
From Prescription Drugs to Natural Health Products: Medication Use in Canadian Infants


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taine, M.; Offredo, L.; Dray-Spira, R.; Weill, A.; Chalumeau, M.; Zureik, M. Paediatric outpatient prescriptions in France between 2010 and 2019: A nationwide population-based study: Paediatric outpatient prescriptions in France, 2010 to 2019. Lancet Reg. Health Eur. 2021, 7, 100129. [Google Scholar] [CrossRef] [PubMed]
- Olsson, J.; Kimland, E.; Pettersson, S.; Odlind, V. Paediatric drug use with focus on off-label prescriptions in Swedish outpatient care--a nationwide study. Acta Paediatr. 2011, 100, 1272–1275. [Google Scholar] [CrossRef] [PubMed]
- Carnovale, C.; Conti, V.; Perrone, V.; Antoniazzi, S.; Pozzi, M.; Merlino, M.; Venegoni, M.; Clementi, E.; Radice, S. Paediatric drug use with focus on off-label prescriptions in Lombardy and implications for therapeutic approaches. Eur. J. Pediatr. 2013, 172, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, N.; Golding, J. A survey of the administration of drugs to young infants. The Alspac Survey Team. Avon Longitudinal Study of Pregnancy and Childhood. Br. J. Clin. Pharmacol. 1995, 40, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.S.; Dreyer, B.P.; Ugboaja, D.C.; Sanchez, D.C.; Paul, I.M.; Moreira, H.A.; Rodriguez, L.; Mendelsohn, A.L. Unit of measurement used and parent medication dosing errors. Pediatrics 2014, 134, e354–e361. [Google Scholar] [CrossRef] [PubMed]
- Star, K.; Edwards, I.R. Pharmacovigilance for children’s sake. Drug Saf. 2014, 37, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Frattarelli, D.A.; Galinkin, J.L.; Green, T.P.; Johnson, T.D.; Neville, K.A.; Paul, I.M.; Van Den Anker, J.N. Off-label use of drugs in children. Pediatrics 2014, 133, 563–567. [Google Scholar] [PubMed]
- Fortescue, E.B.; Kaushal, R.; Landrigan, C.P.; McKenna, K.J.; Clapp, M.D.; Federico, F.; Goldmann, D.A.; Bates, D.W. Prioritizing strategies for preventing medication errors and adverse drug events in pediatric inpatients. Pediatrics 2003, 111 Pt 1, 722–729. [Google Scholar] [CrossRef]
- Yewale, V.N.; Dharmapalan, D. Promoting appropriate use of drugs in children. Int. J. Pediatr. 2012, 2012, 906570. [Google Scholar] [CrossRef]
- World Health Organization. Promoting Safety of Medicines for Children; World Health Organization: Geneva, Switzerland, 2007; Available online: http://site.ebrary.com/id/10214534 (accessed on 8 February 2015).
- Subbarao, P.; Anand, S.S.; Becker, A.B.; Befus, A.D.; Brauer, M.; Brook, J.R.; A Denburg, J.; HayGlass, K.T.; Kobor, M.; Kollmann, T.; et al. The Canadian Healthy Infant Longitudinal Development (CHILD) Study: Examining developmental origins of allergy and asthma. Thorax 2015, 70, 998–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Canada. Health Canada Drug Product Database (DPD). Health Canada Website. Published 28 May 2013. Available online: http://www.hc-sc.gc.ca/dhp-mps/prodpharma/databasdon/index-eng.php (accessed on 14 February 2015).
- Health Canada. Licensed Natural Health Products Database (LNHPD). Health Canada Website. Published 2 December 2013. Available online: http://www.hc-sc.gc.ca/dhp-mps/prodnatur/applications/licen-prod/lnhpd-bdpsnh-eng.php (accessed on 14 February 2015).
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2015. WHO Collaborating Centre for Drug Statistics Methodology Website. Published 19 December 2013. Available online: http://www.whocc.no/atc_ddd_index/ (accessed on 14 February 2015).
