
Spoken Expressive Vocabulary in 2-Year-Old Children with Hearing Loss: A Community Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Participants with Permanent Hearing Loss
2.3. Participants without Known Permanent Hearing Loss
2.4. Outcome
2.5. Exposures
2.6. Potential Confounders
2.7. Statistical Analyses
2.7.1. Aim 1
2.7.2. Aim 2
3. Results
3.1. Sample Characteristics
3.2. Aim 1: Impact of Hearing Loss on Expressive Vocabulary
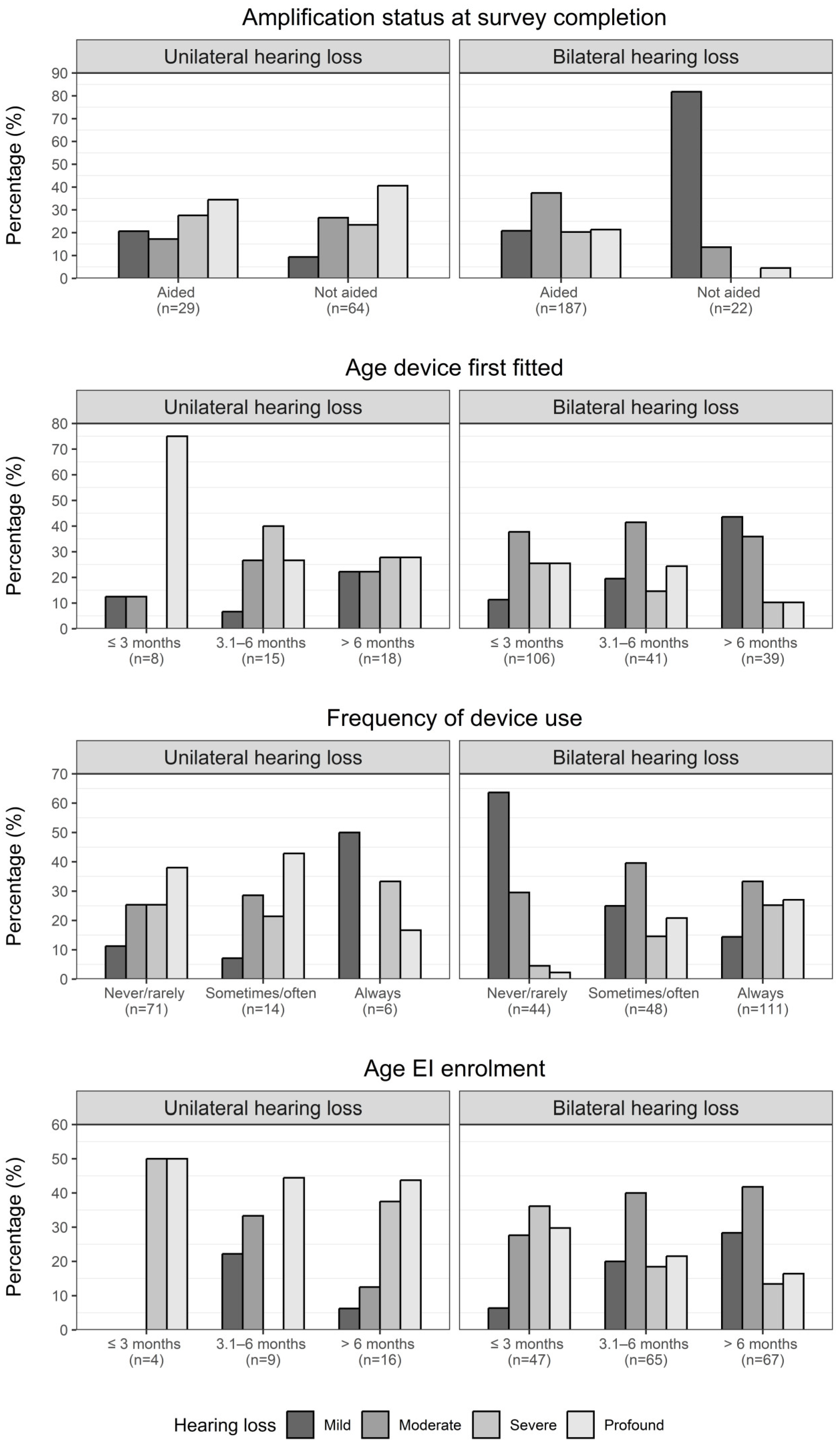
3.3. Aim 2: Impact of Intervention-Related Factors on Expressive Vocabulary in Children with Hearing Loss
4. Discussion
4.1. Principal Findings
4.2. Strengths of the Study
4.3. Limitations
4.4. Interpretation in Light of Other Studies
5. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Supplementary Methods: Statistical Analyses
References
- Sininger, Y.S.; Martinez, A.; Eisenberg, L.; Christensen, E.; Grimes, A.; Hu, J. Newborn hearing screening speeds diagnosis and access to intervention by 20–25 months. J. Am. Acad. Audiol. 2009, 20, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, S.A.; Sutton, G.J.; Davis, A.C. Performance and characteristics of the Newborn Hearing Screening Programme in England: The first seven years. Int. J. Audiol. 2015, 54, 353–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, C.R.; McCann, D.C.; Campbell, M.J.; Law, C.M.; Mullee, M.; Petrou, S.; Watkin, P.; Worsfold, S.; Yuen, H.M.; Stevenson, J. Language ability after early detection of permanent childhood hearing impairment. N. Engl. J. Med. 2006, 354, 2131–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ching, T.Y.C.; Dillon, H.; Leigh, G.; Cupples, L. Learning from the Longitudinal Outcomes of Children with Hearing Impairment (LOCHI) study: Summary of 5-year findings and implications. Int. J. Audiol. 2018, 57, S105–S111. [Google Scholar] [CrossRef]
- Wake, M.; Ching, T.; Wirth, K.; Poulakis, Z.; Mensah, F.K.; Gold, L.; King, A.; Bryson, H.; Reilly, S.; Rickards, F. Population Outcomes of Three Approaches to Detection of Congenital Hearing Loss. Pediatrics 2016, 137, e20151722. [Google Scholar] [CrossRef] [Green Version]
- Fulcher, A.; Purcell, A.A.; Baker, E.; Munro, N. Listen up: Children with early identified hearing loss achieve age-appropriate speech/language outcomes by 3 years-of-age. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1785–1794. [Google Scholar] [CrossRef]
- Stika, C.J.; Eisenberg, L.S.; Johnson, K.C.; Henning, S.C.; Colson, B.G.; Ganguly, D.H.; DesJardin, J.L. Developmental outcomes of early-identified children who are hard of hearing at 12 to 18 months of age. Early Hum. Dev. 2015, 91, 47–55. [Google Scholar] [CrossRef] [Green Version]
