
Stress Keratin 17 Is a Predictive Biomarker Inversely Associated with Response to Immune Check-Point Blockade in Head and Neck Squamous Cell Carcinomas and Beyond
 , , , , , , , , and
, , , , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Selection
2.1.1. Discovery Set (UW Cohort)
2.1.2. Validation Set (Yale Cohort)
2.2. Immunohistochemistry
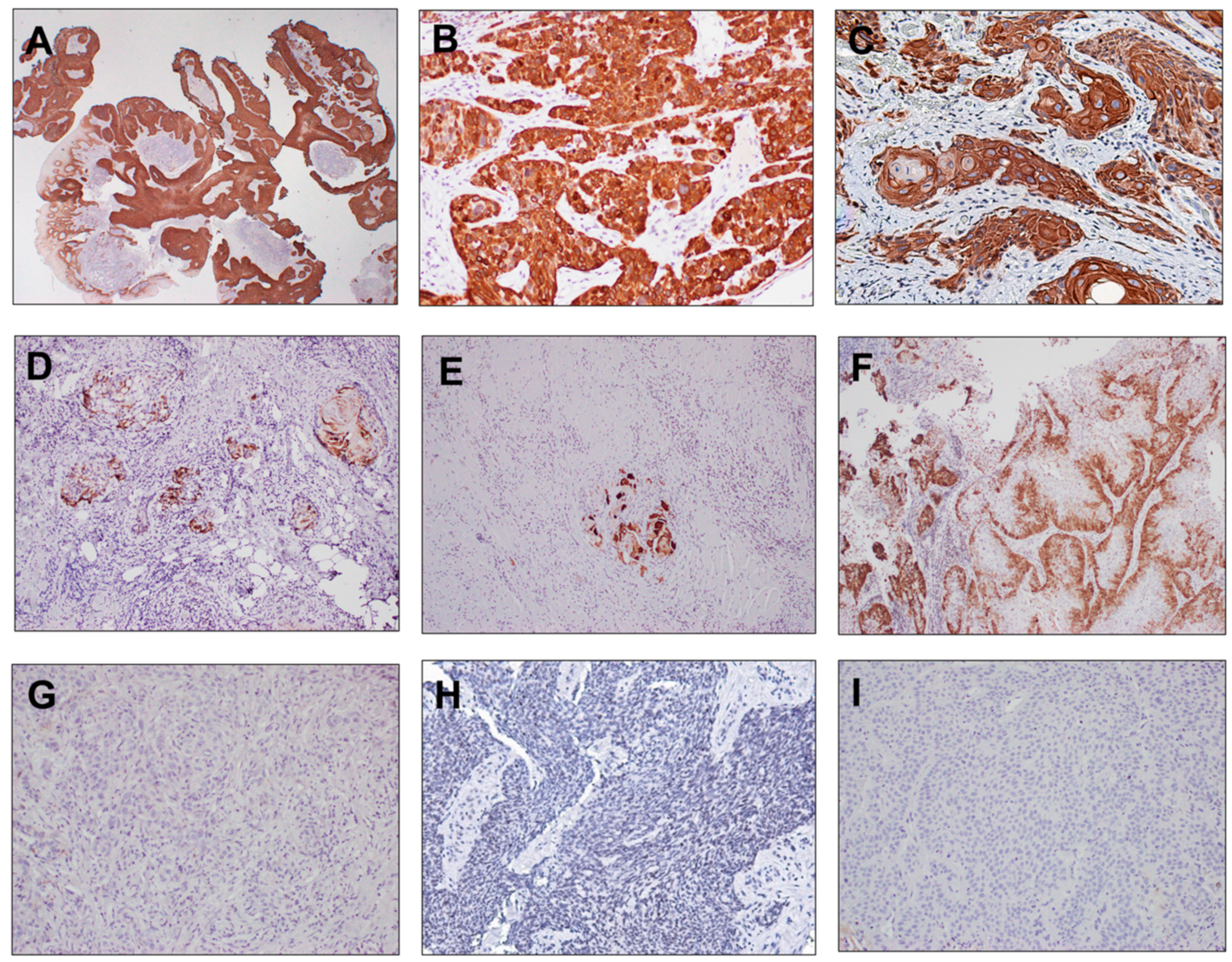
2.3. Sample Evaluation and Development of a CK17 IHC Scoring System
2.4. PD-L1 and p16 IHC Interpretation
2.5. Next-Generation Sequencing
2.6. Spatial Transcriptomics
2.7. Pan-Cancer Analysis
2.8. Study Endpoints
2.9. Statistical Analysis
3. Results
3.1. Discovery Set
