Blood-Based Detection of Colorectal Cancer Using Cancer-Specific DNA Methylation Markers

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Samples
2.2. Cell Culture and Reagents
2.3. Xenograft Mouse Model
2.4. DNA Extraction and Bisulfite Modification
2.5. Selection of Target Probes
2.6. ddMethyLight Assay
2.7. Data Analysis of ddMethyLight
2.8. Statistical Analysis
3. Results
3.1. Proportional Increase in Methylated DNA Alleles in cfDNA Samples from Xenografted Mice
3.2. Sensitivity and Specificity of Ten DNA Methylation Markers for the Detection of CRC with cfDNA Samples
3.3. Panels of DNA Methylation Markers and the Comparison of Their Sensitivity
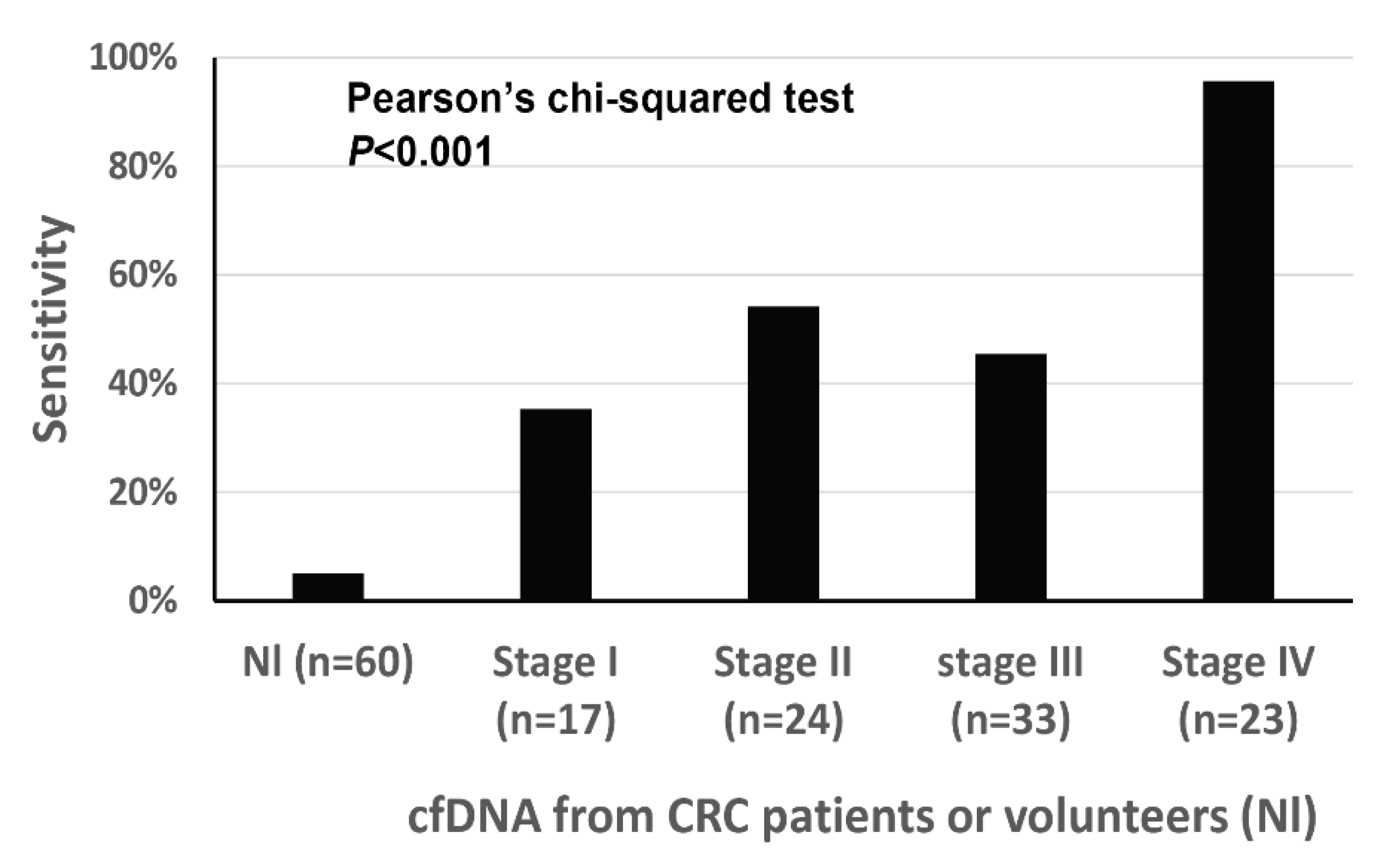
3.4. Detection of Methylated DNA in cfDNA and Its Relationship with Clinicopathological Features
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CRC | Colorectal cancer |
| cfDNA | Cell-free DNA |
| ctDNA | Circulating tumor DNA |
| GEO | Gene Expression Omnibus |
| TCGA | The Cancer Genome Atlas |
| ddMethyLight | droplet digital PCR-based MethyLight |
References
- Lo, Y.M.; Zhang, J.; Leung, T.N.; Lau, T.K.; Chang, A.M.; Hjelm, N.M. Rapid clearance of fetal DNA from maternal plasma. Am. J. Hum. Genet 1999, 64, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Yao, W.; Mei, C.; Nan, X.; Hui, L. Evaluation and comparison of in vitro degradation kinetics of DNA in serum, urine and saliva: A qualitative study. Gene 2016, 590, 142–148. [Google Scholar] [CrossRef]
- Wan, J.C.; Massie, C.; Garcia-Corbacho, J.; Mouliere, F.; Brenton, J.D.; Caldas, C.; Pacey, S.; Baird, R.; Rosenfeld, N. Liquid biopsies come of age: Towards implementation of circulating tumour DNA. Nat. Rev. Cancer 2017, 17, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.; Cheng, J.B.; Li, D.; Xie, M.; Hong, C.; Maire, C.L.; Ligon, K.L.; Hirst, M.; Marra, M.A.; Costello, J.F.; et al. Estimating absolute methylation levels at single-CpG resolution from methylation enrichment and restriction enzyme sequencing methods. Genome Res. 2013, 23, 1541–1553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrijver, W.A.; Jiwa, L.S.; van Diest, P.J.; Moelans, C.B. Promoter hypermethylation profiling of distant breast cancer metastases. Breast Cancer Res. Treat. 