The Use of the Central Vein Sign in the Diagnosis of Multiple Sclerosis: A Systematic Review and Meta-analysis

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search: Databases and Search Phrase
2.2. Eligibility Criteria
2.3. Paper Summary and Data Extraction
- Appears as a thin hypointense line or small hypointense dot;
- Has a small apparent diameter;
- Runs partially or entirely through the lesion;
- Is positioned centrally in the lesion, regardless of the lesion’s shape.
2.4. Statistical Analysis
3. Results
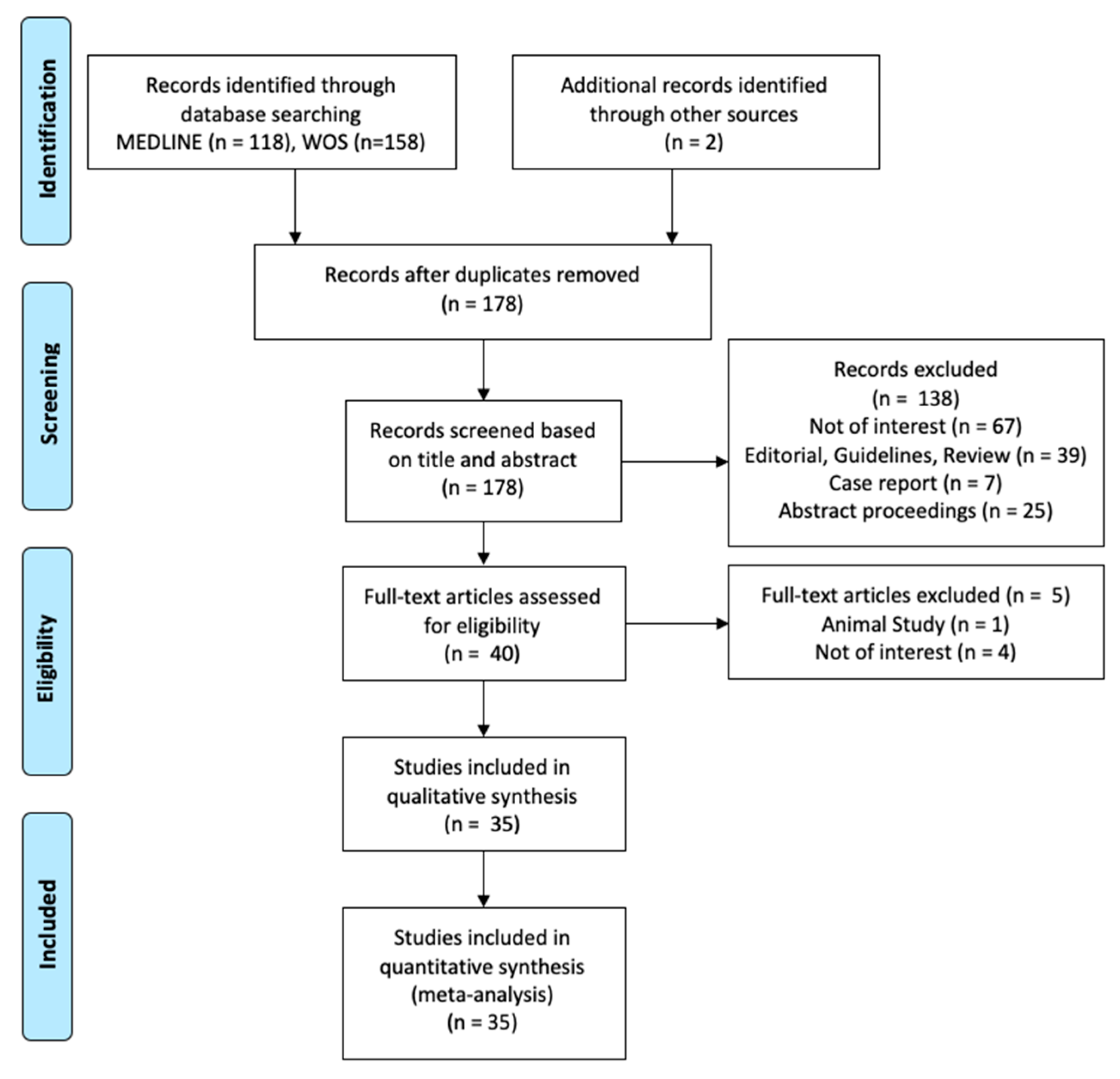
3.1. Literature Review
3.2. Features of the Eligible Studies
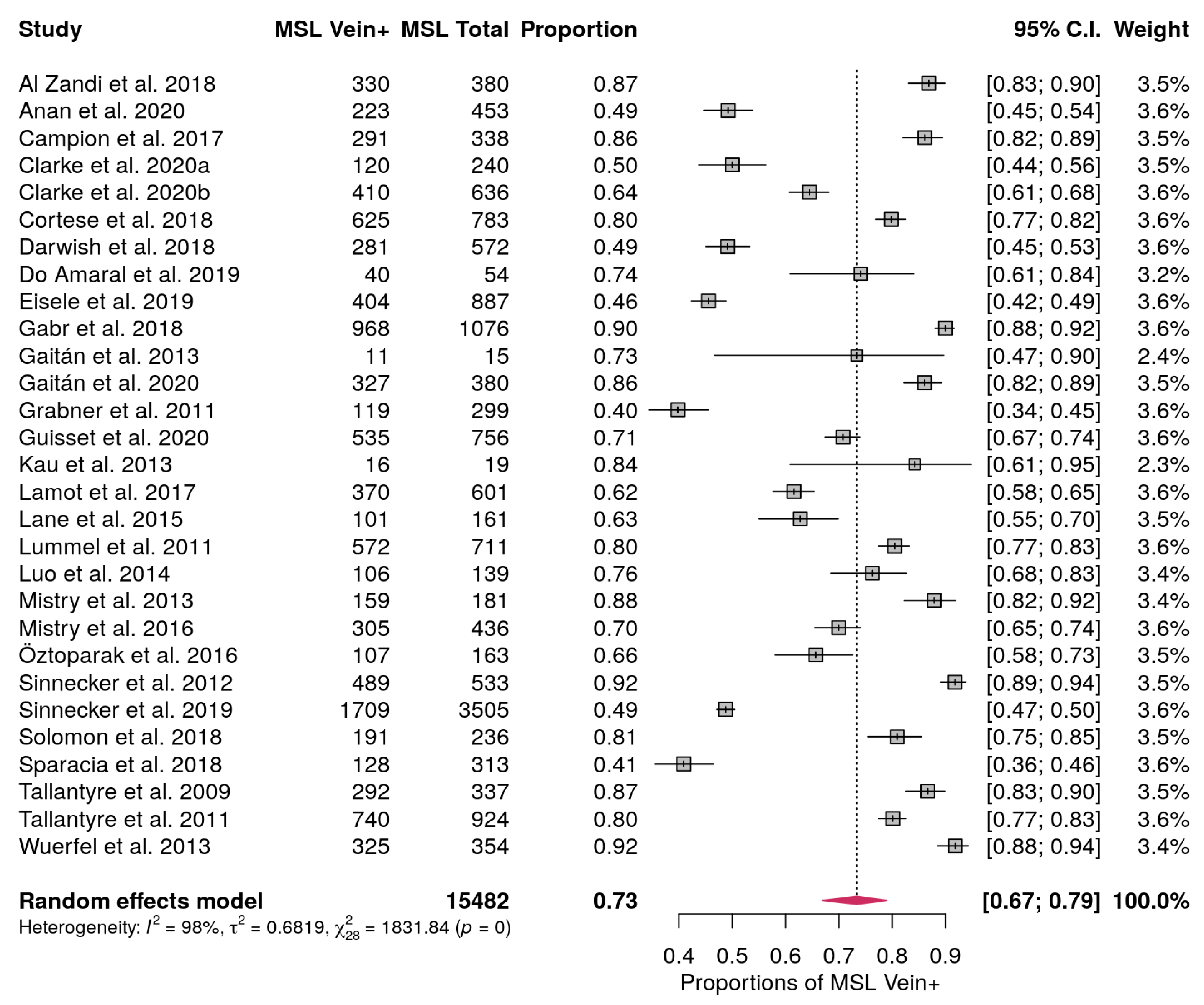
3.3. MS Lesions with Central Vein Pooled Proportion
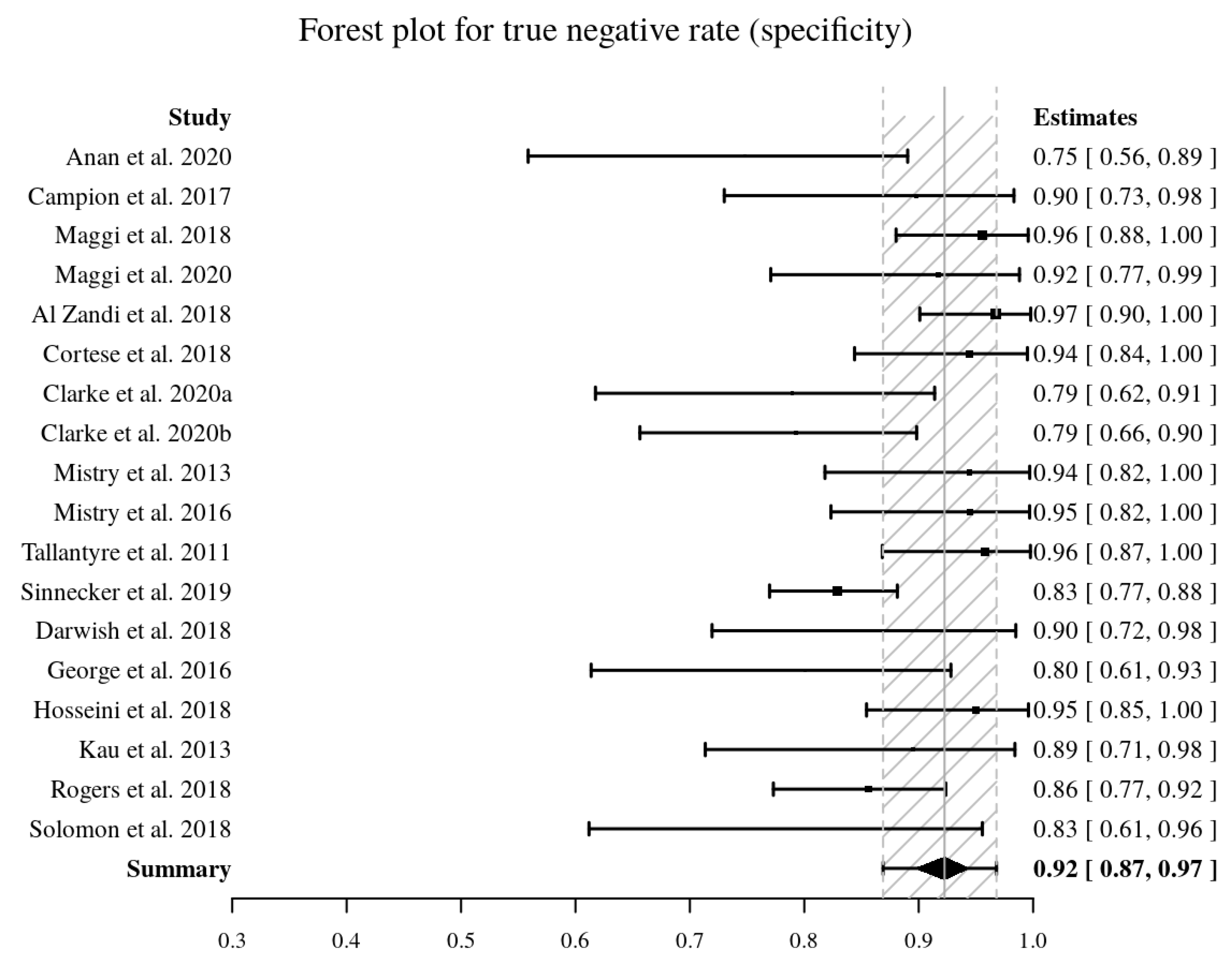
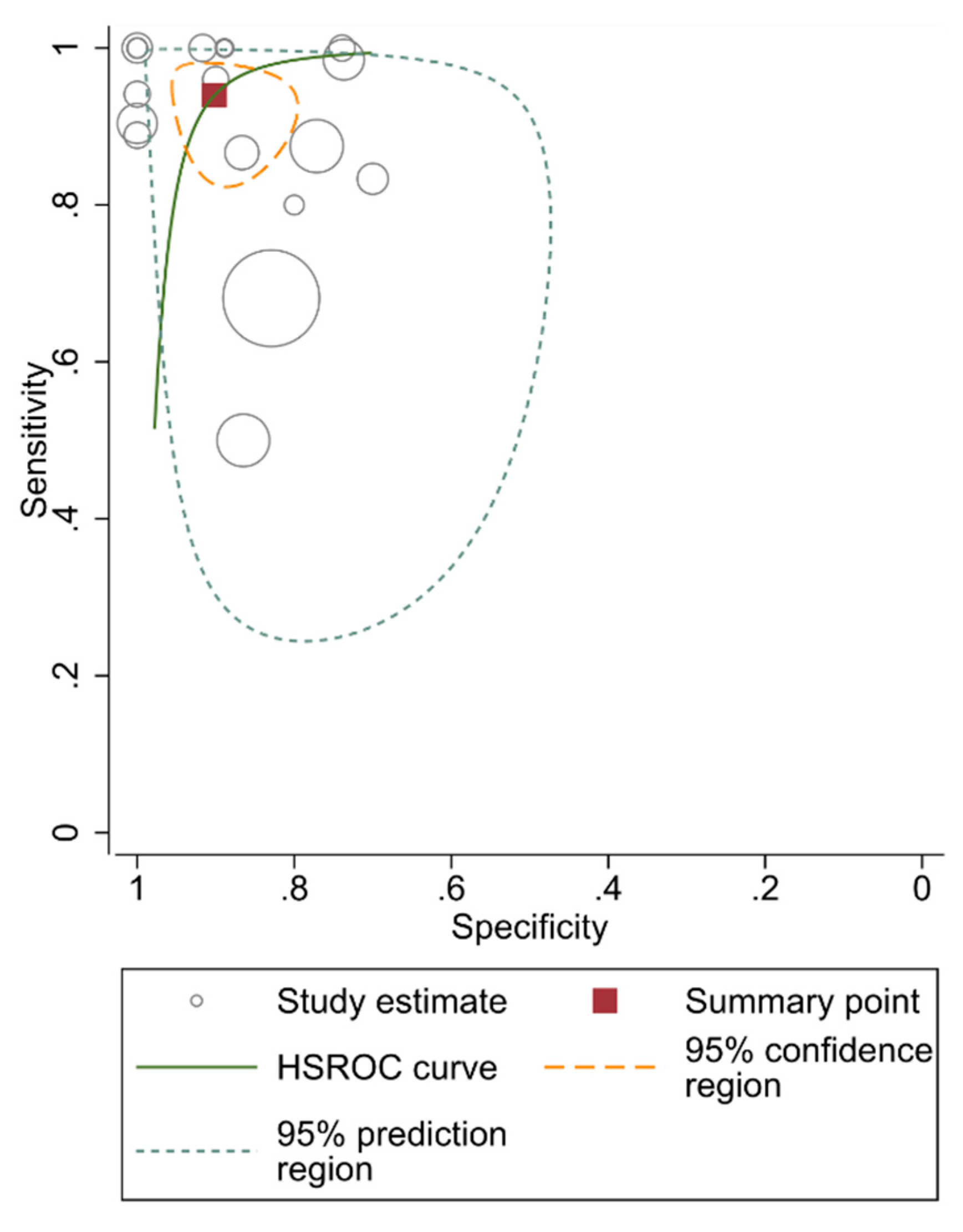
3.4. MS Diagnostic Accuracy Measured by Pooled Sensitivity and Specificity
3.5. Diagnostic Performance using Distinct Patient Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef]
- Schwenkenbecher, P.; Wurster, U.; Konen, F.F.; Gingele, S.; Sühs, K.-W.; Wattjes, M.P.; Stangel, M.; Skripuletz, T. Impact of the mcdonald criteria 2017 on early diagnosis of relapsing-remitting multiple sclerosis. Front. Neurol. 2019, 10, 188. [Google Scholar] [CrossRef] [Green Version]
- Solomon, A.J.; Corboy, J.R. The tension between early diagnosis and misdiagnosis of multiple sclerosis. Nat. Rev. Neurol. 2017, 13, 567–572. [Google Scholar] [CrossRef]
- Calabrese, M.; Gasperini, C.; Tortorella, C.; Schiavi, G.; Frisullo, G.; Ragonese, P.; Fantozzi, R.; Prosperini, L.; Annovazzi, P.; Cordioli, C.; et al. “Better explanations” in multiple sclerosis diagnostic workup: A 3-year longitudinal study. Neurology 2019, 92, e2527–e2537. [Google Scholar] [CrossRef] [Green Version]
- Hammond, K.E.; Metcalf, M.; Carvajal, L.; Okuda, D.T.; Srinivasan, R.; Vigneron, D.; Nelson, S.J.; Pelletier, D. Quantitative in vivo magnetic resonance imaging of multiple sclerosis at 7 Tesla with sensitivity to iron. Ann. Neurol. 2008, 64, 707–713. [Google Scholar] [CrossRef]
- Tallantyre, E.C.; Brookes, M.J.; Dixon, J.E.; Morgan, P.S.; Evangelou, N.; Morris, P.G. Demonstrating the perivascular distribution of ms lesions in vivo with 7-tesla mri. Neurology 2008, 70, 2076–2078. [Google Scholar] [CrossRef]
