
Effects of Robotic Interactive Gait Training Combined with Virtual Reality and Augmented Reality on Balance, Gross Motor Function, Gait Kinetic, and Kinematic Characteristics in Angelman Syndrome: A Case Report

Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Description
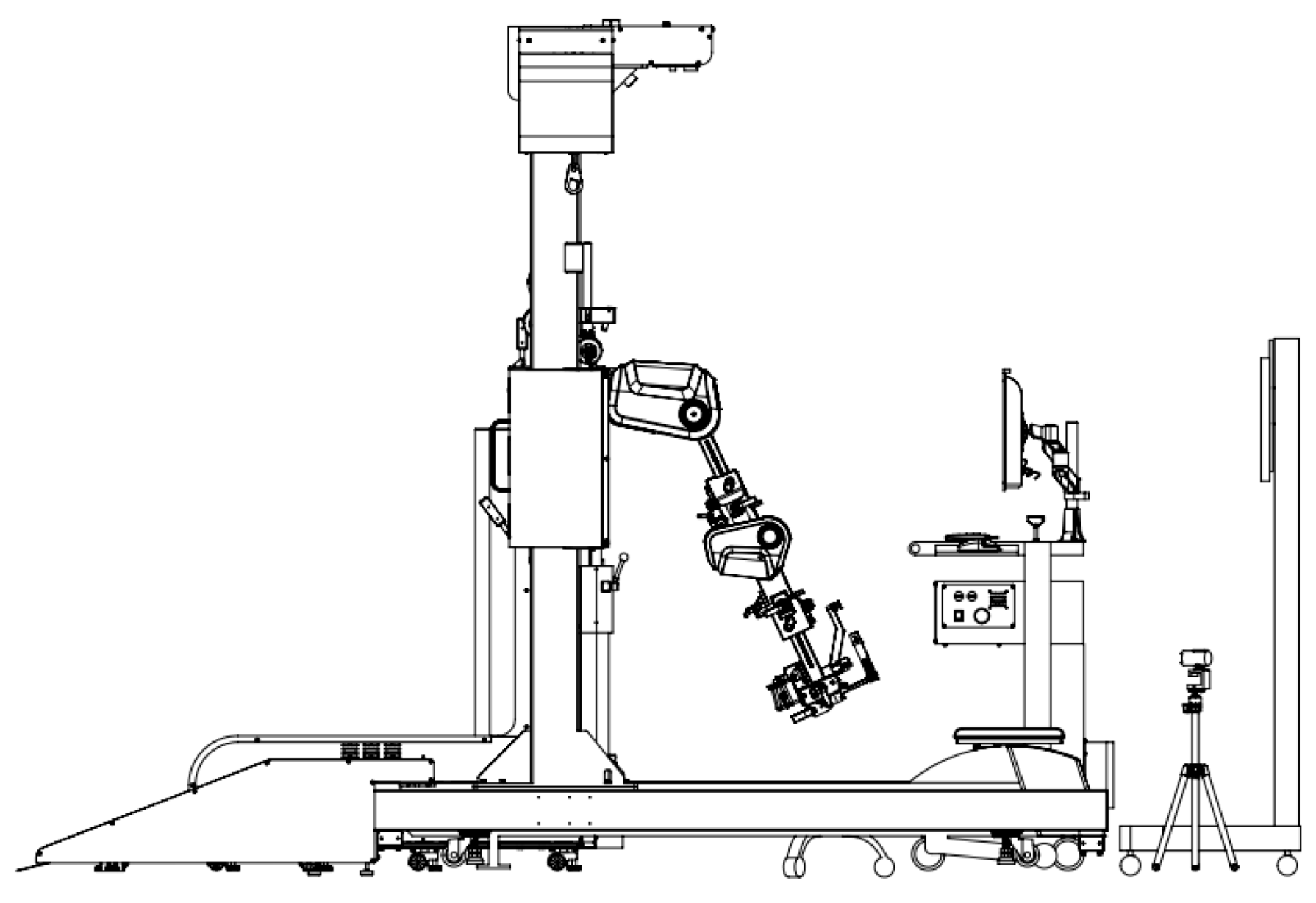
2.2. Robotic Interactive Gait-Training System
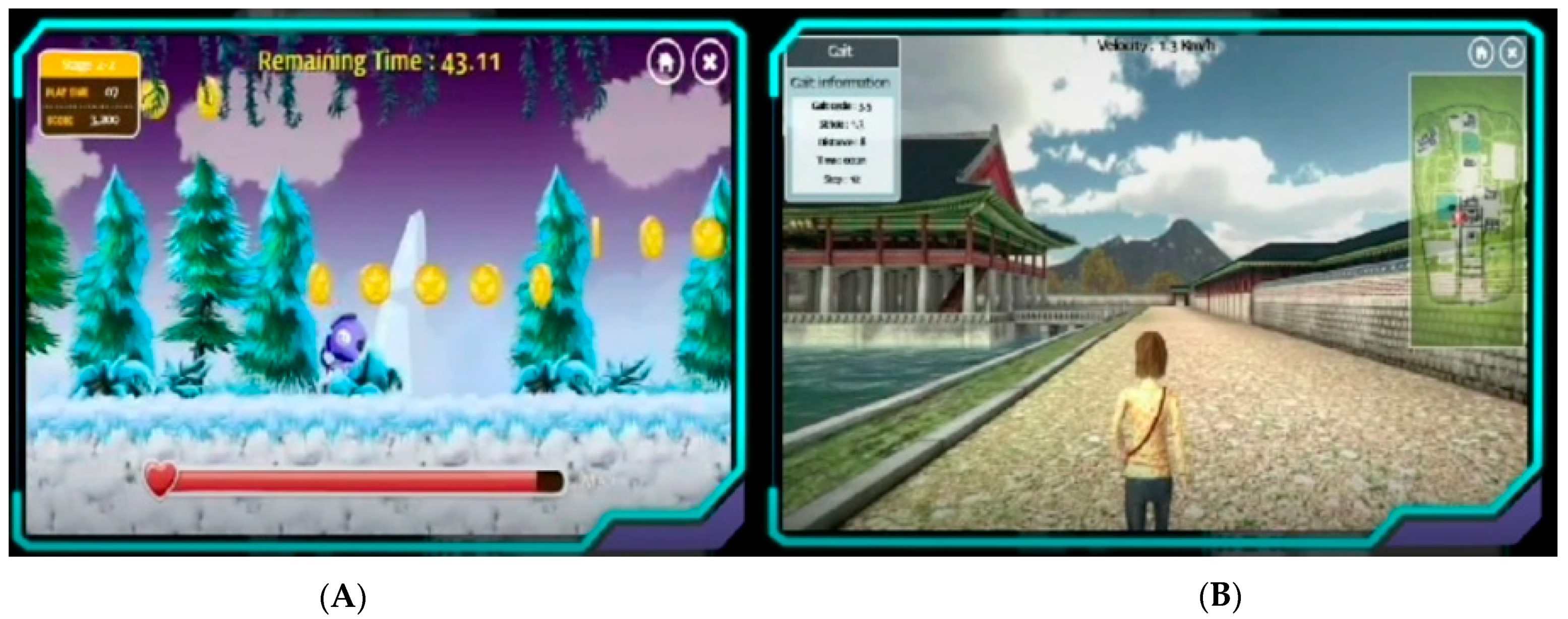
2.3. Experimental Task and Procedures
2.4. Clinical Outcome Measurements
2.4.1. Tinetti Performance-Oriented Mobility Assessment
2.4.2. Gross Motor Function Measures
2.4.3. Pediatric Balance Scale
2.4.4. Short Fall Efficacy Scale
2.4.5. Biomechanical Measurement
3. Results
3.1. Clincial Outcome Measurements
3.2. Biomechanics Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buiting, K.; Williams, C.; Horsthemke, B. Angelman syndrome—Insights into a rare neurogenetic disorder. Nat. Rev. Neurol. 2016, 12, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.A. Angelman syndrome: Consensus for diagnostic criteria. Am. J. Med. Genet. 1995, 56, 237–238. [Google Scholar] [CrossRef] [PubMed]
- Heald, M.; Adams, D.; Walls, E.; Oliver, C. Refining the Behavioral Phenotype of Angelman Syndrome: Examining Differences in Motivation for Social Contact between Genetic Subgroups. Front. Behav. Neurosci. 2021, 15, 10. [Google Scholar] [CrossRef]
- Williams, C.A.; Driscoll, D.J.; Dagli, A.I. Clinical and genetic aspects of Angelman syndrome. Genet. Med. 2010, 12, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Thibert, R.L.; Larson, A.M.; Hsieh, D.T.; Raby, A.R.; Thiele, E.A. Neurologic manifestations of Angelman syndrome. Pediatr. Neurol. 2013, 48, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.J.; Palisano, R.J. Physical therapists’ perceptions of factors influencing the acquisition of motor abilities of children with cerebral palsy: Implications for clinical reasoning. Phys. Ther. 2002, 82, 237–248. [Google Scholar] [CrossRef]
- Lowe, L.; McMillan, A.G.; Yates, C. Body weight support treadmill training for children with developmental delay who are ambulatory. Pediatr. Phys. Ther. 2015, 27, 386. [Google Scholar] [CrossRef] [Green Version]
