Quantifying the Language Barrier—A Total Survey of Parents’ Spoken Languages and Local Language Skills as Perceived by Different Professions in Pediatric Palliative Care



Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Setting and Participants
2.2. Recording Sheet
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Spoken Languages
3.2. Local Language Skills
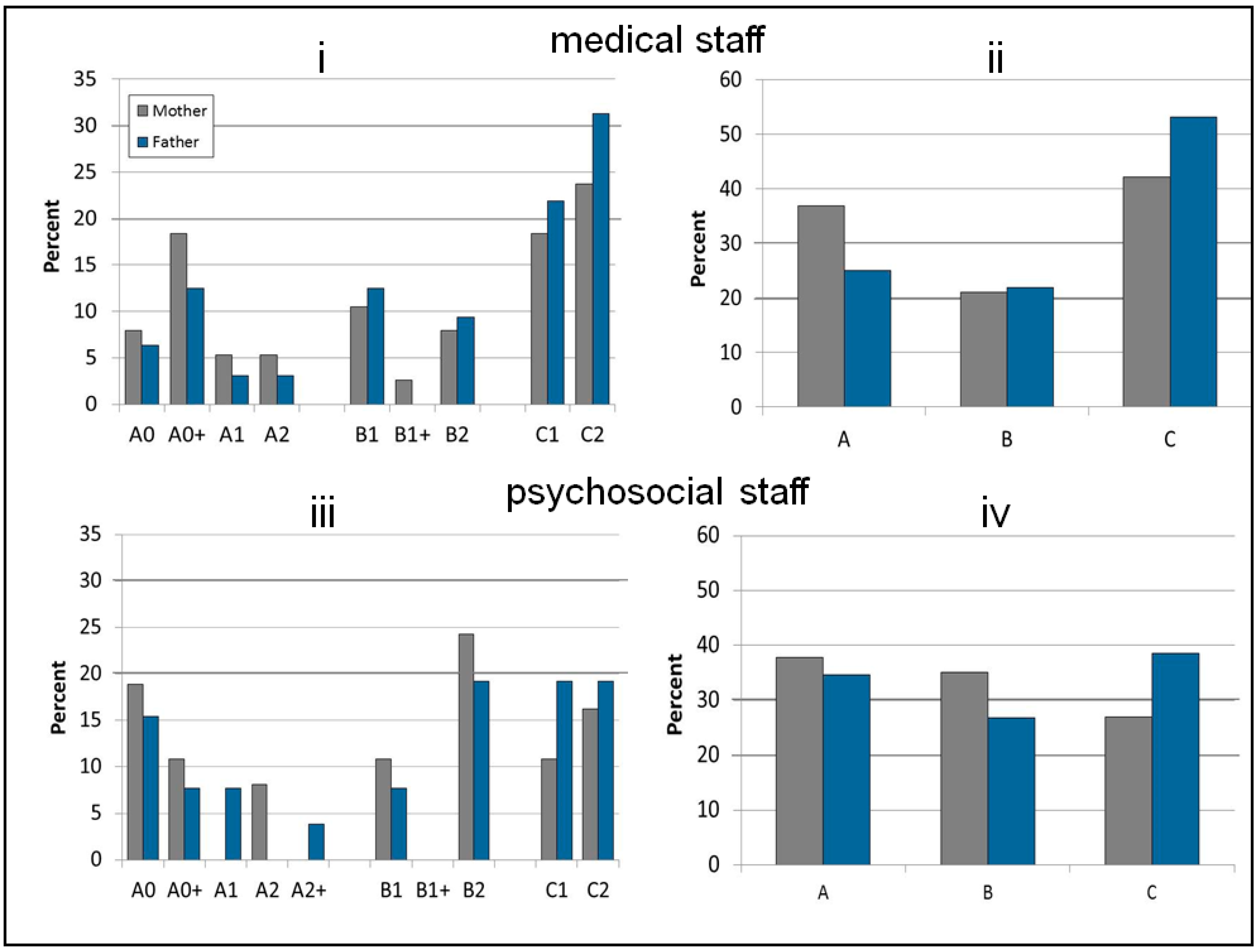
3.2.1. Overall Distribution of Language Skills
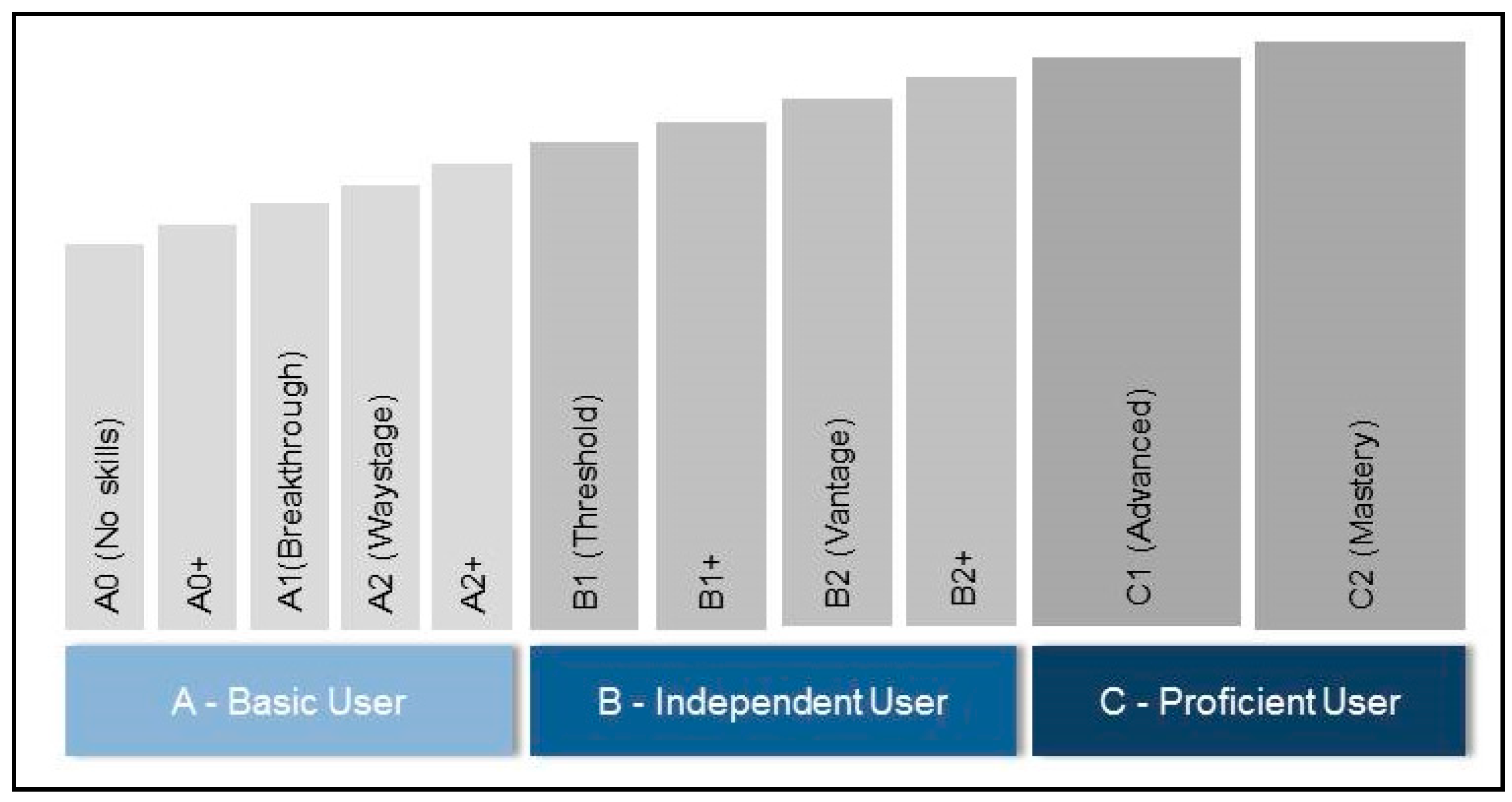
3.2.2. Superordinate Competence Levels
3.2.3. Subordinate Language Skills Levels
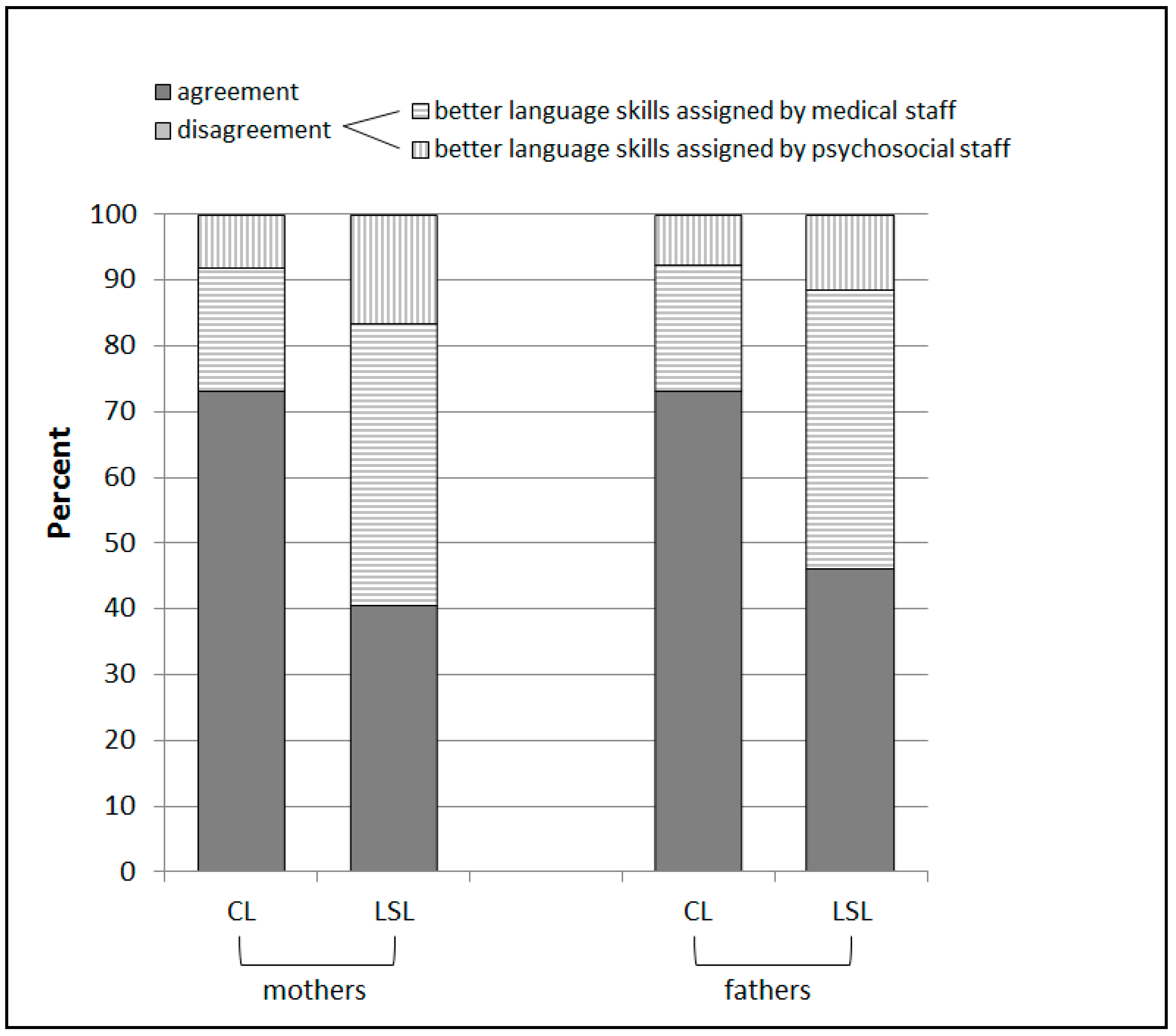
3.3. Interprofessional Agreement
3.3.1. Superordinate Competence Levels
3.3.2. Subordinate Language Skills Levels
4. Discussion
4.1. Main Findings
4.2. Implications for Clinical Practice
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Joint Commission. Sentinel Event Data: Root Causes by Event Type 2004–2014. 2015. Available online: http://www.tolcam.com/wp-content/uploads/2015/04/TJC-Sentinel-Event-Root_Causes_by_Event_Type_2004-20141.pdf (accessed on 29 March 2019).