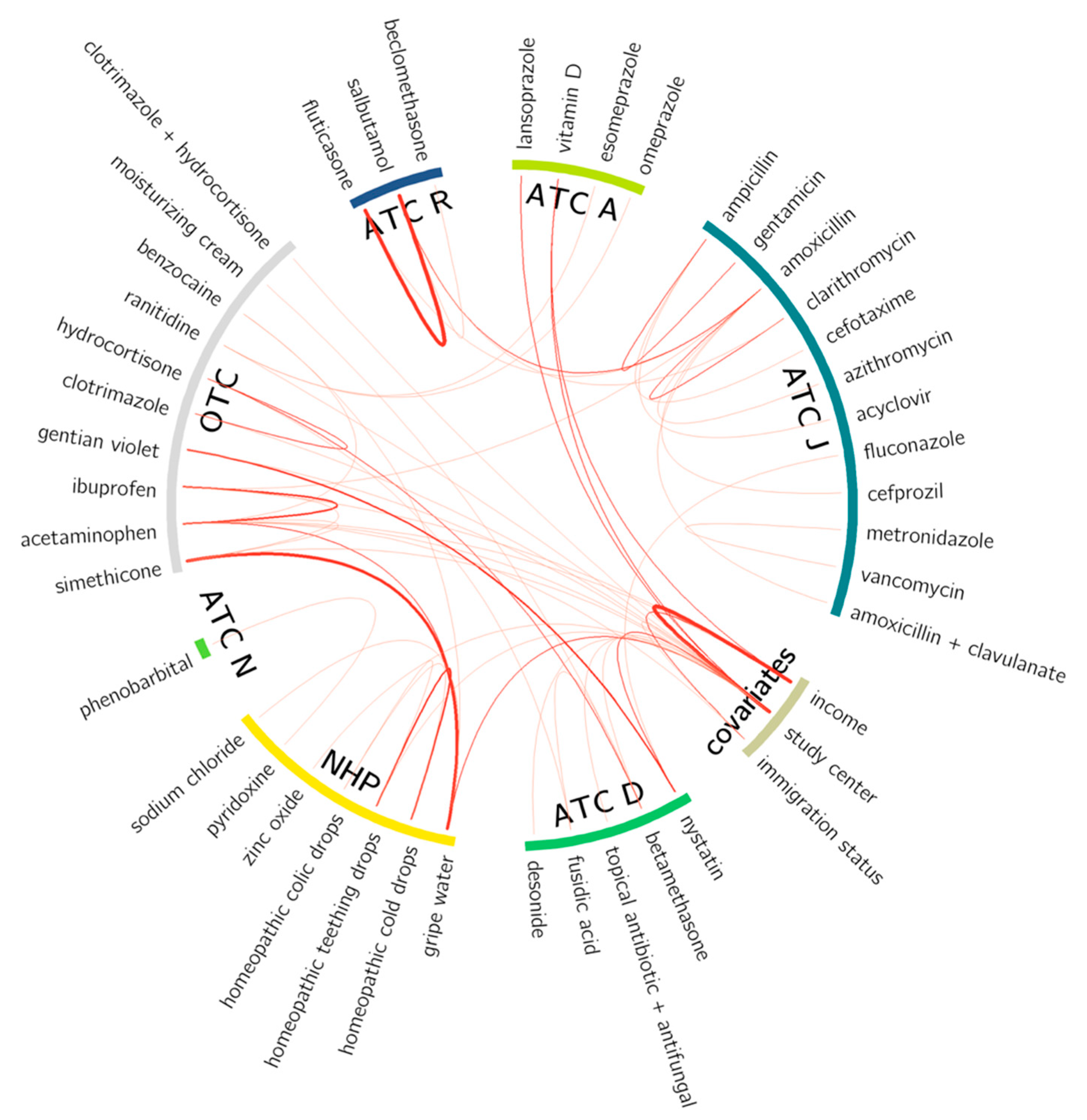
- Krzywinski, M.; Schein, J.; Birol, I.; Connors, J.; Gascoyne, R.; Horsman, D.; Jones, S.J.; Marra, M.A. Circos: An information aesthetic for comparative genomics. Genome Res. 2009, 19, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Smith, M.A.; Camp, P.G.; Shajari, S.; MacLeod, S.M.; Carleton, B.C. Prescription drug dispensing profiles for one million children: A population-based analysis. Eur. J. Clin. Pharmacol. 2013, 69, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Kit, B.K.; Gu, Q.; Ogden, C.L. Trends in Prescription Medication Use Among Children and Adolescents—United States, 1999–2014. JAMA 2018, 319, 2009–2020. [Google Scholar] [CrossRef] [PubMed]
- Drall, K.M.; Field, C.J.; Haqq, A.M.; de Souza, R.J.; Tun, H.M.; Morales-Lizcano, N.P.; Konya, T.B.; Guttman, D.S.; Azad, M.B.; Becker, A.B.; et al. Vitamin D supplementation in pregnancy and early infancy in relation to gut microbiota composition and C. difficile colonization: Implications for viral respiratory infections. Gut Microbes 2020, 12, 1799734. [Google Scholar] [CrossRef] [PubMed]
- Crocker, B.; Green, T.J.; I Barr, S.; Beckingham, B.; Bhagat, R.; Dabrowska, B.; Douthwaite, R.; Evanson, C.; Friesen, R.; Hydamaka, K.; et al. Very high vitamin D supplementation rates among infants aged 2 months in Vancouver and Richmond, British Columbia, Canada. BMC Public Health 2011, 11, 905. [Google Scholar] [CrossRef]
- Fegan, S.; Bassett, E.; Peng, Y.; Steel O’Connor, K. Adherence to complementary feeding recommendations for infants and implications for public health. Public Health Nutr. 2016, 19, 638–649. [Google Scholar] [CrossRef]
- Gönen, M.S.; Alaylıoğlu, M.; Durcan, E.; Özdemir, Y.; Şahin, S.; Konukoğlu, D.; Konukoğlu, O.K.; Ürkmez, S.; Küçükece, B.; Balkan, I.I.; et al. Rapid and effective vitamin D supplementation may present better clinical outcomes in COVID-19 (SARS-CoV-2) patients by altering serum INOS1, IL1B, IFNg, cathelicidin-LL37, and ICAM1. Nutrients 2021, 13, 4047. [Google Scholar] [CrossRef]
- Alpcan, A.; Tursun, S.; Kandur, Y. Vitamin D levels in children with COVID-19: A report from Turkey. Epidemiol. Infect. 2021, 149, e180. [Google Scholar] [CrossRef]
