
Twenty-Year Retrospective Study of Post-Enucleation Chemotherapy in High-Risk Patients with Unilateral Retinoblastoma

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Study Design
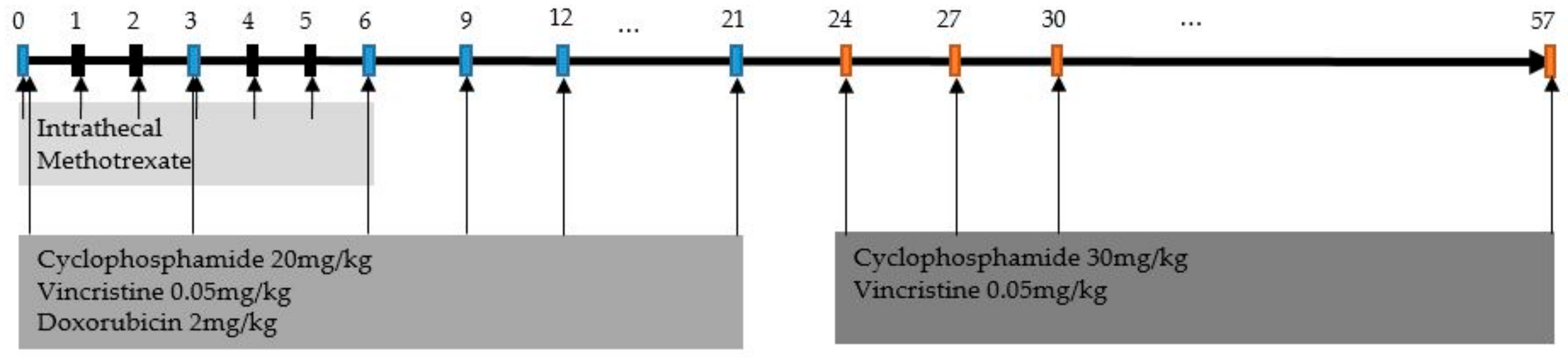
2.2. Treatment
2.3. Toxicity and Response Evaluation
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
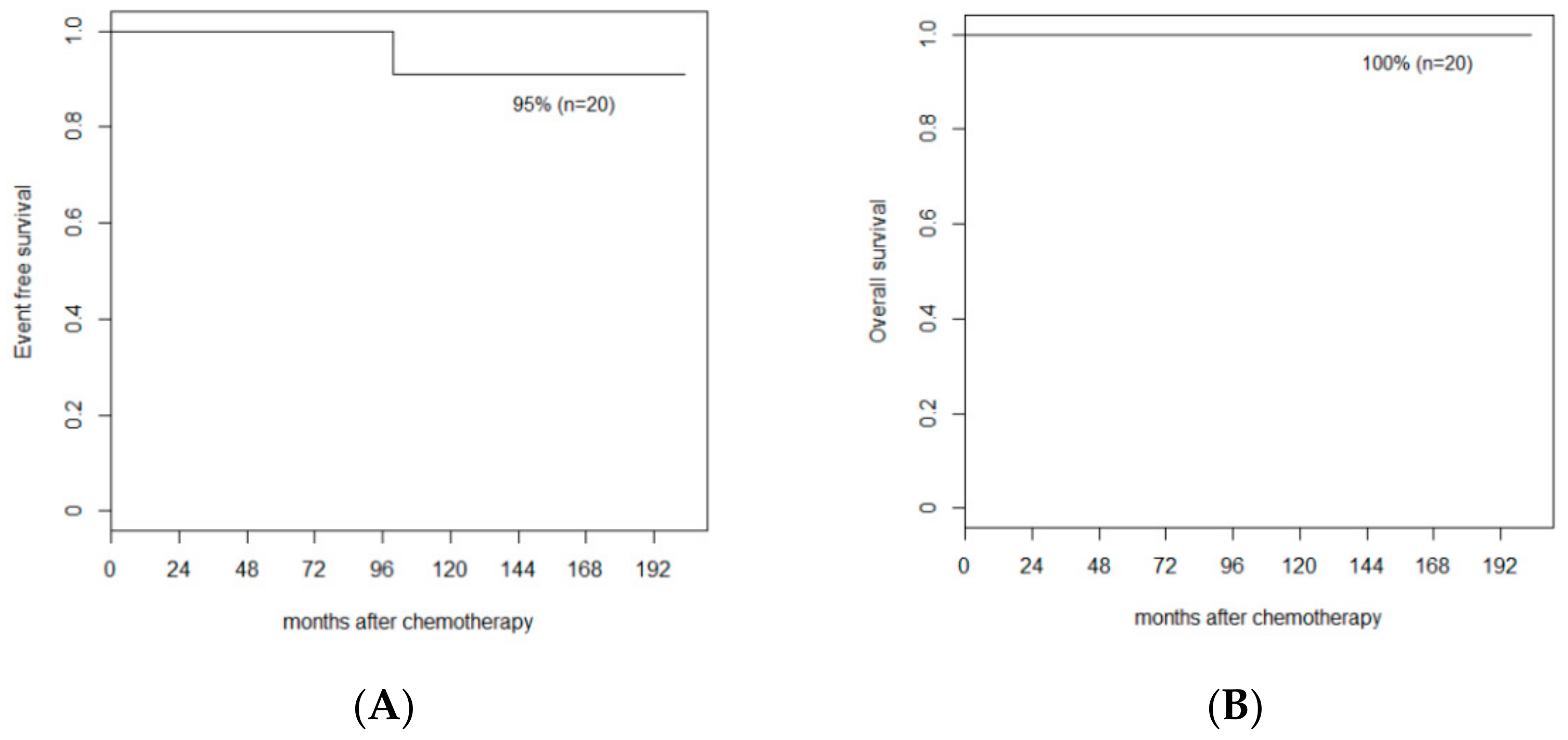
3.2. Response and Survival
3.3. Toxicity
3.4. Late Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abramson, D.H. Retinoblastoma incidence in the United States. Arch. Ophthalmol. 1990, 108, 1514. [Google Scholar] [CrossRef] [PubMed]
- Seregard, S.; Lundell, G.; Svedberg, H.; Kivela, T. Incidence of retinoblastoma from 1958 to 1998 in Northern Europe: Advantages of birth cohort analysis. Ophthalmology 2004, 111, 1228–1232. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.M.; Phillips, R.A.; Becker, A.J.; Gallie, B.L. Identification of germline and somatic mutations affecting the retinoblastoma gene. Science 1988, 241, 1797–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broaddus, E.; Topham, A.; Singh, A.D. Incidence of retinoblastoma in the USA: 1975–2004. Br. J. Ophthalmol. 2009, 93, 21–23. [Google Scholar] [CrossRef] [PubMed]
- MacCarthy, A.; Birch, J.M.; Draper, G.J.; Hungerford, J.L.; Kingston, J.E.; Kroll, M.E.; Onadim, Z.; Stiller, C.A.; Vincent, T.J.; Murphy, M.F. Retinoblastoma in Great Britain 1963–2002. Br. J. Ophthalmol. 2009, 93, 33–37. [Google Scholar] [CrossRef]
- Ghassemi, F.; Khodabande, A. Risk definition and management strategies in retinoblastoma: Current perspectives. Clin. Ophthalmol. 2015, 9, 985–994. [Google Scholar] [CrossRef] [Green Version]
- Honavar, S.G.; Singh, A.D.; Shields, C.L.; Meadows, A.T.; Demirci, H.; Cater, J.; Shields, J.A. Postenucleation adjuvant therapy in high-risk retinoblastoma. Arch. Ophthalmol. 2002, 120, 923–931. [Google Scholar] [CrossRef]
- Uusitalo, M.S.; Van Quill, K.R.; Scott, I.U.; Matthay, K.K.; Murray, T.G.; O’Brien, J.M. Evaluation of chemoprophylaxis in patients with unilateral retinoblastoma with high-risk features on histopathologic examination. Arch. Ophthalmol. 2001, 119, 41–48. [Google Scholar]
