
Chaperone-Mediated Autophagy Markers LAMP2A and HSPA8 in Advanced Non-Small Cell Lung Cancer after Neoadjuvant Therapy

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Next Generation Tissue Microarrays (TMA)
2.3. Immunohistochemical Staining and Scoring
2.4. Statistical Methods
3. Results
3.1. No Significant Intratumoral or Region-Specific Heterogeneity of LAMP2A and HSPA8
3.2. No Correlation between LAMP2A and HSPA8 Expression
3.3. Association of LAMP2A and HSPA8 Expression Levels with Pathological Parameters and Preoperative Chemotherapy
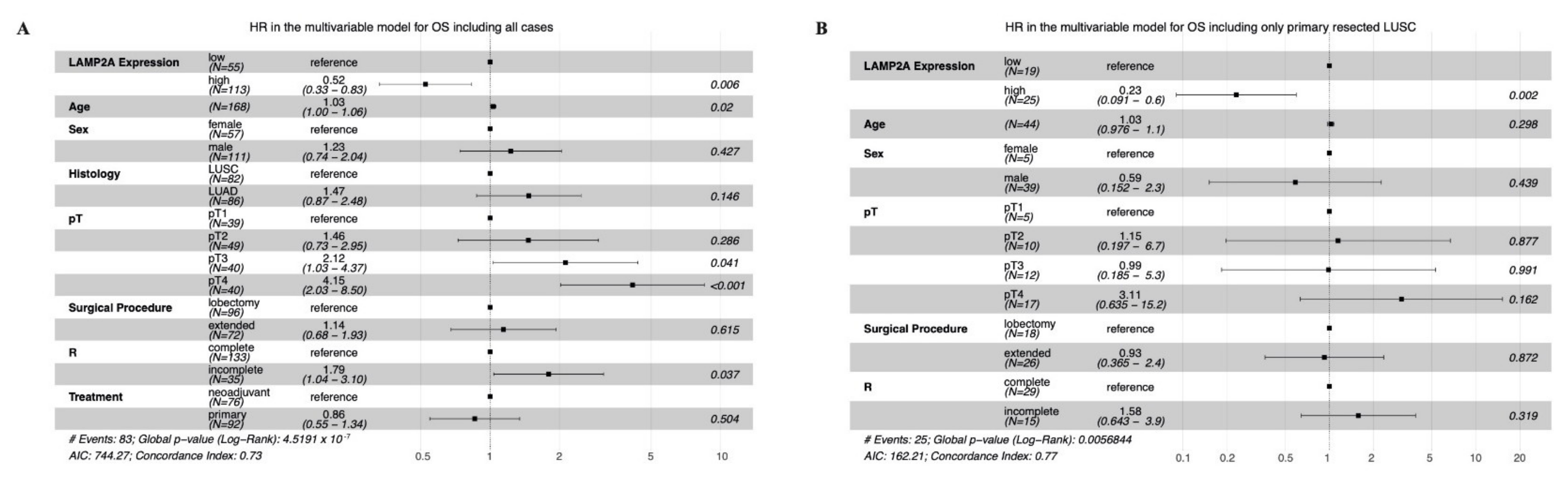
3.4. Correlation with Survival (OS and DFS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global Epidemiology of Lung Cancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, D.S.; Fakih, M.G.; Strickler, J.H.; Desai, J.; Durm, G.A.; Shapiro, G.I.; Falchook, G.S.; Price, T.J.; Sacher, A.; Denlinger, C.S.; et al. KRAS G12C Inhibition with Sotorasib in Advanced Solid Tumors. N. Engl. J. Med. 2020, 383, 1207–1217. [Google Scholar] [CrossRef] [PubMed]
- Mayekar, M.K.; Bivona, T.G. Current Landscape of Targeted Therapy in Lung Cancer. Clin. Pharmacol. Ther. 2017, 102, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Faehling, M.; Schwenk, B.; Kramberg, S.; Eckert, R.; Volckmar, A.-L.; Stenzinger, A.; Sträter, J. Oncogenic Driver Mutations, Treatment, and EGFR-TKI Resistance in a Caucasian Population with Non-Small Cell Lung Cancer: Survival in Clinical Practice. Oncotarget 2017, 8, 77897–77914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remon, J.; Soria, J.-C.; Peters, S.; ESMO Guidelines Committee. Early and Locally Advanced Non-Small-Cell Lung Cancer: An Update of the ESMO Clinical Practice Guidelines Focusing on Diagnosis, Staging, Systemic and Local Therapy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, S0923-7534(21)04279–4. [Google Scholar] [CrossRef]
- Filippi, A.R.; Di Muzio, J.; Badellino, S.; Mantovani, C.; Ricardi, U. Locally-Advanced Non-Small Cell Lung Cancer: Shall Immunotherapy Be a New Chance? J. Thorac. Dis. 2018, 10, S1461–S1467. [Google Scholar] [CrossRef]
- Lu, T.; Yang, X.; Huang, Y.; Zhao, M.; Li, M.; Ma, K.; Yin, J.; Zhan, C.; Wang, Q. Trends in the Incidence, Treatment, and Survival of Patients with Lung Cancer in the Last Four Decades. Cancer Manag. Res. 2019, 11, 943–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of Stage I and II Non-Small Cell Lung Cancer. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef]
- Souquet, P.J.; Geriniere, L. The Role of Chemotherapy in Early Stage of Non-Small Cell Lung Cancer. Lung Cancer 2001, 34, S155–S158. [Google Scholar] [CrossRef]
