Diagnostic Balance Tests for Assessing Risk of Falls and Distinguishing Older Adult Fallers and Non-Fallers: A Systematic Review with Meta-Analysis


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Population (P): Male or female older adults. The criterion for inclusion was mean sample age ≥ 60.0 years. The study had to include either two groups (fallers and non-fallers) or a single cohort that was prospectively tracked for falls.
- Intervention (I): No allocated intervention.
- Comparisons (C): Fallers and non-fallers were compared.
- Outcomes (O): Any tests assessing balance ability, either instrumented (body sway assessment through CoP analysis using force plates or other technology) or non-instrumented (Romberg test, functional reach test, star excursion balance test, stance time in different postures, etc.)
- Study design (S): Prospective and retrospective cohort studies or case-control studies.
2.2. Search Strategy
2.3. Data Extraction
2.4. Data Analysis and Synthesis
3. Results
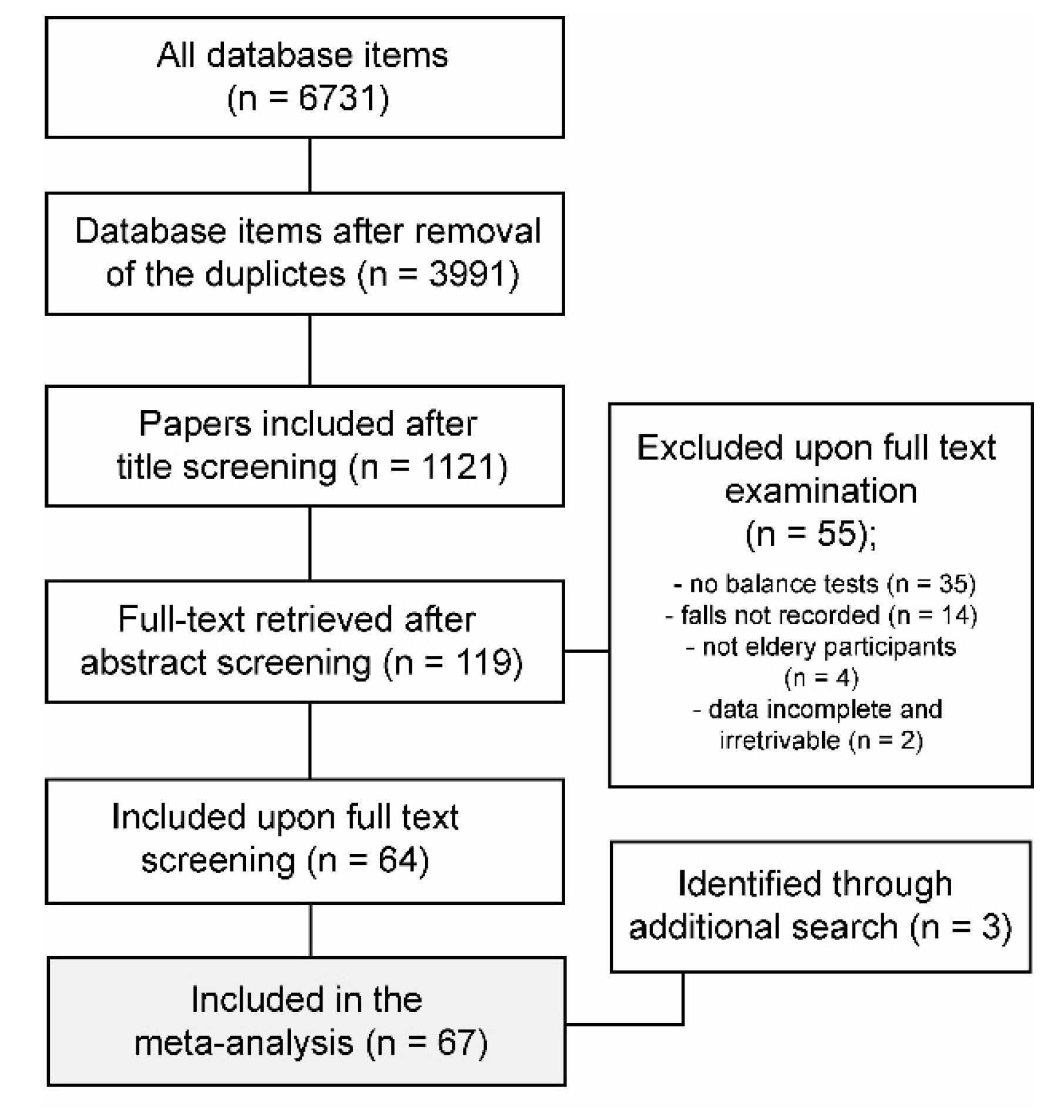
3.1. Summary of Search Results and Characteristics of Included Studies
3.2. Discrimination of Fallers and Non-Fallers with Balance Tests
3.3. Fall Risk Associated with Outcomes of Balance Tests
3.4. Sensitivity and Specificity of Balance Tests to Detect Fallers
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cuevas-Trisan, R. Balance Problems and Fall Risks in the Elderly. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Luk, J.K.H.; Chan, T.Y.; Chan, D.K.Y. Falls prevention in the elderly: Translating evidence into practice. Hong Kong Med. J. 2015, 21, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of interventions for preventing falls in older adults: A systematic review and meta-analysis. JAMA-J. Am. Med. Assoc. 2017, 318, 1687–1699. [Google Scholar] [CrossRef]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: A systematic review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [Green Version]
- Aranda-Gallardo, M.; Morales-Asencio, J.M.; Canca-Sanchez, J.C.; Barrero-Sojo, S.; Perez-Jimenez, C.; Morales-Fernandez, A.; De Luna-Rodriguez, M.E.; Moya-Suarez, A.B.; Mora-Banderas, A.M. Instruments for assessing the risk of falls in acute hospitalized patients: A systematic review and meta-analysis. BMC Health Serv. Res. 2013, 13, 122. [Google Scholar] [CrossRef] [Green Version]
- Park, S.H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Park, S.H.; Lee, Y.S. The Diagnostic Accuracy of the Berg Balance Scale in Predicting Falls. West. J. Nurs. Res. 2017, 39, 1502–1525. [Google Scholar] [CrossRef]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: A systematic review and meta-analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef]
