Convolutional Neural Network-Based Humerus Segmentation and Application to Bone Mineral Density Estimation from Chest X-ray Images of Critical Infants

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
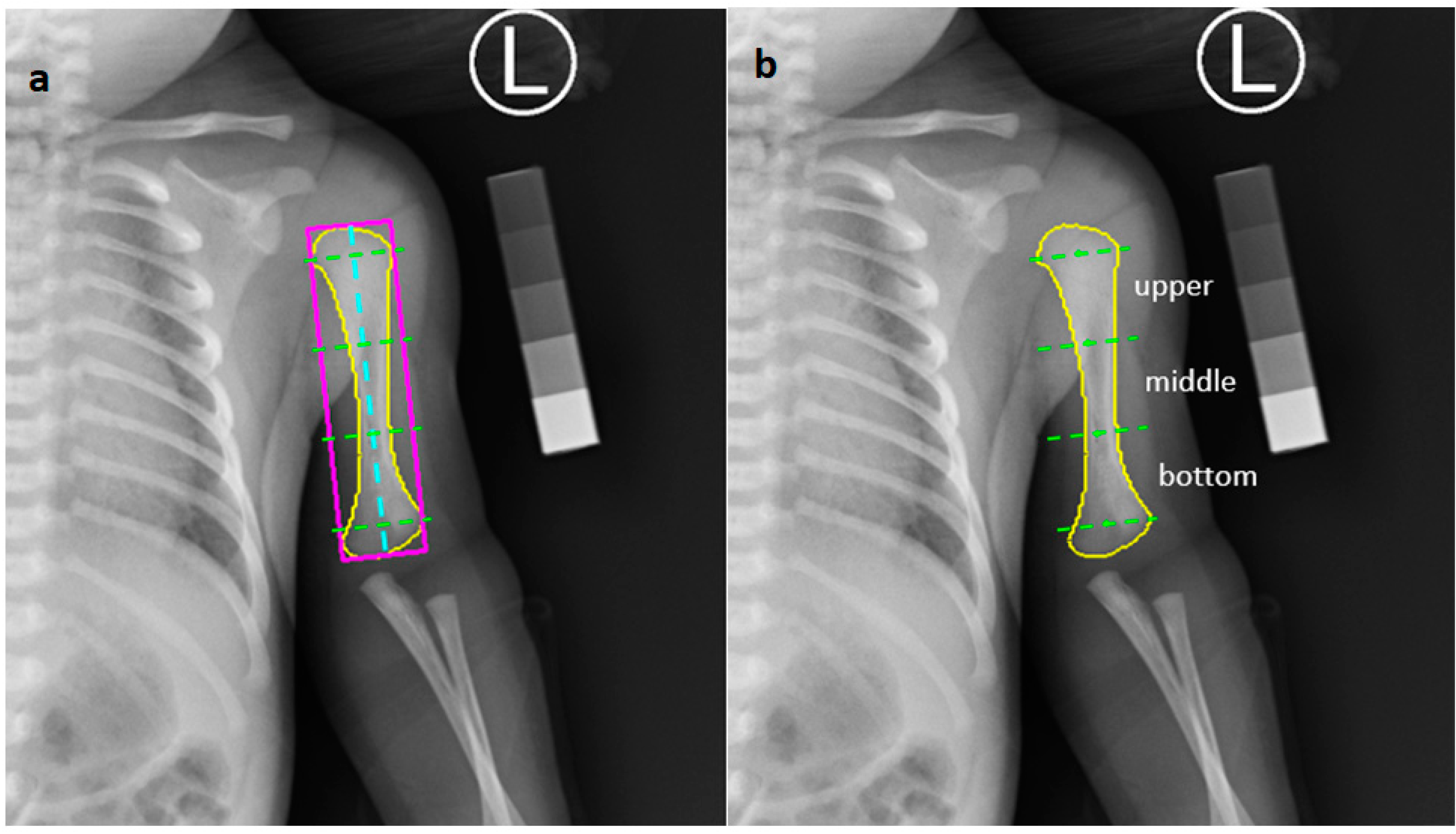
2.2. Bone Segmentation
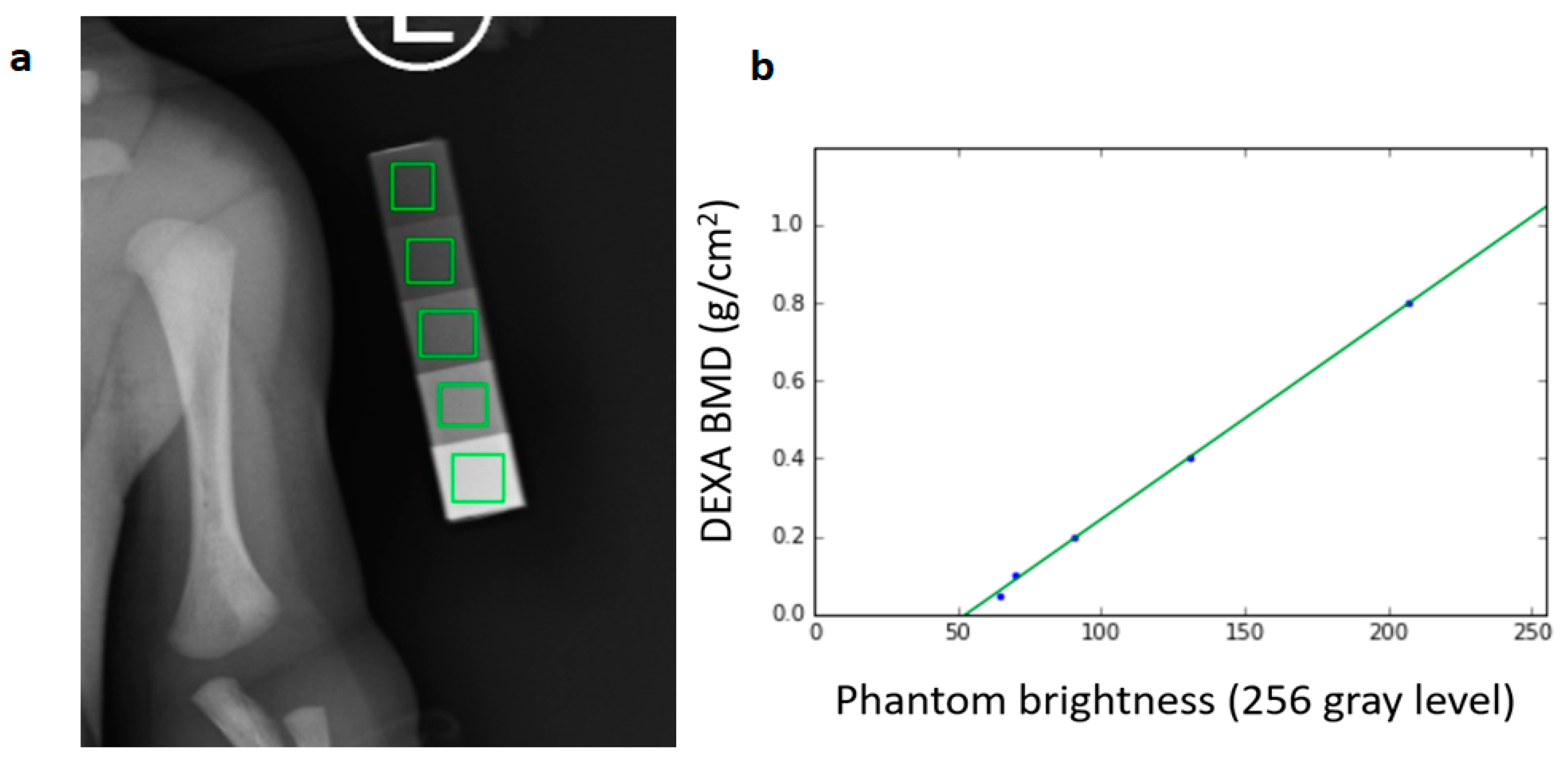
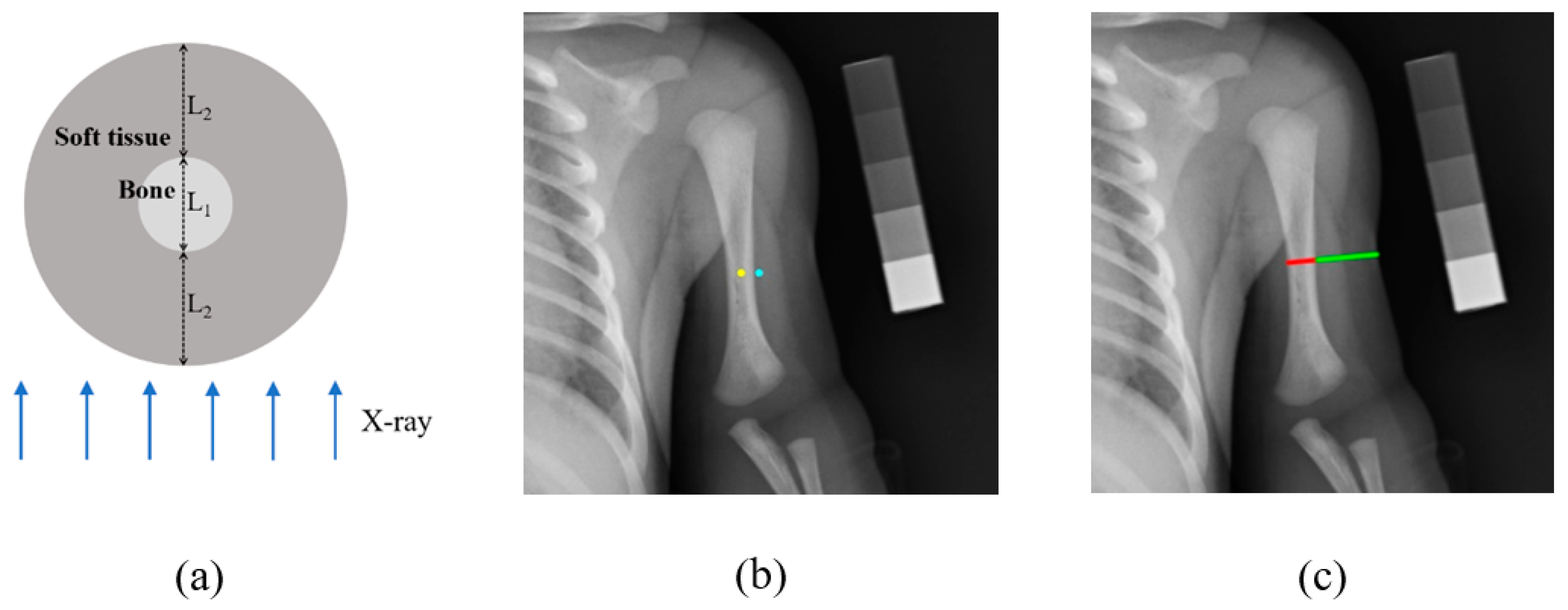
2.3. Association between DEXA Phantom Brightness and BMD Value
2.4. BMD Estimation in Prematurity
3. Results
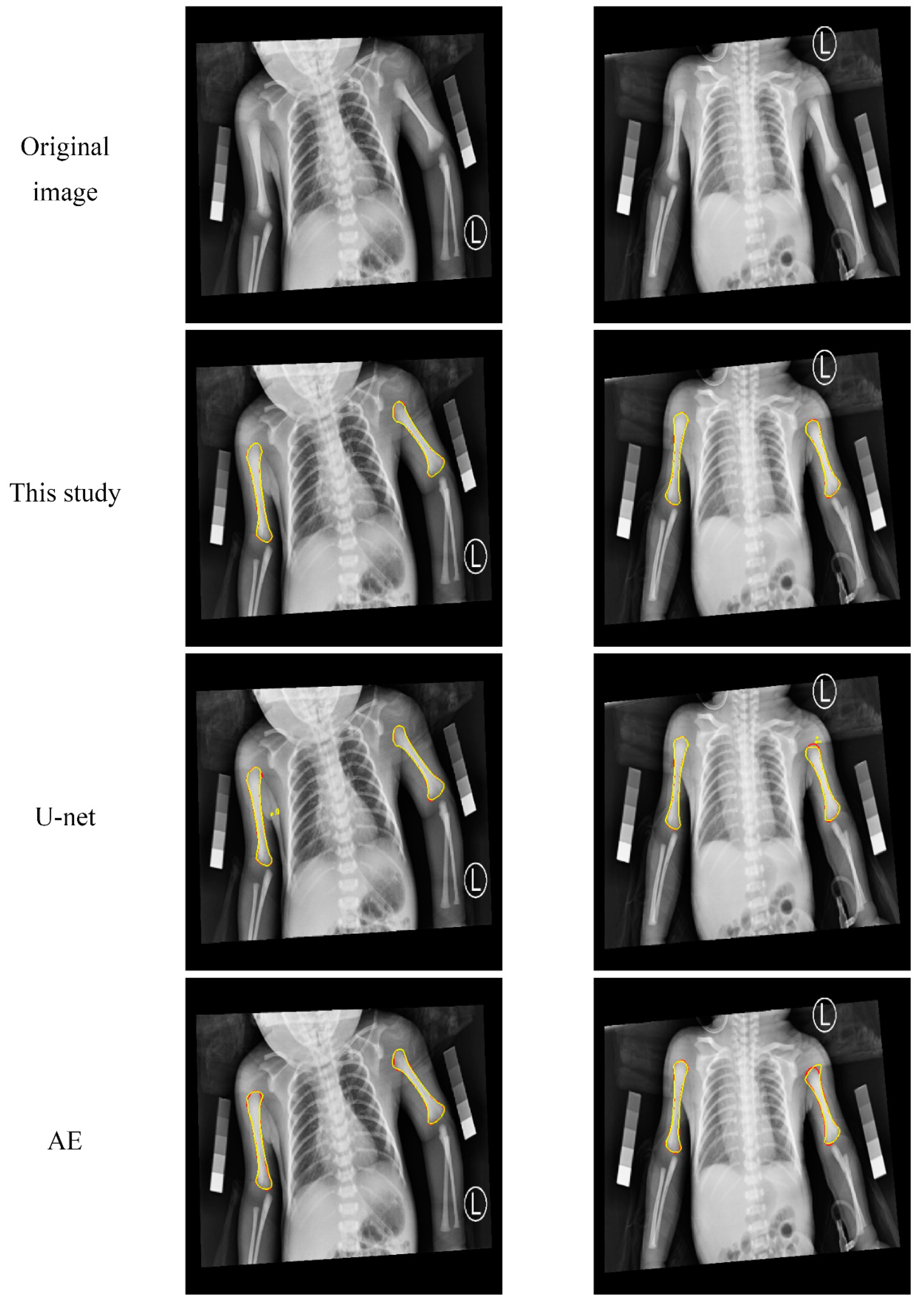
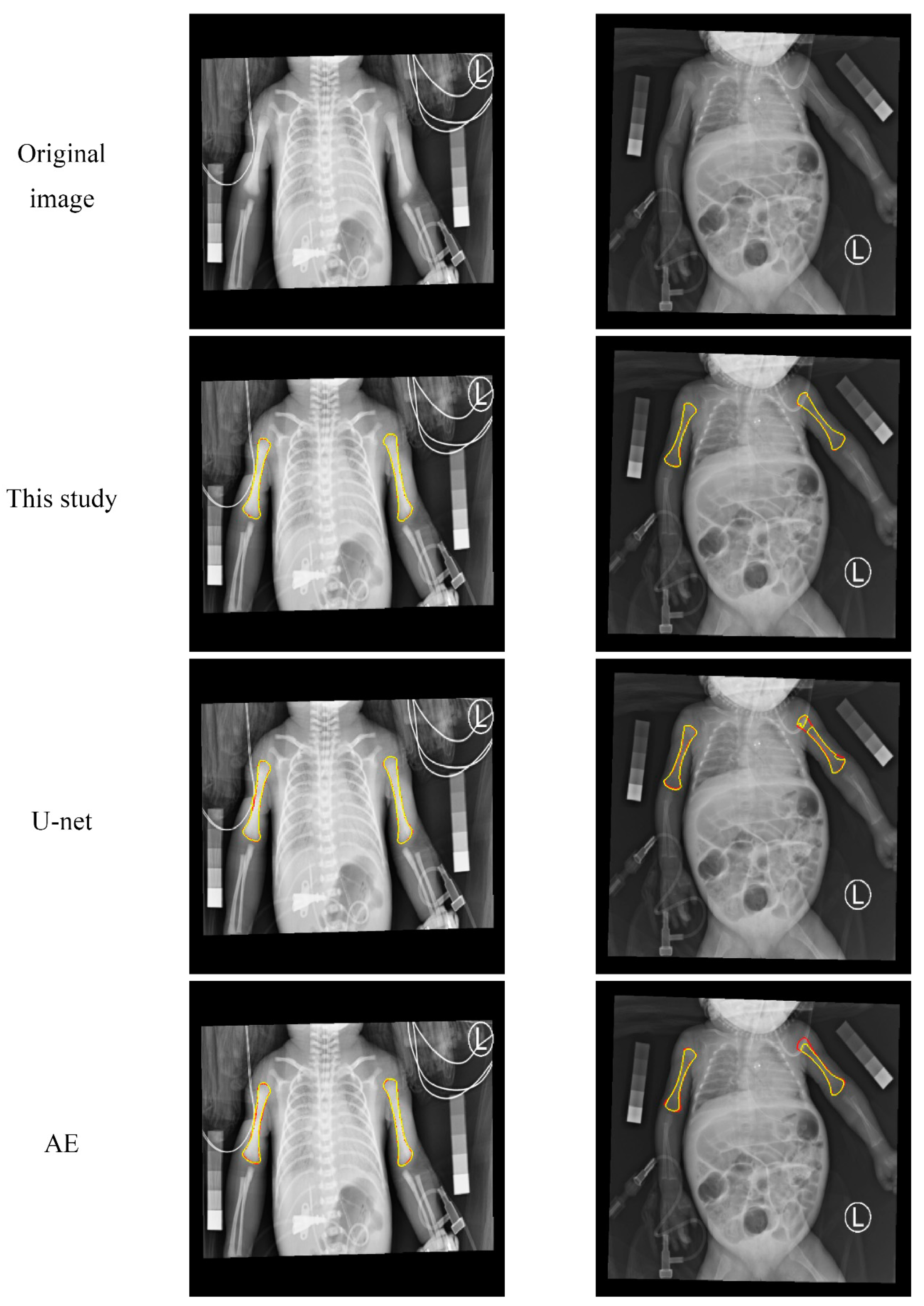
3.1. Qualitative Evaluation of the Humerus Segmentation
3.2. Quantitative Analysis of the Segmentation Results
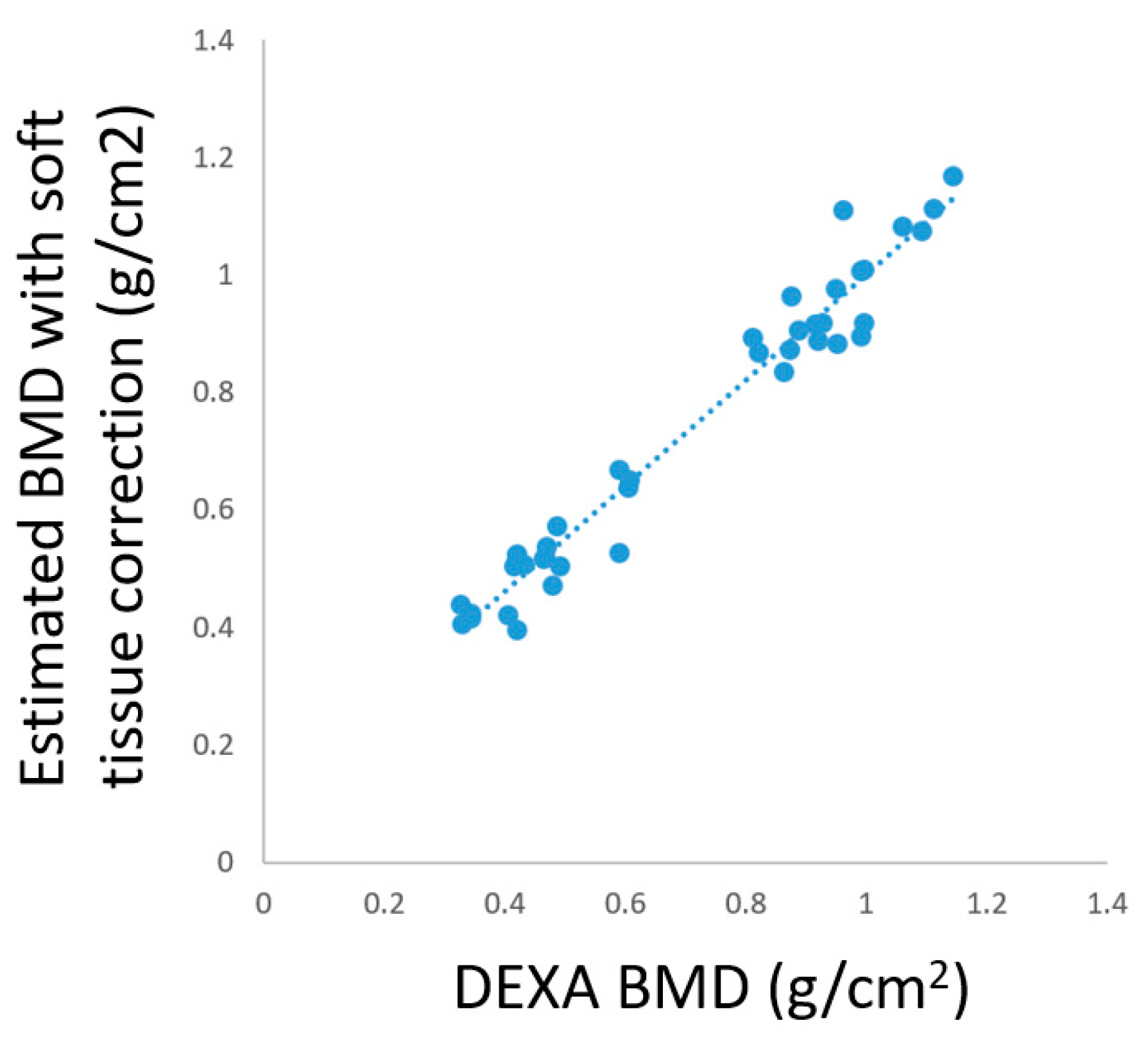
3.3. BMD Estimation in Prematurity
4. Discussion
4.1. Number of Parameters and Computation Time
4.2. Feasibility of the Soft Tissue Correction Mechanism
4.3. Limitation and Strength
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Related Settings |
|---|---|
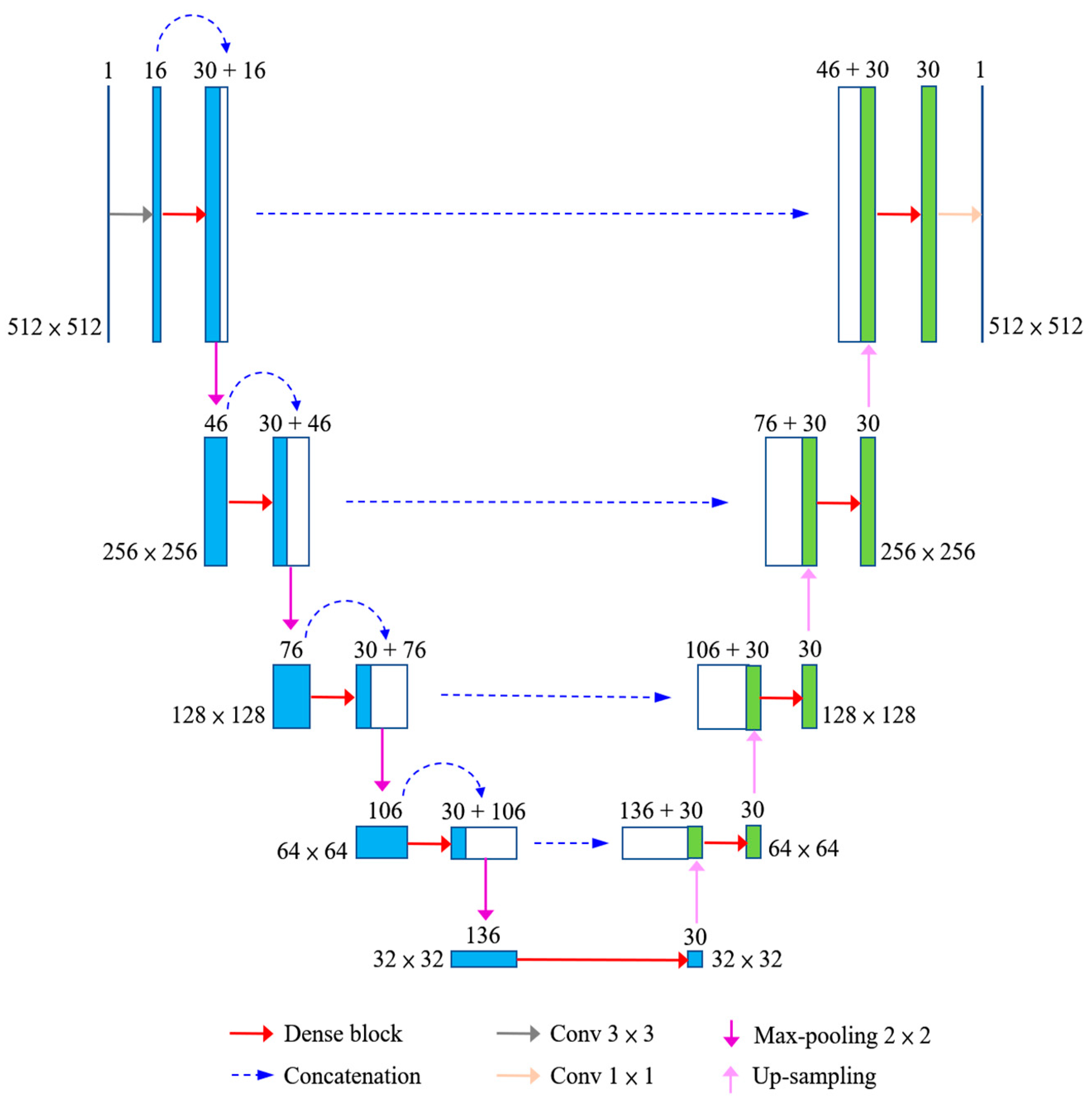
| Filter size of convolution in the main network architecture | 3 × 3 or 1 × 1, as shown in Figure 2 |
| Filter size of max pooling in the main network architecture | 2 × 2 |
| Batch size | 4 |
| Epoch | 100 |
| Learning rate | 0.001, with a decay of 0.5% after each epoch |
| Optimizer | Adam |
| Loss function | L2-norm, as Equation (1) |
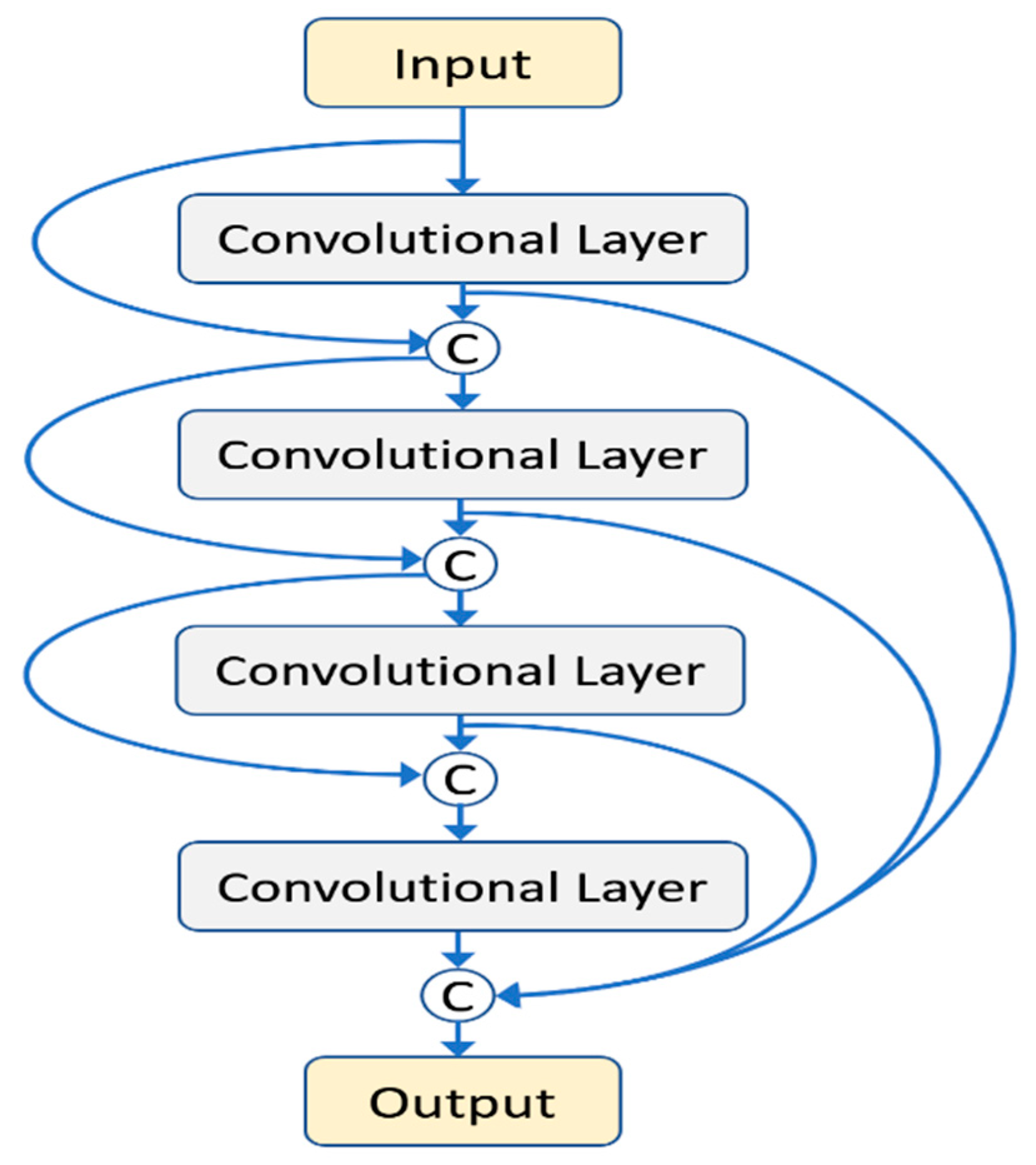
| Layer (l) in the dense block | 5 |
| Growth rate (r) in the dense block | 6 |
| Filter size of convolution in the dense block | 3 × 3 |
| Setting | r | l | DSC Avg. (%) | Training Time (hour/fold) |
|---|---|---|---|---|
| 1 | 5 | 6 | 97.66 ± 1.40 | 7.8 |