- Pignon, J.-P.; Tribodet, H.; Scagliotti, G.V.; Douillard, J.-Y.; Shepherd, F.A.; Stephens, R.J.; Dunant, A.; Torri, V.; Rosell, R.; Seymour, L.; et al. Lung Adjuvant Cisplatin Evaluation: A Pooled Analysis by the LACE Collaborative Group. J. Clin. Oncol. 2008, 26, 3552–3559. [Google Scholar] [CrossRef]
- Preoperative Chemotherapy for Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis of Individual Participant Data. Lancet 2014, 383, 1561–1571. [CrossRef] [Green Version]
- Song, W.-A.; Zhou, N.-K.; Wang, W.; Chu, X.-Y.; Liang, C.-Y.; Tian, X.-D.; Guo, J.-T.; Liu, X.; Liu, Y.; Dai, W.-M. Survival Benefit of Neoadjuvant Chemotherapy in Non-Small Cell Lung Cancer: An Updated Meta-Analysis of 13 Randomized Control Trials. J. Thorac. Oncol. 2010, 5, 510–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizushima, N.; Levine, B. Autophagy in Human Diseases. N. Engl. J. Med. 2020, 383, 1564–1576. [Google Scholar] [CrossRef]
- Kung, C.-P.; Budina, A.; Balaburski, G.; Bergenstock, M.K.; Murphy, M.E. Autophagy in Tumor Suppression and Cancer Therapy. Crit. Rev. Eukaryot. Gene Expr. 2011, 21, 71–100. [Google Scholar] [CrossRef]
- Karsli-Uzunbas, G.; Guo, J.Y.; Price, S.; Teng, X.; Laddha, S.V.; Khor, S.; Kalaany, N.Y.; Jacks, T.; Chan, C.S.; Rabinowitz, J.D.; et al. Autophagy Is Required for Glucose Homeostasis and Lung Tumor Maintenance. Cancer Discov. 2014, 4, 914–927. [Google Scholar] [CrossRef] [Green Version]
- Poillet-Perez, L.; White, E. Role of Tumor and Host Autophagy in Cancer Metabolism. Genes Dev. 2019, 33, 610–619. [Google Scholar] [CrossRef] [Green Version]
- Feng, Y.; He, D.; Yao, Z.; Klionsky, D.J. The Machinery of Macroautophagy. Cell Res. 2014, 24, 24–41. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Li, J.; Bao, J. Microautophagy: Lesser-Known Self-Eating. Cell. Mol. Life Sci. 2012, 69, 1125–1136. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, S.; Cuervo, A.M. The Coming of Age of Chaperone-Mediated Autophagy. Nat. Rev. Mol. Cell Biol. 2018, 19, 365–381. [Google Scholar] [CrossRef]
- Li, W.; Nie, T.; Xu, H.; Yang, J.; Yang, Q.; Mao, Z. Chaperone-Mediated Autophagy: Advances from Bench to Bedside. Neurobiol. Dis. 2019, 122, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Chen, S.; Ammar, A.-B.; Xu, J.; Wu, Q.; Pan, K.; Zhang, J.; Hong, Y. Crosstalk Between Macroautophagy and Chaperone-Mediated Autophagy: Implications for the Treatment of Neurological Diseases. Mol. Neurobiol. 2015, 52, 1284–1296. [Google Scholar] [CrossRef] [Green Version]