- MacDonald, N.E.; MacLeod, S.; Stanbrook, M.B.; Hébert, P.C.; Flegel, K.; Rosenfield, D. No regulatory double standard for natural health products. CMAJ 2011, 183, 2079. [Google Scholar] [CrossRef]
- Knopf, H.; Wolf, I.K.; Sarganas, G.; Zhuang, W.; Rascher, W.; Neubert, A. Off-label medicine use in children and adolescents: Results of a population-based study in Germany. BMC Public Health 2013, 13, 631. [Google Scholar] [CrossRef] [Green Version]
- Lizano-Díez, I.; Kargodorian, J.; Piñero-López, M.Á.; Lastra, C.F.; Mariño, E.L.; Modamio, P. Off-label drug use in neonates and infants in Spain: A five-year observational study. Pharmacoepidemiol. Drug Saf. 2022, 31, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Kimland, E.; Odlind, V. Off-label drug use in pediatric patients. Clin Pharmacol Ther. 2012, 91, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Yackey, K.; Stukus, K.; Cohen, D.; Kline, D.; Zhao, S.; Stanley, R. Off-label medication prescribing patterns in pediatrics: An update. Hosp. Pediatr. 2019, 9, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Council of Canadian Academies. Improving Medicines for Children in Canada; The Expert Panel on Therapeutic Products for Infants, Children, and Youth; Council of Canadian Academies: Ottawa, ON, Canada, 2014; Available online: http://www.scienceadvice.ca/uploads/eng/assessments%20and%20publications%20and%20news%20releases/therapeutics/therapeutics_fullreporten.pdf (accessed on 4 July 2015).
- Vernacchio, L.; Kelly, J.P.; Kaufman, D.W.; Mitchell, A.A. Medication use among children <12 years of age in the United States: Results from the Slone Survey. Pediatrics 2009, 124, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Kogan, M.D.; Pappas, G.; Yu, S.M.; Kotelchuck, M. Over-the-counter medication use among US preschool-age children. JAMA 1994, 272, 1025–1030. [Google Scholar] [CrossRef]
- Canadian Pediatric Society. Fever and Temperature Taking. Caring for Kids. Published September 2013. Available online: http://www.caringforkids.cps.ca/handouts/fever_and_temperature_taking (accessed on 29 March 2015).