- Lassmann, H. Multiple sclerosis pathology: Evolution of pathogenetic concepts. Brain Pathol. 2006, 15, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Sati, P.; Oh, J.; Constable, R.T.; Evangelou, N.; Guttmann, C.R.G.; Henry, R.G.; Klawiter, E.C.; Mainero, C.; Massacesi, L.; McFarland, H.; et al. The central vein sign and its clinical evaluation for the diagnosis of multiple sclerosis: A consensus statement from the North American imaging in multiple sclerosis cooperative. Nat. Rev. Neurol. 2016, 12, 714–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggi, P.; Absinta, M.; Grammatico, M.; Vuolo, L.; Emmi, G.; Carlucci, G.; Spagni, G.; Barilaro, A.; Repice, A.M.; Emmi, L.; et al. Central vein sign differentiates Multiple Sclerosis from central nervous system inflammatory vasculopathies. Ann. Neurol. 2018, 83, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Tallantyre, E.C.; Dixon, J.E.; Donaldson, I.; Owens, T.; Morgan, P.S.; Morris, P.G.; Evangelou, N. Ultra-high-field imaging distinguishes MS lesions from asymptomatic white matter lesions. Neurology 2011, 76, 534–539. [Google Scholar] [CrossRef]
- Mistry, N.; Abdel-Fahim, R.; Samaraweera, A.; Mougin, O.; Tallantyre, E.; Tench, C.; Jaspan, T.; Morris, P.; Morgan, P.S.; Evangelou, N. Imaging central veins in brain lesions with 3-T T2*-weighted magnetic resonance imaging differentiates multiple sclerosis from microangiopathic brain lesions. Mult. Scler. J. 2016, 22, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.J.; Watts, R.; Ontaneda, D.; Absinta, M.; Sati, P.; Reich, D.S. Diagnostic performance of central vein sign for multiple sclerosis with a simplified three-lesion algorithm. Mult. Scler. Houndmills Basingstoke Engl. 2018, 24, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Reichenbach, J.R.; Venkatesan, R.; Schillinger, D.J.; Kido, D.K.; Haacke, E.M. Small vessels in the human brain: MR venography with deoxyhemoglobin as an intrinsic contrast agent. Radiology 1997, 204, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Haacke, E.M.; Mittal, S.; Wu, Z.; Neelavalli, J.; Cheng, Y.-C.N. Susceptibility-weighted imaging: Technical aspects and clinical applications, part 1. Am. J. Neuroradiol. 2009, 30, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Mittal, S.; Wu, Z.; Neelavalli, J.; Haacke, E.M. Susceptibility-weighted imaging: Technical aspects and clinical applications, part 2. AJNR Am. J. Neuroradiol. 2009, 30, 232–252. [Google Scholar] [CrossRef] [Green Version]