- Hou, W.H.; Kang, C.M.; Ho, M.H.; Kuo, J.M.C.; Chen, H.L.; Chang, W.Y. Evaluation of an inpatient fall risk screening tool to identify the most critical fall risk factors in inpatients. J. Clin. Nurs. 2017, 26, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Poe, S.S.; Dawson, P.B.; Cvach, M.; Burnett, M.; Kumble, S.; Lewis, M.; Thompson, C.B.; Hill, E.E. The Johns Hopkins Fall Risk Assessment Tool: A Study of Reliability and Validity. J. Nurs. Care Qual. 2018, 33, 10–19. [Google Scholar] [CrossRef]
- Sarabon, N.; Löfler, S.; Hosszu, G.; Hofer, C. Mobility test protocols for the elderly: A methodological note. Eur. J. Transl. Myol. 2015, 25, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goble, D.J.; Baweja, H.S. Postural sway normative data across the adult lifespan: Results from 6280 individuals on the Balance Tracking System balance test. Geriatr. Gerontol. Int. 2018, 18, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Demura, S.I.; Kitabayashi, T.; Aoki, H. Body-sway characteristics during a static upright posture in the elderly. Geriatr. Gerontol. Int. 2008, 8, 188–197. [Google Scholar] [CrossRef]
- Kitabayashi, T.; Demura, S.I.; Kawabata, H.; Uchiyama, M.; Demura, T. Comparison of the body-sway characteristics of young adults compared to healthy elderly and elderly with equilibrium disorder. Percept. Mot. Skills 2011, 113, 547–556. [Google Scholar] [CrossRef]
- Morrison, S.; Colberg, S.R.; Parson, H.K.; Vinik, A.I. Relation between risk of falling and postural sway complexity in diabetes. Gait Posture 2012, 35, 662–668. [Google Scholar] [CrossRef]
- Frames, C.W.; Soangra, R.; Lockhart, T.E.; Lach, J.; Ha, D.S.; Roberto, K.A.; Lieberman, A. Dynamical properties of postural control in obese community-dwelling older adults. Sensors 2018, 18, 1692. [Google Scholar] [CrossRef] [Green Version]
- Mignardot, J.-B.; Beauchet, O.; Annweiler, C.; Cornu, C.; Deschamps, T. Postural sway, falls, and cognitive status: A cross-sectional study among older adults. J. Alzheimers. Dis. 2014, 41, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Behrman, A.L.; Light, K.E.; Flynn, S.M.; Thigpen, M.T. Is the functional reach test useful for identifying falls risk among individuals with Parkinson’s disease? Arch. Phys. Med. Rehabil. 2002, 83, 538–542. [Google Scholar] [CrossRef] [Green Version]
- Cho, C.Y.; Kamen, G. Detecting balance deficits in frequent fallers using clinical and quantitative evaluation tools. J. Am. Geriatr. Soc. 1998, 46, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Gerdhem, P.; Ringsberg, K.A.M.; Åkesson, K.; Obrant, K.J. Clinical history and biologic age predicted falls better than objective functional tests. J. Clin. Epidemiol. 2005, 58, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.J.; Chang, Y.S.; Yang, S.W. Using single leg standing time to predict the fall risk in elderly. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Osaka, Japan, 3–7 July 2013; pp. 7456–7458. [Google Scholar]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions | Cochrane Training. Available online: https://training.cochrane.org/handbook/current (accessed on 15 May 2020).
