“We Want to Talk about Death, Dying and Grief and to Learn about End-of-Life Care”—Lessons Learned from a Multi-Center Mixed-Methods Study on Last Aid Courses for Kids and Teens

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Concept and Curriculum of the Last Aid Course for Kids and Teens (LAC-KT)
- The old badger; about dying and grief suited for children and teenagers [15].
- Bill’s story; about compassionate communities and what everyone in the community may contribute [16].
- Knietzsche und der Tod (Knietzsche and death); about philosophical views on death and dying from the perspective of a child philosopher [17].
- Sowieso; a music video from Mark Forster as farewell at the end of the course [18].
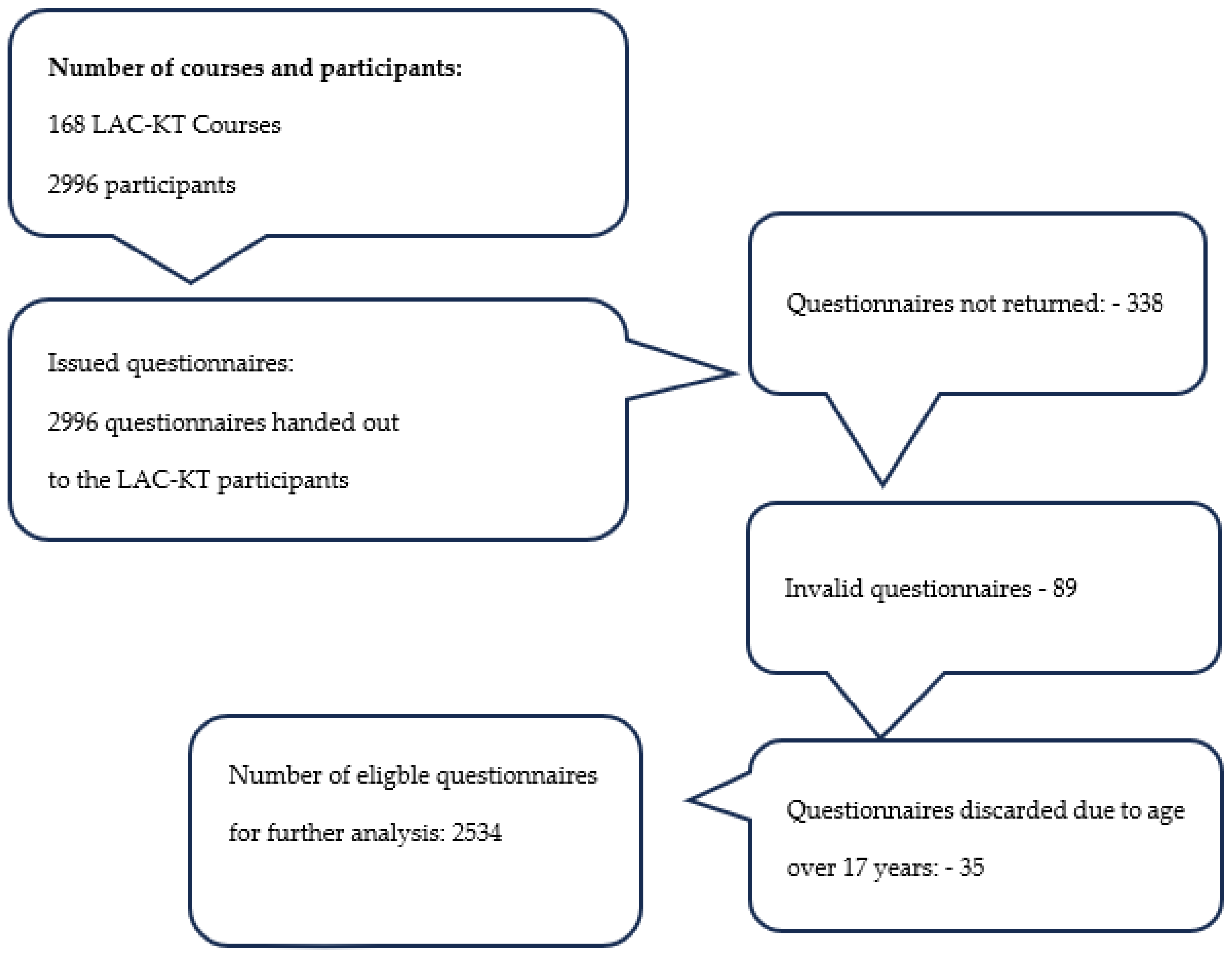
2.2. Setting and Participants
2.3. Data Collection and Analysis
- What are your experiences with Last Aid Courses for Kids and Teens in general?
- What are your positive experiences with Last Aid Courses for Kids and Teens?
- What are your negative experiences with Last Aid Courses for Kids and Teens?
- Which methods did you use for practice and hands-on training in the Last Aid Courses for Kids and Teens?
