Circulating Brain Injury Exosomal Proteins following Moderate-to-Severe Traumatic Brain Injury: Temporal Profile, Outcome Prediction and Therapy Implications

 , , ,
, , ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population and Sample Collection
2.2. Extracellular Vesicles (EVs) Isolation and Characterization
2.3. Exosomal Protein Quantification
2.4. Measurement of Circulating Protein Concentrations
2.5. Statistical Analysis
3. Results
3.1. Description of Population
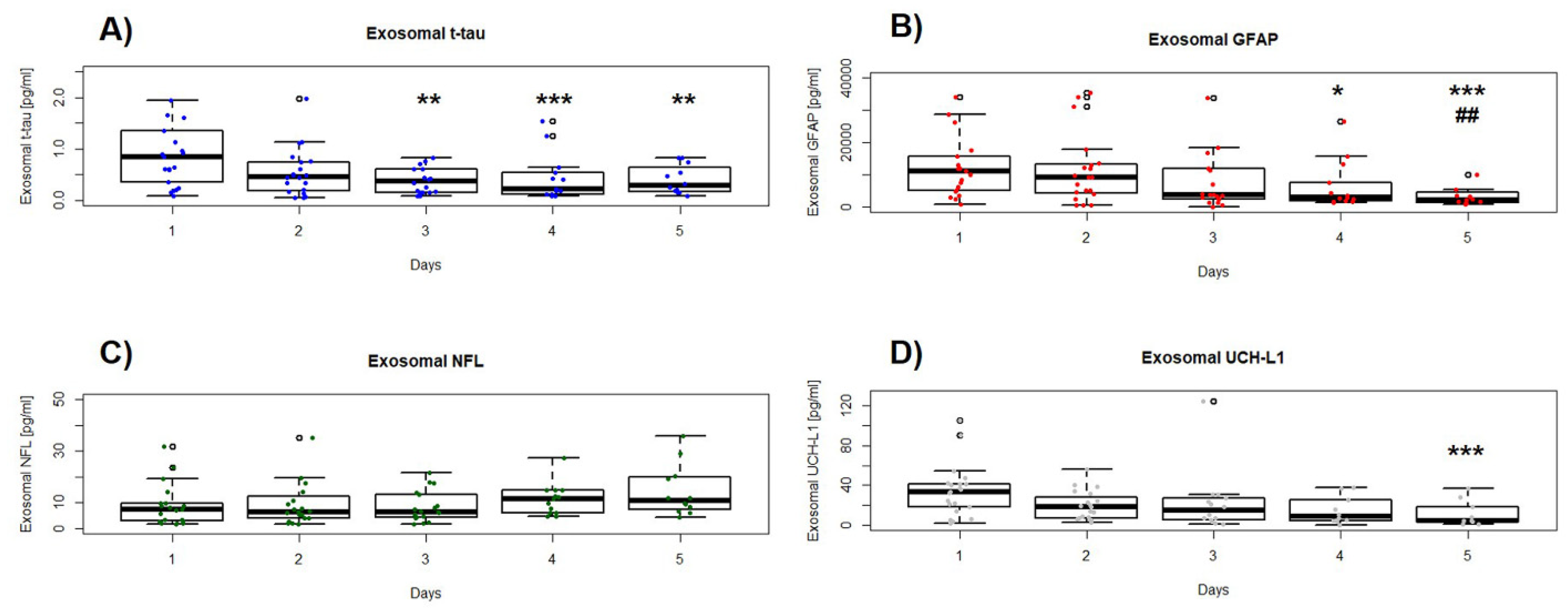
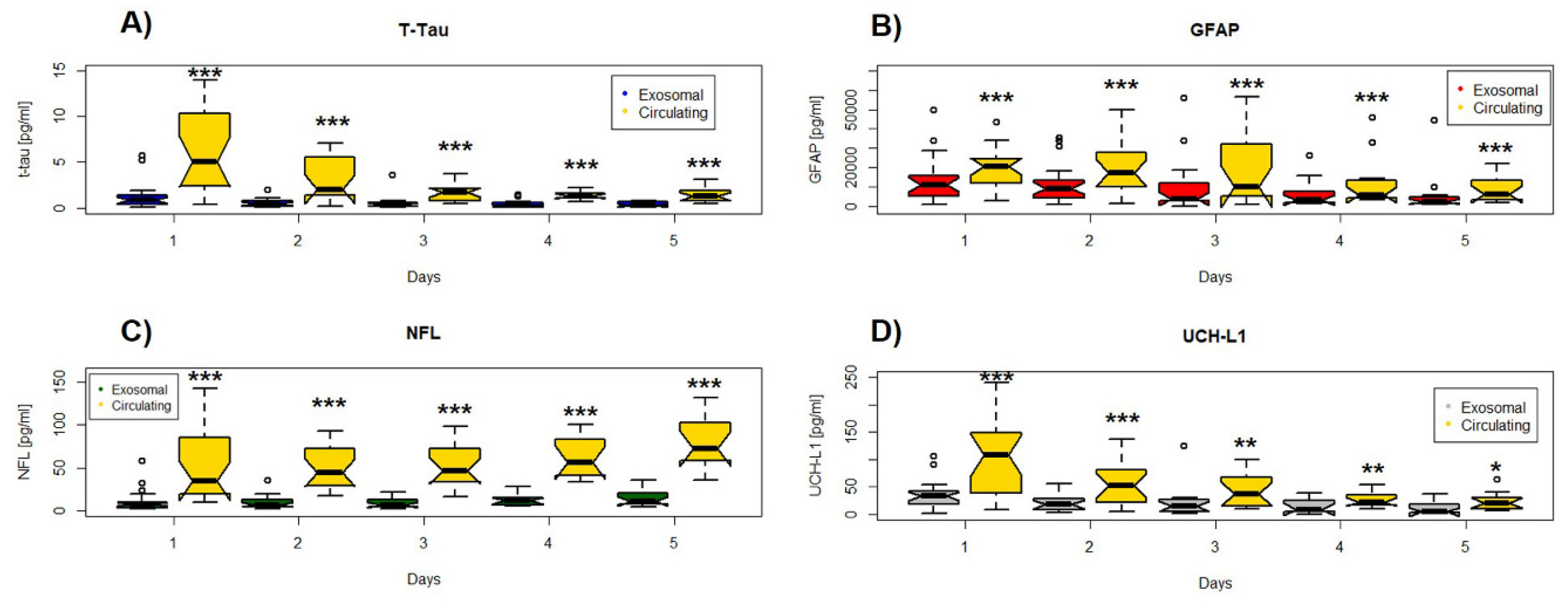
3.2. Concentrations and Longitudinal Profiles of Serum Exosomal Brain Damage Biomarkers
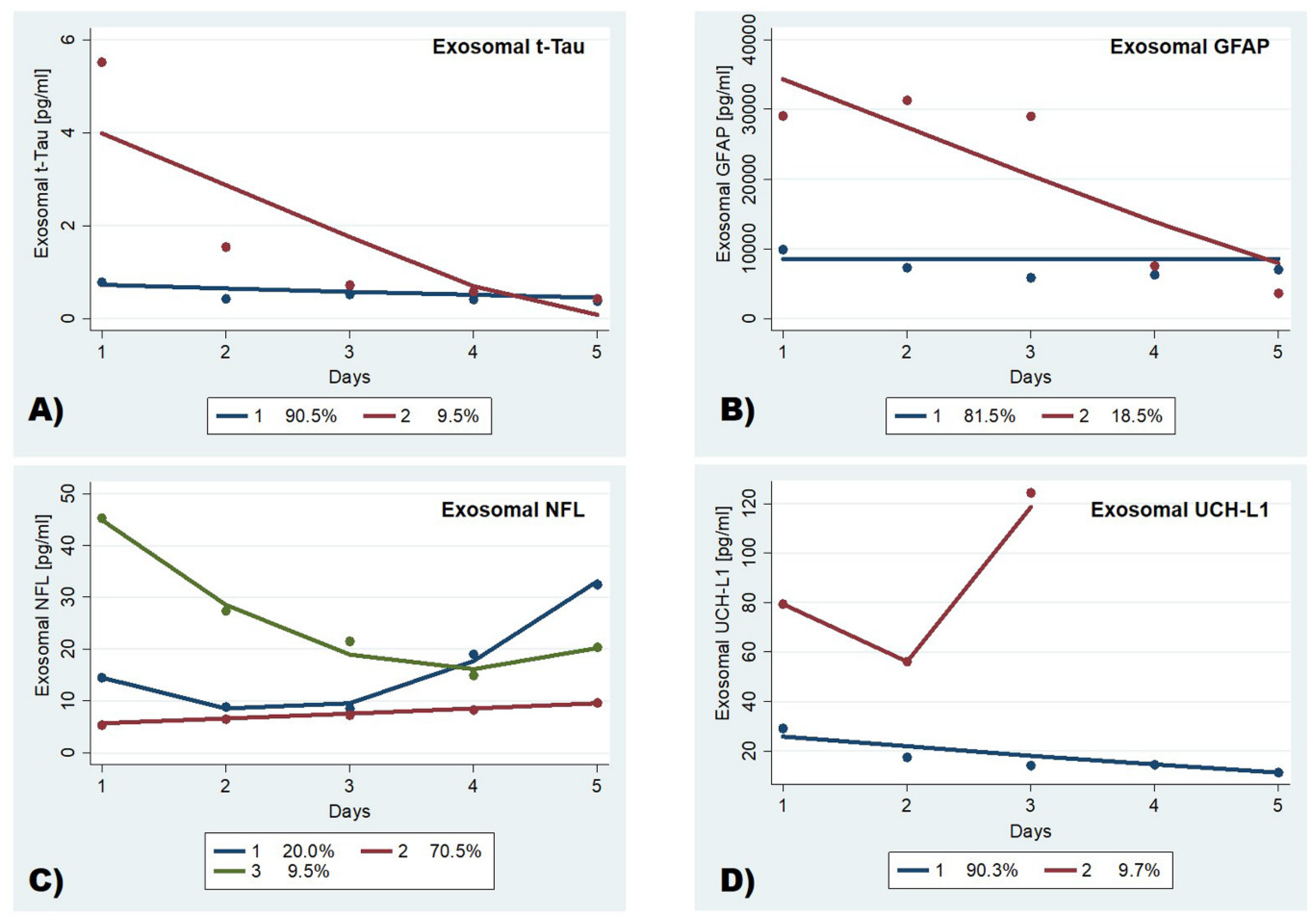
3.3. Trajectory Profiles of Serum Exosomal Brain Damage Biomarkers in Moderate-to-Severe TBI Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Maas, A.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef] [Green Version]
- GBD 2016 Traumatic Brain Injury; Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 56–87. [Google Scholar] [CrossRef] [Green Version]