- Un Lam, C.; Hsu, C.Y.S.; Yee, R.; Koh, D.; Lee, Y.S.; Chong, M.F.F.; Cai, M.; Kwek, K.; Saw, S.M.; Gluckman, P.; et al. Early-life factors affect risk of pain and fever in infants during teething periods. Clin. Oral Investig. 2016, 20, 1861–1870. [Google Scholar] [CrossRef]
- Thompson, K.; Huntington, M.K. Methods of Symptomatic Relief of Teething in Infants and Young Children Recommended by South Dakota Physicians. SD Med. 2019, 72, 509–512. [Google Scholar]
- Stagnara, J.; Besse, P.; El Kebir, S.; Bordet, M.F. Symptoms associated with teething and response to three treatments, including homeopathic medicine: A multicenter prospective observational study among 190 French pediatricians. Minerva Pediatr. 2018, 70, 519–528. [Google Scholar] [CrossRef]
- Barnes, P.M.; Bloom, B.; Nahin, R.L. Complementary and alternative medicine use among adults and children: United States, 2007. Natl. Health Stat. Rep. 2008, 12, 1–23. [Google Scholar]
- Ekins-Daukes, S.; Helms, P.J.; Taylor, M.W.; Simpson, C.R.; McLay, J.S. Paediatric homoeopathy in general practice: Where, when and why? Br. J. Clin. Pharmacol. 2005, 59, 743–749. [Google Scholar] [CrossRef]
- Kemper, K.J.; Vohra, S.; Walls, R. The use of complementary and alternative medicine in pediatrics. Pediatrics 2008, 122, 1374–1386. [Google Scholar] [CrossRef]
- Godwin, M.; Crellin, J.; Mathews, M.; Chowdhury, N.L.; Newhook, L.A.; Pike, A.; McCrate, F.; Law, R. Use of natural health products in children: Survey of parents in waiting rooms. Can. Fam. Physician 2013, 59, e364–e371. [Google Scholar] [PubMed]