- What are your views and experiences concerning communication with teachers and schools?
2.4. Ethical Considerations and Ethics Approval
3. Results
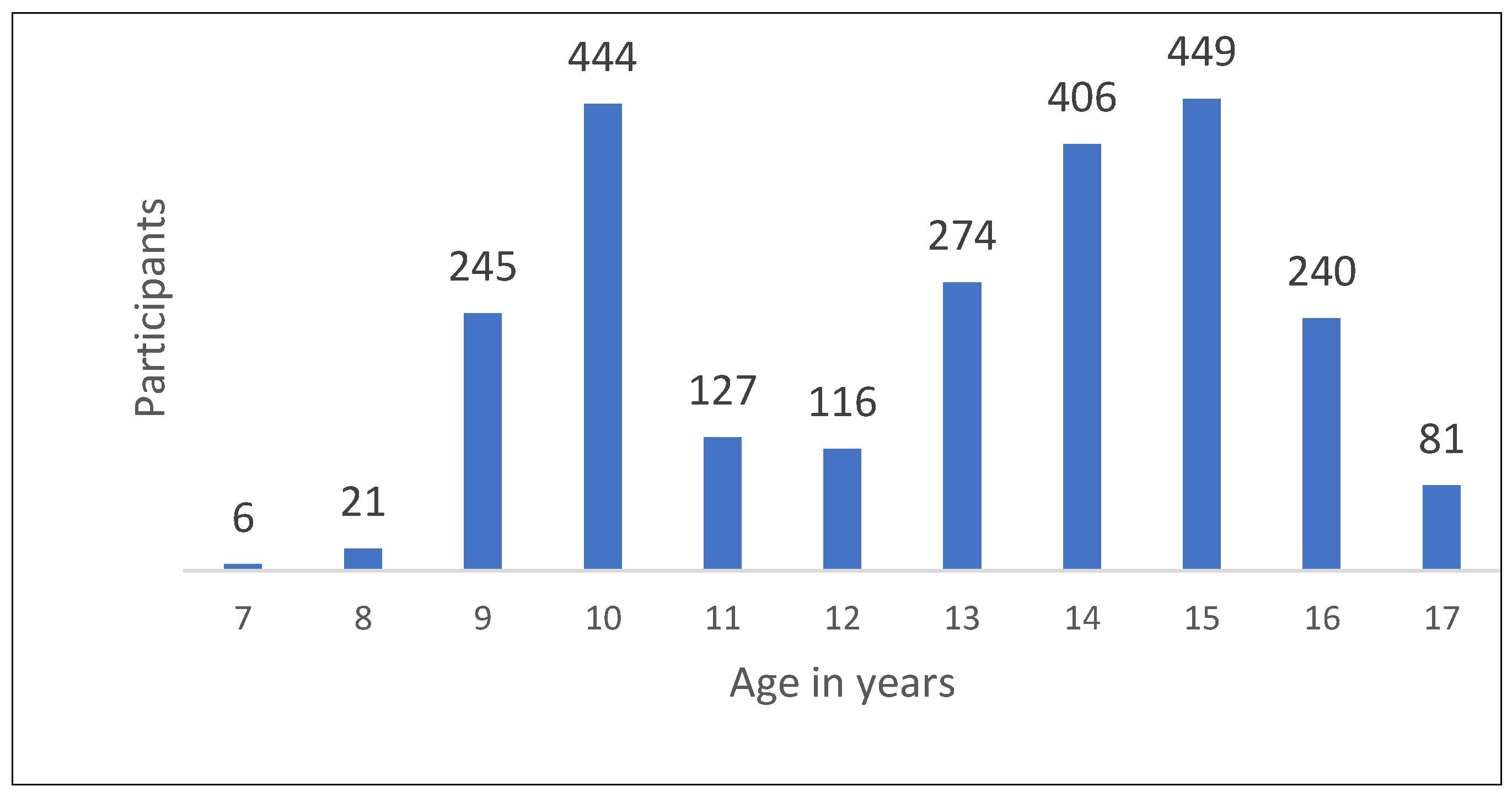
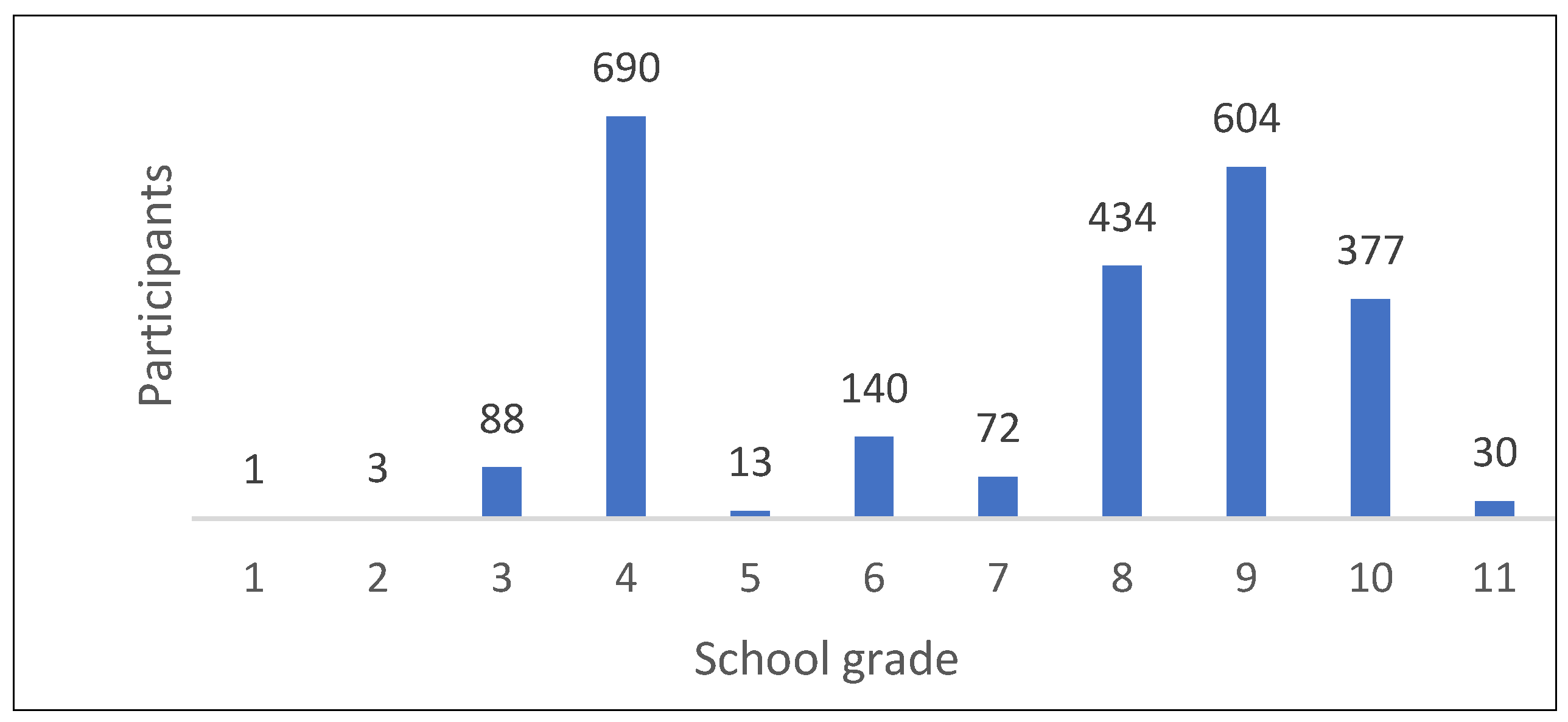
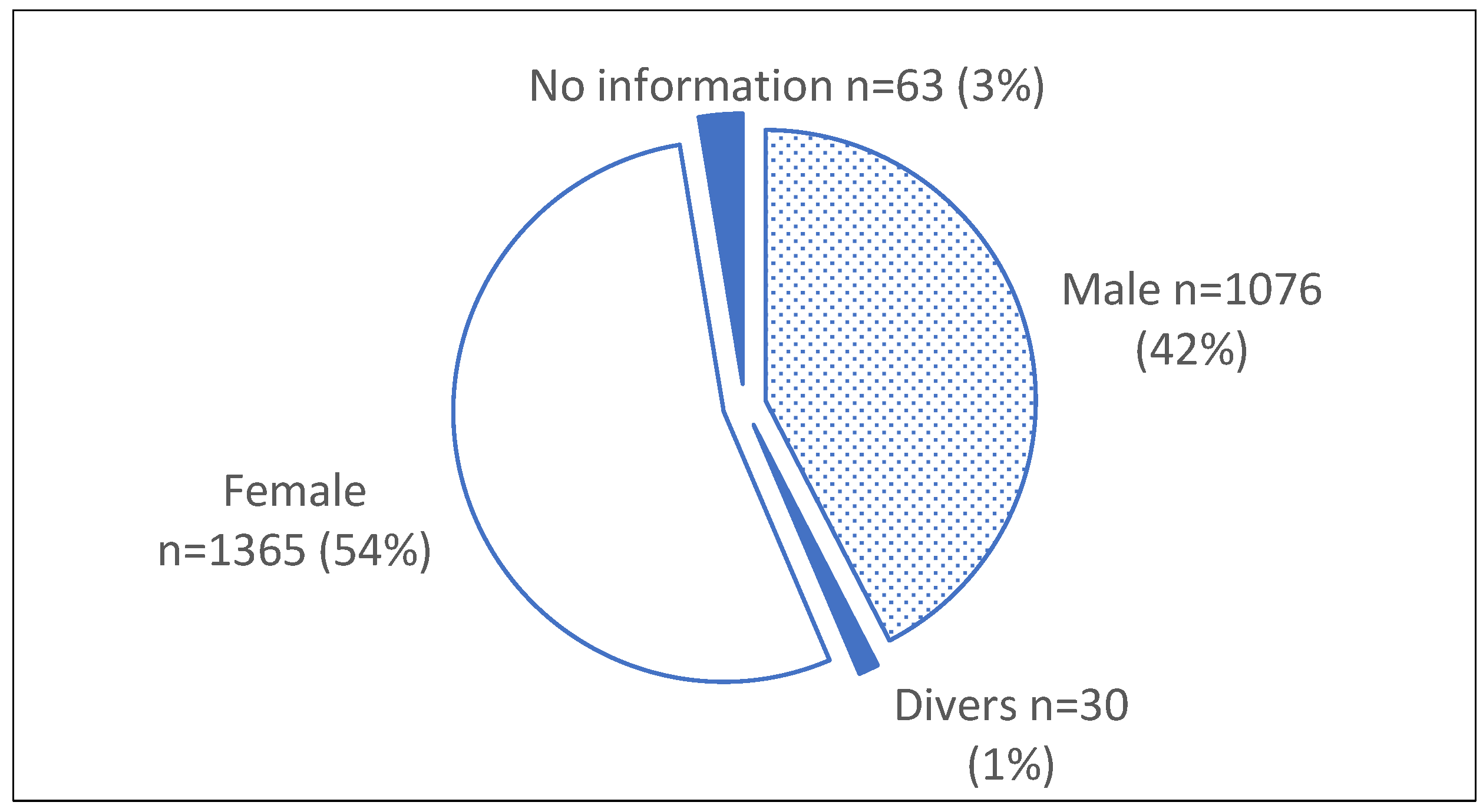
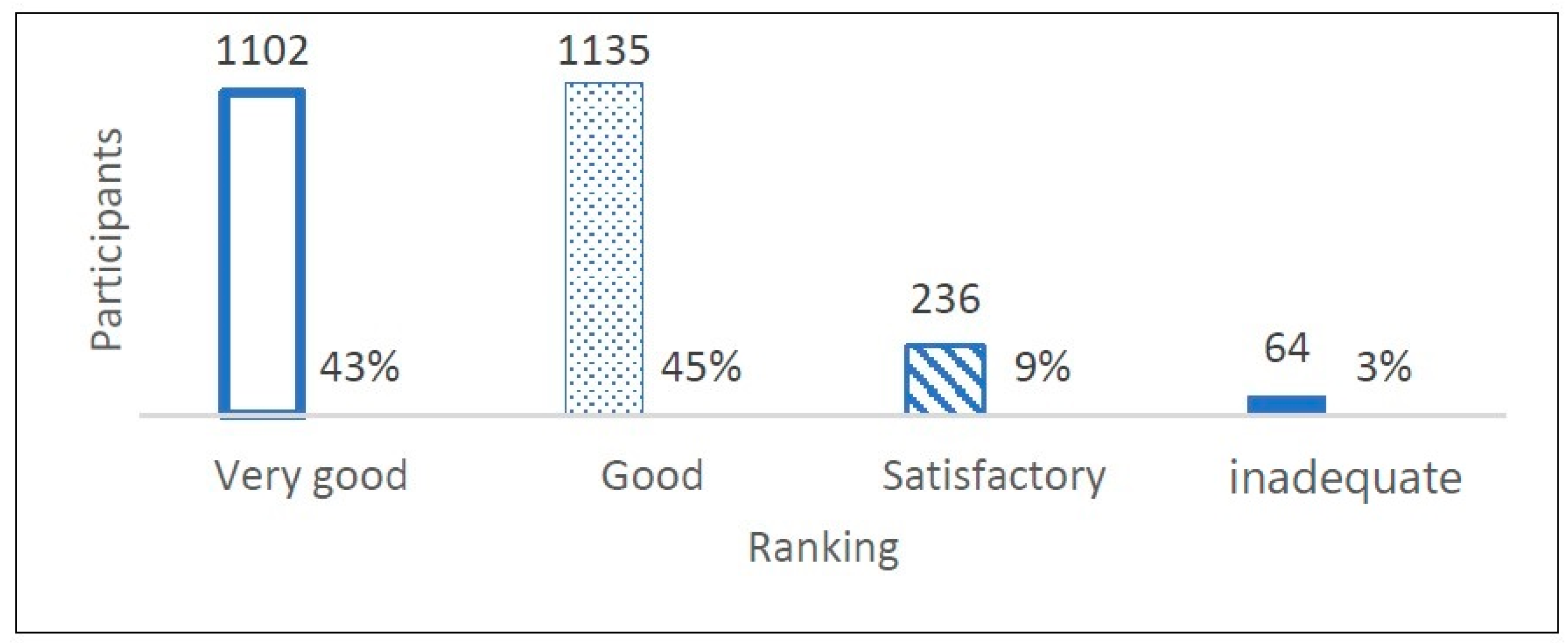
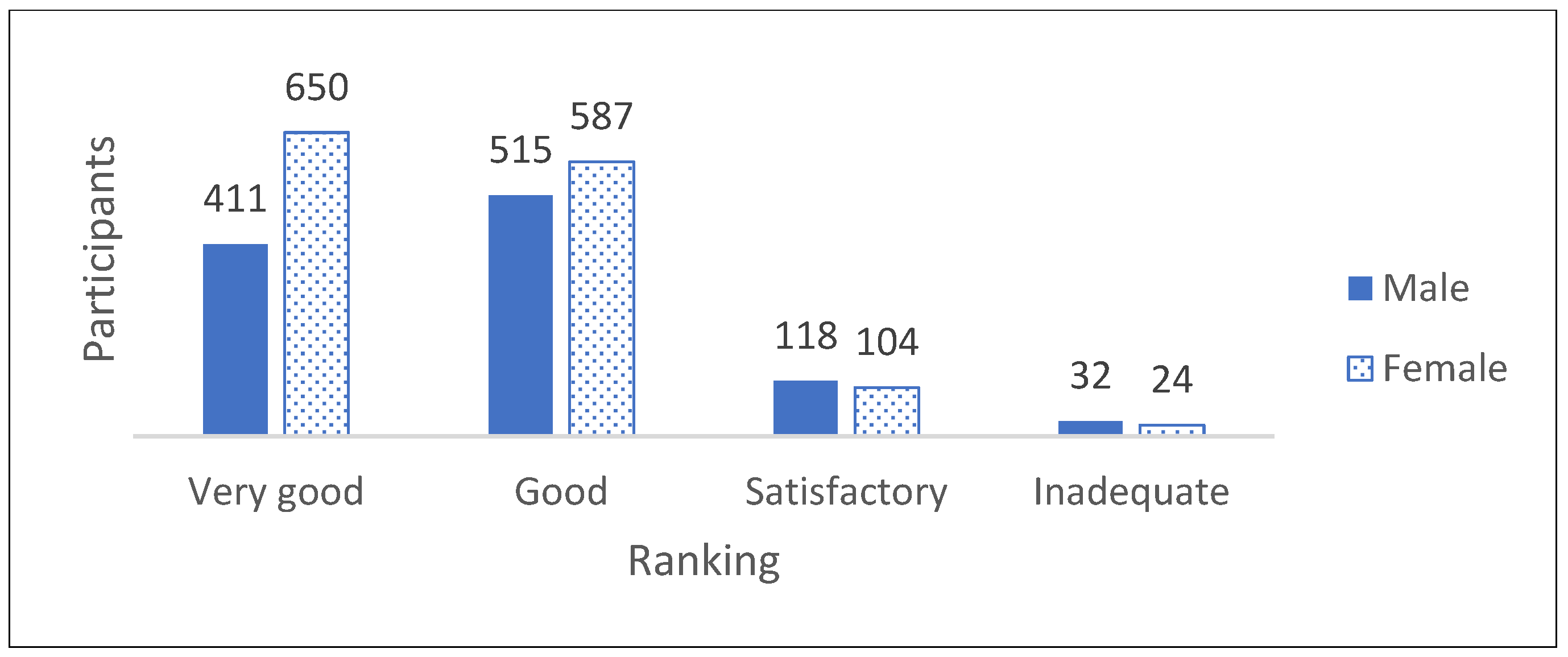
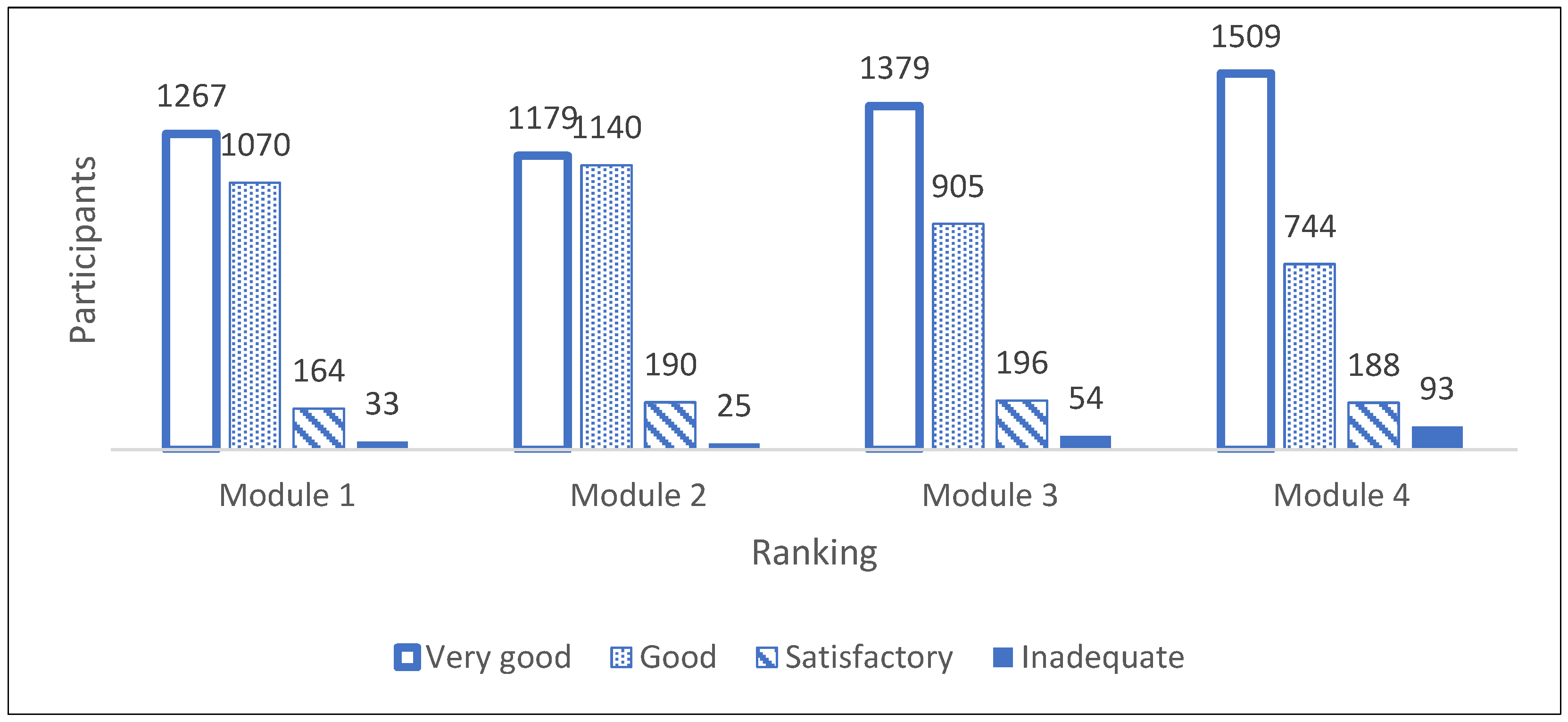
3.1. Results from the Quantitative Data from the Questionnaire
3.2. Results from the Qualitative Data from the Questionnaire and the Focus Group Interviews
3.2.1. Results from the Qualitative Data from the Questionnaire
I liked module 3 best because I found it very interesting what oneself can do.(girl, 8 years)