- Walter, C.; Matar, Z. Interkulturelle Kommunikation in der Gesundheitswirtschaft: Herausforderungen, Chancen und Fallbeispiele; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2018. [Google Scholar]
- Imai, M.; Kanero, J.; Masuda, T. The relation between language, culture, and thought. Curr. Opin. Psychol. 2016, 8, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W. The relationship between culture and language. ELT J. 2000, 54, 328–334. [Google Scholar] [CrossRef]
- Association for Children with Life-Threatening or Terminal Conditions and Their Families; Royal College of Paediatrics and Child Health. A Guide to the Development of Children’s Palliative Care Services; ACT: Bristol, UK, 1997. [Google Scholar]
- Jassal, S.S. Symptom control in paediatric palliative care. Paediatr. Child Health 2016, 26, 87–88. [Google Scholar] [CrossRef]
- Craig, F.; Abu-Saad Huijer, H.; Benini, F.; Kuttner, L.; Wood, C.; Feraris, P.C.; Zernikow, B. IMPaCCT: Standards of paediatric palliative care. Schmerz (Berl. Ger.) 2008, 22, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Hasan, C.; Zernikow, B. Organisation pädiatrischer palliativversorgung in deutschland. Kinderärztliche Prax. 2009, 80, 279–285. [Google Scholar]
- Irish Hospice Foundation. A Palliative Care Needs Assessment for Children; Stationary Office: Dublin, Ireland, 2005. [Google Scholar]
- Lazzarin, P.; Schiavon, B.; Brugnaro, L.; Benini, F. Parents spend an average of nine hours a day providing palliative care for children at home and need to maintain an average of five life-saving devices. Acta Paediatr. 2018, 107, 289–293. [Google Scholar] [CrossRef]
- Davies, B.; Sehring, S.A.; Partridge, J.C.; Cooper, B.A.; Hughes, A.; Philp, J.C.; Amidi-Nouri, A.; Kramer, R.F. Barriers to palliative care for children: Perceptions of pediatric health care providers. Pediatrics 2008, 121, 282–288. [Google Scholar] [CrossRef]
- Watts, K.J.; Meiser, B.; Zilliacus, E.; Kaur, R.; Taouk, M.; Girgis, A.; Butow, P.; Kissane, D.W.; Hale, S.; Perry, A.; et al. Perspectives of oncology nurses and oncologists regarding barriers to working with patients from a minority background: Systemic issues and working with interpreters. Eur. J. Cancer Care 2018, 27, e12758. [Google Scholar] [CrossRef]
- Suurmond, J.; Lieveld, A.; van de Wetering, M.; Schouten-van Meeteren, A.Y.N. Towards culturally competent paediatric oncology care. A qualitative study from the perspective of care providers. Eur. J. Cancer Care 2017, 26, e12680. [Google Scholar] [CrossRef]
- Ngui, E.M.; Flores, G. Satisfaction with care and ease of using health care services among parents of children with special health care needs: The roles of race/ethnicity, insurance, language, and adequacy of family-centered care. Pediatrics 2006, 117, 1184–1196. [Google Scholar] [CrossRef]
- Contro, N.; Davies, B.; Larson, J.; Sourkes, B. Away from home: Experiences of mexican american families in pediatric palliative care. J. Soc. Work End Life Palliat. Care 2010, 6, 185–204. [Google Scholar] [CrossRef] [PubMed]
- Eneriz-Wiemer, M.; Sanders, L.M.; Barr, D.A.; Mendoza, F.S. Parental limited english proficiency and health outcomes for children with special health care needs: A systematic review. Acad Pediatr. 2014, 14, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Contro, N.; Larson, J.; Scofield, S.; Sourkes, B.; Cohen, H. Family perspectives on the quality of pediatric palliative care. Arch. Pediatr. Adolesc. Med. 2002, 156, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz-Blanco, S.; Raisanen, J.C.; Donohue, P.K.; Boss, R.D. Enhancing pediatric palliative care for latino children and their families: A review of the literature and recommendations for research and practice in the united states. Children 2017, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brisset, C.; Leanza, Y.; Rosenberg, E.; Vissandjee, B.; Kirmayer, L.J.; Muckle, G.; Xenocostas, S.; Laforce, H. Language barriers in mental health care: A survey of primary care practitioners. J. Immigr. Minor. Health 2014, 16, 1238–1246. [Google Scholar] [CrossRef] [PubMed]