- Sati, P.; Thomasson, D.; Li, N.; Pham, D.; Biassou, N.; Reich, D.; Butman, J. Rapid, high-resolution, whole-brain, susceptibility-based MRI of multiple sclerosis. Mult. Scler. J. 2014, 20, 1464–1470. [Google Scholar] [CrossRef]
- Li, N.; Wang, W.-T.; Sati, P.; Pham, D.L.; Butman, J.A. Quantitative assessment of susceptibility weighted imaging processing methods. J. Magn. Reson. Imaging JMRI 2014, 40, 1463–1473. [Google Scholar] [CrossRef] [Green Version]
- Sati, P.; George, I.C.; Shea, C.D.; Gaitán, M.I.; Reich, D.S. FLAIR*: A combined MR contrast technique for visualizing white matter lesions and parenchymal veins. Radiology 2012, 265, 926–932. [Google Scholar] [CrossRef]
- Frank, R.A.; Bossuyt, P.M.; McInnes, M.D.F. Systematic reviews and meta-analyses of diagnostic test accuracy: The PRISMA-DTA statement. Radiology 2018, 289, 313–314. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; PRISMA-DTA Group; et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The prisma-dta statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Suh, C.H.; Kim, S.J.; Jung, S.C.; Choi, C.G.; Kim, H.S. The “Central Vein Sign” on T2*-weighted Images as a Diagnostic Tool in Multiple Sclerosis: A Systematic Review and Meta-analysis using Individual Patient Data. Sci. Rep. 2019, 9, 18188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandari, A.; Xiang, H.; Lechner-Scott, J.; Agzarian, M. Central vein sign for multiple sclerosis: A systematic review and meta-analysis. Clin. Radiol. 2020, 75, 479.e9–479.e15. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Williams, D.A. Generalized linear model diagnostics using the deviance and single case deletions. Appl. Stat. 1987, 36, 181. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Anan, R.A.; El-Adalany, M.A.; Belal, T.M.I.; Elmogy, S.A.E.-D. Detection of central veins using susceptibility weighted imaging (SWI) for discrimination between lesions in multiple sclerosis (MS) and cerebral small vessel disease (CSVD). Egypt. J. Radiol. Nucl. Med. 2020, 51, 1–7. [Google Scholar] [CrossRef]
- Campion, T.; Smith, R.J.P.; Altmann, D.R.; Brito, G.C.; Turner, B.P.; Evanson, J.; George, I.C.; Sati, P.; Reich, D.S.; Miquel, M.E.; et al. FLAIR* to visualize veins in white matter lesions: A new tool for the diagnosis of multiple sclerosis? Eur. Radiol. 2017, 27, 4257–4263. [Google Scholar] [CrossRef] [Green Version]