- Stika, C.J.; Eisenberg, L.S.; Carter, A.S.; Johnson, K.C.; Ganguly, D.M.H.; Henning, S.C.; DesJardin, J.L. Developmental Outcomes in Early-Identified Children Who Are Hard of Hearing at 2 to 3 Years of Age. Ear. Hear 2021. publish ahead of print. [Google Scholar] [CrossRef]
- Yoshinaga-Itano, C.; Sedey, A.L.; Wiggin, M.; Chung, W. Early Hearing Detection and Vocabulary of Children with Hearing Loss. Pediatrics 2017, 140, e20162964. [Google Scholar] [CrossRef] [Green Version]
- Ching, T.Y.C. Is Early Intervention Effective in Improving Spoken Language Outcomes of Children with Congenital Hearing Loss? Am. J. Audiol. 2015, 24, 345–348. [Google Scholar] [CrossRef] [Green Version]
- Whitehouse, A.J.O.; Robinson, M.; Zubrick, S.R. Late Talking and the Risk for Psychosocial Problems during Childhood and Adolescence. Pediatrics 2011, 128, e324–e332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J. Size matters: Early vocabulary as a predictor of language and literacy competence. Appl. Psycholinguist. 2011, 32, 69–92. [Google Scholar] [CrossRef]
- Can, D.D.; Ginsburg-Block, M.; Golinkoff, R.M.; Hirsh-Pasek, K. A long-term predictive validity study: Can the CDI Short Form be used to predict language and early literacy skills four years later? J. Child Lang. 2013, 40, 821–835. [Google Scholar] [CrossRef] [PubMed]
- Carew, P.; Mensah, F.K.; Rance, G.; Flynn, T.; Poulakis, Z.; Wake, M. Mild-moderate congenital hearing loss: Secular trends in outcomes across four systems of detection. Child Care Health Dev. 2017, 44, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Sung, V.; Smith, L.; Poulakis, Z.; A Burt, R.; Carew, P.; Tobin, S.; Wake, M. Data Resource Profile: The Victorian Childhood Hearing Impairment Longitudinal Databank (VicCHILD). Int. J. Epidemiol. 2019, 48, 1409–1410h. [Google Scholar] [CrossRef]
- Reilly, S.; Bavin, E.L.; Bretherton, L.; Conway, L.; Eadie, P.; Cini, E.; Prior, M.; Ukoumunne, O.C.; Wake, M. The Early Language in Victoria Study (ELVS): A prospective, longitudinal study of communication skills and expressive vocabulary development at 8, 12 and 24 months. Int. J. Speech Lang Pathol. 2009, 11, 344–357. [Google Scholar] [CrossRef]
- Reilly, S.; Cook, F.; Bavin, E.L.; Bretherton, L.; Cahir, P.; Eadie, P.; Gold, L.; Mensah, F.; Papadopoullos, S.; Wake, M. Cohort Profile: The Early Language in Victoria Study (ELVS). Int. J. Epidemiol. 2017, 47, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Fenson, L.; Marchman, V.A.; Thal, D.J.; Dale, P.S.; Reznick, J.S.; Bates, E. The MacArthur-Bates Communicative Development Inventories User’s Guide and Technical Manual, 2nd ed.; Brookes Publishing: Baltimore, MA, USA, 2006. [Google Scholar]