| 2 | 6 | 5 | 97.81 ± 1.14 | 6.8 |
| 3 | 6 | 6 | 97.79 ± 1.18 | 8.8 |
| 4 | 6 | 7 | 97.79 ± 1.28 | 10.9 |
| 5 | 7 | 6 | 97.81 ± 1.11 | 9.9 |
References
- Abrams, S.A.; Committee on Nutrition. Calcium and vitamin d requirements of enterally fed preterm infants. Pediatrics 2013, 131, e1676–e1683. [Google Scholar] [CrossRef] [Green Version]
- Faienza, M.F.; D’Amato, E.; Natale, M.P.; Grano, M.; Chiarito, M.; Brunetti, G.; D’Amato, G. Metabolic Bone Disease of Prematurity: Diagnosis and Management. Front. Pediatr. 2019, 7, 143. [Google Scholar] [CrossRef]
- Czech-Kowalska, J.; Czekuc-Kryskiewicz, E.; Pludowski, P.; Zaniuk, K.; Jaworski, M.; Luba, A.; Grzybowska, K.; Pilat, K.; Dobrzanska, A. The Clinical and Biochemical Predictors of Bone Mass in Preterm Infants. PLoS ONE 2016, 11, e0165727. [Google Scholar] [CrossRef] [Green Version]
- Tong, L.; Gopal-Kothandapani, J.S.; Offiah, A.C. Feasibility of quantitative ultrasonography for the detection of metabolic bone disease in preterm infants—Systematic review. Pediatr. Radiol. 2018, 48, 1537–1549. [Google Scholar] [CrossRef] [Green Version]
- Humbert, L.; Whitmarsh, T.; Craene, M.D.; Del Río Barquero, L.M.; Frangi, A.F. Technical note: Comparison between single and multiview simulated DXA configurations for reconstructing the 3D shape and bone mineral density distribution of the proximal femur. Med. Phys. 2012, 39, 5272–5276. [Google Scholar] [CrossRef] [PubMed]