- Roozenbeek, B.; Maas, A.; Menon, D.K. Changing patterns in the epidemiology of traumatic brain injury. Nat. Rev. Neurol. 2013, 9, 231–236. [Google Scholar] [CrossRef]
- Stocchetti, N.; Carbonara, M.; Citerio, G.; Ercole, A.; Skrifvars, M.B.; Smieleweski, P.; Zoerle, T.; Menon, D.K. Severe traumatic brain injury: Targeted management in the intensive care unit. Lancet Neurol. 2017, 16, 452–464. [Google Scholar] [CrossRef] [Green Version]
- Spitz, G.; Downing, M.; McKenzie, D.; Ponsford, J.L. Mortality following Traumatic Brain Injury Inpatient Rehabilitation. J. Neurotrauma 2015, 32, 1272–1280. [Google Scholar] [CrossRef]
- Mondello, S.; Thelin, E.; Shaw, G.; Salzet, M.; Visalli, C.; Cizkova, D.; Kobeissy, F.; Büki, A.; Salzet, M. Extracellular vesicles: Pathogenetic, diagnostic and therapeutic value in traumatic brain injury. Expert Rev. Proteom. 2018, 15, 451–461. [Google Scholar] [CrossRef]
- Tian, Y.; Salsbery, B.; Wang, M.; Yuan, H.; Yang, J.; Zhao, Z.; Wu, X.; Zhang, Y.; Konkle, B.A.; Thiagarajan, P.; et al. Brain-derived microparticles induce systemic coagulation in a murine model of traumatic brain injury. Blood 2015, 125, 2151–2159. [Google Scholar] [CrossRef] [Green Version]
- Osier, N.; Motamedi, V.; Edwards, K.; Puccio, A.; Diaz-Arrastia, R.; Kenney, K.; Gill, J. Exosomes in Acquired Neurological Disorders: New Insights into Pathophysiology and Treatment. Mol. Neurobiol. 2018, 55, 9280–9293. [Google Scholar] [CrossRef]
- Mondello, S.; Papa, L.; Büki, A.; Bullock, M.R.; Czeiter, E.; Tortella, F.C.; Wang, K.K.; Hayes, R.L. Neuronal and glial markers are differently associated with computed tomography findings and outcome in patients with severe traumatic brain injury: A case control study. Crit. Care 2011, 15, R156. [Google Scholar] [CrossRef] [Green Version]
- Shahim, P.; Gren, M.; Liman, V.; Andreasson, U.; Norgren, N.; Tegner, Y.; Mattsson, N.; Andreasen, N.; Öst, M.; Zetterberg, H.; et al. Serum neurofilament light protein predicts clinical outcome in traumatic brain injury. Sci Rep. 2016, 6, 36791. [Google Scholar] [CrossRef]
- Hellewell, S.C.; Mondello, S.; Conquest, A.; Shaw, G.; Madorsky, I.; Deng, J.V.; Little, L.; Kobeissy, F.; Bye, N.; Bellomo, R.; et al. Erythropoietin Does Not Alter Serum Profiles of Neuronal and Axonal Biomarkers After Traumatic Brain Injury. Crit. Care Med. 2018, 46, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; Mukherjee, P.; Valadka, A.B.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau-Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol. 2017, 74, 1063–1072. [Google Scholar] [CrossRef]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.; Bratton, S.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2016, 80, 6–15. [Google Scholar] [CrossRef]
- Nationa Institute for Health and Care Excellence, Head Injury: Triage, Assessment, Investigation and Early Management of Head in-Jury in Children, Young People and Adults. 2014. Available online: https://www.nice.org.uk/guidance/CG176 (accessed on 24 February 2020).
