
Titanium Meshes in Guided Bone Regeneration: A Systematic Review


 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Questions
- Is the use of titanium mesh in combination with a particulate bone graft (autologous and/or heterologous) a successful technique regarding the quantity of augmented bone?
- What is the percentage of membrane exposures?
- What are the implant survival, success, and failure rate when performing this bone regeneration technique in simultaneous or delayed implant placement?
2.2. PICO Question
- P: Patients with partially o total edentulism candidates for GBR.
- I: Bone regeneration through autologous and/or heterologous bone graft and the use of titanium meshes.
- C: Different grafting materials and techniques.
- O: The success rate of this technique regarding the quantity of augmented bone, complications, and predictability of this surgical technique.
2.3. Eligibility Criteria
2.4. Information Sources
2.5. Search Strategy
- (Titanium mesh [All Fields] AND bone graft [All Fields]).
- ((Titanium mesh [All Fields] AND (guided bone regeneration [All Fields] OR GBR [All Fields])).
- (Titanium mesh [All Fields] AND ridge augmentation [All Fields]).
2.6. Study Selection
2.7. Data Collection Process and Items
2.8. Risk of Bias in Individual Studies
3. Results
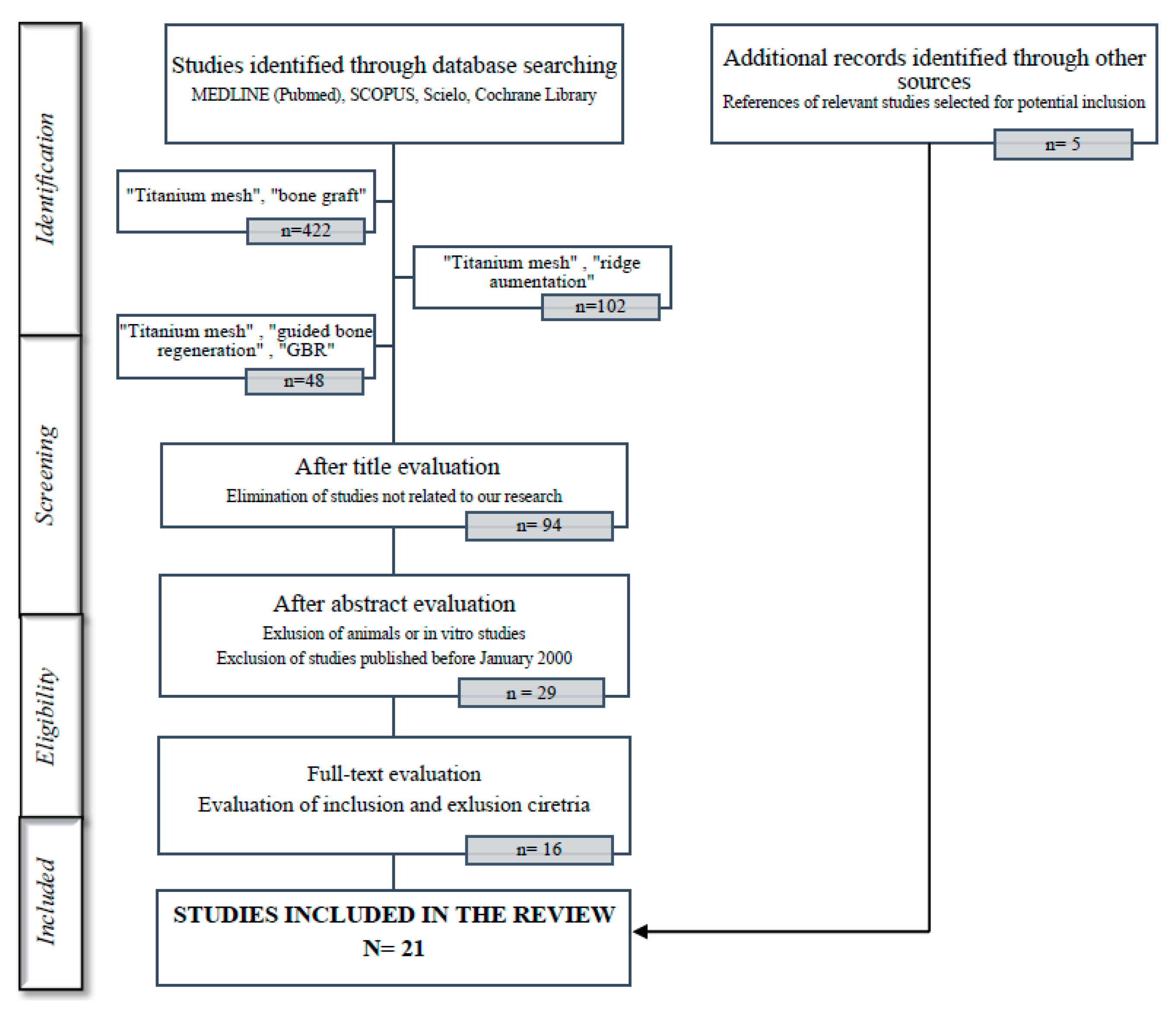
3.1. Study Selection
3.2. Study Methods and Characteristics
3.3. Quality Assessment and Risk of Bias within Studies
3.4. Characteristics of the Mesh
3.5. Bone Gain
3.6. Mesh Exposure
3.7. Implant Placement
4. Discussion
4.1. Bone Gain

{kind=link}
{kind=link}
| Author | Type of Barrier/Membrane | Exposure Rate (%) |
|---|---|---|
| Rasia dal Polo et al. [10] | Titanium mesh | 16 |
| Ricci et al. [11] | Titanium mesh | 22 |
| Briguglio et al. [12] | Titanium mesh | 52 |
| Wessing et al. [41] | Collagen membrane | 20 |
| Wessing et al. [41] | Cross-linked membrane | 28 |
| Ricci et al. [11] | d-PTFE | 17 |
| Roca-Millan et al. [42] | Titanium foils | 23 |
4.2. Mesh Exposure
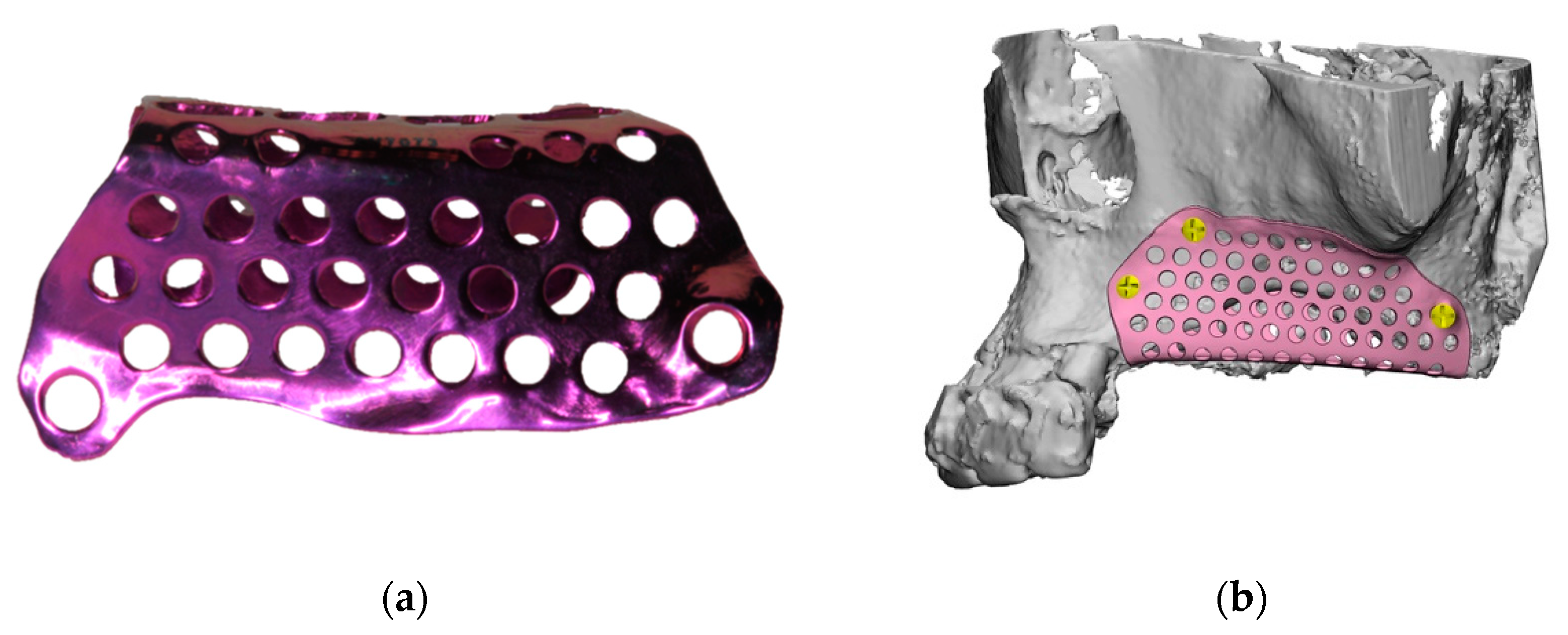
4.3. Characteristics of the Mesh
4.4. Implant Success and Survival Rates
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237–259. [Google Scholar]
- Wang, H.L.; Boyapati, L. “PASS” principles for predictable bone regeneration. Implant. Dent. 2006, 15, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Dahlin, C.; Linde, A.; Gottlow, J.; Nyman, S. Healing of bone defects by guided tissue regeneration. Plast. Reconstr. Surg. 1988, 81, 672–676. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.; Jung, R.E.; Feloutzis, A. A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients. J. Clin. Periodontol. 