- Khelfaoui, F.; Validire, P.; Auperin, A.; Quintana, E.; Michon, J.; Pacquement, H.; Desjardins, L.; Asselain, B.; Schlienger, P.; Vielh, P.; et al. Histopathologic risk factors in retinoblastoma: A retrospective study of 172 patients treated in a single institution. Cancer 1996, 77, 1206–1213. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L.; Shah, S.U.; Eagle, R.C., Jr.; Shields, J.A.; Leahey, A. Postenucleation adjuvant chemotherapy with vincristine, etoposide, and carboplatin for the treatment of high-risk retinoblastoma. Arch. Ophthalmol. 2011, 129, 1422–1427. [Google Scholar] [CrossRef] [Green Version]
- Dittner-Moormann, S.; Reschke, M.; Abbink, F.C.H.; Aerts, I.; Atalay, H.T.; Fedorovna Bobrova, N.; Biewald, E.; Brecht, I.B.; Caspi, S.; Cassoux, N.; et al. Adjuvant therapy of histopathological risk factors of retinoblastoma in Europe: A survey by the European Retinoblastoma Group (EURbG). Pediatr. Blood Cancer 2021, 68, e28963. [Google Scholar] [CrossRef]
- Kim, H.; Lee, J.W.; Kang, H.J.; Park, H.J.; Kim, Y.Y.; Shin, H.Y.; Yu, Y.S.; Kim, I.H.; Ahn, H.S. Clinical results of chemotherapy based treatment in retinoblastoma patients: A single center experience. Cancer Res. Treat. 2008, 40, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Chévez-Barrios, P.; Eagle, R.C., Jr.; Krailo, M.; Piao, J.; Albert, D.M.; Gao, Y.; Vemuganti, G.; Ali, M.J.; Khetan, V.; Honavar, S.G.; et al. Study of Unilateral Retinoblastoma with and without Histopathologic High-Risk Features and the Role of Adjuvant Chemotherapy: A Children’s Oncology Group Study. J. Clin. Oncol. 2019, 37, 2883–2891. [Google Scholar] [CrossRef]
- Chantada, G.L.; Fandino, A.C.; Guitter, M.R.; Raslawski, E.C.; Dominguez, J.L.; Manzitti, J.; de Davila, M.T.; Zubizarreta, P.; Scopinaro, M. Results of a prospective study for the treatment of unilateral retinoblastoma. Pediatr. Blood Cancer 2010, 55, 60–66. [Google Scholar] [CrossRef]
- Aerts, I.; Sastre-Garau, X.; Savignoni, A.; Lumbroso-Le Rouic, L.; Thebaud-Leculee, E.; Frappaz, D.; Coze, C.; Thomas, C.; Gauthier-Villars, M.; Levy-Gabriel, C.; et al. Results of a multicenter prospective study on the postoperative treatment of unilateral retinoblastoma after primary enucleation. J. Clin. Oncol. 2013, 31, 1458–1463. [Google Scholar] [CrossRef]
- Sullivan, E.M.; Wilson, M.W.; Billups, C.A.; Wu, J.; Merchant, T.E.; Brennan, R.C.; Haik, B.G.; Shulkin, B.; Free, T.M.; Given, V.; et al. Pathologic risk-based adjuvant chemotherapy for unilateral retinoblastoma following enucleation. J. Pediatr. Hematol. Oncol. 2014, 36, e335–e340. [Google Scholar] [CrossRef] [Green Version]