- Gabr, R.E.; Pednekar, A.S.; Kamali, A.; Lincoln, J.A.; Nelson, F.M.; Wolinsky, J.S.; Narayana, P.A. Interleaved susceptibility-weighted and FLAIR MRI for imaging lesion-penetrating veins in multiple sclerosis. Magn. Reson. Med. 2018, 80, 1132–1137. [Google Scholar] [CrossRef]
- Gaitán, M.I.; Yañez, P.; Paday Formenti, M.E.; Calandri, I.; Figueiredo, E.; Sati, P.; Correale, J. SWAN-venule: An optimized mri technique to detect the central vein sign in ms plaques. AJNR Am. J. Neuroradiol. 2020, 41, 456–460. [Google Scholar] [CrossRef]
- Maggi, P.; Absinta, M.; Sati, P.; Perrotta, G.; Massacesi, L.; Dachy, B.; Pot, C.; Meuli, R.; Reich, D.S.; Filippi, M.; et al. The “central vein sign” in patients with diagnostic “red flags” for multiple sclerosis: A prospective multicenter 3T study. Mult. Scler. Houndmills Basingstoke Engl. 2020, 26, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Cortese, R.; Magnollay, L.; Tur, C.; Abdel-Aziz, K.; Jacob, A.; De Angelis, F.; Yiannakas, M.C.; Prados, F.; Ourselin, S.; Yousry, T.A.; et al. Value of the central vein sign at 3T to differentiate MS from seropositive NMOSD. Neurology 2018, 90, e1183–e1190. [Google Scholar] [CrossRef] [Green Version]
- Clarke, M.A.; Samaraweera, A.P.; Falah, Y.; Pitiot, A.; Allen, C.M.; Dineen, R.A.; Tench, C.R.; Morgan, P.S.; Evangelou, N. Single Test to ARrive at Multiple Sclerosis (STAR-MS) diagnosis: A prospective pilot study assessing the accuracy of the central vein sign in predicting multiple sclerosis in cases of diagnostic uncertainty. Mult. Scler. Houndmills Basingstoke Engl. 2020, 26, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Mistry, N.; Dixon, J.; Tallantyre, E.; Tench, C.; Abdel-Fahim, R.; Jaspan, T.; Morgan, P.S.; Morris, P.; Evangelou, N. Central veins in brain lesions visualized with high-field magnetic resonance imaging: A pathologically specific diagnostic biomarker for inflammatory demyelination in the brain. JAMA Neurol. 2013, 70, 623–628. [Google Scholar] [CrossRef]
- Kau, T.; Taschwer, M.; Deutschmann, H.; Schönfelder, M.; Weber, J.R.; Hausegger, K.A. The “central vein sign”: Is there a place for susceptibility weighted imaging in possible multiple sclerosis? Eur. Radiol. 2013, 23, 1956–1962. [Google Scholar] [CrossRef] [PubMed]