2002, 29, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Scantlebury, T.V. 1982–1992: A decade of technology development for guided tissue regeneration. J. Periodontol. 1993, 1129–1137. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, Q.; Huang, C.; Mo, A.; Li, J.; Zuo, Y. Biological properties of an anti-bacterial membrane for guided bone regeneration: An experimental study in rats. Clin. Oral Implant. Res. 2010, 21, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.; Jung, R.E. Bone augmentation by means of barrier membranes. Periodontology 2000 2003, 33, 36–53. [Google Scholar] [CrossRef] [Green Version]
- Rakhmatia, Y.D.; Ayukawa, Y.; Furuhashi, A.; Koyano, K. Current barrier membranes: Titanium mesh and other membranes for guided bone regeneration in dental applications. J. Prosthodont. Res. 2013, 57, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Ricci, L.; Perrotti, V.; Ravera, L.; Scarano, A.; Piattelli, A.; Iezzi, G. Rehabilitation of deficient alveolar ridges using titanium grids before and simultaneously with implant placement: A systematic review. J. Periodontol. 2013, 84, 1234–1242. [Google Scholar] [CrossRef]
- Rasia-dal Polo, M.; Poli, P.P.; Rancitelli, D.; Beretta, M.; Maiorana, C. Alveolar ridge reconstruction with titanium meshes: A systematic review of the literature. Med. Oral Patol. Oral Cir. Buccal 2014, 19, e639–e646. [Google Scholar] [CrossRef] [PubMed]
- Briguglio, F.; Falcomatà, D.; Marconcini, S.; Fiorillo, L.; Briguglio, R.; Farronato, D. The Use of Titanium Mesh in Guided Bone Regeneration: A Systematic Review. Int. J. Dent. 2019, 2019, 9065423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting ítems for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.-R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M. ROBINS-1: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Miyamoto, I.; Funaki, K.; Yamauchi, K.; Kodama, T.; Takahashi, T. Alveolar ridge reconstruction with titanium mesh and autogenous particulate bone graft: Computed tomography-based evaluations of augmented bone quality and quantity. Clin. Implant Dent. Relat. Res. 2012, 14, 304–311. [Google Scholar] [CrossRef]
- Degidi, M.; Scarano, A.; Piattelli, A. Regeneration of the alveolar crest using titanium micromesh with autologous bone and a resorbable membrane. J. Oral Implantol. 2003, 29, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Proussaefs, P.; Lozada, J. Use of titanium mesh for staged localized alveolar ridge augmentation: Clinical and histologic-histomorphometric evaluation. J. Oral Implantol. 2006, 32, 237–247. [Google Scholar] [CrossRef] [Green Version]