- Dasher, L.G.; Newton, C.D.; Lenchik, L. Dual X-ray absorptiometry in today’s clinical practice. Radiol. Clin. N. Am. 2010, 48, 541–560. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.L.; Tseng, H.I.; Yang, S.N.; Yang, R.C. Bone status and associated factors measured by quantitative ultrasound in preterm and full-term newborn infants. Early Hum. Dev. 2012, 88, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Sotoca, J.M.; Inesta, J.M.; Belmonte, M.A. Hand bone segmentation in radioabsorptiometry images for computerised bone mass assessment. Comput. Med. Imaging Graph 2003, 27, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Rosholm, A.; Hyldstrup, L.; Backsgaard, L.; Grunkin, M.; Thodberg, H.H. Estimation of bone mineral density by digital X-ray radiogrammetry: Theoretical background and clinical testing. Osteoporos. Int. 2001, 12, 961–969. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, J.; Wang, R.; Li, T. Study on medical image segmentation methods of humerus. In Proceedings of the 2017 29th Chinese Control and Decision Conference (CCDC), Chongqing, China, 28–30 May 2017; pp. 7224–7228. [Google Scholar]
- Sapthagirivasan, V.; Anburajan, M. Diagnosis of osteoporosis by extraction of trabecular features from hip radiographs using support vector machine: An investigation panorama with DXA. Comput. Biol. Med. 2013, 43, 1910–1919. [Google Scholar] [CrossRef]
- Hassaballah, M.; Awad, A. Deep Learning in Computer Vision: Principles and Applications; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016; Volume 1. [Google Scholar]
- Arevalo, J.; Cruz-Roa, A.; Arias, V.; Romero, E.; Gonzalez, F.A. An unsupervised feature learning framework for basal cell carcinoma image analysis. Artif. Intell. Med. 2015, 64, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Jia, Z.; Ai, Y.; Zhang, F.; Lai, M.; Chang, E.I. Deep