- Roy, P.; Kersley, H.; Law, J. The Sure Start Language Measure Standardisation Study; City University: Nottingham, UK, 2005. [Google Scholar]
- Dale, P.S.; Dionne, G.; Eley, T.C.; Plomin, R. Lexical and grammatical development: A behavioural genetic perspective. J. Child Lang. 2000, 27, 619–642. [Google Scholar] [CrossRef]
- Rose, E.; Sung, V. Otolaryngology. In Paediatric Handbook, 10th ed.; Harding, K., Mason, D.S., Efron, D., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2022; Available online: http://ebookcentral.proquest.com/lib/unimelb/detail.action?docID=6375231 (accessed on 3 August 2022).
- R Core Team. R: A Language and Environment for Statistical Computing. 2017. Available online: https://www.R-project.org/ (accessed on 9 July 2023).
- Hernán, M.; Robins, J. Causal Inference: What If; Chapman & Hall/CRC: Boca Raton, FL, USA, 2020. [Google Scholar]
- The Joint Committee on Infant Hearing. Year 2019 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. J. Early Hear. Detect. Interv. 2019, 4, 1–44. [Google Scholar] [CrossRef]
- Vohr, B.; Jodoin-Krauzyk, J.; Tucker, R.; Topol, D.; Johnson, M.J.; Ahlgren, M.; Pierre, L. Expressive vocabulary of children with hearing loss in the first 2 years of life: Impact of early intervention. J. Perinatol. 2011, 31, 274–280. [Google Scholar] [CrossRef] [Green Version]
- McCreery, R.W.; Walker, E.A.; Spratford, M. Understanding Limited Use of Amplification in Infants and Children Who Are Hard of Hearing. Perspect Hear Hear Disord Child. 2015, 25, 15–23. [Google Scholar] [CrossRef]
- Halliday, L.F.; Tuomainen, O.; Rosen, S. Language Development and Impairment in Children with Mild to Moderate Sensorineural Hearing Loss. J. Speech Lang Hear. Res. 2017, 60, 1551–1567. [Google Scholar] [CrossRef] [Green Version]
- Edquist, G.; Flynn, T.; Jennische, M. Expressive vocabulary of school-age children with mild to moderately severe hearing loss. Int. J. Pediatr. Otorhinolaryngol. 2022, 162, 111281. [Google Scholar] [CrossRef]
- Tomblin, J.B.; Harrison, M.; Ambrose, S.E.; Walker, E.A.; Oleson, J.J.; Moeller, M.P. Language Outcomes in Young Children with Mild to Severe Hearing Loss. Ear Hear. 2015, 36, 76S–91S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, E.M.; Durieux-Smith, A.; Gaboury, I.; Coyle, D.; Whittingham, J. Communication Development in Early- Identified Children with Mild Bilateral and Unilateral Hearing Loss. Am. J. Audiol. 2015, 24, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Yoshinaga-Itano, C.; Manchaiah, V.; Hunnicutt, C. Outcomes of Universal Newborn Screening Programs: Systematic Review. J. Clin. Med. 2021, 10, 2784. [Google Scholar] [CrossRef]