- Pinho, M.N.; Roriz, V.L.; Novaes, A.B.; Taba, M.; Grisi, M.F.; de Souza, S.L.; Palioto, D.B. Titanium membranes in prevention of alveolar collapse after tooth extraction. Implant. Dent. 2006, 15, 53–61. [Google Scholar] [CrossRef]
- Corinaldesi, G.; Pieri, F.; Marchetti, C.; Fini, M.; Aldini, N.N.; Giardino, R. Histologic and histomorphometric evaluation of alveolar ridge augmentation using bone grafts and titanium micromesh in humans. J. Periodontol. 2007, 78, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Pieri, F.; Corinaldesi, G.; Fini, M.; Aldini, N.N.; Giardino, R.; Marchetti, C. Alveolar ridge augmentation with titanium mesh and a combination of autogenous bone and anorganic bovine bone: A 2-year prospective study. J. Periodontol. 2008, 79, 2093–2103. [Google Scholar] [CrossRef] [PubMed]
- Corinaldesi, G.; Pieri, F.; Sapigni, L.; Marchetti, C. Evaluation of survival and success rates of dental implants placed at the time of or after alveolar ridge augmentation with an autogenous mandibular bone graft and titanium mesh: A 3- to 8-year retrospective study. Int. J. Oral Maxillofac. Implant. 2009, 24, 1119–1128. [Google Scholar]
- Torres, J.; Tamimi, F.; Alkhraisat, M.H.; Manchón, A.; Linares, R.; Prados-Frutos, J.C.; Hernández, G.; López Cabarcos, E. Platelet-rich plasma may prevent titanium-mesh exposure in alveolar ridge augmentation with anorganic bovine bone. J. Clin. Periodontol. 2010, 37, 943–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Her, S.; Kang, T.; Fien, M.J. Titanium mesh as an alternative to a membrane for ridge augmentation. J. Oral Maxillofac. Surg. 2012, 70, 803–810. [Google Scholar] [CrossRef]
- Lizio, G.; Corinaldesi, G.; Marchetti, C. Alveolar ridge reconstruction with titanium mesh: A three-dimensional evaluation of factors affecting bone augmentation. Int. J. Oral Maxillofac. Implant. 2014, 1354–1363. [Google Scholar] [CrossRef]
- Poli, P.P.; Beretta, M.; Cicciù, M.; Maiorana, C. Alveolar ridge augmentation with titanium mesh. A retrospective clinical study. Open Dent. J. 2014, 8, 148–158. [Google Scholar] [CrossRef] [Green Version]
- Sumida, T.; Otawa, N.; Kamata, Y.U.; Kamakura, S.; Mtsushita, T.; Kitagaki, H.; Mori, S.; Sasaki, K.; Fujibayashi, S.; Takemoto, M.; et al. Custom-made titanium devices as membranes for bone augmentation in implant treatment: Clinical application and the comparison with conventional titanium mesh. J. Craniomaxillofac. Surg. 2015, 43, 2183–2188. [Google Scholar]
- Uehara, S.; Kurita, H.; Shimane, T.; Sakai, H.; Kamata, T.; Teramoto, Y.; Yamada, S. Predictability of staged localized alveolar ridge augmentation using a micro titanium mesh. Oral Maxillofac. Surg. 2015, 19, 411–416. [Google Scholar] [CrossRef]