- Gill, J.; Latour, L.; Diaz-Arrastia, R.; Motamedi, V.; Turtzo, C.; Shahim, P.; Mondello, S.; Devoto, C.; Veras, E.; Hanlon, D.; et al. Glial fibrillary acidic protein elevations relate to neuroimaging abnormalities after mild TBI. Neurology 2018, 91, e1385–e1389. [Google Scholar] [CrossRef] [PubMed]
- Mondello, S.; Büki, A.; Italiano, D.; Jeromin, A. -Synuclein in CSF of patients with severe traumatic brain injury. Neurology 2013, 80, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.K.; McCullough, E.H.; Niyonkuru, C.; Ozawa, H.; Loucks, T.; Dobos, J.A.; Brett, C.A.; Santarsieri, M.; Dixon, C.E.; Berga, S.L.; et al. Acute Serum Hormone Levels: Characterization and Prognosis after Severe Traumatic Brain Injury. J. Neurotrauma 2011, 28, 871–888. [Google Scholar] [CrossRef] [Green Version]
- Wan, M.; Ning, B.; Spiegel, S.; Lyon, C.J.; Hu, T.Y. Tumor-derived exosomes (TDEs): How to avoid the sting in the tail. Med. Res. Rev. 2019, 40, 385–412. [Google Scholar] [CrossRef]
- Duan, P.; Tan, J.; Miao, Y.; Zhang, Q. Potential role of exosomes in the pathophysiology, diagnosis, and treatment of hypoxic diseases. Am. J. Transl. Res. 2019, 11, 1184–1201. [Google Scholar]
- Ferreira, J.V.; Rosa Soares, A.; Ramalho, J.S.; Ribeiro-Rodrigues, T.; Máximo, C.; Zuzarte, M.; Girão, H.; Pereira, P. Exosomes and STUB1/CHIP cooperate to maintain intracellular proteostasis. PLoS ONE 2019, 14, e0223790. [Google Scholar] [CrossRef] [Green Version]
- Shi, M.; Sheng, L.; Stewart, T.; Zabetian, C.P.; Zhang, J. New windows into the brain: Central nervous system-derived extracellular vesicles in blood. Prog. Neurobiol. 2019, 175, 96–106. [Google Scholar] [CrossRef]
- Nutma, E.; Gent, D.; Amor, S.; Peferoen, L. Astrocyte and Oligodendrocyte Cross-Talk in the Central Nervous System. Cells 2020, 9, 600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halford, J.; Shen, S.; Itamura, K.; Levine, J.; Chong, A.; Czerwieniec, G.; Glenn, T.; A Hovda, D.; Vespa, P.; Bullock, R.; et al. New astroglial injury-defined biomarkers for neurotrauma assessment. Br. J. Pharmacol. 2017, 37, 3278–3299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkas, O.; Lifshitz, J.; Povlishock, J.T. Mechanoporation Induced by Diffuse Traumatic Brain Injury: An Irreversible or Reversible Response to Injury? J. Neurosci. 2006, 26, 3130–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sword, J.; Masuda, T.; Croom, D.; Kirov, S.A. Evolution of neuronal and astroglial disruption in the peri-contusional cortex of mice revealed by in vivo two-photon imaging. Brain 2013, 136, 1446–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.H.; Uryu, K.; E Saatman, K.; Trojanowski, J.Q.; McIntosh, T.K. Protein Accumulation in Traumatic Brain Injury. NeuroMolecular Med. 2003, 4, 59–72. [Google Scholar] [CrossRef]
- Zetterberg, H. Tauomics and Kinetics in Human Neurons and Biological Fluids. Neuron 2018, 97, 1202–1205. [Google Scholar] [CrossRef] [Green Version]
- Day, I.N.; Thompson, R.J. UCHL1 (PGP 9.5): Neuronal biomarker and ubiquitin system protein. Prog. Neurobiol. 2010, 90, 327–362. [Google Scholar] [CrossRef]