convolutional activation features for large scale Brain Tumor histopathology image classification and segmentation. In Proceedings of the 2015 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), South Brisbane, Australia, 19–24 April 2015; pp. 947–951. [Google Scholar]
- Ibragimov, B.; Xing, L. Segmentation of organs-at-risks in head and neck CT images using convolutional neural networks. Med. Phys. 2017, 44, 547–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cernazanu-Glavan, C.; Holban, S. Segmentation of Bone Structure in X-ray Images using Convolutional Neural Network. Adv. Electr. Comput. Eng. 2013, 13, 87–94. [Google Scholar] [CrossRef]
- Wang, C.; Yan, X.; Smith, M.; Kochhar, K.; Rubin, M.; Warren, S.M.; Wrobel, J.; Lee, H. A unified framework for automatic wound segmentation and analysis with deep convolutional neural networks. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, 25–29 August 2015; pp. 2415–2418. [Google Scholar]
- Al Arif, S.; Knapp, K.; Slabaugh, G. Fully automatic cervical vertebrae segmentation framework for X-ray images. Comput. Methods Programs Biomed. 2018, 157, 95–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, N.; Gou, S.; Yang, S.; Ruan, D.; Sheng, K. Fully automatic multi-organ segmentation for head and neck cancer radiotherapy using shape representation model constrained fully convolutional neural networks. Med. Phys. 2018, 45, 4558–4567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zabihollahy, F.; Schieda, N.; Krishna Jeyaraj, S.; Ukwatta, E. Automated segmentation of prostate zonal anatomy on T2-weighted (T2W) and apparent diffusion coefficient (ADC) map MR images using U-Nets. Med. Phys. 2019, 46, 3078–3090. [Google Scholar] [CrossRef] [PubMed]
