
Care Coordination Needs of Families of Children with Down Syndrome: A Scoping Review to Inform Development of mHealth Applications for Families


Abstract
:1. Introduction
2. Methods
2.1. Protocol
2.2. Eligibility Criteria
- Articles appearing in peer reviewed journals;
- Research implementing any study methodology and design;
- Published in journals between January 2010 and January 2020;
- English language;
- Study population includes caregivers of children with DS birth to twenty-one years old;
- Article addresses health management of child with DS, including dental management;
- Article reports results reflecting perspectives of parents.
- Not research;
- Age of child with DS not reported;
- Focused exclusively on educational management of a child with DS;
- Did not differentiate children with DS from other possible conditions included in the sample;
- Focused exclusively on the prenatal period or diagnosis experience;
- Review articles;
- Reporting only the providers’ perspective.
2.3. Information Sources
2.4. Search
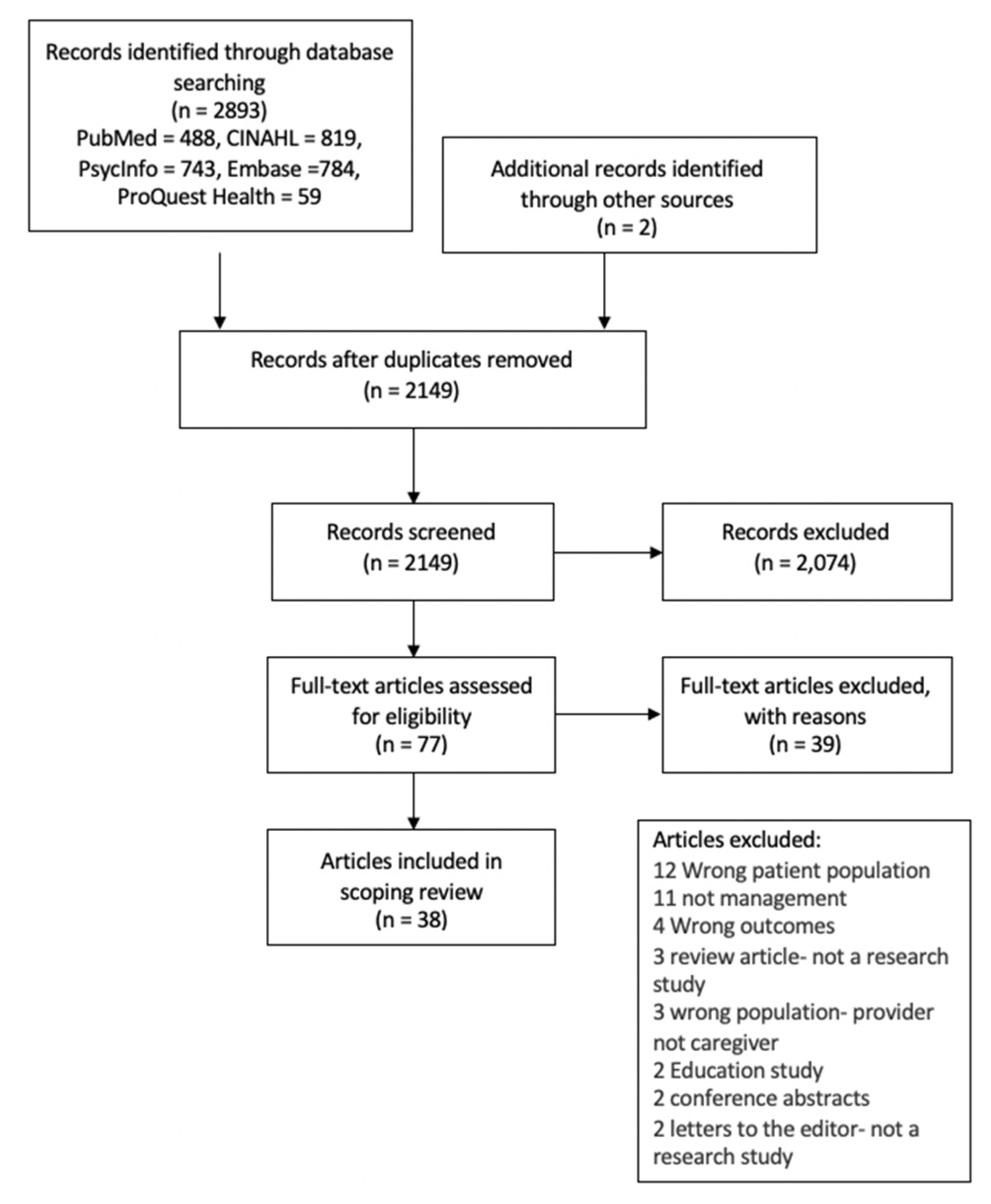
2.5. Selection of Sources of Evidence
2.6. Charting the Data
2.7. Collating and Summarizing Data
3. Results
3.1. Characteristics of Sources of Evidence
3.2. Study Design
3.3. Measures
3.4. Analysis
3.5. Respondents
3.6. Age of Children with DS
3.7. Study Purpose
4. Research Question One
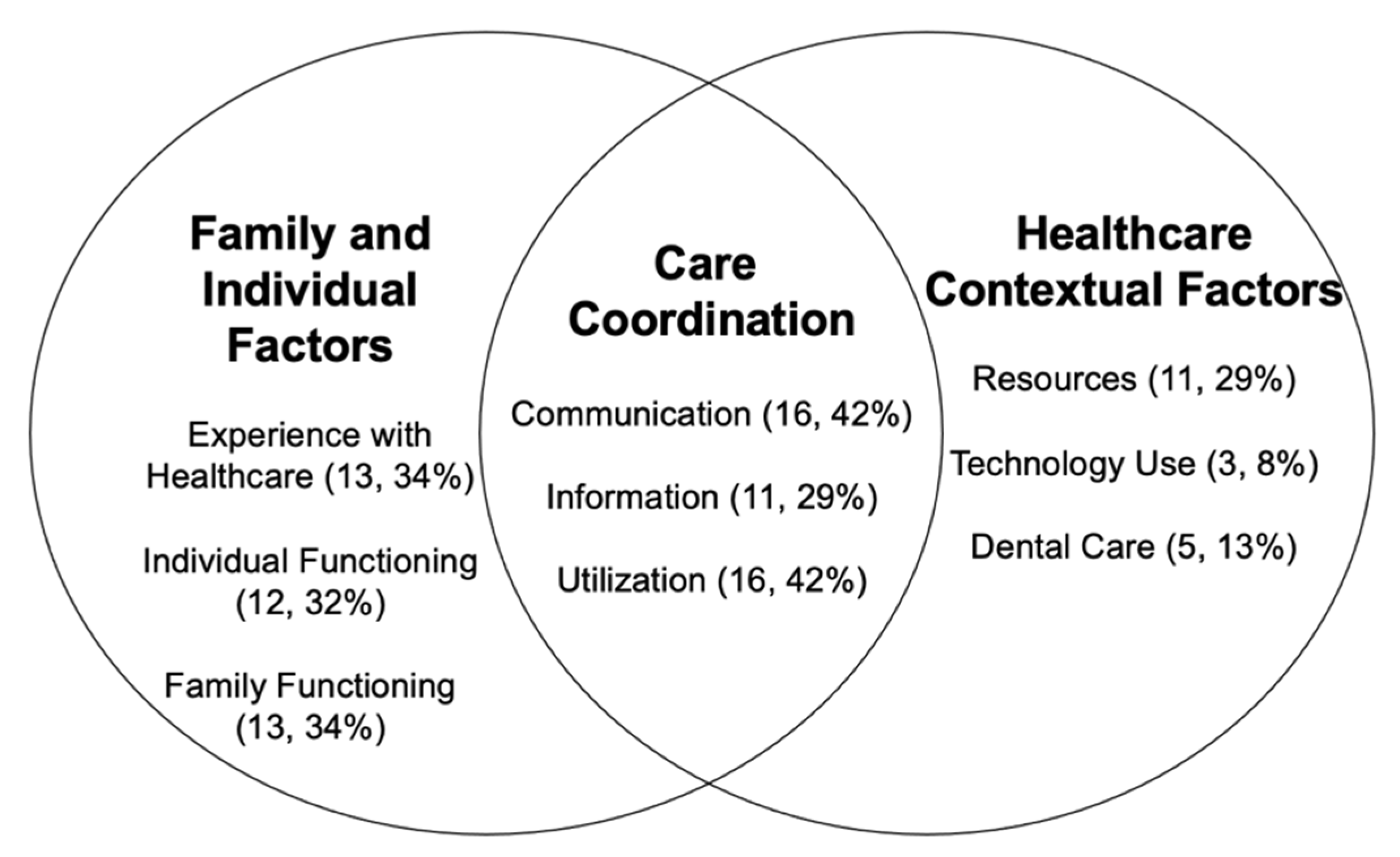
5. Communication
6. Information
7. Utilization
8. Experiences with Healthcare
9. Individual Functioning
10. Family Functioning
11. Resources
12. Technology Use
13. Dental Care
14. Research Question Two
15. Care Coordination Factors
16. Family and Individual Factors
17. Discussion
18. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Article First Author, Date, Country of Origin | Purpose (Direct Quote) | Design | Caregiver * | Age range of Children | Measures/Analysis | Use of Technology |
|---|---|---|---|---|---|---|
| Amitha (2015) [22] India | The study was conducted to determine the parental views, attitudes and perceptions of oral healthcare and treatment requirements among children with disabilities attending various special schools in Mangalore. | Cross-sectional survey design | 50 families | Does not specify | Researcher generated survey | |
| Barros da Silva (2018) [23] Portugal | The aim of this study was to understand the breastfeeding experiences of mothers of children with Down syndrome, and their specific practices. | Qualitative interviews | 10 mothers | 2 months to 10 years old | Interview guide | Several mothers reported using the internet to search for information regarding DS (especially if healthcare providers were negative). They also reported using internet forums and Facebook groups for support. |
| Bertoli (2011) [47] Italy | The aim of the present study is to explore the needs and challenges in health, social integration, and daily life, of people with DS living in Rome. | Mixed Methods Cross-sectional, census-based survey | 501 families 286 mothers 155 fathers 15 other caregivers | 0 to 64 years old 181 were under the age of 19, with 25 did not disclose age | Researcher generated questionnaire- National Institute of Statistics (ISTAT) household survey used as reference | |
| Cartwright (2018) [24] United Kingdom | The aim of this study was to explore the experiences of mothers of IDS regarding feeding, and to provide information to better inform health professionals caring for new mothers and their babies. | Qualitative focus groups | 8 mothers | <5 years old | Focus groups Interpretative Phenomenology | Report using the internet to find information and expressed frustration that there was little support in providing information from health professionals. |
| Choi (2019) [57] South Korea | The aim of this study was twofold: (1) to explore the feasibility of using the mHealth Family Adaptation Intervention (FamilyAdapt-DS) with families of young children with DS and (2) to address the effect of participating in this mHealth intervention on family adaptation. | One group pre-test, post-test design- survey data focus groups | 8 families 16 parents | Birth to 3 years old | FIRA-G, Family Management Measure (FaMM), and Family Problem Solving Communication (FPSC), Brief FAM: General Scale Family Member Well-Being scale | The mHealth app entitled FamilyAdapt-DS combined information on mHealth apps with the use of therapeutic conversations with both parents and nurse. |