- Thompson, A.G.; Gray, E.; Heman-Ackah, S.M.; Mäger, I.; Talbot, K.; El Andaloussi, S.; Wood, M.J.; Turner, M.R. Extracellular vesicles in neurodegenerative disease — pathogenesis to biomarkers. Nat. Rev. Neurol. 2016, 12, 346–357. [Google Scholar] [CrossRef]
- Thelin, E.; Zeiler, F.A.; Ercole, A.; Mondello, S.; Büki, A.; Bellander, B.-M.; Helmy, A.; Menon, D.K.; Nelson, D.W. Serial Sampling of Serum Protein Biomarkers for Monitoring Human Traumatic Brain Injury Dynamics: A Systematic Review. Front. Neurol. 2017, 8, 300. [Google Scholar] [CrossRef] [Green Version]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef]
- Yue, J.K.; Yuh, E.L.; Korley, F.K.; A Winkler, E.; Sun, X.; Puffer, R.C.; Deng, H.; Choy, W.; Chandra, A.; Taylor, S.R.; et al. Association between plasma GFAP concentrations and MRI abnormalities in patients with CT-negative traumatic brain injury in the TRACK-TBI cohort: A prospective multicentre study. Lancet Neurol. 2019, 18, 953–961. [Google Scholar] [CrossRef]
- Roozenbeek, B.; Lingsma, H.F.; Maas, A. New considerations in the design of clinical trials for traumatic brain injury. Clin. Investig. 2012, 2, 153–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roozenbeek, B.; Lingsma, H.F.; Lecky, F.E.; Lu, J.; Weir, J.; Butcher, I.; McHugh, G.S.; Murray, G.; Perel, P.; Maas, A.; et al. Prediction of outcome after moderate and severe traumatic brain injury. Crit. Care Med. 2012, 40, 1609–1617. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W.; Mushkudiani, N.; Perel, P.; Butcher, I.; Lu, J.; McHugh, G.S.; Murray, G.; Marmarou, A.; Roberts, I.; Habbema, J.D.F.; et al. Predicting Outcome after Traumatic Brain Injury: Development and International Validation of Prognostic Scores Based on Admission Characteristics. PLoS Med. 2008, 5, e165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steyerberg, E.W.; Moons, K.G.M.; Van Der Windt, D.A.; Hayden, J.A.; Perel, P.; Schroter, S.; Riley, R.D.; Hemingway, H.; Altman, D.G. Prognosis Research Strategy (PROGRESS) 3: Prognostic Model Research. PLoS Med. 2013, 10, e1001381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, P.; De-La-Cruz, J.; Lora, D.; Jimenez-Roldan, L.; Rodríguez-Boto, G.; Sarabia, R.; Sahuquillo, J.; Lastra, R.; Morera, J.; Lazo, E.; et al. Validation of a prognostic score for early mortality in severe head injury cases. J. Neurosurg. 2014, 121, 1314–1322. [Google Scholar] [CrossRef]
- Rodríguez-Boto, G.; Gomez, P.; De La Cruz, J.; Lobato, R.D. Severe head injury and the risk of early death. J. Neurol. Neurosurg. Psychiatry 2006, 77, 1054–1059. [Google Scholar] [CrossRef] [Green Version]
- Czeiter, E.; Mondello, S.; Kovacs, N.; Sandor, J.; Gabrielli, A.; Schmid, K.; Tortella, F.; Wang, K.K.; Hayes, R.L.; Barzo, P.; et al. Brain Injury Biomarkers May Improve the Predictive Power of the IMPACT Outcome Calculator. J. Neurotrauma 2012, 29, 1770–1778. [Google Scholar] [CrossRef] [Green Version]
- He, X.; Cui, H.; Simpson, D. Longitudinal data analysis using t-type regression. J. Stat. Plan. Inference 2004, 122, 253–269. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value | |
|---|---|---|
| Age (years) Mean (SD) | 52 ± 17 | |
| Range | 20–77 | |
| F/M, n (%) | 3/18 (15%/85%) | |
| Ethnicity, n (%) | White | 21 (100) |
| Race, n (%) | Caucasian | 21 (100) |