I liked very much that we have talked about it, because you do not talk about death very often.(girl, 13 years)
I liked that we have talked extensively and open about life and death and that we also have talked about the feelings of dying people.(girl, 13 years)
I liked everything.(boy, 9 years)
Most of all I liked the videos and the practical activities.(boy, 14 years)
I liked everything. The best theme was final goodbyes.(girl, 15 years)
I liked best the network game and the mouth care.(girl, 9 years)
3.2.2. Interview Findings from the Focus Group Interviews of LAC-KT Instructors
Instructors’ Experiences
Most of them (the participants) say thank you that they were able to say everything they wanted.
We actually had a confirmand who had lost her grandmother one week ago. She came crying to the course and discussed with the priest if she should participate in the course. She was allowed to decide on her own if she wanted to participate. We then lit a candle for her grandmother and she stayed. This led to a great solidarity within the group and she left the course with a smile.
The lack of time was a problem. In the confirmand teaching program time is very restricted. We were able to get 1.5 h in the first and 1.5 h in the second week. And we won’t get more time. We have to do it (the LAC-KT) within 3 h. This makes it hard for us and sometimes we have to hurry through the course. We would love to have more time.
Practical and Logistical Aspects
The children often become less fearful and felt better prepared for participating in end-of-life care, especially after the practical parts of the course. Many of us instructors use an extensive introductory round, often guided by postcards with a variety of images. The practical parts included painting stones, activities around Emoji-cards showing feelings, a jumping sheet to illustrate networking and teamwork and mouth care. Many participants loved the activity with the jumping sheet. This method shows them in practice how networks can support.
Implementation
You need someone who knows the school. We have often been in the newspaper with our Last Aid Course in the 6th grade. Now the schools contact me. In the beginning I used to write many Emails or letter with information material but there was no response. Sometimes they replied that they would look at it and contact me again.
Barriers
Last time (we did a LAC-KT) the parents of a girl decided that she should not participate. And I thought that this is a bad experience (for the girl). There is so much restraint for talking about this topic (death and dying) that people do not give their children a chance to participate.
We have given many courses and within the last half year there are always two or three children who do not speak enough German. That was very exhausting for the children because they did not understand anything.