- Zita Gomes, R.; Paraud Freixas, A.; Han, C.H.; Bechara, S.; Tawil, I. Alveolar Ridge Reconstruction with Titanium Meshes and Simultaneous Implant Placement: A Retrospective, Multicenter Clinical Study. Biomed. Res. Int. 2016, 2016, 5126838. [Google Scholar] [CrossRef]
- Andreasi Bassi, M.; Andrisani, C.; Lico, S.; Ormanier, Z.; Ottria, L.; Gargari, M. Guided bone regeneration via a preformed titanium foil: Clinical, histological and histomorphometric outcome of a case series. Oral Implantol. 2016, 16, 164–174. [Google Scholar]
- Ciocca, L.; Lizio, G.; Baldissara, P.; Sambuco, A.; Scotti, R.; Corinaldesi, G. Prosthetically CAD-CAM-Guided Bone Augmentation of Atrophic Jaws Using Customized Titanium Mesh: Preliminary Results of an Open Prospective Study. J. Oral Implantol. 2018, 44, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Cucchi, A.; Sartori, M.; Parrilli, A.; Aldini, N.N.; Vignudelli, E.; Corinaldesi, G. Histological and histomorphometric analysis of bone tissue after guided bone regeneration with non-resorbable membranes vs. resorbable membranes and titanium mesh. Clin. Implant. Dent. Relat. Res. 2019, 21, 693–701. [Google Scholar] [CrossRef]
- Zhang, T.; Zhang, T.; Cai, X. The application of a newly designed L-shaped titanium mesh for GBR with simultaneous implant placement in the esthetic zone: A retrospective case series study. Clin. Implant. Dent. Relat. Res. 2019, 21, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Atef, M.; Tarek, A.; Shaheen, M.; Alarawi, R.M.; Askar, N. Horizontal ridge augmentation using native collagen membrane vs. titanium mesh in atrophic maxillary ridges: Randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2020, 22, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.; Gupta, A.; Bansal, P.; Sharma, R.; Sharma, S. Evaluation of Alveolar Ridge Height Gained by Vertical Ridge Augmentation Using Titanium Mesh and Novabone Putty in Posterior Mandible. J. Maxillofac. Oral Surg. 2020, 19, 32–39. [Google Scholar] [CrossRef]
- Cucchi, A.; Bianchi, A.; Calamai, P.; Rinaldi, L.; Mangano, F.; Vignudelli, E.; Corinaldesi, G. Clinical and volumetric outcomes after vertical ridge augmentation using computer-aided-design/computer-aided manufacturing (CAD/CAM) customized titanium meshes: A pilot study. BMC Oral Health 2020, 20, 219. [Google Scholar] [CrossRef] [PubMed]
- Celletti, R.; Davarpanah, M.; Etienne, D.; Pecora, G.; Tecucianu, J.F.; Djukanovic, D.; Donath, K. Guided tissue regeneration around dental implants in immediate extraction sockets: Comparison of e-PTFE and a new titanium membrane. Int. J. Periodontics Restor. Dent. 1994, 14, 242–253. [Google Scholar]