- Guisset, F.; Lolli, V.; Bugli, C.; Perrotta, G.; Absil, J.; Dachy, B.; Pot, C.; Théaudin, M.; Pasi, M.; van Pesch, V.; et al. The central vein sign in multiple sclerosis patients with vascular comorbidities. Mult. Scler. J. 2020, 135245852094378. [Google Scholar] [CrossRef] [PubMed]
- Lamot, U.; Avsenik, J.; Šega, S.; Šurlan Popovič, K. Presence of central veins and susceptibility weighted imaging for evaluating lesions in multiple sclerosis and leukoaraiosis. Mult. Scler. Relat. Disord. 2017, 13, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Sparacia, G.; Agnello, F.; Gambino, A.; Sciortino, M.; Midiri, M. Multiple sclerosis: High prevalence of the “central vein” sign in white matter lesions on susceptibility-weighted images. Neuroradiol. J. 2018, 31, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Do Amaral, L.L.F.; Fragoso, D.C.; Nunes, R.H.; Littig, I.A.; da Rocha, A.J. gadolinium-enhanced susceptibility-weighted imaging in multiple sclerosis: Optimizing the recognition of active plaques for different mr imaging sequences. AJNR Am. J. Neuroradiol. 2019, 40, 614–619. [Google Scholar] [CrossRef]
- Eisele, P.; Fischer, K.; Szabo, K.; Platten, M.; Gass, A. Characterization of contrast-enhancing and non-contrast-enhancing multiple sclerosis lesions using susceptibility-weighted imaging. Front. Neurol. 2019, 10, 1082. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, Z.; Matusinec, J.; Rudko, D.A.; Liu, J.; Kwan, B.Y.M.; Salehi, F.; Sharma, M.; Kremenchutzky, M.; Menon, R.S.; Drangova, M. Morphology-specific discrimination between ms white matter lesions and benign white matter hyperintensities using ultra-high-field mri. AJNR Am. J. Neuroradiol. 2018, 39, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.I.; Bolster, B.; Campeau, N.G.; Welker, K.M.; Gilbertson, J.R. Characterization of multiple sclerosis plaques using susceptibility-weighted imaging at 1.5 T: Can perivenular localization improve specificity of imaging criteria? J. Comput. Assist. Tomogr. 2015, 39, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Öztoprak, B.; Öztoprak, I.; Yıldız, Ö.K. The effect of venous anatomy on the morphology of multiple sclerosis lesions: A susceptibility-weighted imaging study. Clin. Radiol. 2016, 71, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Rogers, D.M.; Shah, L.M.; Wiggins, R.H. 3rd the central vein: Flair signal abnormalities associated with developmental venous anomalies in patients with multiple sclerosis. AJNR Am. J. Neuroradiol. 2018, 39, 2007–2013. [Google Scholar] [CrossRef]
