) | |||||
| Optimal Cutoff † | 59.2 (47.3–70.4) | 83.5 (77.4–88.5) | 59.2 (47.3–70.4) | 0.43 (0.32–0.52) | ||
| Cutoff for High Sensitivity | 78.9 (68.1–87.5) | 59.0 (51.7–66.1) | 43.8 (35.3–52.5) | 0.34 (0.23–0.45) | ||
| Cutoff for High Specificity | 38.2 (27.2–50.0) | 95.2 (91.1–97.8) | 76.3 (59.8–88.6) | 0.43 (0.33–0.52) | ||
| Radiologist | ||||||
| 1 | 61.8 (50.0–72.8) | 78.2 (71.6–83.9) | 53.4 (45.3–61.3) | 0.38 (0.28–0.48) | 0.74 (0.68–0.80) | 0.170 |
| 2 | 51.3 (39.6–63.0) | 75.0 (68.2–81.0) | 45.4 (37.4–53.6) | 0.25 (0.14–0.36) | 0.63 (0.55–0.70) | <0.001 * |
| 3 | 61.8 (50.0–72.8) | 66.0 (58.7–72.7) | 42.3 (36.0–48.9) | 0.25 (0.14–0.36) | 0.69 (0.62–0.76) | 0.024 |
| 4 | 50.0 (38.3–61.7) | 82.4 (76.2–87.6) | 53.5 (44.0–62.8) | 0.33 (0.22–0.43) | 0.69 (0.62–0.76) | 0.028 |
| Overall ‡ | 56.2 | 75.4 | 0.69 (0.61–0.76) | 0.012 * | ||
| Maxillary Sinusitis | Sensitivity | Specificity | PPV | MCC | AUC | p-Value † |
| Deep learning algorithm | 0.88 (0.84–0.92) | |||||
| Optimal Cutoff † | 80.3 (69.5–88.5) | 71.8 (64.8–78.1) | 78.6 (69.1–86.2) | 0.58 (0.50–0.66) | ||
| Cutoff for High Sensitivity | 85.3 (77.3–91.4) | 72.9 (65.2–79.7) | 68.9 (60.4–76.6) | 0.57 (0.49–0.65) | ||
| Cutoff for High Specificity | 63.3 (53.5–72.3) | 93.5 (88.5–96.9) | 87.3 (78.0–93.8) | 0.61 (0.53–0.68) | ||
| Radiologist | ||||||
| 1 | 75.2 (66.0–83.0) | 87.1 (80.8–91.9) | 80.4 (72.9–86.2) | 0.63 (0.55–0.70) | 0.84 (0.79–0.89) | 0.112 |
| 2 | 72.5 (63.1–80.6) | 69.7 (61.8–76.8) | 62.7 (56.3–68.7) | 0.42 (0.31–0.51) | 0.74 (0.67–0.80) | <0.001 * |
| 3 | 74.3 (65.1–82.2) | 70.3 (62.5–77.4) | 63.8 (57.4–69.7) | 0.44 (0.34–0.53) | 0.78 (0.72–0.84) | 0.002 * |
| 4 | 84.4 (76.2–90.6) | 65.8 (57.8–73.2) | 63.5 (57.9–68.7) | 0.50 (0.40–0.58) | 0.81 (0.76–0.86) | 0.016 |
| Overall ‡ | 76.6 | 73.2 | 0.79 (0.73–0.86) | 0.013 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, Y.; Lee, K.; Sunwoo, L.; Choi, D.; Oh, D.Y.; Lee, K.J.; Kim, Y.; Kim, J.-W.; Cho, S.J.; Baik, S.H.; et al. Deep Learning for Diagnosis of Paranasal Sinusitis Using Multi-View Radiographs. Diagnostics 2021, 11, 250. https://doi.org/10.3390/diagnostics11020250
Jeon Y, Lee K, Sunwoo L, Choi D, Oh DY, Lee KJ, Kim Y, Kim J-W, Cho SJ, Baik SH, et al. Deep Learning for Diagnosis of Paranasal Sinusitis Using Multi-View Radiographs. Diagnostics. 2021; 11(2):250. https://doi.org/10.3390/diagnostics11020250
Chicago/Turabian StyleJeon, Yejin, Kyeorye Lee, Leonard Sunwoo, Dongjun Choi, Dong Yul Oh, Kyong Joon Lee, Youngjune Kim, Jeong-Whun Kim, Se Jin Cho, Sung Hyun Baik, and et al. 2021. "Deep Learning for Diagnosis of Paranasal Sinusitis Using Multi-View Radiographs" Diagnostics 11, no. 2: 250. https://doi.org/10.3390/diagnostics11020250