Others
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McIlfatrick, S.; Hasson, F.; McLaughlin, D.; Johnston, G.; Roulston, A.; Rutherford, L.; Noble, H.; Kelly, S.; Craig, A.; Kernohan, W.G. Public awareness and attitudes toward palliative care in Northern Ireland. BMC Palliat. Care 2013, 12, 34. [Google Scholar] [CrossRef]
- McIlfatrick, S.; Noble, H.; McCorry, N.K.; Roulston, A.; Hasson, F.; McLaughlin, D.; Johnston, G.; Rutherford, L.; Payne, C.; Kernohan, G.; et al. Exploring public awareness and perceptions of palliative care: A qualitative study. Palliat. Med. 2014, 28, 273–280. [Google Scholar] [CrossRef]
- Gopal, K.S.; Archana, P.S. Awareness, knowledge and attitude about palliative care, in general, population and health care professionals in tertiary care hospital. Int. J. Sci. Study 2016, 3, 31–35. [Google Scholar]
- Kozlov, E.; McDarby, M.; Reid, M.C.; Carpenter, B.D. Knowledge of Palliative Care Among Community-Dwelling Adults. Am. J. Hosp. Palliat. Care 2018, 35, 647–651. [Google Scholar] [CrossRef]
- Boucher, N.A.; Bull, J.H.; Cross, S.H.; Kirby, C.; Davis, J.K.; Taylor, D.H. Patient, Caregiver, and Taxpayer Knowledge of Palliative Care and Views on a Model of Community-Based Palliative Care. J. Pain Symptom Manag. 2018, 56, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Westerlund, C.; Tishelman, C.; Benkel, I.; Fürst, C.J.; Molander, U.; Rasmussen, B.H.; Sauter, S.; Lindqvist, O. Public awareness of palliative care in Sweden. Scand. J. Public Health 2018, 46, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Noonan, K. Death literacy—Developing a tool to measure the social impact of public health initiatives. Ann. Palliat. Med. 2018, 7 (Suppl. 1), AB007. [Google Scholar] [CrossRef] [PubMed]
- Bollig, G.; Brandt, F.; Ciurlionis, M.; Knopf, B. Last Aid Course. An Education For All Citizens and an Ingredient of Compassionate Communities. Healthcare 2019, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Kellehear, A. Compassionate communities: End-of-life care as everyone’s responsibility. QJM Int. J. Med. 2013, 106, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Etkind, S.N.; Bone, A.E.; Gomes, B.; Lovell, N.; Evans, C.J.; Higginson, I.J.; Murtagh, F.E.M. How many people will need palliative care in 2040? Past trends, future projections and implications for services. BMC Med. 2017, 15, 102. [Google Scholar] [CrossRef] [PubMed]
- Sallnow, L.; Smith, R.; Ahmedzai, S.H.; Bhadelia, A.; Chamberlain, C.; Cong, Y.; Doble, B.; Dullie, L.; Durie, R.; Finkelstein, E.A.; et al. Report of the Lancet Commission on the Value of Death: Bringing death back into life. Lancet 2022, 399, 837–884. [Google Scholar] [CrossRef]
- Bollig, G.; Brandt Kristensen, F.; Wolff, D.L. Citizens appreciate talking about death and learning end-of-life care—A mixed-methods study on views and experiences of 5469 Last aid Course participants. Prog. Palliat. Care 2021, 29, 140–148. [Google Scholar] [CrossRef]
- Bollig, G.; Hayes Bauer, E. Last Aid Courses as measure for public palliative care education—A narrative review. Ann. Pall. Med. 2021, 10, 8242–8253. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Ottawa Charter for Health Promotion; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- Westdeutscher Rundfunk. Der Alte Dachs (The Old Badger). Available online: https://www.youtube.com/watch?v=YMCg6DRJtrU (accessed on 27 December 2023).
- Milford Care Center. Bills Story—Talking Together Facing Death and Dying. Available online: https://www.youtube.com/watch?v=_5tJGaWjRZk (accessed on 27 December 2023).
- Knietzsche und der Tod (Knietzsche and Death). Available online: https://www.youtube.com/watch?v=1YGYzBi55JE (accessed on 27 December 2023).
- Mark Forster. Sowieso (Official Video). Available online: https://www.youtube.com/watch?v=jP4-XrbGt3M (accessed on 27 December 2023).
- Bollig, G.; Mainzer, K.; Fiedler, H.; Pothmann, R. The last aid course for kids and teens from 8–14 years: -preliminary results from the first pilot test. Hosp. Palliat. Med. Int. J. 2020, 4, 1–3. [Google Scholar]
- Letzte Hilfe Deutschland. Available online: https://www.letztehilfe.info (accessed on 27 December 2023).