- Perez, V.; Sampor, C.; Rey, G.; Parareda-Salles, A.; Kopp, K.; Dabezies, A.P.; Dufort, G.; Zelter, M.; Lopez, J.P.; Urbieta, M.; et al. Treatment of Nonmetastatic Unilateral Retinoblastoma in Children. JAMA Ophthalmol. 2018, 136, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Zelter, M.; Damel, A.; Gonzalez, G.; Schwartz, L. A prospective study on the treatment of retinoblastoma in 72 patients. Cancer 1991, 68, 1685–1690. [Google Scholar] [CrossRef]
- Freeman, C.R.; Esseltine, D.L.; Whitehead, V.M.; Chevalier, L.; Little, J.M. Retinoblastoma: The case for radiotherapy and for adjuvant chemotherapy. Cancer 1980, 46, 1913–1918. [Google Scholar] [CrossRef]
- Chantada, G.L.; Doz, F.; Orjuela, M.; Qaddoumi, I.; Sitorus, R.S.; Kepak, T.; Furmanchuk, A.; Castellanos, M.; Sharma, T.; Chevez-Barrios, P.; et al. World disparities in risk definition and management of retinoblastoma: A report from the International Retinoblastoma Staging Working Group. Pediatr. Blood Cancer 2008, 50, 692–694. [Google Scholar] [CrossRef]
- Chantada, G.L.; Dunkel, I.J.; de Davila, M.T.; Abramson, D.H. Retinoblastoma patients with high risk ocular pathological features: Who needs adjuvant therapy? Br. J. Ophthalmol. 2004, 88, 1069–1073. [Google Scholar] [CrossRef] [PubMed]
- Sreelakshmi, K.V.; Chandra, A.; Krishnakumar, S.; Natarajan, V.; Khetan, V. Anterior Chamber Invasion in Retinoblastoma: Not an Indication for Adjuvant Chemotherapy. Invest Ophthalmol. Vis. Sci. 2017, 58, 4654–4661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuenca, A.; Giron, F.; Castro, D.; Fandino, A.; Guitter, M.; de Davila, M.T.; Chantada, G. Microscopic scleral invasion in retinoblastoma: Clinicopathological features and outcome. Arch. Ophthalmol. 2009, 127, 1006–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chantada, G.L.; Guitter, M.R.; Fandino, A.C.; Raslawski, E.C.; de Davila, M.T.; Vaiani, E.; Scopinaro, M.J. Treatment results in patients with retinoblastoma and invasion to the cut end of the optic nerve. Pediatr. Blood Cancer 2009, 52, 218–222. [Google Scholar] [CrossRef]
- MacCarthy, A.; Bayne, A.M.; Draper, G.J.; Eatock, E.M.; Kroll, M.E.; Stiller, C.A.; Vincent, T.J.; Hawkins, M.M.; Jenkinson, H.C.; Kingston, J.E.; et al. Non-ocular tumours following retinoblastoma in Great Britain 1951 to 2004. Br. J. Ophthalmol. 2009, 93, 1159–1162. [Google Scholar] [CrossRef]