2015, 151, 41–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, A.F.; Assenov, Y.; Martin-Subero, J.I.; Balint, B.; Siebert, R.; Taniguchi, H.; Yamamoto, H.; Hidalgo, M.; Tan, A.C.; Galm, O.; et al. A DNA methylation fingerprint of 1628 human samples. Genome Res. 2012, 22, 407–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Liu, S.; Shen, C.; Wu, Y.; Zhang, L.; Chen, X.; Lu, F. DNA methylation consistency implicates the primary tumor cell origin of recurrent hepatocellular carcinoma. Epigenomics 2015, 7, 581–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lister, R.; Pelizzola, M.; Dowen, R.H.; Hawkins, R.D.; Hon, G.; Tonti-Filippini, J.; Nery, J.R.; Lee, L.; Ye, Z.; Ngo, Q.M.; et al. Human DNA methylomes at base resolution show widespread epigenomic differences. Nature 2009, 462, 315–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lokk, K.; Modhukur, V.; Rajashekar, B.; Märtens, K.; Mägi, R.; Kolde, R.; Koltšina, M.; Nilsson, T.K.; Vilo, J.; Salumets, A.; et al. DNA methylome profiling of human tissues identifies global and tissue-specific methylation patterns. Genome Biol. 2014, 15, r54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Zhao, H.; Li, J.; Liu, H.; Wang, F.; Wei, Y.; Su, J.; Zhang, D.; Liu, T.; Zhang, Y. The identification of specific methylation patterns across different cancers. PLoS ONE 2015, 10, e0120361. [Google Scholar] [CrossRef] [PubMed]
- Moran, S.; Martínez-Cardús, A.; Sayols, S.; Musulén, E.; Balañá, C.; Estival-Gonzalez, A.; Moutinho, C.; Heyn, H.; Diaz-Lagares, A.; de Moura, M.C.; et al. Epigenetic profiling to classify cancer of unknown primary: A multicentre, retrospective analysis. Lancet Oncol. 2016, 17, 1386–1395. [Google Scholar] [CrossRef]
- Lange, C.P.; Campan, M.; Hinoue, T.; Schmitz, R.F.; van der Meulen-de, A.E.; Slingerland, H.; Kok, P.J.; van Dijk, C.M.; Weisenberger, D.J.; Shen, H.; et al. Genome-scale discovery of DNA-methylation biomarkers for blood-based detection of colorectal cancer. PLoS ONE 2012, 7, e50266. [Google Scholar] [CrossRef]
- Weisenberger, D.J.; Trinh, B.N.; Campan, M.; Sharma, S.; Long, T.I.; Ananthnarayan, S.; Liang, G.; Esteva, F.J.; Hortobagyi, G.N.; McCormick, F.; et al. DNA methylation analysis by digital bisulfite genomic sequencing and digital MethyLight. Nucleic Acids Res. 2008, 36, 4689–4698. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Carter, K.T.; Makar, K.W.; Vickers, K.; Ulrich, C.M.; Schoen, R.E.; Brenner, D.; Markowitz, S.D.; Grady, W.M. MethyLight droplet digital PCR for detection and absolute quantification of infrequently methylated alleles. Epigenetics 2015, 10, 803–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, S.