- Martin, R.M. Epidemiological study designs for health care research and evaluation. In Handbook of Health Research Methods: Investigation, Measurement and Analysis, 1st ed.; Bowling, A., Ebrahim, S., Eds.; Open University Press: London, UK, 2005; pp. 98–163. [Google Scholar]
- Morgan, P.; Farkas, G.; Hillemeier, M.; Scheffner Hammer, C.; Maczuga, S. 24-Month-Old Children with Larger Oral Vocabularies Display Greater Academic and Behavioral Functioning at Kindergarten Entry. Child Dev. 2015, 86, 1351–1370. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Hearing Loss Group (n = 302) | No Hearing Loss Group (n = 1742) | ||||||
|---|---|---|---|---|---|---|---|
| Missing a n (%) | Missing a n (%) | ||||||
| Demographicinformation | |||||||
| Age at assessment, months—mean (SD) | 0 (0) | 25.4 (1.7) | 0 (0) | 24.2 (0.4) | |||
| Sex: male—n (%) | 0 (0) | 170 (56.3) | 0 (0) | 887 (50.9) | |||
| Parent’s education—n (%) | 11 (3.6) | 23 (1.3) | |||||
| Year 10 or less | 21 (7.2) | 150 (8.7) | |||||
| Year 11 | 13 (4.5) | 234 (13.6) | |||||
| Year 12 | 83 (28.5) | 692 (40.3) | |||||
| Tertiary or Postgraduate | 174 (59.8) | 643 (37.4) | |||||
| Primary language at home—n (%) | 12 (4.0) | 8 (0.5) | |||||
| English only | 166 (57.2) | 1644 (94.8) | |||||
| Bilingual (English and other language) | 89 (30.7) | 18 (1.0) | |||||
| Other language only | 35 (12.1) | 72 (4.2) | |||||
| Disadvantage Index, SEIFA—mean (SD) | 1 (0.3) | 1015.6 (61.1) | 1 (0.1) | 1037.6 (59.6) | |||
| Birth-related factors | |||||||
| NICU admission: yes—n (%) | 7 (2.3) | 50 (17.0) | 0 (0) | 284 (16.3) | |||
| Gestational age, weeks—mean (SD) | 1 (0.3) | 38.3 (2.6) | 152 (8.7) | 39.3 (1.8) | |||
| Hearing status—n (%) | 0 (0) | 0 (0) | |||||
| Normal hearing | — | 1742 (100.0) | |||||
| Unilateral hearing loss | 93 (30.8) | — | |||||
| Mild | 12 (4.0) | — | |||||
| Moderate | 22 (7.3) | — | |||||
| Severe | 23 (7.6) | — | |||||
| Profound | 36 (11.9) | — | |||||
| Bilateral hearing loss | 209 (69.2) | — | |||||
| Mild | 57 (18.9) | — | |||||
| Moderate | 73 (24.2) | — | |||||
| Severe | 38 (12.6) | — | |||||
| Profound | 41 (13.6) | — | |||||
| Outcome measures | |||||||
| SSLM score, standardized—mean (SD) | 0 (0) | 88.5 (16.8) | 0 (0) | 98.7 (13.4) | |||
| Combining words yet—n (%) | 24 (8.0) | 30 (1.7) | |||||
| Not yet | 81 (29.1) | 290 (16.9) | |||||
| Sometimes | 82 (29.5) | 573 (33.5) | |||||
| Always | 115 (41.4) | 849 (49.6) | |||||
| Unadjusted | Adjusted a | Adjusted b | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Difference | 95% CI | p-Value | Adj. Mean Difference | 95% CI | p-Value | Adj. Mean Difference | 95% CI | p-Value | Adj. Mean b | ||
| Without hearing loss (ref) | — | — | — | — | — | — | — | — | — | 96.1 | |