| Mechanism of injury, n (%) | Traffic accident | 7 (33) |
| Fall | 13 (62) | |
| Other | 1 (5) | |
| Time to sample withdrawal, h, median (range) a | 10.8 (4.0–23.5) | |
| Injury severity, n (%) | Moderate (GCS 9–12) | 10 (48) |
| Severe (GCS 3–8) | 11 (52) | |
| ISS, median (range) a | 16 (9–50) | |
| Marshall CT classification, n (%) | Diffuse injury I | - |
| Diffuse injury II | 8 (38) | |
| Diffuse injury III | - | |
| Diffuse injury IV | - | |
| Evacuated mass lesion | 12 (57) | |
| Non-evacuated mass lesion | 1 (5) | |
| CT pathology, n (%) | Diffuse axonal injury | 1 (5) |
| Extra-axial lesions only | 7 (33) | |
| Axial lesions only | 2 (10) | |
| Mixed lesions | 11 (52) | |
| Cerebral edema, n (%) b | Yes | 6 (29) |
| No | 15 (71) | |
| Decompressive craniectomy, n (%) | Yes | 8 (38) |
| No | 13 (62) | |
| Hospital disposition, n (%) | Early death (3 days) | 2 (10) |
| Discharged to a long-term acute care facility | 11 (52) | |
| Discharged to an acuterehabilitation facility | 4 (19) | |
| Discharge home | 4 (19) |
| n | Median (25–75th Percentile) Range | ||||
|---|---|---|---|---|---|
| t-tau, pg/mL | GFAP, pg/mL | NFL, pg/mL | UCH-L1, pg/mL | ||
| Day 1 | 21 | 0.85 (0.29–1.48) 0.08–5.74 | 10,944 (5029–16,550) 632.4–49,827 | 7.18 (2.64–12.01) 1.65–58.74 | 32.87 (16.44–41.79) 1.47–105.7 |
| Day 2 | 20 | 0.46 (0.18–0.75) 0.04–1.98 | 9112 (4180–13,306) 553.6–35,368 | 6.45 (3.98–13.2) 1.47–35.28 | 17.8 (6.69–31.28) 2.7–56.13 |
| Day 3 | 18 | 0.37 (0.14–0.63) 0.08–3.64 | 3698 (2212–13,041) 8.407–56,252 | 6.45 (4.25–13.3) 1.74–21.51 | 14.32 (4.37–28) 0.48–124.4 |
| Day 4 | 13 | 0.22 (0.11–0.59) 0.08–1.53 | 2938 (1698–10,378) 1401–26,500 | 11.29 (6.05–14.87) 4.71–27.38 | 8.40 (3.95–28.51) 0.13–37.7 |
| Day 5 | 12 | 0.28 (0.16–0.68) 0.076–0.82 | 2179 (1204–4894) 793.2–44,563 | 10.75 (7.05–20.12) 4.13–35.95 | 4.11 (1.87–22.94) 0.54–36.54 |
| Early Mortality (n = 2) | Survivors (n = 19) | |
|---|---|---|
| Extreme risers | 2 True Positive | 0 False Positive |
| Low decliners | 0 False Negative | 19 True Negative |
| Sensitivity = 100% (2/2); specificity = 100% (19/19) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mondello, S.; Guedes, V.A.; Lai, C.; Czeiter, E.; Amrein, K.; Kobeissy, F.; Mechref, Y.; Jeromin, A.; Mithani, S.; Martin, C.; et al. Circulating Brain Injury Exosomal Proteins following Moderate-to-Severe Traumatic Brain Injury: Temporal Profile, Outcome Prediction and Therapy Implications. Cells 2020, 9, 977. https://doi.org/10.3390/cells9040977
Mondello S, Guedes VA, Lai C, Czeiter E, Amrein K, Kobeissy F, Mechref Y, Jeromin A, Mithani S, Martin C, et al. Circulating Brain Injury Exosomal Proteins following Moderate-to-Severe Traumatic Brain Injury: Temporal Profile, Outcome Prediction and Therapy Implications. Cells. 2020; 9(4):977. https://doi.org/10.3390/cells9040977
Chicago/Turabian StyleMondello, Stefania, Vivian A. Guedes, Chen Lai, Endre Czeiter, Krisztina Amrein, Firas Kobeissy, Yehia Mechref, Andreas Jeromin, Sara Mithani, Carina Martin, and et al. 2020. "Circulating Brain Injury Exosomal Proteins following Moderate-to-Severe Traumatic Brain Injury: Temporal Profile, Outcome Prediction and Therapy Implications" Cells 9, no. 4: 977. https://doi.org/10.3390/cells9040977