- Schlittler, D.X.C.; Lopes, T.F.; Raniero, E.P.; Barela, J.A. Treadmill training effects on walking acquisition and motor development in infants at risk of developmental delay. Rev. Paul. Pediatr. 2011, 29, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Oh-Park, M.; Dohle, C.; Bialek, A.; Friel, K.; Edwards, D.; Krebs, H.I.; You, J.S.H. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. NeuroRehabilitation 2020, 46, 577–587. [Google Scholar] [CrossRef]
- Hwang, J.; Shin, Y.; Park, J.H.; Cha, Y.J.; You, J.S.H. Effects of Walkbot gait training on kinematics, kinetics, and clinical gait function in paraplegia and quadriplegia. NeuroRehabilitation 2018, 42, 481–489. [Google Scholar] [CrossRef]
- Kim, S.Y.; Yang, L.; Park, I.J.; Kim, E.J.; Park, M.S.; You, S.H.; Kim, Y.H.; Ko, H.Y.; Shin, Y.I. Effects of innovative WALKBOT robotic-assisted locomotor training on balance and gait recovery in hemiparetic stroke: A prospective, randomized, experimenter blinded case control study with a four-week follow-up. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.; Reid, D. The influence of virtual reality play on children’s motivation. Can. J. Occup. Ther. 2005, 72, 21–29. [Google Scholar] [CrossRef] [PubMed]
- An, Y.; Park, C. The effects of virtual soccer game on balance, gait function, and kick speed in chronic incomplete spinal cord injury: A randomized controlled trial. Spinal Cord 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Allcoat, D.; Von Mühlenen, A. Learning in virtual reality: Effects on performance, emotion and engagement. Res. Learn. Technol. 2018, 26, 2140. [Google Scholar] [CrossRef] [Green Version]
- Park, C.; Oh-Park, M.; Bialek, A.; Friel, K.; Edwards, D.; You, J.S.H. Abnormal synergistic gait mitigation in acute stroke using an innovative ankle–knee–hip interlimb humanoid robot: A preliminary randomized controlled trial. Sci. Rep. 2021, 11, 22823. [Google Scholar] [CrossRef]
- Jin, L.H.; Yang, S.S.; Choi, J.Y.; Sohn, M.K. The effect of robot-assisted gait training on locomotor function and functional capability for daily activities in children with cerebral palsy: A single-blinded, randomized cross-over trial. Brain Sci. 2020, 10, 801. [Google Scholar] [CrossRef]