- Aoyama, M.; Suzuki, Y.; Onishi, J.; Kuzuya, M. Physical and functional factors in activities of daily living that predict falls in community-dwelling older women. Geriatr. Gerontol. Int. 2011, 11, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Kwok, B.C.; Clark, R.A.; Pua, Y.H. Novel use of the Wii Balance Board to prospectively predict falls in community-dwelling older adults. Clin. Biomech. 2015, 30, 481–484. [Google Scholar] [CrossRef]
- Lin, M.R.; Hwang, H.F.; Hu, M.H.; Wu, H.D.I.; Wang, Y.W.; Huang, F.C. Psychometric comparisons of the timed up and go, one-leg stand, functional reach, and Tinetti balance measures in community-dwelling older people. J. Am. Geriatr. Soc. 2004, 52, 1343–1348. [Google Scholar] [CrossRef]
- Lord, S.R.; Clark, R.D.; Webster, I.W. Physiological Factors Associated with Falls in an Elderly Population. J. Am. Geriatr. Soc. 1991, 39, 1194–1200. [Google Scholar] [CrossRef]
- Maki, B.E.; Holliday, P.J.; Topper, A.K. A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J. Gerontol. 1994, 49, M72–M84. [Google Scholar] [CrossRef]
- Panzer, V.P.; Wakefield, D.B.; Hall, C.B.; Wolfson, L.I. Mobility assessment: Sensitivity and specificity of measurement sets in older adults. Arch. Phys. Med. Rehabil. 2011, 92, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Lord, S.R.; Close, J.C.T.; Barraclough, E.; Taylor, M.; O’Rourke, S.; Kurrle, S.; Tiedemann, A.; Cumming, R.G.; Herbert, R.D. Development of a tool for prediction of falls in rehabilitation settings (predict-first): A Prospective cohort study. J. Rehabil. Med. 2010, 42, 482–488. [Google Scholar] [CrossRef] [Green Version]
- Shimada, H.; Suzukawa, M.; Tiedemann, A.; Kobayashi, K.; Yoshida, H.; Suzuki, T. Which neuromuscular or cognitive test is the optimal screening tool to predict falls in frail community-dwelling older people? Gerontology 2009, 55, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Thapa, P.B.; Gideon, P.; Brockman, K.G.; Fought, R.L.; Ray, W.A. Clinical and biomechanical measures of balance as fall predictors in ambulatory nursing home residents. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 1996, 51, M239–M246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, M.; Ichihashi, N. Predicting the probability of falls in community-dwelling elderly individuals using the trail-walking test. Environ. Health Prev. Med. 2010, 15, 386–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buatois, S.; Gueguen, R.; Gauchard, G.C.; Benetos, A.; Perrin, P.P. Posturography and risk of recurrent falls in healthy non-institutionalized persons aged over. Gerontology 2006, 52, 345–352. [Google Scholar] [CrossRef]
- Davis, J.W.; Ross, P.D.; Nevitt, M.C.; Wasnich, R.D. Risk factors for falls and for serious injuries on falling among older Japanese women in Hawaii. J. Am. Geriatr. Soc. 1999, 47, 792–798. [Google Scholar] [CrossRef]
- Delbaere, K.; Van den Noortgate, N.; Bourgois, J.; Vanderstraeten, G.; Tine, W.; Cambier, D. The physical performance test as a predictor of frequent fallers: A prospective community-based cohort study. Clin. Rehabil. 2006, 20, 83–90. [Google Scholar] [CrossRef]
- Duncan, P.W.; Studenski, S.; Chandler, J.; Prescott, B. Functional reach: Predictive validity in a sample of elderly male veterans. J. Gerontol. 1992, 47, M93–M98. [Google Scholar] [CrossRef]
- Haines, T.; Kuys, S.S.; Morrison, G.; Clarke, J.; Bew, P. Balance impairment not predictive of falls in geriatric rehabilitation wards. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2008, 63, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Howcroft, J.; Lemaire, E.D.; Kofman, J.; McIlroy, W.E. Elderly fall risk prediction using static posturography. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Johansson, J.; Nordström, A.; Gustafson, Y.; Westling, G.; Nordström, P. Increased postural sway during quiet stance as a risk factor for prospective falls in community-dwelling elderly individuals. Age Ageing 2017, 46, 964–970. [Google Scholar] [CrossRef] [Green Version]
- Johansson, J.; Jarocka, E.; Westling, G.; Nordström, A.; Nordström, P. Predicting incident falls: Relationship between postural sway and limits of stability in older adults. Hum. Mov. Sci. 2019, 66, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Daubney, M.E.; Culham, E.G. Lower-extremity muscle force and balance performance in adults aged 65 years older. Phys. Ther. 1999, 79, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Dite, W.; Temple, V.A. A clinical test of stepping and change of direction to identify multiple falling older adults. Arch. Phys. Med. Rehabil. 2002, 83, 1566–1571. [Google Scholar] [CrossRef]