- Gil, S.; Hooke, M.C.; Niess, D. The limited english proficiency patient family advocate role: Fostering respectful and effective care across language and culture in a pediatric oncology setting. J. Pediatr. Oncol. Nurs. Off. J. Assoc. Pediatr. Oncol. Nurses 2016, 33, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Hadziabdic, E.; Albin, B.; Hjelm, K. Arabic-speaking migrants’ attitudes, opinions, preferences and past experiences concerning the use of interpreters in healthcare: A postal cross-sectional survey. BMC Res. Notes 2014, 7, 71. [Google Scholar] [CrossRef] [Green Version]
- Jirwe, M.; Gerrish, K.; Emami, A. Student nurses’ experiences of communication in cross-cultural care encounters. Scand. J. Caring Sci. 2010, 24, 436–444. [Google Scholar] [CrossRef]
- Lee, S.K.; Sulaiman-Hill, C.R.; Thompson, S.C. Overcoming language barriers in community-based research with refugee and migrant populations: Options for using bilingual workers. BMC Int. Health Hum. Rights 2014, 14, 11. [Google Scholar] [CrossRef]
- Lindley, L.C.; Held, M.L.; Henley, K.M.; Miller, K.A.; Pedziwol, K.E.; Rumley, L.E. Nursing unit environment associated with provision of language services in pediatric hospices. J. Racial Ethn. Health Dispar. 2017, 4, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.D.; Genoff, M.; Zaballa, A.; Jewell, S.; Stabler, S.; Gany, F.M.; Diamond, L.C. Interpreting at the end of life: A systematic review of the impact of interpreters on the delivery of palliative care services to cancer patients with limited English proficiency. J. Pain Symptom Manag. 2016, 51, 569–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, L.A.; Bloomer, M.J.; Manias, E. Culturally sensitive communication at the end-of-life in the intensive care unit: A systematic review. Aust. Crit. Care 2018, 32, 516–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansky, M.; Owusu-Boakye, S.; Nauck, F. “An odyssey without receiving proper care”—Experts’ views on palliative care provision for patients with migration background in germany. BMC Palliat. Care 2019, 18, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schouten, B.C.; Meeuwesen, L. Cultural differences in medical communication: A review of the literature. Patient Educ. Couns. 2006, 64, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Suurmond, J.; Seeleman, C. Shared decision-making in an intercultural context. Barriers in the interaction between physicians and immigrant patients. Patient Educ. Couns. 2006, 60, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Tavallali, A.G.; Jirwe, M.; Kabir, Z.N. Cross-cultural care encounters in paediatric care: Minority ethnic parents’ experiences. Scand. J. Caring Sci. 2017, 31, 54–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiener, L.; McConnell, D.G.; Latella, L.; Ludi, E. Cultural and religious considerations in pediatric palliative care. Palliat. Support. Care 2013, 11, 47–67. [Google Scholar] [CrossRef] [Green Version]
- Garske, D.; Schmidt, P.; Hasan, C.; Wager, J.; Zernikow, B. Palliativversorgung auf der pädiatrischen palliativstation „lichtblicke“—Eine retrospektive studie. Palliativmedizin 2016, 17, 302–307. [Google Scholar] [CrossRef]
- Council of Europe. Common European Framework of Reference for Languages: Learning, Teaching, Assessment; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Beckstrand, R.L.; Rawle, N.L.; Callister, L.; Mandleco, B.L. Pediatric nurses’ perceptions of obstacles and supportive behaviors in end-of-life care. Am. J. Crit. Care Off. Publ. Am. Assoc. Crit. Care Nurses 2010, 19, 543–552. [Google Scholar] [CrossRef]
- Zurca, A.D.; Fisher, K.R.; Flor, R.J.; Gonzalez-Marques, C.D.; Wang, J.; Cheng, Y.I.; October, T.W. Communication with limited English-proficient families in the picu. Hosp. Pediatr. 2017, 7, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, B.; Contro, N.; Larson, J.; Widger, K. Culturally-sensitive information-sharing in pediatric palliative care. Pediatrics 2010, 125, e859–e865. [Google Scholar] [CrossRef] [PubMed]