- Chava, S.; Lee, C.; Aydin, Y.; Chandra, P.K.; Dash, A.; Chedid, M.; Thung, S.N.; Moroz, K.; Wu, T.; Nayak, N.C.; et al. Chaperone-Mediated Autophagy Compensates for Impaired Macroautophagy in the Cirrhotic Liver to Promote Hepatocellular Carcinoma. Oncotarget 2017, 8, 40019–40036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichikawa, A.; Fujita, Y.; Hosaka, Y.; Kadota, T.; Ito, A.; Yagishita, S.; Watanabe, N.; Fujimoto, S.; Kawamoto, H.; Saito, N.; et al. Chaperone-mediated Autophagy Receptor Modulates Tumor Growth and Chemoresistance in Non–Small Cell Lung Cancer. Cancer Sci. 2020, 111, 4154–4165. [Google Scholar] [CrossRef] [PubMed]
- Hattori, A.; Takamochi, K.; Oh, S.; Suzuki, K. New Revisions and Current Issues in the Eighth Edition of the TNM Classification for Non-Small Cell Lung Cancer. Jpn. J. Clin. Oncol. 2019, 49, 3–11. [Google Scholar] [CrossRef] [Green Version]
- WHO Classification of Tumours Editorial Board. Thoracic Tumours; International Agency for Research on Cancer: Lyon, France, 2021; ISBN 978-92-832-4506-3. [Google Scholar]
- Zens, P.; Bello, C.; Scherz, A.; Koenigsdorf, J.; Pöllinger, A.; Schmid, R.A.; Ochsenbein, A.; Neppl, C.; Langer, R.; Berezowska, S. A Prognostic Score for Non-Small Cell Lung Cancer Resected after Neoadjuvant Therapy in Comparison with the Tumor-Node-Metastases Classification and Major Pathological Response. Mod. Pathol. 2021, 34, 1333–1344. [Google Scholar] [CrossRef]
- Travis, W.D.; Dacic, S.; Wistuba, I.; Sholl, L.; Adusumilli, P.; Bubendorf, L.; Bunn, P.; Cascone, T.; Chaft, J.; Chen, G.; et al. IASLC Multidisciplinary Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy. J. Thorac. Oncol. 2020, 15, 709–740. [Google Scholar] [CrossRef]
- Zlobec, I.; Suter, G.; Perren, A.; Lugli, A. A Next-Generation Tissue Microarray (NgTMA) Protocol for Biomarker Studies. JoVE J. Vis. Exp. 2014, 91, e51893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saper, C.B. A Guide to the Perplexed on the Specificity of Antibodies. J. Histochem. Cytochem. 2009, 57, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losmanová, T.; Janser, F.A.; Humbert, M.; Tokarchuk, I.; Schläfli, A.M.; Neppl, C.; Schmid, R.A.; Tschan, M.P.; Langer, R.; Berezowska, S. Chaperone-Mediated Autophagy Markers LAMP2A and HSC70 Are Independent Adverse Prognostic Markers in Primary Resected Squamous Cell Carcinomas of the Lung. Oxid. Med. Cell. Longev. 2020, 2020, 8506572. [Google Scholar] [CrossRef]
- Fedchenko, N.; Reifenrath, J. Different Approaches for Interpretation and Reporting of Immunohistochemistry Analysis Results in the Bone Tissue—A Review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef] [Green Version]
- Hothorn, T.; Lausen, B. On the Exact Distribution of Maximally Selected Rank Statistics. Comput. Stat. Data Anal. 2003, 43, 121–137. [Google Scholar] [CrossRef]