- Doheny, E.P.; McGrath, D.; Greene, B.R.; Walsh, L.; McKeown, D.; Cunningham, C.; Crosby, L.; Kenny, R.A.; Caulfield, B. Displacement of centre of mass during quiet standing assessed using accelerometry in older fallers and non-fallers. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar]
- Eto, M.; Miyauchi, S. Relationship between occlusal force and falls among community-dwelling elderly in Japan: A cross-sectional correlative study. BMC Geriatr. 2018, 18, 111. [Google Scholar] [CrossRef]
- Figueiredo, A.I.; Balbinot, G.; Brauner, F.O.; Schiavo, A.; Baptista, R.R.; Pagnussat, A.S.; Hollands, K.; Mestriner, R.G. SPARC Metrics Provide Mobility Smoothness Assessment in Oldest-Old with and Without a History of Falls: A Case Control Study. Front. Physiol. 2020, 11, 540. [Google Scholar] [CrossRef]
- Fino, P.C.; Mojdehi, A.R.; Adjerid, K.; Habibi, M.; Lockhart, T.E.; Ross, S.D. Comparing Postural Stability Entropy Analyses to Differentiate Fallers and Non-fallers. Ann. Biomed. Eng. 2016, 44, 1636–1645. [Google Scholar] [CrossRef]
- Fujimoto, A.; Hori, H.; Tamura, T.; Hirai, T.; Umemura, T.; Iguchi, F.; Sawa, S.; Ogawa, K.; Sato, K.; Kusaka, Y. Relationships between estimation errors and falls in healthy aged dwellers. Gerontology 2015, 61, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Gai, J.; Gomes, L.; Nóbrega, O.d.T.; Rodrigues, M.P. Factors related to falls of elderly women residents in a community. Rev. Assoc. Med. Bras. 2010, 56, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Hachiya, M.; Murata, S.; Otao, H.; Ihara, T.; Mizota, K.; Asami, T. Usefulness of a 50-m round walking test for fall prediction in the elderly requiring long-term care. J. Phys. Ther. Sci. 2015, 27, 3663–3666. [Google Scholar] [CrossRef] [Green Version]
- Hewson, D.J.; Singh, N.K.; Snoussi, H.; Duchêne, J. Classification of elderly as fallers and non-fallers using Centre of Pressure velocity. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010. [Google Scholar]
- Huang, H.C.; Gau, M.L.; Lin, W.C.; Kernohan, G. Assessing Risk of Falling in Older Adults. Public Health Nurs. 2003, 20, 399–411. [Google Scholar] [CrossRef]
- Jalali, M.M.; Gerami, H.; Heidarzadeh, A.; Soleimani, R. Balance performance in older adults and its relationship with falling. Aging Clin. Exp. Res. 2015, 27, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Kurz, I.; Oddsson, L.; Melzer, I. Characteristics of balance control in older persons who fall with injury—A prospective study. J. Electromyogr. Kinesiol. 2013, 23, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Laatar, R.; Baccouch, R.; Borji, R.; Kachouri, H.; Rebai, H.; Sahli, S. Ramadan Fasting Effects on Postural Control in the Elderly: A Comparison Between Fallers and Non-fallers. J. Relig. Health 2019, 58, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Lajoie, Y.; Gallagher, S.P. Predicting falls within the elderly community: Comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch. Gerontol. Geriatr. 2004, 38, 11–26. [Google Scholar] [CrossRef]
- Lichtenstein, M.J.; Shields, S.L.; Shiavi, R.G.; Burger, M.C. Clinical Determinants of Biomechanics Platform Measures of Balance in Aged Women. J. Am. Geriatr. Soc. 1988, 36, 996–1002. [Google Scholar] [CrossRef]
- Lockhart, T.E.; Frames, C.W.; Soangra, R.; Lieberman, A. Effects of Obesity and Fall Risk on Gait and Posture of Community-Dwelling Older Adults. Int. J. Prog. Health Manag. 2019, 10, 19. [Google Scholar]
- MacRae, P.G.; Lacourse, M.; Moldavon, R. Physical performance measures that predict faller status in community- dwelling older adults. J. Orthop. Sports Phys. Ther. 1992, 16, 123–128. [Google Scholar] [CrossRef]
- Maranesi, E.; Merlo, A.; Fioretti, S.; Zemp, D.D.; Campanini, I.; Quadri, P. A statistical approach to discriminate between non-fallers, rare fallers and frequent fallers in older adults based on posturographic data. Clin. Biomech. 2016, 32, 8–13. [Google Scholar] [CrossRef]
- McGrath, D.; Doheny, E.P.; Walsh, L.; McKeown, D.; Cunningham, C.; Crosby, L.; Kenny, R.A.; Stergiou, N.; Caulfield, B.; Greene, B.R. Taking balance measurement out of the laboratory and into the home: Discriminatory capability of novel centre of pressure measurement in fallers and non-fallers. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 3296–3299. [Google Scholar]