| Choi (2015) [36] South Korea | This study examined the factors related to resilience of families of children with DS in Korea. | Cross-sectional survey design | 126 families 117 mothers 9 fathers | Average age 5.4 years old +/−3.88 | Questionnaire on resource and stress (QRS) Beck depression inventory (BDI) Emotionality, Activity, Sociability survey (EAS) Family Adaptability and Cohesion Evaluation Scale (III), Family Problem Solving and Communication Scale (FPSC) Family APGAR Stigma and Discrimination | |
| Crossman (2018) [56] United States | The following 3 aims were designed to address gaps in the existing literature: (1) To determine the trajectory of parental competence for fathers of children with DD from age 3 to age 15. (2) Controlling for child and family characteristics, determine the main effects of the family environment, EI service and informal support on paternal competence when their child with a developmental disability was 3. (3) To determine whether there were lasting effects of the family environment, EI services and informal support on differences in paternal competence. | Quantitative longitudinal analysis of secondary data | 93 fathers | 3–15 years old | Parenting Stress Index- sense of competence subscale Family Environment Scale Family Support Scale | |
| Descamps (2015) [37] Belgium | We were interested in the responses to 3 major questions: (1) what do parents know about dental care for their child with DS? (2) Have they ever been to a dentist? (3) How would they describe their experience of this dental visit? | Cross-sectional survey design | 100 families 86 mothers 14 fathers | 2–21 years old | Adapted Oral Assessment DS questionnaire Researcher generated survey | |
| Farkas (2018) [25] United States | The purpose of the present study was to extend the current literature on parents’ experiences by offering a balanced view of both the positive and negative sides of parenting a child with DS, specifically through analysis of parent perspectives. | Qualitative interviews | 435 families 361 mothers 74 fathers | 1 to 55 years old mean 9.43 years old | Grounded theory using thematic coding | |
| Gibson (2019) [26] United States | The following questions were addressed: How do participants describe their information practices and information-seeking experiences? What contextual factors contribute to defensive information? behaviors and knowledge practices described by participants? | Qualitative interview | 24 mothers | 2–26 years old | Grounded theory combining thematic analysis and constant comparative method | Trust was a major component to information seeking from online sources and the trust in maintenance of confidentiality among group participants. |
| Hall (2018) [49] United Kingdom | The objective of this study are, for children with DS, OME, and hearing loss, to (1) scope the range of current service provision across England; (2) explore professional decision making; and (3) explore patient, parent, and public views on the direction of future research. | Mixed methods design, survey, interview, and focus groups | 13 families 12 mothers 1 grandmother | Not specified | Interview guide Researcher developed survey | |
| Hall (2012) [48] United States | The purpose of this study is to follow up on findings from the focus group interviews to explore parental stress in families of children with disabilities in the context of the Resiliency Model of Stress and Adjustment. | Mixed methods, survey, focus groups | 25 families 23 mothers 3 fathers 1 grandmother | Mean age of child 9.96 (stressed family group) and 5.58 (non- stressed group) | Parenting Stress Index Short Form Content analysis for qualitative findings | |
| Hsiao (2014) [38] Taiwan | The purpose of this study was to examine how family demographics, family demands, and social support relate to family functioning, as well as the potential mediating effect of social support on the relationship between family demands and family functioning in Taiwanese families of children with DS. | Cross-sectional survey design | 83 families 80 mothers 75 fathers | 4 to 17 years old | Family Stressors Index Family Management Measure—condition management effort and family life difficulty scale Perceived Social Support Scale General Family Functioning—Family Assessment device | |