- Van Howe, R.S.; Storms, M.R. Gastroesophageal reflux symptoms in infants in a rural population: Longitudinal data over the first six months. BMC Pediatr. 2010, 10, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Study Participants, n (%) |
|---|---|
| Sex | |
| Female | 1447 (47.4) |
| Male | 1603 (52.6) |
| Season of birth | |
| Winter | 753 (24.7) |
| Spring | 816 (26.8) |
| Summer | 763 (25.0) |
| Autumn | 718 (23.5) |
| Year of birth | |
| 2009 | 62 (2.0) |
| 2010 | 779 (25.5) |
| 2011 | 1669 (54.7) |
| 2012 | 540 (17.7) |
| Study center | |
| Vancouver | 679 (22.3) |
| Edmonton | 717 (23.5) |
| Manitoba | 922 (30.2) |
| Toronto | 732 (24.0) |
| Parental socioeconomic status | |
| Low income (USD 0–29,999) | 132 (4.3) |
| Middle income (USD 30,000–99,999) | 1133 (37.1) |
| High income (≥ USD 100,000) | 1417 (46.4) |
| Did not answer | 368 (12.2) |
| Maternal time lived in Canada | |
| <5 years | 216 (7.1) |
| ≥5 years | 2763 (90.6) |
| Did not answer | 71 (2.3) |
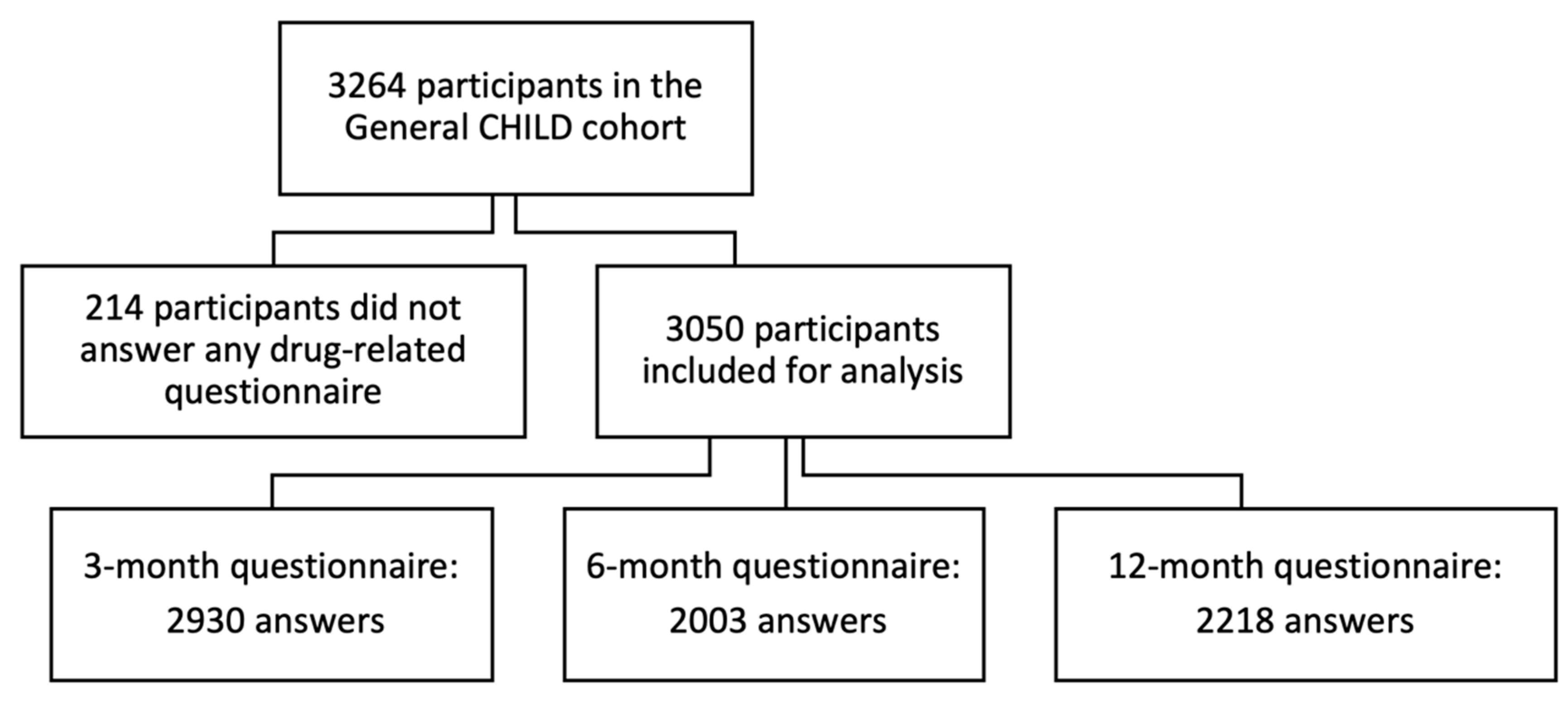
| Type | 0–3 Months | 4–6 Months | 7–12 Months | 0–12 Months |
|---|---|---|---|---|
| (n = 2930) | (n = 2003) | (n = 2218) | (n = 3050) | |
| Pharmaceutical products, n (%) | 2449 (83.6) | 1697 (84.7) | 1983 (89.4) | 2927 (96.0) |
| Prescription drugs | 536 (18.3) | 235 (11.7) | 556 (25.1) | 1036 (34.0) |
| OTC drugs | 1391(47.5) | 1150 (57.4) | 1538 (69.3) | 2349(77.0) |
| NHPs | 1894 (64.6) | 1213 (60.6) | 1205 (54.3) | 2433 (79.8) |
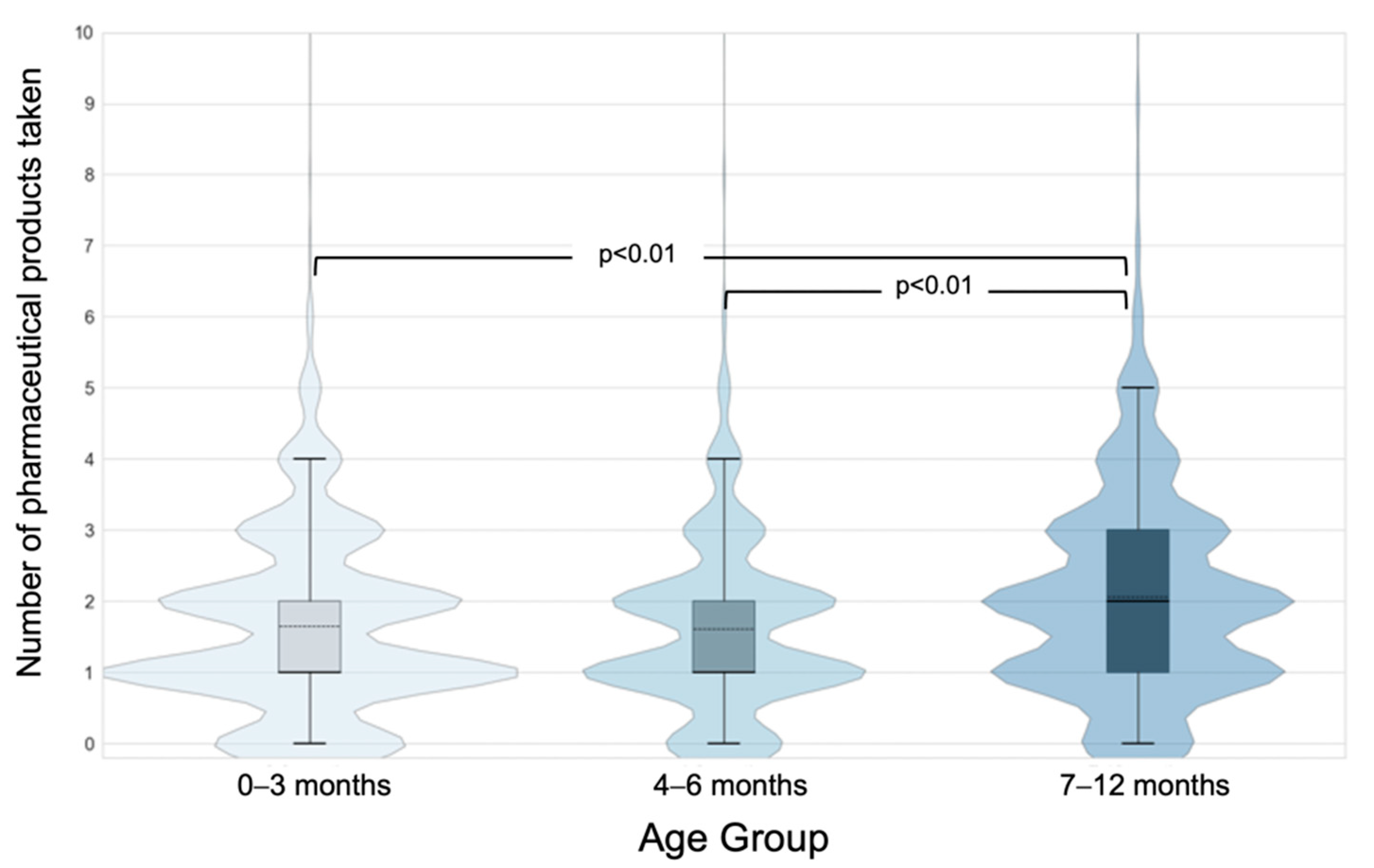