- Melzer, I.; Benjuya, N.; Kaplanski, J. Postural stability in the elderly: A comparison between fallers and non-fallers. Age Ageing 2004, 33, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Melzer, I.; Kurz, I.; Oddsson, L.I.E. A retrospective analysis of balance control parameters in elderly fallers and non-fallers. Clin. Biomech. 2010, 25, 984–988. [Google Scholar] [CrossRef]
- Merlo, A.; Zemp, D.; Zanda, E.; Rocchi, S.; Meroni, F.; Tettamanti, M.; Recchia, A.; Lucca, U.; Quadri, P. Postural stability and history of falls in cognitively able older adults: The Canton Ticino study. Gait Posture 2012, 36, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Morita, M.; Takamura, N.; Kusano, Y.; Abe, Y.; Moji, K.; Takemoto, T.I.; Aoyagi, K. Relationship between falls and physical performance measures among community-dwelling elderly women in Japan. Aging Clin. Exp. Res. 2005, 17, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Muir, J.W.; Kiel, D.P.; Hannan, M.; Magaziner, J.; Rubin, C.T. Dynamic Parameters of Balance Which Correlate to Elderly Persons with a History of Falls. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.R.; Vieira, E.R.; Gil, A.W.O.; Fernandes, K.B.P.; Teixeira, D.C.; Amorim, C.F.; da Silva, R.A. One-legged stance sway of older adults with and without falls. PLoS ONE 2018, 13, e0203887. [Google Scholar] [CrossRef] [Green Version]
- Pajala, S.; Era, P.; Koskenvuo, M.; Kaprio, J.; Törmäkangas, T.; Rantanen, T. Force platform balance measures as predictors of indoor and outdoor falls in community-dwelling women aged 63-76 years. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 171–178. [Google Scholar] [CrossRef]
- Pua, Y.H.; Ong, P.H.; Lim, E.C.W.; Huang, K.S.; Clark, R.A.; Chandran, M. Functional heterogeneity and outcomes in community-dwelling women with osteoporosis, with and without a history of falls. Gait Posture 2014, 39, 971–977. [Google Scholar] [CrossRef]
- Ricci, N.A.; de Faria Figueiredo Gonçalves, D.; Coimbra, A.M.V.; Coimbra, I.B. Sensory interaction on static balance: A comparison concerning the history of falls of community-dwelling elderly. Geriatr. Gerontol. Int. 2009, 9, 165–171. [Google Scholar] [CrossRef]
- Sample, R.B.; Kinney, A.L.; Jackson, K.; Diestelkamp, W.; Bigelow, K.E. Identification of key outcome measures when using the instrumented timed up and go and/or posturography for fall screening. Gait Posture 2017, 57, 168–171. [Google Scholar] [CrossRef]
- Akizuki, K.; Echizenya, Y.; Kaneno, T.; Ohashi, Y. Usefulness of an unstable board balance test to accurately identify community-dwelling elderly individuals with a history of falls. J. Rehabil. Med. 2019, 51, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Shumway-Cook, A.; Woollacott, M.; Kerns, K.A.; Baldwin, M. The effects of two types of cognitive tasks on postural stability in older adults with and without a history of falls. J. Gerontol. A Biol. Sci. Med. Sci. 1997, 52A, M232–M240. [Google Scholar] [CrossRef] [Green Version]
- Sihvonen, S.; Era, P.; Helenius, M. Postural balance and health-related factors in middle-aged and older women with injurious falls and non-fallers. Aging Clin. Exp. Res. 2004, 16, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Stel, V.S.; Smit, J.H.; Pluijm, S.M.F.; Lips, P. Balance and mobility performance as treatable risk factors for recurrent falling in older persons. J. Clin. Epidemiol. 2003, 56, 659–668. [Google Scholar] [CrossRef]
- Thomas, J.I.; Lane, J.V. A pilot study to explore the predictive validity of 4 measures of falls risk in frail elderly patients. Arch. Phys. Med. Rehabil. 2005, 86, 1636–1640. [Google Scholar] [CrossRef] [PubMed]
- Uiga, L.; Capio, C.M.; Ryu, D.; Wilson, M.R.; Masters, R.S.W. The role of conscious control in maintaining stable posture. Hum. Mov. Sci. 2018, 57, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, D.K.; Gossman, M.R.; Shaddeau, S.A.; Jackson, J.R. Balance performance and step width in noninstitutionalized, elderly, female fallers and nonfallers. Phys. Ther. 1989, 69, 923–931. [Google Scholar] [CrossRef]
- Moreira, M.N.; Bilton, T.L.; Dias, R.C.; Ferriolli, E.; Perracini, M.R. What are the Main Physical Functioning Factors Associated with Falls Among Older People with Different Perceived Fall Risk? Physiother. Res. Int. 2017, 22. [Google Scholar] [CrossRef]