- Park, C.; Hwang, J.; You, J.S.H. Comparative effectiveness of robot-interactive gait training with and without ankle robotic control in patients with brain damage. J. Mech. Med. Biol. 2021, 21, 2140035. [Google Scholar] [CrossRef]
- Canbek, J.; Fulk, G.; Nof, L.; Echternach, J. Test-retest reliability and construct validity of the tinetti performance-oriented mobility assessment in people with stroke. J. Neurol. Phys. Ther. 2013, 37, 14–19. [Google Scholar] [CrossRef]
- Bodkin, A.W.; Robinson, C.; Perales, F.P. Reliability and validity of the gross motor function classification system for cerebral palsy. Pediatr. Phys. Ther. 2003, 15, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.L.; Shen, I.H.; Chen, C.Y.; Wu, C.Y.; Liu, W.Y.; Chung, C.Y. Validity, responsiveness, minimal detectable change, and minimal clinically important change of Pediatric Balance Scale in children with cerebral palsy. Res. Dev. Disabil. 2013, 34, 916–922. [Google Scholar] [CrossRef]
- Kempen, G.I.; Yardley, L.; Van Haastregt, J.C.; Zijlstra, G.R.; Beyer, N.; Hauer, K.; Todd, C. The Short FES-I: A shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing 2008, 37, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faber, M.J.; Bosscher, R.J.; van Wieringen, P.C. Clinimetric properties of the performance-oriented mobility assessment. Phys. Ther. 2006, 86, 944–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Mahmud, A.; Soysa, A.I. POMA: A tangible user interface to improve social and cognitive skills of Sri Lankan children with ASD. Int. J. Hum. Comput. Stud. 2020, 144, 102486. [Google Scholar] [CrossRef]
- Tinetti, M.; Williams, T.; Mayewski, R. Is the Tinetti Performance Oriented Mobility Assessment (POMA) a feasible and valid predictor of short-term fall risk in nursing home residents with dementia. J. Am. Geriatr. Soc. 1986, 3, 119–126. [Google Scholar] [CrossRef]
- Russell, D.J.; Rosenbaum, P.L.; Cadman, D.T.; Gowland, C.; Hardy, S.; Jarvis, S. The gross motor function measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.J.; Rosenbaum, P.; Wright, M.; Avery, L.M. Gross Motor Function Measure (GMFM-66 & GMFM-88) User’s Manual; Mac Keith Press: London, UK, 2002. [Google Scholar]