- Gaitán, M.I.; Sati, P.; Inati, S.J.; Reich, D.S. Initial investigation of the blood-brain barrier in MS lesions at 7 tesla. Mult. Scler. Houndmills Basingstoke Engl. 2013, 19, 1068–1073. [Google Scholar] [CrossRef] [Green Version]
- Samaraweera, A.P.R.; Falah, Y.; Pitiot, A.; Dineen, R.A.; Morgan, P.S.; Evangelou, N. The MRI central vein marker; differentiating PPMS from RRMS and ischemic SVD. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5. [Google Scholar] [CrossRef] [Green Version]
- Al-Zandi, S.H.; Fayadh, N.A.H.; Al-Waely, N.K.N. Central vein sign detected by SWI at 3 T MRI as a discriminator between multiple sclerosis and leukoaraiosis. Egypt. J. Radiol. Nucl. Med. 2018, 49, 158–164. [Google Scholar] [CrossRef]
- Clarke, M.A.; Pareto, D.; Pessini-Ferreira, L.; Arrambide, G.; Alberich, M.; Crescenzo, F.; Cappelle, S.; Tintoré, M.; Sastre-Garriga, J.; Auger, C.; et al. Value of 3T Susceptibility-Weighted Imaging in the Diagnosis of Multiple Sclerosis. AJNR Am. J. Neuroradiol. 2020. [Google Scholar] [CrossRef]
- Tallantyre, E.C.; Morgan, P.S.; Dixon, J.E.; Al-Radaideh, A.; Brookes, M.J.; Evangelou, N.; Morris, P.G. A comparison of 3T and 7T in the detection of small parenchymal veins within MS lesions. Investig. Radiol. 2009, 44, 491–494. [Google Scholar] [CrossRef] [Green Version]
- Wuerfel, J.; Sinnecker, T.; Ringelstein, E.B.; Jarius, S.; Schwindt, W.; Niendorf, T.; Paul, F.; Kleffner, I.; Dörr, J. Lesion morphology at 7 Tesla MRI differentiates Susac syndrome from multiple sclerosis. Mult. Scler. Houndmills Basingstoke Engl. 2012, 18, 1592–1599. [Google Scholar] [CrossRef]
- Sinnecker, T.; Clarke, M.A.; Meier, D.; Enzinger, C.; Calabrese, M.; De Stefano, N.; Pitiot, A.; Giorgio, A.; Schoonheim, M.M.; Paul, F.; et al. Evaluation of the central vein sign as a diagnostic imaging biomarker in multiple sclerosis. JAMA Neurol. 2019, 76. [Google Scholar] [CrossRef] [PubMed]
- Darwish, E.A.F.; Ibrahim, Y.A.; Zamzam, D.A. Value of central vein sign in discriminating multiple sclerosis plaques from other white matter lesions. Egypt. J. Radiol. Nucl. Med. 2018, 49, 165–171. [Google Scholar] [CrossRef]