- Aslan, U.B.; Cavlak, U.; Yagci, N.; Akdag, B. Balance performance, aging and falling: A comparative study based on a Turkish sample. Arch. Gerontol. Geriatr. 2008, 46, 283–292. [Google Scholar] [CrossRef]
- Cabral, K.d.N.; Brech, G.C.; Alonso, A.C.; Soares, A.T.; Opaleye, D.C.; Greve, J.M.D.; Jacob-Filho, W. Posturographic measures did not improve the predictive power to identify recurrent falls in community-dwelling elderly fallers. Clinics 2020, 75, e1409. [Google Scholar] [CrossRef] [Green Version]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Van Hoecke, J.; Gremeaux, V.; Martin, A. Ankle muscle strength discriminates fallers from non-fallers. Front. Aging Neurosci. 2014, 6. [Google Scholar] [CrossRef] [Green Version]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Gremeaux, V.; Martin, A. The involvement of ankle muscles in maintaining balance in the upright posture is higher in elderly fallers. Exp. Gerontol. 2016, 77, 38–45. [Google Scholar] [CrossRef]
- Cho, B.L.; Scarpace, D.; Alexander, N.B. Tests of stepping as indicators of mobility, balance, and fall risk in balance-impaired older adults. J. Am. Geriatr. Soc. 2004, 52, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Giorgetti, M.M.; Harris, B.A.; Jette, A. Reliability of clinical balance outcome measures in the elderly. Physiother. Res. Int. 1998, 3, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.; Tesio, L.; Martino, M.T.; Ricupero, C. Reliability of four simple, quantitative tests of balance and mobility in healthy elderly females. Aging Clin. Exp. Res. 1998, 10, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Johnsson, E.; Henriksson, M.; Hirschfeld, H. Does the functional reach test reflect stability limits in elderly people? J. Rehabil. Med. 2003, 35, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Beauchet, O.; Fantino, B.; Allali, G.; Muir, S.W.; Montero-Odasso, M.; Annweiler, C. Timed up and go test and risk of falls in older adults: A systematic review. J. Nutr. Heal. Aging 2011, 15, 933–938. [Google Scholar] [CrossRef]
- Bauer, C.M.; Gröger, I.; Rupprecht, R.; Tibesku, C.O.; Gaßmann, K.G. Reliabilität der statischen Posturografie bei älteren Personen. Z. Gerontol. Geriatr. 2010, 43, 245–248. [Google Scholar] [CrossRef]
- Stemplewski, R.; Maciaszek, J.; Osiński, W.; Szeklicki, R. Test-retest reliability of measurements of the center of pressure displacement in quiet standing and during maximal voluntary body leaning among healthy elderly men. J. Hum. Kinet. 2011, 28, 15–23. [Google Scholar] [CrossRef]
- Roman-Liu, D. Age-related changes in the range and velocity of postural sway. Arch. Gerontol. Geriatr. 2018, 77, 68–80. [Google Scholar] [CrossRef]
- Ghai, S.; Ghai, I.; Effenberg, A.O. Effects of dual tasks and dual-task training on postural stability: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 557–577. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, J.; Ansai, J.H.; Masse, F.A.A.; Vale, F.A.C.; Takahashi, A.C.d.M.; Andrade, L.P. de Dual-task as a predictor of falls in older people with mild cognitive impairment and mild Alzheimer’s disease: A prospective cohort study. Braz. J. Phys. Ther. 2018, 22, 417–423. [Google Scholar] [CrossRef]
- Tomas-Carus, P.; Biehl-Printes, C.; Pereira, C.; Vieiga, G.; Costa, A.; Collado-Mateo, D. Dual task performance and history of falls in community-dwelling older adults. Exp. Gerontol. 2019, 120, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Sarabon, N.; Kern, H.; Loefler, S.; Jernej, R. Selection of body sway parameters according to their sensitivity and repeatability. Eur. J. Transl. Myol. 2010, 20, 5. [Google Scholar] [CrossRef]
- Van Parys, J.A.P.; Njiokiktjien Ch., J. Romberg’s sign expressed in a quotient. Agressologie 1976, 17, 95–100. [Google Scholar] [PubMed]
- Oreská, Ľ.; Slobodová, L.; Vajda, M.; Kaplánová, A.; Tirpáková, V.; Cvečka, J.; Buzgó, G.; Ukropec, J.; Ukropcová, B.; Sedliak, M. The effectiveness of two different multimodal training modes on physical performance in elderly. Eur. J. Transl. Myol. 2020, 30, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Cvecka, J.; Tirpakova, V.; Sedliak, M.; Kern, H.; Mayr, W.; Hamar, D. Physical activity in elderly. Eur. J. Transl. Myol. 2015, 25, 249–252. [Google Scholar] [CrossRef]
- Sarabon, N.; Loefler, S.; Cvecka, J.; Sedliak, M.; Kern, H. Strength training in elderly people improves static balance: A randomized controlled trial. Eur. J. Transl. Myol. 2013, 23, 85–95. [Google Scholar] [CrossRef]