| Hubner (2016) [51] United States | This study uses a population based national sample to assess differences in both presence and degree of SDM in ASD and 2 other complex neurodevelopmental disorders—CP and Down syndrome—with adjustment for factors (child, family and health system) shown to impact SDM. | Secondary analysis | 353 families | 2–17 years old | 2009–2010 National Survey of Children with Special Health Care Needs | |
| Huiracocha (2017) [27] Ecuador | This article focuses specifically on (i) how families received a diagnosis of DS and (ii) how the families subsequently adapted and coped. | Qualitative focus-group interviews | 4 families 4 mothers 1 father 1 dyad | <2 to 16 years old | Descriptive coding | |
| Krueger (2019) [28] United States | The purpose of this study was to gain information regarding parents’ advocacy behaviors and strategies they used for their child with DS. | Qualitative survey design | 435 families 371 mothers 64 fathers | <1 to 55 years old | Triangulation | |
| Leonard (2016) [50] Australia | The aim of this study was to further understand the impact of these factors, as well as to describe the current state of parental and student engagement in transition planning in Australia | Mixed methods; qualitative and quantitative survey data | 190 families | 15–30 years old | Researcher generated survey Open ended questions as part of DS “needs opinions wishes” study Content analysis | |
| Lollar (2012) [52] United States | To describe the functional difficulties of children with special health needs and to demonstrate the shared and unique contributions in predicting health outcomes and informing therapeutic interventions, policies, and research by using data from the 2005–2006 National Survey of Children with Special Health Care Needs | Secondary data analysis | 395 families | Birth to 17 years old | 2005–2006 National Survey of Children with Special Health Care Needs Multiple regression modeling | |
| Marshall (2019) [20] United States | The purpose of our study was to examine the experiences of parents or caregivers of children with Down syndrome related to prenatal care, the birth setting, primary and specialty care and care coordination | Mixed-methods cross-sectional survey design | 101 families 93 mothers 6 fathers 2 other caregiver | 0 to 18 years old | Family Experience Survey | |
| Marshall (2014) [29] United States | Our purpose was to better understand services and supports most needed and accessed by families of children birth to age 3 who have DS, identify gaps and barriers to accessing these services. | Qualitative interviews and focus groups | 13 families 10 mothers 3 fathers | 0–3 years old | Interviews Focus group A priori coded transcripts | |
| Melvin (2018) [30] Australia | This studied aimed to (1) explore families’ experiences of communication information provision and (2) identify families’ preferences regarding when, what, and how they would like to receive information about communication. | Qualitative interviews | 9 families 5 mothers 3 fathers 1 grandmother | 0 to 15 years old | Researcher generated interview guide Thematic analysis | Parents felt that electronic resources would have saved them having to sort piles of paper which were easily lost Wanted access to a website to access information and keep track of key messages. They also wanted interactive workshops with written and video information. |
| Mengoni (2019) [39] United Kingdom | The aim of this study was to investigate whether children with Down syndrome had received recommended health checks at birth and during early childhood and whether known health conditions were monitored. | Cross-sectional survey design | 24 families | 0–5 years old | Researcher generated survey | |
| Murphy (2017) [31] Australia | This current study explored parent observations of QOL important for a sample of children with Down syndrome including children who cannot speak for themselves. | Qualitative interviews | 17 mothers | 6–18 years old | Grounded theory approach | |