- Cucchi, A.; Vignudelli, E.; Napolitano, A.; Marchetti, C.; Corinaldesi, G. Evaluation of complication rates and vertical bone gain after guided bone regeneration with non-resorbable membranes versus titanium meshes and resorbable membranes. A randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 821–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagheb, K.; Schiegnitz, E.; Moergel, M.; Walter, C.; Al-Nawas, B.; Wagner, W. Clinical outcome of alveolar ridge augmentation with individualized CAD-CAM-produced titanium mesh. Int. J. Implant. Dent. 2017, 3, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 87–100. [Google Scholar] [CrossRef]
- Roca-Millan, E.; Jané-Salas, E.; Estrugo-Devesa, A.; López-López, J. Evaluation of Bone Gain and Complication Rates after Guided Bone Regeneration with Titanium Foils: A Systematic Review. Materials 2020, 13, 5346. [Google Scholar] [CrossRef]
- Lim, G.; Lin, G.H.; Monje, A.; Chan, H.L.; Wang, H.L. Wound Healing Complications Following Guided Bone Regeneration for Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Stenport, V.F.; Örtorp, A.; Thor, A. Onlay and inlay bone grafts with platelet-rich plasma: Histologic evaluations from human biopsies. J. Oral Maxillofac. Surg. 2011, 69, 1079–1085. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.; Dodge, A.; Luepke, P.; Wang, H.L.; Kapila, Y.; Lin, G.H. Effect of membrane exposure on guided bone regeneration: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benic, G.I.; Bernasconi, M.; Jung, R.E.; Hämmerle, C.H. Clinical and radiographic intra-subject comparison of implants placed with or without guided bone regeneration: 15-year results. J. Clin. Periodontol. 2017, 44, 315–325. [Google Scholar] [CrossRef]
- Clementini, M.; Morlupi, A.; Canullo, L.; Agrestini, C.; Barlattani, A. Success rate of dental implants inserted in horizontal and vertical guided bone regenerated areas: A systematic review. Int. J. Oral Maxillofac. Surg. 2012, 41, 847–855. [Google Scholar] [CrossRef] [PubMed]


| Author/Country | Type of Study | “N” | Mean Ages | Number of Sites | Type of Defects | Graft Materials | Second-Stage Surgery (m) | Mesh Exposure (%) | Bone Augmentation (mm) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | F | (y) | Mx | Md | MHA | MVA | ||||||
| Miyamoto et al., 2001/Japan [17] | Case series | 16 | 25 | 46 | 29 | 21 | C, V, S | Autologous | 6 | 36 | 4 | 8,9 |
| Degidi et al., 2003/Italy [18] | Case series | 4 | 14 | 47.5 | - | - | - | Autologous | 4Md | 0 | - | - |
| 6Mx | ||||||||||||
| Proussaefs et al., 2006/USA [19] | Case series | 10 | 7 | 50.6 | 17 | C | Autologous + ABB 50:50 | 8.47 | 35.3 | 3.75 | 2.56 | |