- Peri, E.; Ambrosini, E.; Pedrocchi, A.; Ferrigno, G.; Nava, C.; Longoni, V.; Monticone, M.; Ferrante, S. Can FES-augmented active cycling training improve locomotion in post-acute elderly stroke patients? Eur. J. Transl. Myol. 2016, 26, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Zampieri, S.; Mosole, S.; Löfler, S.; Fruhmann, H.; Burggraf, S.; Cvečka, J.; Hamar, D.; Sedliak, M.; Tirptakova, V.; Šarabon, N.; et al. Physical exercise in Aging: Nine weeks of leg press or electrical stimulation training in 70 years old sedentary elderly people. Eur. J. Transl. Myol. 2015, 25, 237–242. [Google Scholar] [CrossRef]


{kind=link}
| Test/Outcome Measure | SMD (95% CI) * | Statistical Significance (p) | Number of Studies and Heterogeneity (I2) | Number of Participants (F/NF) |
|---|---|---|---|---|
| Instrumented body sway analysis | ||||
| CoP Velocity—Parallel EO | 0.12 (−0.04, 0.29) | 0.140 | 12 (I2 = 42%) | 486/823 |
| CoP Velocity—Parallel EC | 0.21 (−0.01, 0.43) | 0.060 | 7 (I2 = 48%) | 290/448 |
| CoP Velocity—Parallel Foam EO | 0.29 (−0.19, 0.78) | 0.230 | 1 (I2 = N/A) | 19/124 |
| CoP Velocity—Semi-tandem EO | −0.01 (−0.72, 0.69) | 0.970 | 2 (I2 = 86%) | 121/109 |
| CoP Velocity—Parallel EO + COG | 0.05 (−0.25, 0.35) | 0.730 | 2 (I2 = 0%) | 123/71 |
| CoP Velocity AP—Parallel EO | 0.26 (0.06, 0.46) | 0.010 | 9 (I2 = 63%) | 547/972 |
| CoP Velocity AP—Parallel EC | 0.17 (0.05, 0.28) | 0.004 | 7 (I2 = 0%) | 473/863 |
| CoP Velocity AP—Tandem EO | 0.09 (−0.17, 0.34) | 0.500 | 2 (I2 = 0%) | 7/264 |
| CoP Velocity AP—Single-leg | 0.96 (0.62, 1.31) | <0.001 | 1 (I2 = N/A) | 50/120 |
| CoP Velocity AP—Parallel EO + COG | 0.37 (−0.04, 0.77) | 0.070 | 2 (I2 = 48%) | 75/297 |
| CoP Velocity ML—Parallel EO | 0.24 (0.09, 0.38) | 0.002 | 8 (I2 = 0%) | 317/591 |
| CoP Velocity ML—Parallel EC | 0.30 (0.14, 0.47) | <0.001 | 6 (I2 = 0%) | 243/482 |
| CoP Velocity ML—Tandem EO | 0.06 (−0.20, 0.31) | 0.660 | 2 (I2 = 0%) | 79/264 |
| CoP Velocity ML—Single-leg | 0.33 (−0.01, 0.66) | 0.052 | 1 (I2 = N/A) | 50/120 |
| CoP Velocity ML—Parallel EO + COG | 0.24 (−0.18, 0.66) | 0.260 | 2 (I2 = 0.52%) | 75/297 |
| CoP Area—Parallel EO | 0.60 (0.20, 1.00) | 0.003 | 11 (I2 = 90%) | 591/2649 |
| CoP Area—Parallel EC | 0.30 (0.07, 0.54) | 0.010 | 7 (I2 = 65%) | 525/2443 |
| CoP Area—Parallel Foam EO | 0.57 (0.21, 0.93) | 0.002 | 2 (I2 = 0%) | 37/191 |
| CoP Area—Single-leg EO | 0.66 (0.04, 1.28) | 0.040 | 1 (I2 = N/A) | 15/35 |
| CoP Area—Single-leg EC | −0.32 (−0.93, 0.29) | 0.300 | 1 (I2 = N/A) | 15/35 |
| CoP Area—Parallel EO + COG | 0.56 (0.08, 1.04) | 0.020 | 1 (I2 = N/A) | 34/36 |
| CoP Amplitude AP—Parallel EO | 0.24 (0.03, 0.45) | 0.020 | 7 (I2 = 51%) | 341/729 |
| CoP Amplitude AP—Parallel EC | 0.15 (−0.01, 0.31) | 0.070 | 6 (I2 = 13%) | 285/675 |
| CoP Amplitude AP—Parallel Foam EO | 0.71 (−0.21, 1.63) | 0.130 | 2 (I2 = 85%) | 37/191 |
| CoP Amplitude AP—Semi-tandem EO | 0.25 (−0.12, 0.63) | 0.190 | 1 (I2 = N/A) | 56/54 |
| CoP Amplitude AP—Single-leg EO | 0.80 (0.06, 1.55) | 0.040 | 1 (I2 = N/A) | 15/15 |
| CoP Amplitude ML—Parallel EO | 0.35 (0.12, 0.58) | 0.003 | 8 (I2 = 65%) | 430/764 |
| CoP Amplitude ML—Parallel EC | 0.38 (0.12, 0.64) | 0.004 | 6 (I2 = 62%) | 285/675 |
| CoP Amplitude ML—Parallel Foam EO | 0.62 (0.27, 0.98) | <0.001 | 2 (I2 = 0%) | 37/191 |
| CoP Amplitude ML—Semi-tandem EO | 0.21 (−0.16, 0.59) | 0.260 | 1 (I2 = N/A) | 56/54 |
| CoP Amplitude ML—Single-leg EO | 1.31 (0.51, 2.10) | 0.002 | 1 (I2 = N/A) | 15/15 |
| CoP Path—Parallel EO | 0.34 (0.12, 0.56) | 0.003 | 9 (I2 = 71%) | 597/2284 |
| CoP Path—Parallel EC | 0.26 (0.15, 0.37) | <0.001 | 3 (I2 = 0%) | 376/2079 |
| CoP Path—Parallel Foam EO | 0.51 (0.07, 0.95) | 0.020 | 2 (I2 =20%) | 39/144 |
| CoP Path—Semi-tandem EO | −0.03 (−0.70, 0.64) | 0.930 | 2 (I2 =85%) | 121/109 |
| CoP Path AP—Parallel EO | 0.63 (−0.01, 1.28) | 0.060 | 3 (I2 = 74%) | 95/96 |
| CoP Path AP—Parallel EC | 1.00 (0.14, 1.85) | 0.020 | 1 (I2 = N/A) | 12/12 |
| CoP Path ML—Parallel EO | 0.58 (0.06, 1.10) | 0.030 | 3 (I2 = 61%) | 95/96 |
| CoP Path ML—Parallel EC | 3.14 (1.88, 4.39) | <0.001 | 1 (I2 = N/A) | 12/12 |
| CoP Frequency AP—Parallel EO | 0.14 (−0.32, 0.60) | 0.550 | 3 (I2 = 70%) | 122/189 |
| CoP Frequency AP—Parallel EC | 0.05 (−0.40, 0.51) | 0.820 | 3 (I2 = 71%) | 142/159 |
| CoP Frequency AP—Semi-tandem EO | −0.50 (−0.87, −0.14) | 0.007 | 1 (I2 = N/A) | 65/55 |
| CoP Frequency ML—Parallel EO | 0.12 (−0.29, 0.53) | 0.570 | 3 (I2 = 63%) | 122/189 |