- Pataer, A.; Kalhor, N.; Correa, A.M.; Raso, M.G.; Erasmus, J.J.; Kim, E.S.; Behrens, C.; Lee, J.J.; Roth, J.A.; Stewart, D.J.; et al. Histopathologic Response Criteria Predict Survival of Patients with Resected Lung Cancer After Neoadjuvant Chemotherapy. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2012, 7, 825–832. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society International Multidisciplinary Classification of Lung Adenocarcinoma. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2011, 6, 244–285. [Google Scholar] [CrossRef] [Green Version]
- Kon, M.; Kiffin, R.; Koga, H.; Chapochnick, J.; Macian, F.; Varticovski, L.; Cuervo, A.M. Chaperone-Mediated Autophagy Is Required for Tumor Growth. Sci. Transl. Med. 2011, 3, 109ra117. [Google Scholar] [CrossRef] [Green Version]
- Gomes, L.R.; Menck, C.F.M.; Cuervo, A.M. Chaperone-Mediated Autophagy Prevents Cellular Transformation by Regulating MYC Proteasomal Degradation. Autophagy 2017, 13, 928–940. [Google Scholar] [CrossRef]
- Arias, E.; Cuervo, A.M. Pros and Cons of Chaperone-Mediated Autophagy in Cancer Biology. Trends Endocrinol. Metab. 2020, 31, 53–66. [Google Scholar] [CrossRef]
- Liu, G.; Pei, F.; Yang, F.; Li, L.; Amin, A.D.; Liu, S.; Buchan, J.R.; Cho, W.C. Role of Autophagy and Apoptosis in Non-Small-Cell Lung Cancer. Int. J. Mol. Sci. 2017, 18, 367. [Google Scholar] [CrossRef]
- Humbert, M.; Morán, M.; de la Cruz-Ojeda, P.; Muntané, J.; Wiedmer, T.; Apostolova, N.; McKenna, S.L.; Velasco, G.; Balduini, W.; Eckhart, L.; et al. Assessing Autophagy in Archived Tissue or How to Capture Autophagic Flux from a Tissue Snapshot. Biology 2020, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Daniels, C.K.; Cao, S. Comprehensive Review on the HSC70 Functions, Interactions with Related Molecules and Involvement in Clinical Diseases and Therapeutic Potential. Pharmacol. Ther. 2012, 136, 354–374. [Google Scholar] [CrossRef] [PubMed]
- Cuervo, A.M.; Dice, J.F. Lamp2s and Chaperone-Mediated Autophagy. J. Cell Sci. 2000, 113, 4441–4450. [Google Scholar] [CrossRef] [PubMed]
- Okayama, H.; Kohno, T.; Ishii, Y.; Shimada, Y.; Shiraishi, K.; Iwakawa, R.; Furuta, K.; Tsuta, K.; Shibata, T.; Yamamoto, S.; et al. Identification of Genes Upregulated in ALK-Positive and EGFR/KRAS/ALK-Negative Lung Adenocarcinomas. Cancer Res. 2012, 72, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichikawa, A.; Fujita, Y.; Hosaka, Y.; Kadota, T.; Ito, A.; Nakano, T.; Saito, N.; Yoshida, M.; Minagawa, S.; Numata, T.; et al. Chaperone-Mediated Autophagy-Dependent Chemoresistance in Non-Small Cell Lung Cancer. Eur. Respir. J. 2019, 54, OA1605. [Google Scholar] [CrossRef]