Ø.; Øgaard, N.; Ørntoft, M.B.W.; Rasmussen, M.H.; Bramsen, J.B.; Kristensen, H.; Mouritzen, P.; Madsen, M.R.; Madsen, A.H.; Sunesen, K.G.; et al. Novel DNA methylation biomarkers show high sensitivity and specificity for blood-based detection of colorectal cancer-a clinical biomarker discovery and validation study. Clin. Epigenetics 2019, 11, 158. [Google Scholar] [CrossRef] [PubMed]
- Church, T.R.; Wandell, M.; Lofton-Day, C.; Mongin, S.J.; Burger, M.; Payne, S.R.; Castaños-Vélez, E.; Blumenstein, B.A.; Rösch, T.; Osborn, N.; et al. Prospective evaluation of methylated SEPT9 in plasma for detection of asymptomatic colorectal cancer. Gut 2014, 63, 317–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, H.; Zhao, Q.; Wei, W.; Zheng, L.; Yi, S.; Li, G.; Wang, W.; Sheng, H.; Pu, H.; Mo, H.; et al. Circulating tumor DNA methylation profiles enable early diagnosis, prognosis prediction, and screening for colorectal cancer. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.C. Comment on ‘Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA’ by M. C. Liu et al. Ann. Oncol. 2020, 31, 1266–1267. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M. Response to W.C. Taylor, and C. Fiala and E.P. Diamandis. Ann. Oncol. 2020, 31, 1268–1270. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cut-off for Positivity Set at 1 Methylated Droplet | Cut-off for Positivity Set at 2 Methylated Droplets | |||
|---|---|---|---|---|
| Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | |
| TMEM90B | 52.1 | 81.7 | 22.2 | 100.0 |
| PCDHG | 48.7 | 81.7 | 20.5 | 95.0 |
| PPP1R16B | 47.0 | 86.7 | 23.1 | 96.7 |
| ADGRB1 | 47.0 | 71.7 | 23.9 | 95.0 |
| GLI3 | 43.6 | 93.3 | 21.4 | 100.0 |
| ANKRD13B | 41.0 | 88.3 | 20.5 | 98.3 |
| THBD | 39.3 | 78.3 | 20.5 | 100.0 |
| c9orf50 | 31.6 | 85.0 | 17.1 | 96.7 |
| FAM123A | 23.1 | 96.7 | 10.3 | 100.0 |
| SLIT3 | 22.2 | 95.0 | 10.3 | 100.0 |
| No. of Markers | Sum of Markers with ≥ 1 Methylated Droplet(s) | AUC | 95% C.I. | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||||||
| 6 | ANKRD13 | FAM123A | GLI3 | PCDHG | PPP1R16B | TMEM90B | 0.866 | 0.814 | 0.917 | ||
| 8 | ADGRB1 | ANKRD13 | FAM123A | GLI3 | PCDHG | PPP1R16B | SLIT3 | TMEM90B | 0.862 | 0.809 | 0.915 |