| CoP Frequency ML—Parallel EC | −0.09 (−0.64, 0.46) | 0.750 | 3 (I2 =79%) | 142/159 |
| CoP Frequency ML—Semi-tandem EO | −0.42 (−0.79, −0.06) | 0.020 | 1 (I2 = N/A) | 65/55 |
| Computerized board test—EO, Stable | 0.09 (−0.05, 0.24) | 0.220 | 1 (I2 = N/A) | 232/746 |
| Computerized board test—EC, Stable | 0.10 (−0.04, 0.25) | 0.160 | 1 (I2 = N/A) | 232/746 |
| Computerized board test—EO, Unstable | 0.07 (−0.08, 0.22) | 0.340 | 1 (I2 = N/A) | 232/746 |
| Non-instrumented balance tests | ||||
| Functional Reach Test | −0.33 (−0.62, −0.04) | 0.030 | 17 (I2 = 91%) | 824/2593 |
| Single-leg ST—EO | −0.56 (−0.95, −0.18) | 0.004 | 14 (I2 = 94%) | 807/2259 |
| Singe-leg ST—EC | −0.03 (−0.38, 0.32) | 0.870 | 4 (I2 = 47%) | 123/186 |
| Tandem ST—EO | −0.44 (−0.88, 0.00) | 0.050 | 1 (I2 = N/A) | 26/84 |
| Tandem ST—EC | −0.16 (−0.60, 0.28) | 0.470 | 1 (I2 = N/A) | 26/84 |
| Romberg Parallel—EO | −0.25 (−0.74, 0.24) | 0.320 | 1 (I2 = N/A) | 32/32 |
| Romberg Parallel—EC | −0.46 (−0.95, 0.04) | 0.070 | 1 (I2 = N/A) | 32/32 |
| Romberg Parallel Foam—EO | −0.89 (−1.40, −0.37) | <0.001 | 1 (I2 = N/A) | 32/32 |
| Romberg Parallel Foam—EC | −0.52 (−1.02, −0.02) | 0.040 | 1 (I2 = N/A) | 32/32 |
| Romberg Parallel Foam with Visual Disturbance | −0.57 (−1.07, −0.07) | 0.020 | 1 (I2 = N/A) | 32/32 |
| Romberg (sum of 4 conditions) | −0.17 (−0.31, −0.02) | 0.030 | 1 (I2 = N/A) | 232/746 |
| Test / Outcome Measure * | Type of Risk Measure | Risk Measure with 95% CI | Cut-Off/Comparison and Study Reference |
|---|---|---|---|
| CoP Velocity AP—Parallel EO | Odds ratio | 1.98 (1.16–3.40) | Lowest to highest quartile [27] |
| CoP Area—Parallel EC | Odds ratio | 1.03 (1.01–1.05) | Per 1 cm2 increase [43] |
| CoP Amplitude AP—Parallel EO | Odds ratio | 1.30 (0.60–3.00) | >4.8 mm [77] |
| CoP Amplitude AP—Parallel EC | Odds ratio | 1.50 (0.70–3.60) | >6.7 mm [77] |
| CoP Amplitude ML—Parallel EO | Odds ratio | 2.9 (1.3–6.8) | >4.6 mm [77] |
| CoP Amplitude ML—Parallel EC | Odds ratio | 2.3 (1.00–5.4) | >6.8 mm [77] |
| CoP Path—Parallel EO | Odds ratio | 1.90 (1.27–2.84) | Being in lowest quintile [42] |
| Odds ratio | 2.00 (0.9–4.69 | >67.0 cm (30 s trial) [77] | |
| CoP Path—Parallel EC | Odds ratio | 1.65 (1.07–2.55) | Being in lowest quintile [42] |
| Odds ratio | 1.00 (0.40–2.30) | >113 cm (30 s trial) [77] | |
| Functional Reach Test | Relative risk | 1.10 (0.71–1.72) | <18 cm [33] |
| Odds ratio | 5.28 (0.84–33.2) | <18.5 cm [78] | |
| Odds ratio | 8.67 (2.26–33.29) | <25 cm [55] | |
| Incidence density ratio | 1.12 (0.98–1.28) | Per quintile [34] | |
| Rate ratio | 0.60 (0.50–0.90) | Being in lowest quartile [37] | |
| Single-leg ST—EO | Relative risk | 1.62 (1.03–2.56) | <3 s [33] |
| Odds ratio | 8.54 (4.86–14.99) | <12.7 s [55] | |
| Odds ratio | 15.22 (1.72–133.95) | <1.02 s [78] | |
| Odds ratio | 0.38 (0.17–0.84) | Per 1 standard deviation [86] | |
| Tandem ST—EO | Odds ratio | 2.33 (1.34–4.04) | Able/unable [32] |
| Romberg Parallel—EO | Odds ratio | 7.53 (4.58–12.38) | <20 s [55] |
| Romberg (sum of 4 conditions) | Odds ratio | 2.00 (1.21–3.04) | <5 s [22] |
| Table * | Suggested Cut-Off Points/Reference to the Study | Sensitivity | Specificity |
|---|---|---|---|
| CoP Velocity AP—Single-leg | >2.9 cm/s [69] | 0.78 | 0.54 |
| CoP Velocity ML—Single-leg | >3.4 cm/s [69] | 0.70 | 0.58 |
| Functional Reach Test | <4 cm [40] | 0.70 | 0.43 |
| <18.0 cm [33] | 0.47 | 0.59 | |
| <18.5 cm [78] | 0.75 | 0.67 | |
| Single-leg ST—EO | <1.02 s [78] | 0.67 | 0.89 |
| <3.0 s [33] | 0.51 | 0.61 | |
| <8.0 s [40] | 0.67 | 0.48 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozinc, Ž.; Löfler, S.; Hofer, C.; Carraro, U.; Šarabon, N. Diagnostic Balance Tests for Assessing Risk of Falls and Distinguishing Older Adult Fallers and Non-Fallers: A Systematic Review with Meta-Analysis. Diagnostics 2020, 10, 667. https://doi.org/10.3390/diagnostics10090667
Kozinc Ž, Löfler S, Hofer C, Carraro U, Šarabon N. Diagnostic Balance Tests for Assessing Risk of Falls and Distinguishing Older Adult Fallers and Non-Fallers: A Systematic Review with Meta-Analysis. Diagnostics. 2020; 10(9):667. https://doi.org/10.3390/diagnostics10090667
Chicago/Turabian StyleKozinc, Žiga, Stefan Löfler, Christian Hofer, Ugo Carraro, and Nejc Šarabon. 2020. "Diagnostic Balance Tests for Assessing Risk of Falls and Distinguishing Older Adult Fallers and Non-Fallers: A Systematic Review with Meta-Analysis" Diagnostics 10, no. 9: 667. https://doi.org/10.3390/diagnostics10090667