- Franjoine, M.R.; Darr, N.; Held, S.L.; Kott, K.; Young, B.L. The performance of children developing typically on the pediatric balance scale. Pediatr. Phys. Ther. 2010, 22, 350–359. [Google Scholar] [CrossRef] [Green Version]
- Franjoine, M.R.; Gunther, J.S.; Taylor, M.J. Pediatric balance scale: A modified version of the berg balance scale for the school-age child with mild to moderate motor impairment. Pediatr. Phys. Ther. 2003, 15, 114–128. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, S.A. Assessment of fear of falling in older adults: The falls efficacy scale-international (FES-I). Disabil. Rehabil. 2011, 29, 155–162. [Google Scholar]
- Jung, J.H.; Lee, N.G.; You, J.H.; Lee, D.C. Validity and feasibility of intelligent Walkbot system. Electron. Lett. 2009, 45, 1016–1017. [Google Scholar] [CrossRef]
- Van Tran, Q.; Kim, S.; Lee, K.; Kang, S.; Ryu, J. Force/torque sensorless impedance control for indirect driven robot-aided gait rehabilitation system. In Proceedings of the 2015 IEEE International Conference on Advanced Intelligent Mechatronics (AIM), Busan, Korea, 7–11 July 2015; pp. 652–657. [Google Scholar]
- Lee, D.R.; Shin, Y.K.; Park, J.H.; You, J.H. Concurrent validity and test-retest reliability of the walkbot-K system for robotic gait training. J. Mech. Med. Biol. 2016, 16, 1640029. [Google Scholar] [CrossRef] [Green Version]
- Cesar, G.M.; Buster, T.W.; Burnfield, J.M. Cardiorespiratory fitness, balance and walking improvements in an adolescent with cerebral palsy (GMFCS II) and autism after motor-assisted elliptical training. Eur. J. Physiother. 2020, 22, 124–132. [Google Scholar] [CrossRef]
- Yazıcı, M.; Livanelioğlu, A.; Gücüyener, K.; Tekin, L.; Sümer, E.; Yakut, Y. Effects of robotic rehabilitation on walking and balance in pediatric patients with hemiparetic cerebral palsy. Gait Posture 2019, 70, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Sukal-Moulton, T.; Clancy, T.; Zhang, L.-Q.; Gaebler-Spira, D. Clinical application of a robotic ankle training program for cerebral palsy compared to the research laboratory application: Does it translate to practice? Arch. Phys. Med. Rehabil. 