- Giatromanolaki, A.; Kalamida, D.; Sivridis, E.; Karagounis, I.V.; Gatter, K.C.; Harris, A.L.; Koukourakis, M.I. Increased Expression of Transcription Factor EB (TFEB) Is Associated with Autophagy, Migratory Phenotype and Poor Prognosis in Non-Small Cell Lung Cancer. Lung Cancer 2015, 90, 98–105. [Google Scholar] [CrossRef]
- Mauthe, M.; Orhon, I.; Rocchi, C.; Zhou, X.; Luhr, M.; Hijlkema, K.-J.; Coppes, R.P.; Engedal, N.; Mari, M.; Reggiori, F. Chloroquine Inhibits Autophagic Flux by Decreasing Autophagosome-Lysosome Fusion. Autophagy 2018, 14, 1435–1455. [Google Scholar] [CrossRef]
- Onorati, A.; Dyczynski, M.; Ojha, R.; Amaravadi, R.K. Targeting Autophagy in Cancer. Cancer 2018, 124, 3307–3318. [Google Scholar] [CrossRef] [Green Version]
- Malhotra, J.; Jabbour, S.; Orlick, M.; Riedlinger, G.; Joshi, S.; Guo, J.Y.; White, E.; Aisner, J. Modulation of Autophagy with Hydroxychloroquine in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): A Phase Ib Study. J. Clin. Oncol. 2018, 36, e21138. [Google Scholar] [CrossRef]
- Wang, F.; Tasset, I.; Cuervo, A.M.; Muller, S. In Vivo Remodeling of Altered Autophagy-Lysosomal Pathway by a Phosphopeptide in Lupus. Cells 2020, 9, 2328. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Cohort (n = 101) | Control Cohort (n = 114) | p-Value | ||||
|---|---|---|---|---|---|---|
| LAMP2A Low (n = 26) | LAMP2A High (n = 75) | LAMP2A Low (n = 42) | LAMP2A High (n = 72) | |||
| Age, years (median [IQR]) | 64 [56–69.8] | 63 [55–69.5] | 63 [57–70.8] | 64.5 [58.8–70] | 0.945 * | |
| Gender | n = 26 (%) | n = 75 (%) | n = 42 (%) | n = 72 (%) | 0.347 ° | |
| Female | 7 (26.9) | 22 (29.3) | 11 (26.2) | 27 (37.5) | ||
| Male | 19 (73.1) | 53 (70.7) | 31 (73.8) | 45 (62.5) | ||
| Smoking status | n = 22 (%) | n = 63 (%) | n = 33 (%) | n = 57 (%) | 0.133 ° | |
| Never/Ex-smoker | 15 (68.2) | 42 (66.7) | 15 (45.5) | 40 (70.2) | ||
| Active smoker | 7 (31.8) | 21 (33.3) | 18 (54.5) | 17 (29.8) | ||
| Histology | n = 26 (%) | n = 75 (%) | n = 42 (%) | n = 72 (%) | 0.137 ° | |
| LUSC | 11 (42.3) | 35 (46.7) | 24 (57.1) | 30 (41.7) | ||
| LUAD | 13 (50) | 39 (52) | 18 (42.9) | 42 (58.3) | ||
| LUASC | 2 (7.7) | 1 (1.3) | ||||
| Macroscopic tumor bed, cm (median [IQR]) | 4.2 [3.55–5.88] | 3.5 [2.5–5.25] | 5.45 [3.75–7.15] | 4.2 [2.85–6] | 0.059 * | |
| Resection | n = 26 (%) | n = 75 (%) | n = 42 (%) | n = 72 (%) | 0.327 ° | |
| Wedge | 1 (3.8) | 1 (1.3) | 2 (4.8) | 1 (1.4) | ||
| Lobectomy | 15 (57.7) | 38 (50.7) | 17 (40.5) | 45 (62.5) | ||
| Bilobectomy | 1 (3.8) | 5 (6.7) | 5 (11.9) | 3 (4.2) | ||