- Schonfeld, S.J.; Kleinerman, R.A.; Abramson, D.H.; Seddon, J.M.; Tucker, M.A.; Morton, L.M. Long-term risk of subsequent cancer incidence among hereditary and nonhereditary retinoblastoma survivors. Br. J. Cancer 2021, 124, 1312–1319. [Google Scholar] [CrossRef]
- Abramson, D.H.; Frank, C.M. Second nonocular tumors in survivors of bilateral retinoblastoma: A possible age effect on radiation-related risk. Ophthalmology 1998, 105, 573–579, discussion 579–580. [Google Scholar] [CrossRef]
- Moll, A.C.; Imhof, S.M.; Schouten-Van Meeteren, A.Y.; Kuik, D.J.; Hofman, P.; Boers, M. Second primary tumors in hereditary retinoblastoma: A register-based study, 1945-1997: Is there an age effect on radiation-related risk? Ophthalmology 2001, 108, 1109–1114. [Google Scholar] [CrossRef]
- Gombos, D.S.; Hungerford, J.; Abramson, D.H.; Kingston, J.; Chantada, G.; Dunkel, I.J.; Antoneli, C.B.; Greenwald, M.; Haik, B.G.; Leal, C.A.; et al. Secondary acute myelogenous leukemia in patients with retinoblastoma: Is chemotherapy a factor? Ophthalmology 2007, 114, 1378–1383. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Data (n = 20) |
|---|---|
| Age at diagnosis, Median (range), months | 26 (1–45) |
| Sex, No. (%) | |
| Male | 7 (35) |
| Female | 13 (65) |
| Laterality, No. (%) | |
| Right eye | 12 (60) |
| Left eye | 8 (40) |
| Reese–Ellsworth classification, No. (%) | |
| Group IV | 1 (5) |
| Group V | 19 (95) |
| ICRB, No. (%) | |
| Group D | 2 (10) |
| Group E | 18 (90) |
| RB1 mutation analysis, No. (%) | |
| 13q14 deletion | 1 (5) |
| Point mutation | 0 (0) |
| Not detected | 11 (55) |
| Not available | 8 (40) |
| Initial CSF cytology | |
| No evidence of involvement | 20 (100) |
| Degree of ONI, No. (%) | Additional High Risk Factors | Data (n = 20) |
|---|---|---|
| ONI | 19 (95) | |
| Pre-laminar | 0 (0) | |
| Intra-laminar | 3 (15) | |
| Isolated ONI | 1 (33) | |
| CI | 2 (66) | |
| Post-laminar | 16 (80) | |
| Isolated ONI | 9 (56) | |
| CI | 5 (31) | |
| CI and positive surgical margin | 1 (6) | |
| AC and scleral invasion and positive surgical margin | 1 (6) | |
| Not available | Uncheckable | 1 (5) |
| Author Year Area | Criteria | Patient No. | Chemotherapy Regimen | Outcome | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LR | IR | HR | LR | IR | HR | LR | IR | HR | Median FU (Year) | OS (%) | EFS (%) | Recurrence (#) | Second Neoplasm | Death (#) | |