| Nqcobo (2019) [40] South Africa | The aim of this study was therefore to assess the OHRQoL outcomes because of dental caries rate among CSNs. | Cross-sectional survey design and physical exam | 62 mother/child dyads | Average age 8.72 years of age | Parent-Caregiver Perception Questionnaire (P-CPQ) | |
| Nugent (2018) [41] United States | The goals of this study were to compare the prevalence of successful healthcare transition planning in adolescents with Down syndrome and adolescents with OSHCN and to examine the effect of different social and demographic factors on transition preparation. | Cross-sectional survey design | 151 families | 12–17 years old | 2009–2010 National Survey of Children with Special Health Care Needs logistical regression | |
| Nunes (2011) [32] Brazil | The objective of this study was to develop a Theoretical Model representative of the experience of families of children with DS. | Qualitative interviews | 8 families | 5–10 years old | Grounded theory and symbolic interactionism | |
| Oliveira (2010) [33] Brazil | The aim of this qualitative study was to investigate the perceptions of a group of mothers of children and adolescents with Down syndrome (DS concerning the overall health and oral health of their children. | Qualitative interviews | 19 mothers | Did not specify | content thematic analysis | |
| Parrot (2012) [42] United States | RQ1: Does diagnostic status within families relate to illness uncertainty, uncertainty management, or communication preference in families affected by NF, or Marfan or DS? RQ2: Do genetic relativism and diagnostic status interact to predict illness uncertainty, negative feelings about a condition, uncertainty management, or communication preferences in families affected by NF, or Marfan or DS? | Cross-sectional survey design | 106 families | Did not specify | Researcher generated survey | |
| Phelps (2012) [53] United States | Specifically, we sought to determine how children with DS compare with other CYSHCN with respect to national performance measures for CYSHCN measures in the NS-CSHCN, including the following: 1. Receipt of healthcare services with a medical home 2. parental perception of the quality of communication with the physician. 3. Communication of their child’s physician with other physicians and with educators and other professionals. 4.Recipt of needed care coordination. 5. Rates of unmet healthcare needs. Finally, we also sought to determine the relative burden on families of children with DS and ID when compared to other CYSHCN. | Secondary data analysis | 395 families | 0 to 17 years old | 2005–2006 National Survey of Children with Special Health Care Needs. | |
| Pikora (2014) [43] Australia | The aims of this paper were: to examine the prevalence of medical conditions and health service use among adolescents and young adults with Down syndrome; to describe the impact of these conditions open the young person’s daily life; and to explore the relationship between the presence of medical conditions and level of functioning daily life. | Cross-sectional survey design | 197 families | 15–30 years old | Index of Social Competence (ISC) Researcher Generated Survey | |
| Rahim (2014) [44] Malaysia | The main objective of this study was to assess the legal representatives’ perceptions on dental care access for DS and non-DS siblings in Malaysia. | Cross-sectional survey design | 130 families | Mean age 26.4 | Oral Assessment in Down Syndrome Questionnaire | |
| Santoro (2016) [45] United States | The purpose of this article was to describe current screening practices in patients with mDS, comparing these practices with current AAP screening practices with perceptions of physician adherence to the recommended AAP health supervision guidelines for DS. | Cross-sectional survey design | 91 families | 0–12 years old | Researcher generated survey | |
| Schieve (2011) [54] United States | In the current study, we conducted an in-depth population-based assessment of the health and functional status of children with DS, using data from the 2005–2006 National Survey of Children with Special Health Care Needs (NS-CSHCN) | Secondary data analysis | 338 families | 3–18 years old | 2005–2006National Survey of Children with Special Health Care Needs (NS-CSHCN) | |