| Pneumonectomy | 9 (34.6) | 31 (41.3) | 18 (42.9) | 23 (31.9) | ||
| HSPA8, IRS (median [IQR]) | 8 [7.38–8.67] | 8 [7.46–9.33] | 8 [7.36–8.67] | 8 [7.29–9.14] | 0.413 * | |
| AJCC/UICC (yp)TNM stage 2017 | n = 26 (%) | n = 75 (%) | n = 42 (%) | n = 72 (%) | 0.805 + | |
| Stage I | 3 (11.5) | 13 (17.3) | ||||
| Stage II | 6 (23.1) | 19 (25.3) | ||||
| Stage III | 17 (65.4) | 36 (48) | 40 (95.2) | 64 (88.9) | ||
| Stage IV | 7 (9.3) | 2 (4.8) | 8 (11.1) | |||
| Regression, residual tumor | n = 26 (%) | n = 75 (%) | 0.115 + | |||
| MPR | <1% | 1 (3.8) | 7 (9.3) | |||
| 1–10% | 2 (7.7) | 10 (13.3) | ||||
| 10–50% | 4 (15.4) | 16 (21.3) | ||||
| ≥50% | 19 (73.1) | 42 (56) | ||||
| EGFR status | n = 5 (%) | n = 16 | n = 9 | n = 15 | 0.795 ° | |
| WT | 4 (80) | 13 (81.3) | 8 (88.9) | 11 (73.3) | ||
| Mutated | 1 (20) | 3 (18.7) | 1 (11.1) | 4 (26.7) | ||
| ALK status | n = 4 | n = 13 | n = 5 | n = 11 | ||
| WT | 4 (100) | 13 (100) | 5 (100) | 11 (100) | ||
| Mutated | ||||||
| ROS1 status | n = 2 | n = 13 | n = 2 | n = 9 | 0.695 ° | |
| WT | 2 (100) | 12 (92.3) | 2 (100) | 9 (100) | ||
| Mutated | 1 (7.7) | |||||
| KRAS status | n = 2 | n = 13 | n = 1 | n = 6 | 0.81 ° | |
| WT | 1 (50) | 10 (76.9) | 1 (100) | 4 (66.7) | ||
| Mutated | 1 (50) | 3 (23.1) | 2 (33.3) | |||
| TP53 status | n = 2 | n = 12 | n = 1 | n = 6 | 0.094 ° | |
| WT | 8 (66.7) | 5 (83.3) | ||||
| Mutated | 2 (100) | 4 (33.3) | 1 (100) | 1 (16.7) | ||
| HER2 status | n = 2 | n = 12 | n = 2 | n = 6 | 0.198 ° | |
| WT | 2 (100) | 11 (91.7) | 6 (100) | |||
| Mutated | 1 (8.3) | 2 (100) | ||||
| R status | n = 25 (%) | n = 74 (%) | n = 40 (%) | n = 71 (%) | 0.257 ° | |
| R0 | 19 (76) | 63 (85.1) | 28 (70) | 55 (77.5) | ||
| R1/R2 | 6 (24) | 11 (14.9) | 12 (30) | 16 (22.5) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Losmanova, T.; Zens, P.; Scherz, A.; Schmid, R.A.; Tschan, M.P.; Berezowska, S. Chaperone-Mediated Autophagy Markers LAMP2A and HSPA8 in Advanced Non-Small Cell Lung Cancer after Neoadjuvant Therapy. Cells 2021, 10, 2731. https://doi.org/10.3390/cells10102731
Losmanova T, Zens P, Scherz A, Schmid RA, Tschan MP, Berezowska S. Chaperone-Mediated Autophagy Markers LAMP2A and HSPA8 in Advanced Non-Small Cell Lung Cancer after Neoadjuvant Therapy. Cells. 2021; 10(10):2731. https://doi.org/10.3390/cells10102731
Chicago/Turabian StyleLosmanova, Tereza, Philipp Zens, Amina Scherz, Ralph A. Schmid, Mario P. Tschan, and Sabina Berezowska. 2021. "Chaperone-Mediated Autophagy Markers LAMP2A and HSPA8 in Advanced Non-Small Cell Lung Cancer after Neoadjuvant Therapy" Cells 10, no. 10: 2731. https://doi.org/10.3390/cells10102731