| Chantada et al. 2010 Argentina [14] | CI and/or pre/intra- laminar ONI OR PLONI † | Not defined | Sclera and/or margin+ and/or PLONI + massive CI | 65 | Not defined | 30 | Not done | Not defined | 4 × CE 4 × VICy RT for margin+ | 4.1 (0.4–7.6) | LR 96 HR 96 | LR 94 HR 96 | LR CNS (1) systemic (2) HR CNS (1) | 0 | LR (2) † HR (2) |
| Aerts et al. 2013 France [15] | focal CI and/or pre- laminar ONI | AC and/or massive CI and/or intra-/PLONI | Sclera and/or margin+ | 70 | 52 | 1 * | Not done | 2 × CE 2 × VCy | 3 × CE + IT thiotepa 3 × VCy CarboPEC* | 5.9 (2.1–10) | 100 | 100 | 0 | 0 | 0 |
| Sullivan et al. 2014 USA [16] | Focal CI OR pre-/intra- laminar ONI | AC and/or massive CI and/or PLONI and/or ONI + CI | Sclera and/or margin+ | 36 | 7 | 3 | Not done | 4 × VDC | 3 × VDC 3 × VCE | 3.4 (0.8–6.4) | 100 | 100 | 0 | 0 | 0 |
| Perez et al. 2018 Latin America [17] | CI and/or pre-/intra- laminar ONI | Not defined | Sclera and/or margin + and/or PLONI | 84 | Not defined | 42 | Not done | Not defined | 4 × CE 4 × VICy RT for margin+ | 3.8 (0.4–8.2) | LR 100 HR 95 | LR 99 HR 95 | LR ocular (1) HR CNS (1) | 0 | LR (0) HR (2) |
| Chevez-Barrios et al. 2019 USA [13] | Focal CI OR pre-/intra- laminar ONI | Not defined | Sclera and/or margin + and/or massive CI and/or PLONI and/or ONI + CI | 216 | Not defined | 94 | Not done | Not defined | 6 × CEV | 4 | LR 100 HR 97 | LR 99 HR 96 | LR ocular (1) systemic (1) HR CNS (2) unknown (1) | 0 | LR (0) HR (3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sunwoo, Y.; Choi, J.Y.; Park, H.J.; Kim, B.K.; Hong, K.T.; Khwarg, S.I.; Koh, J.; Park, S.-H.; Jo, D.H.; Kim, J.H.; et al. Twenty-Year Retrospective Study of Post-Enucleation Chemotherapy in High-Risk Patients with Unilateral Retinoblastoma. Children 2022, 9, 1983. https://doi.org/10.3390/children9121983
Sunwoo Y, Choi JY, Park HJ, Kim BK, Hong KT, Khwarg SI, Koh J, Park S-H, Jo DH, Kim JH, et al. Twenty-Year Retrospective Study of Post-Enucleation Chemotherapy in High-Risk Patients with Unilateral Retinoblastoma. Children. 2022; 9(12):1983. https://doi.org/10.3390/children9121983
Chicago/Turabian StyleSunwoo, Yoon, Jung Yoon Choi, Hyun Jin Park, Bo Kyung Kim, Kyung Taek Hong, Sang In Khwarg, Jaemoon Koh, Sung-Hye Park, Dong Hyun Jo, Jeong Hun Kim, and et al. 2022. "Twenty-Year Retrospective Study of Post-Enucleation Chemotherapy in High-Risk Patients with Unilateral Retinoblastoma" Children 9, no. 12: 1983. https://doi.org/10.3390/children9121983