- Jégou, S.; Drozdzal, M.; Vázquez, D.; Romero, A.; Bengio, Y. The one hundred layers tiramisu: Fully convolutional DenseNets for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 1175–1183. [Google Scholar]
- Huang, G.; Liu, Z.; Maaten, L.V.D.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar]
- Schneider, A.; Hommel, G.; Blettner, M. Linear regression analysis: Part 14 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2010, 107, 776–782. [Google Scholar] [CrossRef]
- Freeman, H.; Shapira, R. Determining the minimum-area encasing rectangle for an arbitrary closed curve. Commun. ACM 1975, 18, 409–413. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the MICCAI, Munich, Germany, 5–9 October 2015. [Google Scholar]
- Dice, L.R. Measures of the Amount of Ecologic Association Between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Toth, R.; Tiwari, P.; Rosen, M.; Reed, G.; Kurhanewicz, J.; Kalyanpur, A.; Pungavkar, S.; Madabhushi, A. A magnetic resonance spectroscopy driven initialization scheme for active shape model based prostate segmentation. Med. Image Anal. 2011, 15, 214–225. [Google Scholar] [CrossRef] [Green Version]
- Tsukahara, H.; Sudo, M.; Umezaki, M.; Fujii, Y.; Kuriyama, M.; Yamamoto, K.; Ishii, Y. Measurement of lumbar spinal bone mineral density in preterm infants by dual-energy X-ray absorptiometry. Biol. Neonate 1993, 64, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Siddiquee, M.M.R.; Liang, N.T.J. Unet++: A nested u-net architecture for medical image segmentation. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Cham, Switzerland, 2018; pp. 3–11. [Google Scholar]