| Sheehan (2018) [34] Ireland | This study aimed to explore the range of emotions experienced by parents in the early years of managing their child’s disability, to assess the relevance of the Dual Process Model in understanding these emotions within an adjustment process and to identify the types of support and information perceived by parents as helpful during this time. | Qualitative interviews | 6 families 5 mothers 1 father | 5–7 years old | thematic analysis | |
| Skotko (2012) [7] United States | What new diagnoses, if any, were identified in our patients with DS as a result of their visit to our clinic? How many of our new patients were up-to-date on the recommended DS healthcare screenings? And, ultimately, what value does a DS specialty clinic bring to people with DS and their families? | Secondary data analysis | 105 families | >3 years old | Chart Review | |
| Thomas (2011) [55] Australia | To compare the prevalence of parent reported medical conditions and rates of health service utilization in school-age children with Down syndrome in Western Australia in 1997 and 2004. | Longitudinal data | 272 families | 5–17 years old | Intellectual Disability Exploring Answers database (IDEA) (formerly referred to as Disability Services Commission)- | |
| Tozzi (2015) [46] Italy | We therefore performed a study in a population of families of patients with Down’s syndrome, William’s syndrome and 22q11 deletion syndrome to measure their attitude and expectations regarding specific m-health solutions | Cross-sectional survey design | 121 families | Average 17 yo. | Researcher Generated Survey | Interested in mobile technology for time management and increased involvement in disease management Consultation with physicians. Connected to internet both at home and at work. |
| Van den Driessen Mareeuw (2019) [35] the Netherlands | Our aim is therefore to provide insight into the perspectives of PDS, parents and support staff regarding quality of healthcare for PDS in the Netherlands. | Qualitative interviews | 15 families | >12 years old | Interview guides Framework analysis |
References
- McAllister, J.W.; Presler, E.; Cooley, W.C. Practice-Based Care Coordination: A Medical Home Essential. Pediatrics 2007, 120, e723–e733. [Google Scholar] [CrossRef]
- Turchi, R.M.; Berhane, Z.; Bethell, C.; Pomponio, A.; Antonelli, R.; Minkovitz, C.S. Care Coordination for CSHCN: Associations With Family-Provider Relations and Family/Child Outcomes. Pediatrics 2009, 124, S428–S434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schor, E.L. Ten Essential Characteristics of Care Coordination. JAMA Pediatr. 2019, 173, 5. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.A. Pediatric Care Coordination. JAMA Pediatr. 2019, 173, 112. [Google Scholar] [CrossRef]
- Bull, M.J. The Committee on Genetics Health Supervision for Children with Down Syndrome. Pediatrics 2011, 128, 393–406. [Google Scholar] [CrossRef] [Green Version]
- Santoro, S.L.; Yin, H.; Hopkin, R.J. Adherence to Symptom-Based Care Guidelines for Down Syndrome. Clin. Pediatr. 2017, 56, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Skotko, B.G.; Davidson, E.J.; Weintraub, G.S. Contributions of a specialty clinic for children and adolescents with Down syndrome. Am. J. Med. Genet. Part A 2013, 161, 430–437. [Google Scholar] [CrossRef]
- Williams, K.; Wargowski, D.; Wald, E.; Eickhoff, J. Disparities in Health Supervision for Children with Down Syndrome. Clin. Pediatr. 2017, 56, 1319–1327. [Google Scholar] [CrossRef]
- Ramirez, G.M.; Kum, P.; Kelly, J.J. The Association between Care Coordination and Preventive Care among Children With Special Health Care Needs. Clin. Pediatr. 2020, 59, 663–670. [Google Scholar] [CrossRef]
- Lemke, M.; Kappel, R.; McCarter, R.; D’Angelo, L.; Tuchman, L.K. Perceptions of Health Care Transition Care Coordination in Patients With Chronic Illness. Pediatrics 2018, 141, e20173168. [Google Scholar] [CrossRef]
- Cady, R.G.; Belew, J.L. Parent Perspective on Care Coordination Services for Their Child with Medical Complexity. Children 2017, 4, 45. [Google Scholar] [CrossRef] [Green Version]
- Tschudy, M.M.; Raphael, J.L.; Nehal, U.S.; O’Connor, K.G.; Kowalkowski, M.; Stille, C.J. Barriers to Care Coordination and Medical Home Implementation. Pediatrics 2016, 138, e20153458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies. 2011. Available online: https://www.who.int/goe/publications/goe_mhealth_web.pdf (accessed on 1 January 2021).