| Pinho et al., 2006/Brazil [20] | RCT | 10 | 46.3 | 10 | - | V, H | Test: Autologous | 6 | 50 | 8.4 1 | 1.4 1 | |
| 10 | Control: None | 8.8 1 | 1.4 1 | |||||||||
| Corinaldesi et al., 2007/Italy [21] | NRCT | 3 | 3 | 49.3 | 3 | 3 | C | Test: Autologous + BPBM 70:30 | 8−9 | - | - | 4 |
| 4 | 2 | 57.7 | 3 | 3 | Control: Autologous | - | 4.16 | |||||
| Pieri et al., 2008/Italy [22] | Prospective study | 7 | 9 | 49.6 | 9 | 10 | C | Autologous + ABB 70:30 | 8−9 | 5.3 | 4.16 | 3.71 |
| Corinaldesi et al., 2009/Italy [23] | Case series | 9 | 15 | 48.4 | 27 | C | Autologous | 8−9 | 14.8 | - | 4.9 | |
| Torres et al., 2010/Spain [24] | RCT | 7 | 9 | - | 27 | 16 | V, H, C | Test: ABB + PRP | 6 | 0 | 3.4 | 4.1 |
| 6 | 8 | Control: ABB | 28.5 | 3.1 | 3.7 | |||||||
| Her et al., 2012/South Korea [25] | Case series | 11 | 15 | 51 | 9 | 18 | C, H | Autologous + ABB Alloplastic Autologous+Alloplastic | 5.7 | 26 | - | - |
| Lizio et al., 2014/Italy [26] | Case series | 2 | 10 | 49.1 | 11 | 4 | C, V | Autologous + ABB 70:30 | 8−9 | 80 | - | - |
| Poli et al., 2014/Italy [27] | Case series | 8 | 5 | - | 11 | 2 | C | Autologous + DBBM 50:50 | 6 | 7.68 | - | - |
| Sumida et al., 2014/Japan [28] | NRCT | 3 | 10 | 47 | - | - | - | Autologous + CD | 6 | 23.1 | - | - |
| 4 | 9 | 48 | Autologous + CMD | 7.7 | - | - | ||||||
| Uehara et al., 2015/Germany [29] | Case series | 7 | 14 | 47.5 | 11 | 12 | C, V, S | Autologous + Hydroxyapatite 50:50 | 3−7 | 70 | - | - |
| Zita et al., 2016/Portugal [30] | Case series | 15 | 10 | 54.3 | - | - | H | ABB | 3−4 | 24 | 3.67 | - |
| Bassi et al., 2016/Italy [31] | Case series | 1 | 9 | 58 | 0 | 10 | C, H, V | TMAP | 6.7 | 30 | 8.6 | 6.1 |
| Ciocca et al., 2018/Italy [32] | Prospective study | 3 | 6 | 50.2 | 6 | 5 | V | Autologous + ABB 50:50 | 6−8 | 66.6 | - | 3.8 Md 3.9 Mx |
| Cucchi et al., 2019/Italy [33] | RCT | 20 | 52 | - | - | V | Autologous + Allograft 50:50 | 9 | 21.1 | - | 4.1 | |
| Zhang et al., 2019/China [34] | Case series | 12 | - | 16 | 0 | C | ABB | 4−8 | 6.25 | 3.1 | 3.61 | |
| Atef et al., 2020/Egypt [35] | RCT | 10 | - | - | - | H | Autologous + ABB 50:50 | 6 | 40 | 3.7 | - | |
| Malik et al., 2020/India [36] | Case series | 12 | 8 | 48.7 | 0 | 20 | V | TMAP | 6 | 20 | - | 4.82 |
| Cucchi et al., 2020/Italy [37] | Case series | 5 | 5 | 52 | 5 | 5 | V | Autologous + ABB 50:50 | 6−9 | 10 | - | 4.5 |
| Author | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Researchers | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | Other Sources of Bias |
|---|---|---|---|---|---|---|---|
| Pinho et al., 2006 [20] | ? | ? | ? | L | L | ? | L |