| Mean number of products, per child (SD) | 1.65 (1.28) | 1.61 (1.21) | 2.07 (1.48) | 2.99 (1.93) |
| Prescription drugs | 0.24 (0.58) | 0.16 (0.51) | 0.38 (0.82) | 0.56 (1.00) |
| OTC drugs | 0.60 (0.74) | 0.73 (0.76) | 1.00 (0.84) | 1.28 (1.03) |
| NHPs | 0.77 (0.7) | 0.69 (0.65) | 0.63 (0.68) | 1.07 (0.83) |
| Product | ATC Code | Type | Prevalence of Use (%) | Most Common Reported Reasons for Use | |||
|---|---|---|---|---|---|---|---|
| 0–3 m | 4–6 m | 7–12 m | 0–12 m | ||||
| (n = 2930) | (n = 2003) | (n = 2218) | (n = 3050) | ||||
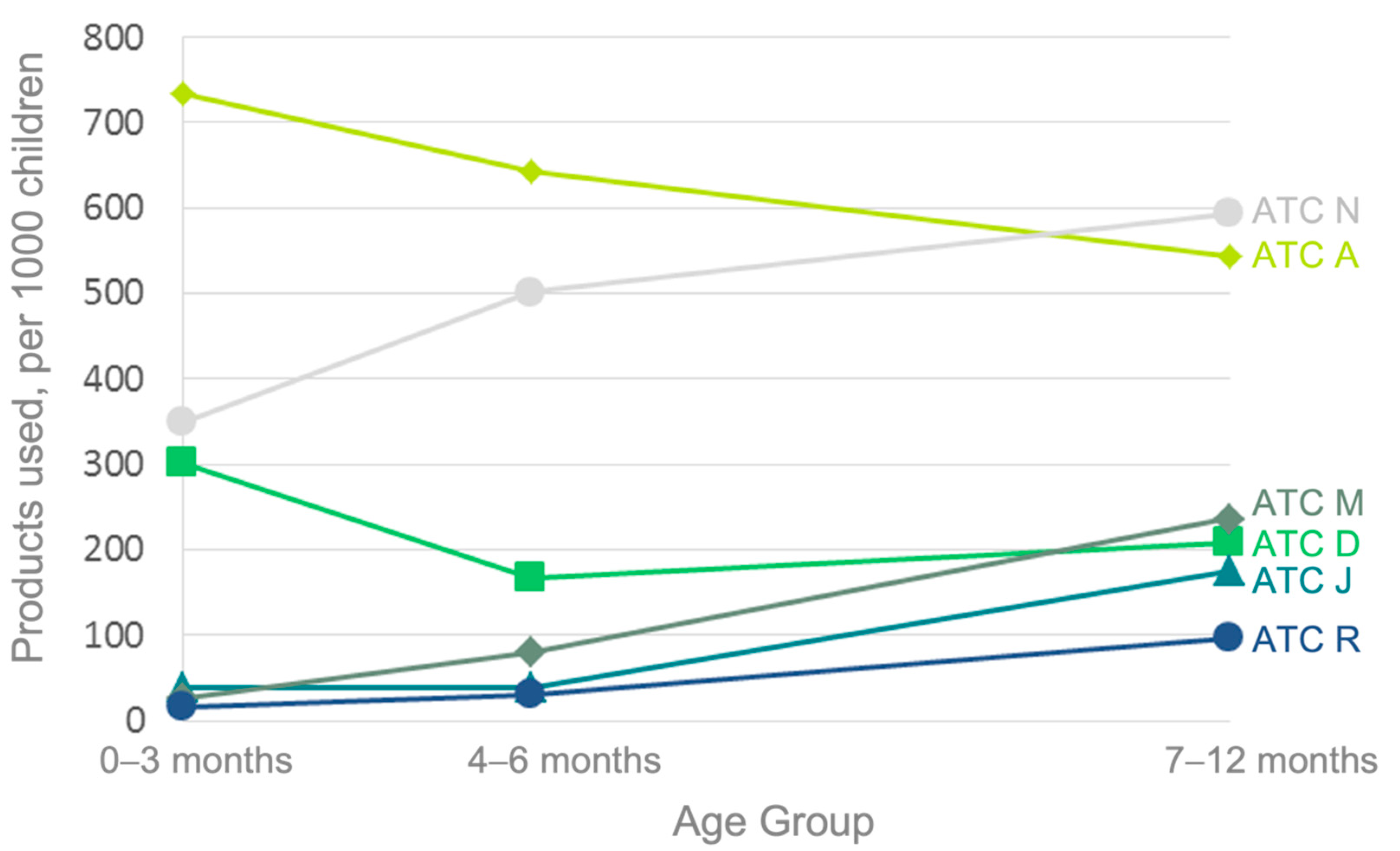
| Vitamin D | A (A11CC) | NHP | 66.2 | 56.9 | 50.1 | 78.7 | Supplement |
| Acetaminophen | N (N02BE01) | OTC | 33.9 | 49.7 | 58.7 | 67.3 | Discomfort, teething |
| Ibuprofen | M (M01AE01) | OTC | 2.6 | 8 | 23.5 | 20.4 | Discomfort, teething |
| Topical hydrocortisone | D (D07XA01) | OTC | 5.6 | 5.2 | 6.9 | 11.3 | Eczema, rash |
| Amoxicillin | J (J01CA04) | Rx | 1.2 | 2.2 | 11 | 9.7 | Ear infection |
| Nystatin | D (D01AA01) | Rx | 8.2 | 1.8 | 2.2 | 9.7 | Candidiasis |
| Simethicone | A (A03AX13) | OTC | 7.6 | 2.7 | 0.6 | 8.4 | Gas |
| Gripe water | N/A | NHP | 6.3 | 2.7 | 0.9 | 7.3 | Gas |
| Topical zinc oxide | D (D02AB) | NHP | 4.6 | 1.6 | 2.2 | 6.3 | Rash, diaper dermatitis |
| Topical clotrimazole | D (D01AC01) | OTC | 3.2 | 0.6 | 1.9 | 4.6 | Rash, diaper dermatitis |
| Homeopathic teething drops | N/A | NHP | 0.7 | 2.9 | 3.5 | 4.5 | Discomfort, teething |
| Ranitidine | A (A02BA02) | OTC | 3.7 | 2.1 | 0.9 | 4.2 | Gastroesophageal reflux |
| Salbutamol | R (R03AC02) | Rx | 0.9 | 1.3 | 3.2 | 3.5 | Wheezing |