- George, I.C.; Sati, P.; Absinta, M.; Cortese, I.C.; Sweeney, E.M.; Shea, C.D.; Reich, D.S. Clinical 3-tesla FLAIR* MRI improves diagnostic accuracy in multiple sclerosis. Mult. Scler. Houndmills Basingstoke Engl. 2016, 22, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Lummel, N.; Boeckh-Behrens, T.; Schoepf, V.; Burke, M.; Brückmann, H.; Linn, J. Presence of a central vein within white matter lesions on susceptibility weighted imaging: A specific finding for multiple sclerosis? Neuroradiology 2011, 53, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Yablonskiy, D.A.; Hildebolt, C.F.; Lancia, S.; Cross, A.H. Gradient echo magnetic resonance imaging correlates with clinical measures and allows visualization of veins within multiple sclerosis lesions. Mult. Scler. Houndmills Basingstoke Engl. 2014, 20, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Grabner, G.; Dal-Bianco, A.; Schernthaner, M.; Vass, K.; Lassmann, H.; Trattnig, S. Analysis of multiple sclerosis lesions using a fusion of 3.0 T FLAIR and 7.0 T SWI phase: FLAIR SWI. J. Magn. Reson. Imaging 2011, 33, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Samaraweera, A.P.R.; Clarke, M.A.; Whitehead, A.; Falah, Y.; Driver, I.D.; Dineen, R.A.; Morgan, P.S.; Evangelou, N. The central vein sign in multiple sclerosis lesions is present irrespective of the T2* sequence at 3 T. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2017, 27, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Sinnecker, T.; Dörr, J.; Pfueller, C.F.; Harms, L.; Ruprecht, K.; Jarius, S.; Brück, W.; Niendorf, T.; Wuerfel, J.; Paul, F. Distinct lesion morphology at 7-T MRI differentiates neuromyelitis optica from multiple sclerosis. Neurology 2012, 79, 708–714. [Google Scholar] [CrossRef]
- Gaitán, M.I.; de Alwis, M.P.; Sati, P.; Nair, G.; Reich, D.S. Multiple sclerosis shrinks intralesional, and enlarges extralesional, brain parenchymal veins. Neurology 2013, 80, 145–151. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Hickey, W.F. The pathology of multiple sclerosis: A historical perspective1Supported in part by award NS 27321.1. J. Neuroimmunol. 1999, 98, 37–44. [Google Scholar] [CrossRef]
- Liu, S.; Kullnat, J.; Bourdette, D.; Simon, J.; Kraemer, D.F.; Murchison, C.; Hamilton, B.E. Prevalence of brain magnetic resonance imaging meeting Barkhof and McDonald criteria for dissemination in space among headache patients. Mult. Scler. J. 2013, 19, 1101–1105. [Google Scholar] [CrossRef] [PubMed]