- O’Cathain, A.; Thomas, K. Combining qualitative and quantitative methods. In Qualitative Research in Health Care, 3rd ed.; Pope, C., Mays, N., Eds.; Blackwell Publishing: Oxford, UK, 2006; pp. 102–111. [Google Scholar]
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description–the poor cousin of health research? BMC Med. Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef] [PubMed]
- Sandelowski, M. What’s in a name? Qualitative description revisited. Res. Nurs. Health 2010, 33, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K. Kvalitative Metoder i Medisinsk Forskning, 3rd ed.; Qualitative Methods in Medical Research, Universitetsforlaget: Oslo, Norway, 2011. [Google Scholar]
- Fancourt, D.; Finn, S. WHO-Report: What Is the Evidence on the Role of the Arts in Improving Health and Well-Being? A Scoping Review. Available online: https://www.artsandhealth.ie/research-evaluation/who-report-what-is-the-evidence-on-the-role-of-the-arts-in-improving-health-and-well-being-a-scoping-review/ (accessed on 27 December 2023).
- Freeman, J.; Epston, D.; Lobovits, D. Ernsten Problemen Spielerisch Begegnen. Narrative Therapie mit Kindern und ihren Familien; Modernes Lernen: Dortmund, Germany, 2000. [Google Scholar]
- Klinkhammer, G. Trauerbegleitung: Kinder trauern anders. Dtsch. Arztebl. 2012, 109. A-1787/B-1451/C-1427. [Google Scholar]
- St. Jude Childrens Research Hospital. Gender Differences in the Grieving Process. Available online: https://together.stjude.org/en-us/for-families/bereavement/gender-differences-in-grieving.html (accessed on 27 December 2023).
- MacAden, L.; Broadfoot, K.; Carolan, C.; Muirhead, K.; Neylon, S.; Keen, J. Last Aid Training Online: Participants’ and Facilitators’ Perceptions from a Mixed-Methods Study in Rural Scotland. Healthcare 2022, 10, 918. [Google Scholar] [CrossRef] [PubMed]
- Woodworth, J. Building Death Literacy Through Last Aid: An Examination of Agency, Ambivalence and Gendered Informal Caregiving within the Swedish Welfare State. NORA Nord. J. Fem. Gend. Res. 2023. [Google Scholar] [CrossRef]
- Mills, J.; Abel, J.; Kellehear, A.; Noonan, K.; Bollig, G.; Grindod, A.; Hamzah, E.; Haberecht, J. The role and contribution of compassionate communities. Lancet 2023. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Module Number | Topic | Course Content |
|---|---|---|
| Module 1 | Dying as a normal part of life |
|
| Module 2 | Planning ahead |
|
| Module 3 | Relieving suffering |
|
| Module 4 | Final goodbyes |
|
| Participants’ Impressions of the Course | Yes | No | No Response |
|---|---|---|---|
| Number and % | Number and % | Number and % | |
| 1. The Last Aid Course is helpful for everyone | 2297 | 164 | 73 |
| 91% | 6% | 3% | |
| 2. I will recommend the Last Aid Course to others | 1994 | 366 | 174 |
| 79% | 14% | 7% | |
| 3. All pupils should participate in a Last Aid course | 1748 | 604 | 182 |
| 69% | 24% | 7% | |
| 4. All parents should participate in a Last Aid course | 1666 | 682 | 186 |
| 66% | 27% | 7% | |
| 5. Should parents and children visit the course together? | 1012 | 1302 | 220 |
| 40% | 51% | 9% | |
| 6. I learned something new | 2337 | 139 | 58 |
| 93% | 5% | 2% | |
| 7. Were the course content easy to understand? | 2209 | 193 | 132 |
| 87% | 8% | 5% | |
| 8. Have you experienced that anyone in your family/circle of friends has died? | 2129 | 369 | 36 |
| 84% | 15% | 1% |
| Theme | Number of Participants | Percent |
|---|---|---|
| Videos | 265 | 10% |
| Painting stones | 250 | 10% |
| Game with swing cloth | 244 | 10% |
| Mouth care practice | 116 | 5% |
| Talking | 111 | 4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bollig, G.; Gräf, K.; Gruna, H.; Drexler, D.; Pothmann, R. “We Want to Talk about Death, Dying and Grief and to Learn about End-of-Life Care”—Lessons Learned from a Multi-Center Mixed-Methods Study on Last Aid Courses for Kids and Teens. Children 2024, 11, 224. https://doi.org/10.3390/children11020224
Bollig G, Gräf K, Gruna H, Drexler D, Pothmann R. “We Want to Talk about Death, Dying and Grief and to Learn about End-of-Life Care”—Lessons Learned from a Multi-Center Mixed-Methods Study on Last Aid Courses for Kids and Teens. Children. 2024; 11(2):224. https://doi.org/10.3390/children11020224
Chicago/Turabian StyleBollig, Georg, Kirsti Gräf, Harry Gruna, Daniel Drexler, and Raymund Pothmann. 2024. "“We Want to Talk about Death, Dying and Grief and to Learn about End-of-Life Care”—Lessons Learned from a Multi-Center Mixed-Methods Study on Last Aid Courses for Kids and Teens" Children 11, no. 2: 224. https://doi.org/10.3390/children11020224