| Hearing loss: Unilateral | |||||||||||
| Mild | −3.19 | (−11.08, 4.69) | 0.43 | −3.43 | (−24.27, 12.92) | 0.73 | −1.46 | (−21.66, 13.46) | 0.88 | 94.7 | |
| Moderate | −8.19 | (−14.56, −8.06) | <0.01 | −4.12 | (−11.75, 3.29) | 0.28 | −3.93 | (−11.63, 3.47) | 0.31 | 92.2 | |
| Severe | −4.35 | (−10.06, 1.37) | 0.14 | −2.17 | (−9.57, 5.51) | 0.57 | −2.22 | (−9.63, 5.24) | 0.56 | 93.9 | |
| Profound | −5.97 | (−10.56, −1.39) | 0.01 | −4.50 | (−10.42, 0.62) | 0.11 | −4.37 | (−10.26, 0.71) | 0.13 | 91.8 | |
| Hearing loss: Bilateral | |||||||||||
| Mild | −9.01 | (−12.68, −5.34) | <0.01 | −7.65 | (−11.76, −2.90) | <0.01 | −7.31 | (−11.38, −2.48) | <0.01 | 88.8 | |
| Moderate | −11.31 | (−14.56, −8.06) | <0.01 | −9.23 | (−13.25, −4.76) | <0.01 | −8.36 | (−12.39, −4.20) | <0.01 | 87.8 | |
| Severe | −15.98 | (−20.45, −11.52) | <0.01 | −13.51 | (−17.79, −9.32) | <0.01 | −13.35 | (−17.78, −9.13) | <0.01 | 82.8 | |
| Profound | −14.77 | (−19.07, −10.46) | <0.01 | −13.91 | (−18.86, −8.80) | <0.01 | −13.54 | (−18.53, −8.37) | <0.01 | 82.6 | |
| Missing Information a n (%) | Hearing Loss Group (N = 302) | Unilateral Loss (N = 93) | Bilateral Loss (N = 209) | |||
|---|---|---|---|---|---|---|
| Age at diagnosis (months) | 61 (30.2) | |||||
| median (IQR) | 1.0 (0.6, 1.6) | 1.0 (0.7, 1.6) | 0.8 (0.6, 1.4) | |||
| UNHS detected—n (%) | 0 (0) | 290 (96.0) | 91 (97.8) | 199 (95.2) | ||
| Any hearing device used ever—n (%) | 0 (0) | 231 (76.5) | 41 (44.1) | 190 (90.9) | ||
| Any hearing device used at survey—n (%) | 0 (0) | 216 (71.5) | 29 (31.2) | 187 (89.5) | ||
| Hearing aid only | 152 (50.3) | 27 (29.0) | 125 (59.8) | |||
| Cochlear implant only | 41 (13.6) | 2 (2.2) | 39 (18.7) | |||
| Hearing aid and cochlear implant | 23 (7.6) | 0 (0) | 23 (11.0) | |||
| None | 86 (28.5) | 64 (68.8) | 22 (10.5) | |||
| Age first hearing device fitted, continuous (months) | 75 (24.8) | |||||
| median (IQR) | 3 (2, 6.5) | 6 (4, 12) | 3 (2, 6) | |||
| Age first hearing device fitted, categorical—n (%) | 75 (24.8) | |||||
| ≤3 months | 114 (50.2) | 36 (45.0) | 78 (53.6) | |||
| 3.1–6 months | 56 (24.7) | 23 (28.8) | 33 (22.5) | |||
| >6 months | 57 (25.1) | 21 (26.3) | 36 (24.5) | |||
| Average hearing device use: week day—n (%) | 8 (2.6) | |||||
| Never/rarely, <4 h | 115 (39.1) | 71 (15.4) | 44 (21.9) | |||
| Sometimes/often, 4–8 h | 62 (21.1) | 14 (78.0) | 48 (23.9) | |||
| Always, >8 h | 117 (39.8) | 6 (6.6) | 111 (55.2) | |||
| EI service used ever—n (%) | 2 (0.7) | 225 (75.0) | 39 (41.9) | 186 (89.9) | ||
| EI service used at survey—n (%) | 78 (25.8) | 209 (93.3) | 29 (78.4) | 180 (96.3) | ||
| Age EI program enrolment (months) | 94 (31.1) | |||||