| k = 1 | k = 2 | k = 3 | k = 4 | k = 5 | Avg. | |
|---|---|---|---|---|---|---|
| This study | 97.65 ± 1.36 | 97.82 ± 1.71 | 97.97 ± 0.71 | 97.90 ± 0.94 | 97.68 ± 0.98 | 97.81 ± 1.14 |
| U-net [26] | 96.51 ± 3.04 | 97.39 ± 2.54 | 97.87 ± 0.66 | 97.25 ± 1.67 | 97.10 ± 1.58 | 97.23 ± 1.90 |
| AE | 95.46 ± 1.88 | 96.28 ± 1.45 | 96.60 ± 0.64 | 95.78 ± 1.78 | 95.14 ± 3.00 | 95.85 ± 1.75 |
| DSC (%) | PPV (%) | SEN (%) | MAD (mm) | HD (mm) | |
|---|---|---|---|---|---|
| This study | 97.81 ± 1.14 | 97.84 ± 1.27 | 97.79 ± 1.41 | 0.12 ± 0.06 | 1.11 ± 1.24 |
| U-net [26] | 97.23 ± 1.90 | 97.42 ± 2.08 | 97.06 ± 2.20 | 0.15 ± 0.10 | 1.51 ± 1.96 |
| AE | 95.85 ± 1.75 | 95.81 ± 2.38 | 95.97 ± 2.24 | 0.23 ± 0.11 | 1.57 ± 1.78 |
| Left Upper Arm | Right Upper Arm | |||||
|---|---|---|---|---|---|---|
| Upper | Middle | Bottom | Upper | Middle | Bottom | |
| Mean | 0.32 | 0.37 | 0.32 | 0.32 | 0.36 | 0.31 |
| S.D. | 0.06 | 0.06 | 0.09 | 0.06 | 0.07 | 0.09 |
| This Study | U-net | AE | |
|---|---|---|---|
| Number of parameters | 258,055 | 31,041,409 | 33,826,689 |
| Training time (h/fold) | 6.8 | 4.2 | 21.5 |
| Testing time per image (s) | 0.30 | 0.23 | 0.23 |
| Case | Region | (1) Estimated BMD without Soft Tissue Correction | (2) Estimated BMD with Soft Tissue Correction | (3) DEXA BMD | Difference between (1) and (3) | Difference between (2) and (3) |
|---|---|---|---|---|---|---|
| Male 1 | Radius 33% | 1.662 | 1.083 | 1.061 | 0.601 | 0.022 |
| Ulna 33% | 1.732 | 1.169 | 1.145 | 0.587 | 0.024 | |