| Sodium chloride | N/A | OTC | 1.9 | 1 | 1.4 | 3.2 | Nasal congestion |
| Homeopathic cold drops | N/A | NHP | 1 | 1.1 | 1.9 | 2.7 | Common cold |
| Diphenhydramine | D (D04AA32) | OTC | 0.1 | 0.6 | 2.6 | 2.3 | Allergy |
| Topical benzocaine | N (N01BA05) | OTC | 0.3 | 1.8 | 1.3 | 2.1 | Discomfort, teething |
| Topical fusidic acid | D (D06AX01) | Rx | 1 | 0.5 | 0.9 | 2 | Rash |
| Topical erythromycin | S (S01AA17) | Rx | 1.1 | 0.3 | 0.5 | 1.6 | Eye infection |
| Lansoprazole | A (A02BC03) | Rx | 1 | 0.9 | 0.7 | 1.5 | Gastroesophageal reflux |
| Dexamethasone | C (C05AA09) | Rx | 0.2 | 0.2 | 1.7 | 1.5 | Croup |
| Topical polymyxin B + gramicidin | S (S01AA30) | OTC | 0.8 | 0.6 | 0.6 | 1.5 | Eye infection |
| Clarithromycin | J (J01FA09) | Rx | 0.1 | 0.2 | 1.7 | 1.4 | Bronchitis |
| Homeopathic teething tablets | N/A | NHP | 0.2 | 1 | 0.9 | 1.4 | Teething |
| Probiotics | A * | NHP | 1 | 0.6 | 0.3 | 1.4 | Intestinal flora |
| Fluticasone | R (R01AD08) | Rx | 0.2 | 0.5 | 1.4 | 1.3 | Wheezing |
| Gentian violet | D (D01046) | OTC | 1.4 | 0.2 | 0 | 1.3 | Candidiasis |
| Moisturizing creams | D * | OTC | 0.5 | 0.8 | 0.4 | 1.2 | Dry skin |
| Cephalexin | J (J01DB01) | Rx | 0.3 | 0.3 | 0.8 | 1.1 | Urinary tract infection, skin infection |
| Azithromycin | J (J01FA10) | Rx | 0.1 | 0.2 | 1.2 | 1 | Ear infection, chest infection |
| Topical betamethasone | D (D07AC01) | Rx | 0.3 | 0.3 | 0.7 | 1 | Eczema, rash |
| Homeopathic colic drops | N/A | NHP | 0.9 | 0.3 | 0.1 | 1 | Gas, colic |
| Type | 0–3 Months | 4–6 Months | 7–12 Months | 0–12 Months |