- Dzubur, E.; Li, M.; Kawabata, K.; Sun, Y.; McConnell, R.; Intille, S.; Dunton, G.F. Design of a smartphone application to monitor stress, asthma symptoms, and asthma inhaler use. Ann. Allergy Asthma Immunol. 2015, 114, 341–342. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Wang, R.; Zhou, D.; Hong, Z. Smartphone applications for seizure care and management in children and adolescents with epilepsy: Feasibility and acceptability assessment among caregivers in China. Epilepsy Res. 2016, 127, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Quigley, L.; Lacombe-Duncan, A.; Adams, S.; Hepburn, C.M.; Cohen, E. A qualitative analysis of information sharing for children with medical complexity within and across health care organizations. BMC Health Serv. Res. 2014, 14, 283. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Knafl, K.A.; Deatrick, J.A.; Havill, N.L. Continued Development of the Family Management Style Framework. J. Fam. Nurs. 2012, 18, 11–34. [Google Scholar] [CrossRef]
- Marshall, J.; Ramakrishnan, R.; Slotnick, A.L.; Tanner, J.P.; Salemi, J.L.; Kirby, R.S. Family-Centered Perinatal Services for Children With Down Syndrome and Their Families in Florida. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Corbin, J.M.; Strauss, A. Grounded theory research: Procedures, canons, and evaluative criteria. Qual. Sociol. 1990, 13, 3–21. [Google Scholar] [CrossRef]
- Hegde, A.M.; Babu, A.A.; Mohammed, A.; John, A.; Singh, K.; Preethi, V.C.; Shetty, S. Special needs of special children-parental view. Nitte Univ. J. Health Sci. 2015, 5, 038–044. [Google Scholar] [CrossRef] [Green Version]
- Barros da Silva, R.; Barbieri-Figueiredo, M.D.C.; Van Riper, M. Breastfeeding Experiences of Mothers of Children with Down Syndrome. Compr. Child Adolesc. Nurs. 2018, 42, 250–264. [Google Scholar] [CrossRef]
- Cartwright, A.; Boath, E. Feeding infants with Down’s Syndrome: A qualitative study of mothers’ experiences. J. Neonatal Nurs. 2018, 24, 134–141. [Google Scholar] [CrossRef]
- Farkas, L.; Cless, J.D.; Cless, A.W.; Goff, B.S.N.; Bodine, E.; Edelman, A. The Ups and Downs of Down Syndrome: A Qualitative Study of Positive and Negative Parenting Experiences. J. Fam. Issues 2019, 40, 518–539. [Google Scholar] [CrossRef]
- Gibson, A.N.; Martin, J.D., III. Re-situating information poverty: Information marginalization and parents of individuals with disabilities. J. Assoc. Inf. Sci. Technol. 2019, 70, 476–487. [Google Scholar] [CrossRef] [Green Version]
- Huiracocha, L.; Almeida, C.; Huiracocha, K.; Arteaga, J.; Arteaga, A.; Blume, S. Parenting children with Down syndrome: Societal influences. J. Child Health Care 2017, 21, 488–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krueger, K.; Cless, J.D.; Dyster, M.; Reves, M.; Steele, R.; Nelson Goff, B.S. Understanding the Systems, Contexts, Behaviors, and Strategies of Parents Advocating for Their Children with Down Syndrome. Intellect. Dev. Disabil. 2019, 57, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.; Tanner, J.P.; Kozyr, Y.A.; Kirby, R.S. Services and supports for young children with Down syndrome: Parent and provider perspectives. Child Care Health Dev. 2014, 41, 365–373. [Google Scholar] [CrossRef]
- Melvin, K.; Meyer, C.; Ryan, B. “We don’t know what we don’t know”: Providing information about communication to families of children with Down syndrome. Child Care Health Dev. 2019, 45, 423–432. [Google Scholar] [CrossRef]
- Murphy, N.; Epstein, A.; Leonard, H.; Davis, E.; Reddihough, D.; Whitehouse, A.; Jacoby, P.; Bourke, J.; Williams, K.; Downs, J. Qualitative Analysis of Parental Observations on Quality of Life in Australian Children with Down Syndrome. J. Dev. Behav. Pediatr. 2017, 38, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, M.D.R.; Dupas, G. Independence of children with Down syndrome: The experiences of families. Rev. Lat. Am. Enferm. 2011, 19, 985–993. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.C.; Pordeus, I.A.; Luz, C.L.; Paiva, S.M. Mothers’ perceptions concerning oral health of children and adolescents with Down syndrome: A qualitative approach. Eur. J. Paediatr. Dent. 2010, 11, 27–30. [Google Scholar]
- Sheehan, P.; Guerin, S. Exploring the range of emotional response experienced when parenting a child with an intellectual disability: The role of dual process. Br. J. Learn. Disabil. 2018, 46, 109–117. [Google Scholar] [CrossRef]