| Radius UD | 1.079 | 0.649 | 0.607 | 0.472 | 0.042 | |
| Ulna UD | 0.945 | 0.535 | 0.471 | 0.474 | 0.064 | |
| Male 2 | Radius 33% | 1.532 | 1.111 | 1.114 | 0.418 | 0.003 |
| Ulna 33% | 1.515 | 1.075 | 1.094 | 0.421 | 0.019 | |
| Radius UD | 0.978 | 0.637 | 0.605 | 0.373 | 0.032 | |
| Ulna UD | 0.871 | 0.504 | 0.492 | 0.379 | 0.012 | |
| Male 3 | Radius 33% | 1.393 | 0.976 | 0.950 | 0.443 | 0.026 |
| Ulna 33% | 1.532 | 1.111 | 0.962 | 0.570 | 0.149 | |
| Radius UD | 0.956 | 0.572 | 0.488 | 0.468 | 0.084 | |
| Ulna UD | 0.876 | 0.504 | 0.417 | 0.459 | 0.087 | |
| Male 4 | Radius 33% | 1.400 | 0.964 | 0.877 | 0.523 | 0.087 |
| Ulna 33% | 1.310 | 0.868 | 0.823 | 0.487 | 0.045 | |
| Radius UD | 0.802 | 0.522 | 0.420 | 0.382 | 0.102 | |
| Ulna UD | 0.765 | 0.424 | 0.345 | 0.420 | 0.079 | |
| Male 5 | Radius 33% | 1.682 | 1.008 | 0.997 | 0.685 | 0.011 |
| Ulna 33% | 1.669 | 1.006 | 0.992 | 0.677 | 0.014 | |
| Radius UD | 1.155 | 0.667 | 0.592 | 0.563 | 0.075 | |
| Ulna UD | 0.987 | 0.525 | 0.422 | 0.565 | 0.103 | |
| Female 1 | Radius 33% | 1.156 | 0.889 | 0.922 | 0.234 | 0.033 |
| Ulna 33% | 1.149 | 0.873 | 0.874 | 0.275 | 0.001 | |
| Radius UD | 0.764 | 0.519 | 0.467 | 0.297 | 0.052 | |
| Ulna UD | 0.687 | 0.439 | 0.327 | 0.360 | 0.112 | |
| Female 2 | Radius 33% | 1.241 | 0.917 | 0.927 | 0.314 | 0.010 |
| Ulna 33% | 1.216 | 0.892 | 0.812 | 0.404 | 0.080 | |
| Radius UD | 0.841 | 0.506 | 0.434 | 0.407 | 0.072 | |
| Ulna UD | 0.742 | 0.416 | 0.344 | 0.398 | 0.072 | |
| Female 3 | Radius 33% | 1.226 | 0.835 | 0.864 | 0.362 | 0.029 |
| Ulna 33% | 1.276 | 0.882 | 0.952 | 0.324 | 0.070 | |