|---|---|---|---|---|
| Pharmaceutical products used, n | 4825 | 3221 | 4587 | 9127 |
| Off-label drugs, n (%) | 535 (11.2) | 317 (9.9) | 471 (10.4) | 1342(14.7) |
| NHPs and unlabeled products | 2267 (47.0) | 1383 (43.0) | 1404 (30.6) | 3267(35.8) |
| Prescription drugs used, n | 696 | 319 | 836 | 1705 |
| Off-label prescription drugs, n (%) | 189 (27.2) | 142 (44.5) | 233 (27.9) | 493 (28.9) |
| OTC drugs used, n | 1769 | 1469 | 2215 | 3895 |
| Off-label OTC drugs, n (%) | 346 (19.6) | 175 (11.9) | 238 (10.7) | 849 (21.8) |
| Medication Unknown, n | 93 | 50 | 132 | 260 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedard, P.; Winsor, G.L.; Garlock, E.S.; Azad, M.B.; Becker, A.B.; Mandhane, P.J.; Moraes, T.J.; Sears, M.R.; Turvey, S.E.; Subbarao, P.; et al. From Prescription Drugs to Natural Health Products: Medication Use in Canadian Infants. Children 2022, 9, 1475. https://doi.org/10.3390/children9101475
Bedard P, Winsor GL, Garlock ES, Azad MB, Becker AB, Mandhane PJ, Moraes TJ, Sears MR, Turvey SE, Subbarao P, et al. From Prescription Drugs to Natural Health Products: Medication Use in Canadian Infants. Children. 2022; 9(10):1475. https://doi.org/10.3390/children9101475
Chicago/Turabian StyleBedard, Pascal, Geoffrey L. Winsor, Emma S. Garlock, Meghan B. Azad, Allan B. Becker, Piush J. Mandhane, Theo J. Moraes, Malcolm R. Sears, Stuart E. Turvey, Padmaja Subbarao, and et al. 2022. "From Prescription Drugs to Natural Health Products: Medication Use in Canadian Infants" Children 9, no. 10: 1475. https://doi.org/10.3390/children9101475