- Van den Driessen Mareeuw, F.A.; Coppus, A.M.W.; Delnoij, D.M.J.; de Vries, E. Quality of health care according to people with Down syndrome, their parents and support staff—A qualitative exploration. J. Appl. Res. Intellect. Disabil. 2020, 33, 496–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, E.K.; Yoo, I.Y. Resilience in families of children with D own syndrome in K orea. Int. J. Nurs. Pract. 2015, 21, 532–541. [Google Scholar] [CrossRef]
- Descamps, I.; A Marks, L. Oral health in children with Down syndrome: Parents’ views on dental care in Flanders (Belgium). Eur. J. Paediatr. Dent. 2015, 16, 143–148. [Google Scholar]
- Hsiao, C.-Y. Family demands, social support and family functioning in Taiwanese families rearing children with Down syndrome. J. Intellect. Disabil. Res. 2014, 58, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Mengoni, S.E.; Redman, S. Health monitoring of young children with Down syndrome: A parent-report study. Br. J. Learn. Disabil. 2020, 48, 10–18. [Google Scholar] [CrossRef]
- Nqcobo, C.; Kolisa, Y.M.; Ralephenya, T.; Esan, T.; Yengopal, V. Caregivers’ perceptions of the oral-health-related quality of life of children with special needs in Johannesburg, South Africa. Health SA Gesondheid 2019, 24, 1–7. [Google Scholar] [CrossRef]
- Nugent, J.; Gorman, G.; Erdie-Lalena, C.R. Disparities in Access to Healthcare Transition Services for Adolescents with Down Syndrome. J. Pediatr. 2018, 197, 214–220. [Google Scholar] [CrossRef]
- Parrott, R.; Peters, K.F.; Traeder, T. Uncertainty Management and Communication Preferences Related to Genetic Relativism Among Families Affected by Down Syndrome, Marfan Syndrome, and Neurofibromatosis. Health Commun. 2012, 27, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Pikora, T.J.; Bourke, J.; Bathgate, K.; Foley, K.-R.; Lennox, N.; Leonard, H. Health Conditions and Their Impact among Adolescents and Young Adults with Down Syndrome. PLoS ONE 2014, 9, e96868. [Google Scholar] [CrossRef] [Green Version]
- Abdul Rahim, F.S.; Mohamed, A.M.; Marizan Nor, M.; Saub, R. Dental care access among individuals with Down syndrome: A Malaysian scenario. Acta Odontol. Scand. 2014, 72, 999–1004. [Google Scholar] [CrossRef]
- Santoro, S.L.; Martin, L.J.; Hopkin, R.J. Screening for hematological disorders in mosaic Down syndrome: Parent report of experiences. Clin. Pediatr. 2016, 55, 421–427. [Google Scholar] [CrossRef]
- Tozzi, A.E.; Carloni, E.; Gesualdo, F.; Russo, L.; Raponi, M. Attitude of Families of Patients with Genetic Diseases to Use m-Health Technologies. Telemed. e-Health 2015, 21, 86–89. [Google Scholar] [CrossRef]
- Bertoli, M.; Biasini, G.; Calignano, M.T.; Celani, G.; De Grossi, G.; Digilio, M.C.; Fermariello, C.C.; Loffredo, G.; Luchino, F.; Marchese, A.; et al. Needs and challenges of daily life for people with Down syndrome residing in the city of Rome, Italy. J. Intellect. Disabil. Res. 2011, 55, 801–820. [Google Scholar] [CrossRef] [Green Version]
- Hall, H.R.; Neely-Barnes, S.L.; Graff, J.C.; Krcek, T.E.; Roberts, R.J.; Hankins, J.S. Parental Stress in Families of Children with a Genetic Disorder/Disability and the Resiliency Model of Family Stress, Adjustment, and Adaptation. Issues Compr. Pediatr. Nurs. 2012, 35, 24–44. [Google Scholar] [CrossRef]
- Hall, A.; Pryce, H.; Bruce, I.A.; Callery, P.; Lakhanpaul, M.; Schilder, A.G. A mixed-methods study of the management of hearing loss associated with otitis media with effusion in children with Down syndrome. Clin. Otolaryngol. 2019, 44, 32–38. [Google Scholar] [CrossRef]
- Leonard, H.; Foley, K.-R.; Pikora, T.; Bourke, J.; Wong, K.; McPherson, L.; Lennox, N.; Downs, J. Transition to adulthood for young people with intellectual disability: The experiences of their families. Eur. Child Adolesc. Psychiatry 2016, 25, 1369–1381. [Google Scholar] [CrossRef]
- Hubner, L.M.; Feldman, H.M.; Huffman, L.C. Parent-Reported Shared Decision Making. J. Dev. Behav. Pediatr. 2016, 37, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Lollar, D.J.; Hartzell, M.S.; Evans, M.A. Functional Difficulties and Health Conditions among Children with Special Health Needs. Pediatrics 2012, 129, e714–e722. [Google Scholar] [CrossRef]
- Phelps, R.A.; Pinter, J.D.; Lollar, D.J.; Medlen, J.G.; Bethell, C.D. Health Care Needs of Children With Down Syndrome and Impact of Health System Performance on Children and Their Families. J. Dev. Behav. Pediatr. 2012, 33, 214–220. [Google Scholar] [CrossRef]