- Dal-Bianco, A.; Hametner, S.; Grabner, G.; Schernthaner, M.; Kronnerwetter, C.; Reitner, A.; Vass, C.; Kircher, K.; Auff, E.; Leutmezer, F.; et al. Veins in plaques of multiple sclerosis patients—A longitudinal magnetic resonance imaging study at 7 Tesla. Eur. Radiol. 2015, 25, 2913–2920. [Google Scholar] [CrossRef] [PubMed]
- Maggi, P.; Fartaria, M.J.; Jorge, J.; La Rosa, F.; Absinta, M.; Sati, P.; Meuli, R.; Du Pasquier, R.; Reich, D.S.; Cuadra, M.B.; et al. CVSnet: A machine learning approach for automated central vein sign assessment in multiple sclerosis. NMR Biomed. 2020, 33, e4283. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, J.D.; Sati, P.; Solomon, A.; Pham, D.L.; Watts, R.; Martin, M.L.; Ontaneda, D.; Schindler, M.K.; Reich, D.S.; Shinohara, R.T. Automated integration of multimodal mri for the probabilistic detection of the central vein sign in white matter lesions. AJNR Am. J. Neuroradiol. 2018, 39, 1806–1813. [Google Scholar] [CrossRef]
- Raz, E.; Pontecorvo, S.; Barra, V.; Marincola, B.C.; Morreale, M.; Tinelli, E.; Saba, L.; Di Paolo, P.L.; Aceti, A.; Catalano, C.; et al. MR venography in patients with multiple sclerosis and correlation with clinical and MRI parameters. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2014, 24, 492–497. [Google Scholar] [CrossRef]
- Maggi, P.; Mazzoni, L.N.; Moretti, M.; Grammatico, M.; Chiti, S.; Massacesi, L. SWI enhances vein detection using gadolinium in multiple sclerosis. Acta Radiol. Open 2015, 4, 2047981614560938. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellaro, M.; Tamanti, A.; Pisani, A.I.; Pizzini, F.B.; Crescenzo, F.; Calabrese, M. The Use of the Central Vein Sign in the Diagnosis of Multiple Sclerosis: A Systematic Review and Meta-analysis. Diagnostics 2020, 10, 1025. https://doi.org/10.3390/diagnostics10121025
Castellaro M, Tamanti A, Pisani AI, Pizzini FB, Crescenzo F, Calabrese M. The Use of the Central Vein Sign in the Diagnosis of Multiple Sclerosis: A Systematic Review and Meta-analysis. Diagnostics. 2020; 10(12):1025. https://doi.org/10.3390/diagnostics10121025
Chicago/Turabian StyleCastellaro, Marco, Agnese Tamanti, Anna Isabella Pisani, Francesca Benedetta Pizzini, Francesco Crescenzo, and Massimiliano Calabrese. 2020. "The Use of the Central Vein Sign in the Diagnosis of Multiple Sclerosis: A Systematic Review and Meta-analysis" Diagnostics 10, no. 12: 1025. https://doi.org/10.3390/diagnostics10121025