| 7 | ADGRB1 | ANKRD13 | FAM123A | GLI3 | PCDHG | PPP1R16B | TMEM90B | 0.860 | 0.807 | 0.913 | |
| 5 | FAM123A | GLI3 | PPP1R16B | SLIT3 | TMEM90B | 0.839 | 0.782 | 0.897 | |||
| 6 | ADGRB1 | FAM123A | GLI3 | PPP1R16B | SLIT3 | TMEM90B | 0.828 | 0.769 | 0.888 | ||
| 5 | ADGRB1 | FAM123A | GLI3 | PPP1R16B | SLIT3 | 0.823 | 0.762 | 0.884 | |||
| 3 | GLI3 | PPP1R16B | TMEM90B | 0.822 | 0.761 | 0.884 | |||||
| n | Mean | S.D. | p-Value ** | ||
|---|---|---|---|---|---|
| Tumor subsite | Right colon | 15 | 1.73 | 1.438 | 0.675 |
| Left colon | 63 | 2.02 | 1.314 | ||
| Rectum | 19 | 1.89 | 1.243 | ||
| Differentiation * | WD | 8 | 1.13 | 1.126 | 0.051 |
| MD | 79 | 1.95 | 1.300 | ||
| PD | 10 | 2.55 | 1.265 | ||
| Lymphatic emboli | Absent | 57 | 1.60 | 1.193 | 0.001 |
| Present | 40 | 2.45 | 1.319 | ||
| Venous invasion | Absent | 77 | 1.71 | 1.037 | 0.011 |
| Present | 20 | 2.85 | 1.814 | ||
| Perineural invasion | Absent | 60 | 1.68 | 1.157 | 0.028 |
| Present | 37 | 2.38 | 1.441 | ||
| T category | 1 | 8 | 1.13 | 0.991 | 0.001 |
| 2 | 17 | 1.41 | 0.870 | ||
| 3 | 53 | 1.87 | 1.225 | ||
| 4 | 19 | 3.00 | 1.414 | ||
| N category | 0 | 44 | 1.48 | 0.849 | 0.007 |
| 1 | 33 | 2.24 | 1.480 | ||
| 2 | 20 | 2.50 | 1.539 | ||
| M category | 0 | 74 | 1.53 | 0.996 | <0.001 |
| 1 | 23 | 3.30 | 1.295 | ||
| Stage | I | 17 | 1.24 | 0.831 | <0.001 |
| II | 24 | 1.67 | 0.816 | ||
| III | 33 | 1.58 | 1.173 | ||
| IV | 23 | 3.30 | 1.295 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, N.-Y.; Park, J.-W.; Wen, X.; Shin, Y.-J.; Kang, J.-K.; Song, S.-H.; Kim, H.-P.; Kim, T.-Y.; Bae, J.M.; Kang, G.H. Blood-Based Detection of Colorectal Cancer Using Cancer-Specific DNA Methylation Markers. Diagnostics 2021, 11, 51. https://doi.org/10.3390/diagnostics11010051
Cho N-Y, Park J-W, Wen X, Shin Y-J, Kang J-K, Song S-H, Kim H-P, Kim T-Y, Bae JM, Kang GH. Blood-Based Detection of Colorectal Cancer Using Cancer-Specific DNA Methylation Markers. Diagnostics. 2021; 11(1):51. https://doi.org/10.3390/diagnostics11010051
Chicago/Turabian StyleCho, Nam-Yun, Ji-Won Park, Xianyu Wen, Yun-Joo Shin, Jun-Kyu Kang, Sang-Hyun Song, Hwang-Phill Kim, Tae-You Kim, Jeong Mo Bae, and Gyeong Hoon Kang. 2021. "Blood-Based Detection of Colorectal Cancer Using Cancer-Specific DNA Methylation Markers" Diagnostics 11, no. 1: 51. https://doi.org/10.3390/diagnostics11010051