2014, 95, 1433–1440. [Google Scholar] [CrossRef] [Green Version]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Effect of robotic-assisted gait rehabilitation on dynamic equilibrium control in the gait of children with cerebral palsy. Gait Posture 2018, 60, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Johansson, B.B. Brain plasticity and stroke rehabilitation: The Willis lecture. Stroke 2000, 31, 223–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Sex | Male |
|---|---|
| Age (years) | 15 |
| Height (cm) | 148 |
| Weight (kg) | 43 |
| GMFCS 1 level | II |
| CARS 2 | 38 (moderate autism) |
| FIM 3 cognitive section | 17/35 |
| Pretest | Post-Test | |
|---|---|---|
| POMA 1 | 12 | 15 |
| GMFM 2 | 43 | 48 |
| PBS 3 | 1 | 32 |
| sFES 4 | 16 | 19 |
| Hip | Pre-Test | Post-Test |
|---|---|---|
| Joint torque (Lt 1/Rt. 2) | 8.80/6.10 | 10.20/12.30 |
| Active force (Lt./Rt.) | 3.23/2.81 | 5.67/8.30 |
| Resistive force (Lt./Rt.) | 25.31/22.60 | 17.76/16.31 |
| Joint kinematics (Lt./Rt.) | 10.69/10.20 | 14.44/11.76 |
| Knee | ||
| Joint torque (Lt./Rt.) | 8.10/9.30 | 10.40/12.30 |
| Active force (Lt./Rt.) | 6.56/7.10 | 11.42/16.32 |
| Resistive force (Lt./Rt.) | 11.70/10.80 | 6.50/8.50 |
| Joint kinematics (Lt./Rt.) | 21.56/29.40 | 28.33/30.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.; Park, C.; You, J.H. Effects of Robotic Interactive Gait Training Combined with Virtual Reality and Augmented Reality on Balance, Gross Motor Function, Gait Kinetic, and Kinematic Characteristics in Angelman Syndrome: A Case Report. Children 2022, 9, 544. https://doi.org/10.3390/children9040544
Han S, Park C, You JH. Effects of Robotic Interactive Gait Training Combined with Virtual Reality and Augmented Reality on Balance, Gross Motor Function, Gait Kinetic, and Kinematic Characteristics in Angelman Syndrome: A Case Report. Children. 2022; 9(4):544. https://doi.org/10.3390/children9040544
Chicago/Turabian StyleHan, Sangkeun, Chanhee Park, and Joshua (Sung) H. You. 2022. "Effects of Robotic Interactive Gait Training Combined with Virtual Reality and Augmented Reality on Balance, Gross Motor Function, Gait Kinetic, and Kinematic Characteristics in Angelman Syndrome: A Case Report" Children 9, no. 4: 544. https://doi.org/10.3390/children9040544