| Torres et al., 2010 [21,22,23,24] | L | L | ? | L | L | L | L |
| Cucchi et al., 2019 [33] | L | L | ? | L | L | L | L |
| Atef et al., 2020 [35] | L | L | ? | ? | L | ? | L |
| Author | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias due to Deviations from Intended Interventions | Bias due to Missing data | Bias in Measurement of Outcomes | Overall Bias |
|---|---|---|---|---|---|---|---|
| Corinaldesi et al., 2007 [21] | L | L | ? | ? | L | L | L |
| Sumida et al., 2015 [28] | L | L | ? | L | L | L | L |
| Authors | Characteristics of the Mesh Used | Thickness |
|---|---|---|
| Miyamoto et al., 2001 [17] | Preshaped titanium mesh (M-TAM, Stryker Leinger GmbH & Co., KG, Freiburg ASTM F-67 Jeil Medical Corp., Seoul, Korea) | 0.1 and 0.2 mm thick |
| Degidi et al., 2003 [18] | Preshaped micromesh (Cortical Mesh, Micronova, Bologna, Italy) | NE |
| Proussaefs et al., 2006 [19] | Preshaped titanium mesh (Osteo-Tram; OsteoMed) | 0.2 mm thick |
| Pinho et al., 2006 [20] | Preshaped titanium mesh (Frios Boneshield; DENTSPLY Friadent) | NE |
| Corinaldesi et al., 2007 [21] | Preshaped and trimmed titanium micromesh (ACE surgical supply, Straumann) | 0.2 mm thick |
| Pieri et al., 2008 [22] | Preshaped titanium mesh (Modus 1.5 Mesh, Straumann, Waldenburg, Switzerland) | NE |
| Corinaldesi et al., 2009 [23] | Preshaped and trimmed titanium mesh (ACE Titanium Micro Mesh, ACE Surgical Supply Company; Modus 0.9 Mesh, Medartis) | 0.2 mm thick |
| Torres et al., 2010 [24] | Preshaped and trimmed titanium mesh | NE |
| Her et al., 2012 [25] | Preshaped and trimmed titanium mesh (Jeil Medical, Seoul, South Korea) | 0.1 mm thick |
| Lizio et al., 2014 [26] | Titanium mesh (ridge-form; OsteoMed) | 0.2 mm thick |
| Poli et al., 2014 [27] | Preshaped and trimmed titanium mesh (ridge-form; (KLS Martin, Tuttlingen, Germany) | 0.2 mm thick |
| Sumida et al., 2014 [28] | Custom-made titanium mesh (Ace Surgical SupplyCo., Inc. Brockton, MA, USA) | 0.5 mm thick |
| Uehara et al., 2015 [29] | Preshaped and trimmed microtitanium mesh (Striker-Leibinger, Freiburg, Germany) | 0.1 mm thick |
| Zita et al., 2016 [30] | Titanium mesh (i–Gen, MegaGen, Gyeongbuk, Republic of Korea) | NE |
| Bassi et al., 2016 [31] | Titanium foil (grade 4) | 0.2 mm thick |
| Ciocca et al., 2018 [32] | Custom-made titanium mesh (Electro Optical Systems, Munich, Germany) | 0.1 mm |
| Cucchi et al., 2019 [33] | Preshaped titaium mesh (Trinon Titanium; Karlsruhe, Germany) | NE |
| Zhang et al., 2019 [34] | L-Shaped titanium mesh; Preshaped and trimmed | 0.2 mm thick |
| Atef et al., 2020 [35] | Preshaped titanium mesh (Bioinnovation, Brazil) | NE |
| Malik et al., 2020 [36] | Preshaped and trimmed titanium mesh | NE |