- Schieve, L.A.; Boulet, S.; Kogan, M.D.; Van Naarden-Braun, K.; Boyle, C.A. A population-based assessment of the health, functional status, and consequent family impact among children with Down syndrome. Disabil. Health J. 2011, 4, 68–77. [Google Scholar] [CrossRef]
- Thomas, K.; Bourke, J.; Girdler, S.; Bebbington, A.; Jacoby, P.; Leonard, H. Variation Over Time in Medical Conditions and Health Service Utilization of Children with Down Syndrome. J. Pediatr. 2011, 158, 194–200. [Google Scholar] [CrossRef]
- Crossman, M.K.; Parish, S.L.; Hauser-Cram, P.; Garcia, D.A.; Warfield, M.E. The influence of early intervention, informal support and the family environment on trajectories of competence for fathers raising children with developmental disabilities. Res. Dev. Disabil. 2018, 81, 122–133. [Google Scholar] [CrossRef]
- Choi, H.; Van Riper, M. mHealth Family Adaptation Intervention for Families of Young Children with Down Syndrome: A Feasibility Study. J. Pediatr. Nurs. 2020, 50, e69–e76. [Google Scholar] [CrossRef]
- National Association of Pediatic Nurse Practitioners Executive Board. Position Statement on Pediatric Health Care/Medical Home: Key Issues on Care Coordination, Transitions, and Leadership. J. Pediatr. Health Care 2016, 30, A17–A19. [Google Scholar] [CrossRef]
- Turchi, R.M.; Antonelli, R.C.; Norwood, K.W.; Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee. Patient-and family-centered care coordination: A framework for integrating care for children and youth across multiple systems. Pediatrics 2014, 133, e1451–e1460. [Google Scholar] [CrossRef] [Green Version]
- Litt, J.S.; McCormick, M.C. Care Coordination, the Family-Centered Medical Home, and Functional Disability Among Children With Special Health Care Needs. Acad. Pediatr. 2015, 15, 185–190. [Google Scholar] [CrossRef]
- Zhou, L.; DeAlmeida, D.; Parmanto, B. Applying a User-Centered Approach to Building a Mobile Personal Health Record App: Development and Usability Study. JMIR mHealth uHealth 2019, 7, e13194. [Google Scholar] [CrossRef]
- Maher, M.; Kaziunas, E.; Ackerman, M.; Derry, H.; Forringer, R.; Miller, K.; O’Reilly, D.; An, L.C.; Tewari, M.; Hanauer, D.A.; et al. User-Centered Design Groups to Engage Patients and Caregivers with a Personalized Health Information Technology Tool. Biol. Blood Marrow Transplant. 2016, 22, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.; Donelan, K.; Macklin, E.A.; Schwartz, A.; Elsharkawi, I.; Torres, A.; Hsieh, Y.G.; Parker, H.; Ba, S.L.; Ba, V.P.; et al. A randomized controlled trial of an online health tool about Down syndrome. Genet. Med. 2021, 23, 163–173. [Google Scholar] [CrossRef]
- De La Torre-Díez, I.; López-Coronado, M.; Vaca, C.; Aguado, J.S.; de Castro, C. Cost-Utility and Cost-Effectiveness Studies of Telemedicine, Electronic, and Mobile Health Systems in the Literature: A Systematic Review. Telemed. e-Health 2015, 21, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Rinaldi, G.; Hijazi, A.; Haghparast-Bidgoli, H. Cost and cost-effectiveness of mHealth interventions for the prevention and control of type 2 diabetes mellitus: A systematic review. Diabetes Res. Clin. Pract. 2020, 162, 108084. [Google Scholar] [CrossRef] [PubMed]
- GooglePlay. Available online: https://play.google.com/store/apps/details?id=com.otsimo.app (accessed on 24 June 2021).
- DSC2U. Available online: https://www.dsc2u.org/insurers (accessed on 24 June 2021).
- Desai, A.D.; Wang, G.; Wignall, J.; Kinard, D.; Singh, V.; Adams, S.; Pratt, W. User-centered design of a longitudinal care plan for children with medical complexity. J. Am. Med. Inform. Assoc. 2020, 27, 1860–1870. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skelton, B.; Knafl, K.; Van Riper, M.; Fleming, L.; Swallow, V. Care Coordination Needs of Families of Children with Down Syndrome: A Scoping Review to Inform Development of mHealth Applications for Families. Children 2021, 8, 558. https://doi.org/10.3390/children8070558
Skelton B, Knafl K, Van Riper M, Fleming L, Swallow V. Care Coordination Needs of Families of Children with Down Syndrome: A Scoping Review to Inform Development of mHealth Applications for Families. Children. 2021; 8(7):558. https://doi.org/10.3390/children8070558
Chicago/Turabian StyleSkelton, Beth, Kathleen Knafl, Marcia Van Riper, Louise Fleming, and Veronica Swallow. 2021. "Care Coordination Needs of Families of Children with Down Syndrome: A Scoping Review to Inform Development of mHealth Applications for Families" Children 8, no. 7: 558. https://doi.org/10.3390/children8070558