| median (IQR) | 6 (4, 10) | 8 (5, 12) | 6 (3, 9) | |||
| Age EI program enrolment—n (%) | 94 (31.1) | |||||
| ≤3 months | 51 (24.5) | 4 (13.8) | 47 (26.3) | |||
| 3.1–6 months | 74 (35.6) | 9 (31.0) | 65 (36.3) | |||
| >6 months | 83 (39.9) | 16 (55.2) | 67 (37.4) | |||
| Unadjusted | Adjusted a | Adjusted b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Difference | 95% CI | p-Value | Adj. Mean Difference | 95% CI | p-Value | Adj. Mean Difference | 95% CI | p-Value | n * | Adj. Mean b | ||
| Hearing device used at survey | 199 | |||||||||||
| No (ref) | — | — | — | — | — | — | — | — | — | 90.6 | ||
| Yes | −2.81 | (−10.16, 4.54) | 0.45 | −4.23 | (−12.16, 3.71) | 0.30 | −5.36 | (−13.21, 2.50) | 0.18 | 85.2 | ||
| Age hearing device fitted | 177 | |||||||||||
| <3 months (ref) | — | — | — | — | — | — | — | — | — | 88.0 | ||
| 3.1–6 months | −10.49 | (−16.11, −4.87) | <0.01 | −9.82 | (−15.16, −4.47) | <0.01 | −8.59 | (−14.10, −3.08) | <0.01 | 79.4 | ||
| >6 months | −3.79 | (−9.52, 1.93) | 0.19 | −5.66 | (−11.39, 0.08) | 0.05 | −4.31 | (−10.30, 1.69) | 0.16 | 83.6 | ||
| Average hearing device use | 193 | |||||||||||
| Always (ref) | — | — | — | — | — | — | — | — | — | 86.1 | ||
| Sometimes/often | −5.75 | (−11.32, −0.18) | 0.04 | −5.06 | (−10.31, 0.20) | 0.06 | −4.62 | (−9.80, 0.57) | 0.08 | 81.4 | ||
| Never/rarely | 2.55 | (−3.20, 8.30) | 0.38 | 3.27 | (−3.07, 9.61) | 0.31 | 3.39 | (−2.86, 9.63) | 0.29 | 89.4 | ||
| Age EI program enrolment | 171 | |||||||||||
| <3 months (ref) | — | — | — | — | — | — | — | — | — | 91.3 | ||
| 3.1–6 months | −2.99 | (−8.88, 2.90) | 0.32 | −5.60 | (−11.11, −0.10) | 0.05 | −5.44 | (−10.95, 0.07) | 0.05 | 85.8 | ||
| >6 months | −8.92 | (−14.78, −3.06) | <0.01 | −10.59 | (−16.28, −4.91) | <0.01 | −9.95 | (−15.68, −4.22) | <0.01 | 81.3 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carew, P.; Shepherd, D.A.; Smith, L.; Howell, T.; Lin, M.; Bavin, E.L.; Reilly, S.; Wake, M.; Sung, V. Spoken Expressive Vocabulary in 2-Year-Old Children with Hearing Loss: A Community Study. Children 2023, 10, 1223. https://doi.org/10.3390/children10071223
Carew P, Shepherd DA, Smith L, Howell T, Lin M, Bavin EL, Reilly S, Wake M, Sung V. Spoken Expressive Vocabulary in 2-Year-Old Children with Hearing Loss: A Community Study. Children. 2023; 10(7):1223. https://doi.org/10.3390/children10071223
Chicago/Turabian StyleCarew, Peter, Daisy A. Shepherd, Libby Smith, Tegan Howell, Michelle Lin, Edith L. Bavin, Sheena Reilly, Melissa Wake, and Valerie Sung. 2023. "Spoken Expressive Vocabulary in 2-Year-Old Children with Hearing Loss: A Community Study" Children 10, no. 7: 1223. https://doi.org/10.3390/children10071223