| Cucchi et al., 2020 [37] | Custom-made titanium mesh (3D-Mesh®®, Biotec Srl, Dueville, Vicenza, Italy) | >0.5 mm thick |
| Author/Country | Implant Placement | Implants | Implant Lost | Bone Loss (mm) | Success Rate (%) | Survival Rate (%) | Follow-up (m) | |
|---|---|---|---|---|---|---|---|---|
| Mx | Md | |||||||
| Miyamoto et al., 2001/Japan [17] | After 6 months | 89 | 1 | - | 94 | 92.8 | 47.5 | |
| Degidi et al., 2003/Italy [18] | Simultaneously | 50 | 0 | - | 100 | 100 | 84 | |
| Proussaefs et al., 2006/USA [19] | After 9−10 months | 36 | 5 | - | 0 MBR | - | - | 6 |
| Corinaldesi et al., 2007/Italy [21] | After 8−9 months | 20 | 15 | 0 | - | - | 100 | 12 |
| Pieri et al., 2008/Italy [22] | After 8−9 months | 21 | 23 | 0 | 1.36 MBR | 93.2 | 100 | 12 |
| Corinaldesi et al., 2009/Italy [23] | Simultaneously After 8−9 months | 20 36 | 0 0 | 1.22 MBR 1.26 MBR | 96.4 | 100 | 36−96 | |
| Torres et al., 2010/Spain [24] | After 6 months | 97 | 3 | - | - | 98.6 | 24 | |
| Her et al., 2012/South Korea [25] | After 5−7 months | 27 | 41 | 0 | - | 100 | 100 | 6−24 |
| Poli et al., 2014/Italy [27] | After 6 months | 16 | 4 | 0 | 1.74 M, 1.91 D | 100 | 100 | 88 |
| Uehara et al., 2015/Germany [29] | After 6 months | 64 | 1 | - | - | 98.4 | 40 | |
| Zita et al., 2016/Portugal [30] | Simultaneously | 32 | 8 | 1 | 0.43 MBR | - | 97.5 | 12 |
| Bassi et al., 2016/Italy [31] | After 6−7 months | 0 | 18 | 0 | 1.17 MBR | 88.2 | 100 | 12 |
| Ciocca et al., 2018/Italy [32] | After 6−8 months | 14 | 12 | 0 | - | - | 100 | 24 |
| Cucchi et al., 2019/Italy [33] | Simultaneously | 0 | 19 | 0 | 0 MBR | 100 | 100 | 12 |
| Zhang et al., 2019/China [34] | Simultaneously | 16 | 0 | 0 | 0.81 V 0.13 H | 93.75 | 100 | 24 |
| Cucchi et al., 2020/Italy [37] | After 6−9 months | 14 | 12 | 0 | 0 MBR | 100 | 100 | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aceves-Argemí, R.; Roca-Millan, E.; González-Navarro, B.; Marí-Roig, A.; Velasco-Ortega, E.; López-López, J. Titanium Meshes in Guided Bone Regeneration: A Systematic Review. Coatings 2021, 11, 316. https://doi.org/10.3390/coatings11030316
Aceves-Argemí R, Roca-Millan E, González-Navarro B, Marí-Roig A, Velasco-Ortega E, López-López J. Titanium Meshes in Guided Bone Regeneration: A Systematic Review. Coatings. 2021; 11(3):316. https://doi.org/10.3390/coatings11030316
Chicago/Turabian StyleAceves-Argemí, Ricard, Elisabet Roca-Millan, Beatriz González-Navarro, Antonio Marí-Roig, Eugenio Velasco-Ortega, and José López-López. 2021. "Titanium Meshes in Guided Bone Regeneration: A Systematic Review" Coatings 11, no. 3: 316. https://doi.org/10.3390/coatings11030316