| Radius UD | 0.753 | 0.471 | 0.479 | 0.274 | 0.008 | |
| Ulna UD | 0.698 | 0.421 | 0.406 | 0.292 | 0.015 | |
| Female 4 | Radius 33% | 1.294 | 0.905 | 0.890 | 0.404 | 0.015 |
| Ulna 33% | 1.306 | 0.914 | 0.916 | 0.390 | 0.002 | |
| Radius UD | 0.753 | 0.515 | 0.466 | 0.287 | 0.049 | |
| Ulna UD | 0.702 | 0.404 | 0.331 | 0.371 | 0.073 | |
| Female 5 | Radius 33% | 1.362 | 0.917 | 0.997 | 0.365 | 0.080 |
| Ulna 33% | 1.365 | 0.895 | 0.992 | 0.373 | 0.097 | |
| Radius UD | 0.853 | 0.527 | 0.592 | 0.261 | 0.065 | |
| Ulna UD | 0.722 | 0.396 | 0.422 | 0.300 | 0.026 | |
| Mean: | 0.416 | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-C.; Lin, Y.-C.; Tsai, P.-Y.; Iwata, O.; Chuang, C.-C.; Huang, Y.-H.; Tsai, Y.-S.; Sun, Y.-N. Convolutional Neural Network-Based Humerus Segmentation and Application to Bone Mineral Density Estimation from Chest X-ray Images of Critical Infants. Diagnostics 2020, 10, 1028. https://doi.org/10.3390/diagnostics10121028
Liu Y-C, Lin Y-C, Tsai P-Y, Iwata O, Chuang C-C, Huang Y-H, Tsai Y-S, Sun Y-N. Convolutional Neural Network-Based Humerus Segmentation and Application to Bone Mineral Density Estimation from Chest X-ray Images of Critical Infants. Diagnostics. 2020; 10(12):1028. https://doi.org/10.3390/diagnostics10121028
Chicago/Turabian StyleLiu, Yung-Chun, Yung-Chieh Lin, Pei-Yin Tsai, Osuke Iwata, Chuew-Chuen Chuang, Yu-Han Huang, Yi-Shan Tsai, and Yung-Nien Sun. 2020. "Convolutional Neural Network-Based Humerus Segmentation and Application to Bone Mineral Density Estimation from Chest X-ray Images of Critical Infants" Diagnostics 10, no. 12: 1028. https://doi.org/10.3390/diagnostics10121028