- Leonard, M.; Graham, S.; Bonacum, D. The human factor: The critical importance of effective teamwork and communication in providing safe care. Qual. Saf. Health Care 2004, 13 (Suppl. 1), i85–i90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valizadeh, L.; Zamanzadeh, V.; Ghahramanian, A.; Aghajari, P.; Foronda, C. Factors influencing nurse-to-parent communication in culturally sensitive pediatric care: A qualitative study. Contemp. Nurse 2017, 53, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt. Bevölkerung, familien, lebensformen. In Statistisches Jahrbuch; Statistisches Bundesamt: Wiesbaden, Germany, 2018. [Google Scholar]
- Tietze, A.L.; Zernikow, B.; Michel, E.; Blankenburg, M. Sleep disturbances in children, adolescents, and young adults with severe psychomotor impairment: Impact on parental quality of life and sleep. Dev. Med. Child Neurol. 2014, 56, 1187–1193. [Google Scholar] [CrossRef]
- Morelius, E.; Hemmingsson, H. Parents of children with physical disabilities—Perceived health in parents related to the child’s sleep problems and need for attention at night. Child Care Health Dev. 2014, 40, 412–418. [Google Scholar] [CrossRef]
- Martinovic, I.; Altarriba, J. Bilingualism and emotion: Implications for mental health. Handb. Biling. Multiling. 2012, 292–320. [Google Scholar] [CrossRef]
- Oquendo, M.A. Psychiatric evaluation and psychotherapy in the patient’s second language. Psychiatr. Serv. 1996, 47, 614–618. [Google Scholar]
- Dardas, L.A.; Simmons, L.A. The stigma of mental illness in arab families: A concept analysis. J. Psychiatr. Ment. Health Nurs. 2015, 22, 668–679. [Google Scholar] [CrossRef]
- Zolezzi, M.; Alamri, M.; Shaar, S.; Rainkie, D. Stigma associated with mental illness and its treatment in the arab culture: A systematic review. Int. J. Soc. Psychiatr. 2018, 64, 597–609. [Google Scholar] [CrossRef]
- Bener, A.; Ghuloum, S. Gender differences in the knowledge, attitude and practice towards mental health illness in a rapidly developing arab society. Int. J. Soc. Psychiatr. 2011, 57, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Fearon, D.; Kane, H.; Aliou, N.; Sall, A. Perceptions of palliative care in a lower middle-income muslim country: A qualitative study of health care professionals, bereaved families and communities. Palliat. Med. 2019, 33, 241–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, P.; Rozmus, C. Culturally sensitive care of the muslim patient. J. Transcult. Nurs. 2001, 12, 228–233. [Google Scholar] [CrossRef] [PubMed]
- David, M.; Ilkilic, I. Religiöser glaube–islam. Der Gynäkol. 2010, 43, 53–57. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Language | n | % |
|---|---|---|
| Turkish | 22 | 45.8 |
| Arabic | 6 | 12.5 |
| Albanian | 3 | 6.3 |
| Syriac | 2 | 4.2 |
| Italian | 2 | 4.2 |
| Croatian | 2 | 4.2 |
| Russian | 2 | 4.2 |
| Kurdish | 2 | 4.2 |
| Lebanese | 1 | 2.1 |
| Kazakh | 1 | 2.1 |
| Persian | 1 | 2.1 |
| Romanian | 1 | 2.1 |
| Sinti | 1 | 2.1 |
| Armenian | 1 | 2.1 |
| Total | 48 | 100 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dreier, L.A.; Zernikow, B.; Wager, J. Quantifying the Language Barrier—A Total Survey of Parents’ Spoken Languages and Local Language Skills as Perceived by Different Professions in Pediatric Palliative Care. Children 2020, 7, 118. https://doi.org/10.3390/children7090118
Dreier LA, Zernikow B, Wager J. Quantifying the Language Barrier—A Total Survey of Parents’ Spoken Languages and Local Language Skills as Perceived by Different Professions in Pediatric Palliative Care. Children. 2020; 7(9):118. https://doi.org/10.3390/children7090118
Chicago/Turabian StyleDreier, Larissa Alice, Boris Zernikow, and Julia Wager. 2020. "Quantifying the Language Barrier—A Total Survey of Parents’ Spoken Languages and Local Language Skills as Perceived by Different Professions in Pediatric Palliative Care" Children 7, no. 9: 118. https://doi.org/10.3390/children7090118