3.2. CK17 Expression in Pembrolizumab-Treated HNSCC
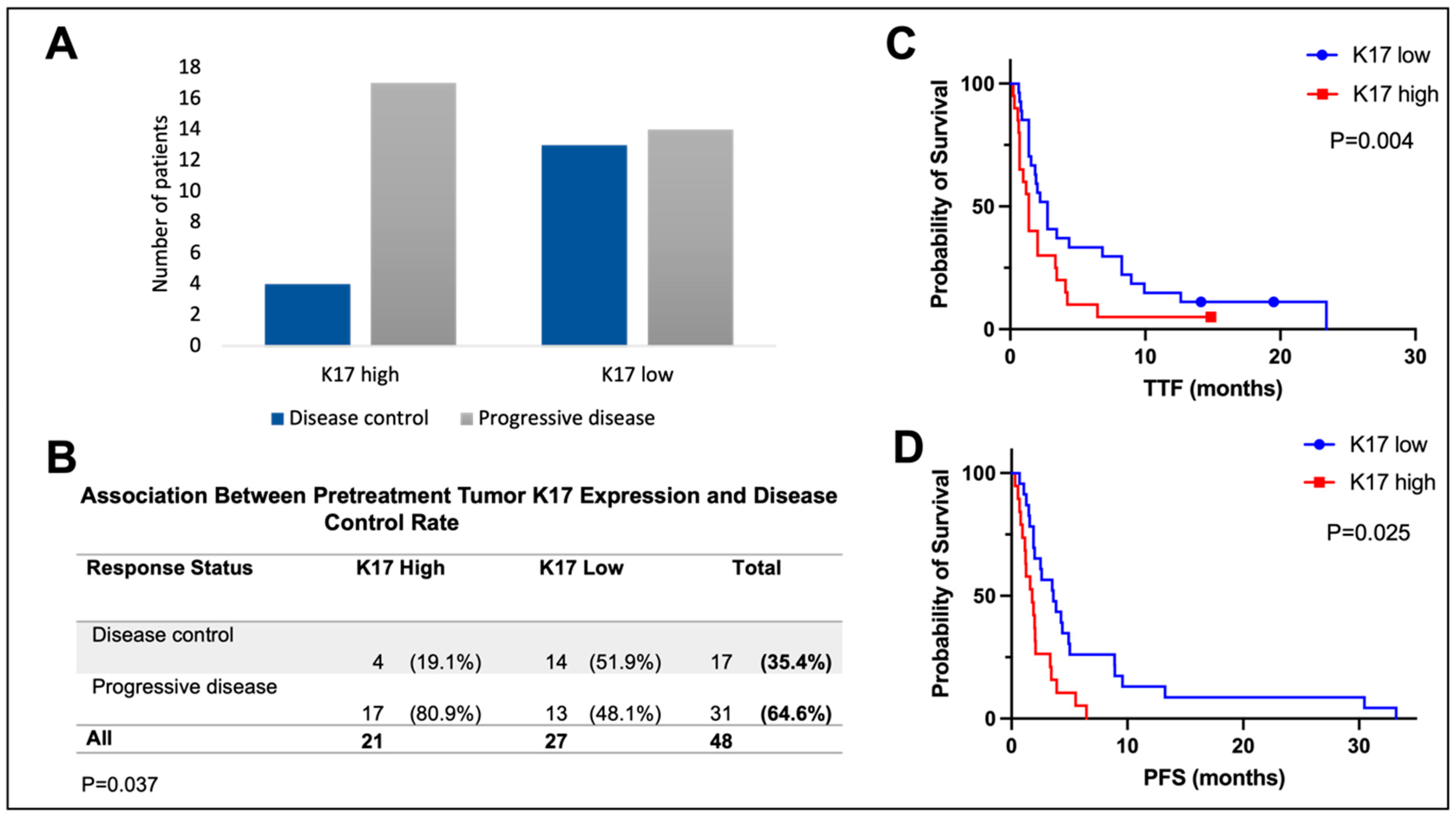
3.3. Stress Keratin 17 Expression Predicts Lack of Disease Control from Pembrolizumab
3.4. Stress Keratin 17 Predicts Lack of Disease Control from Pembrolizumab in an Independent Validation Set
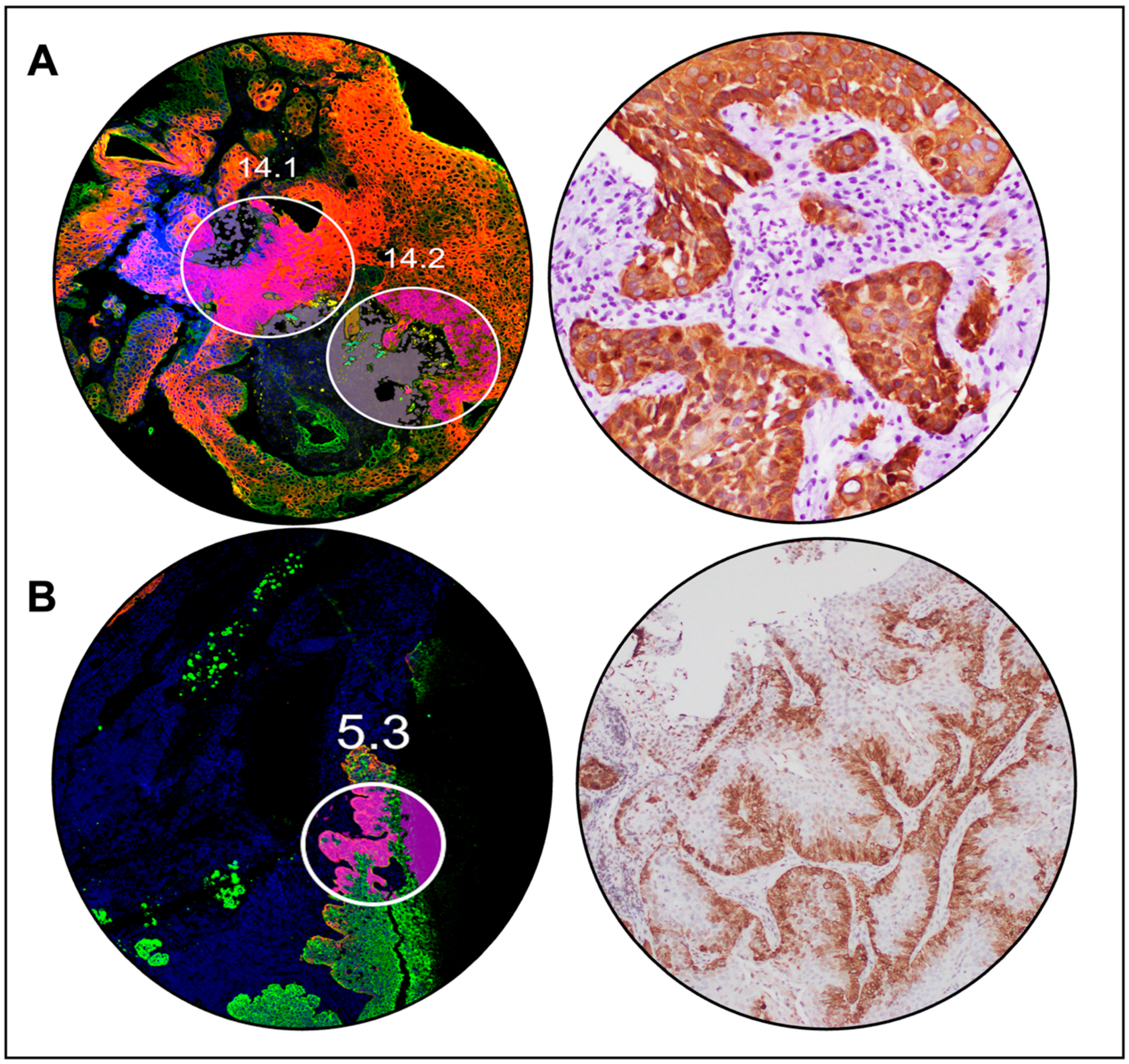
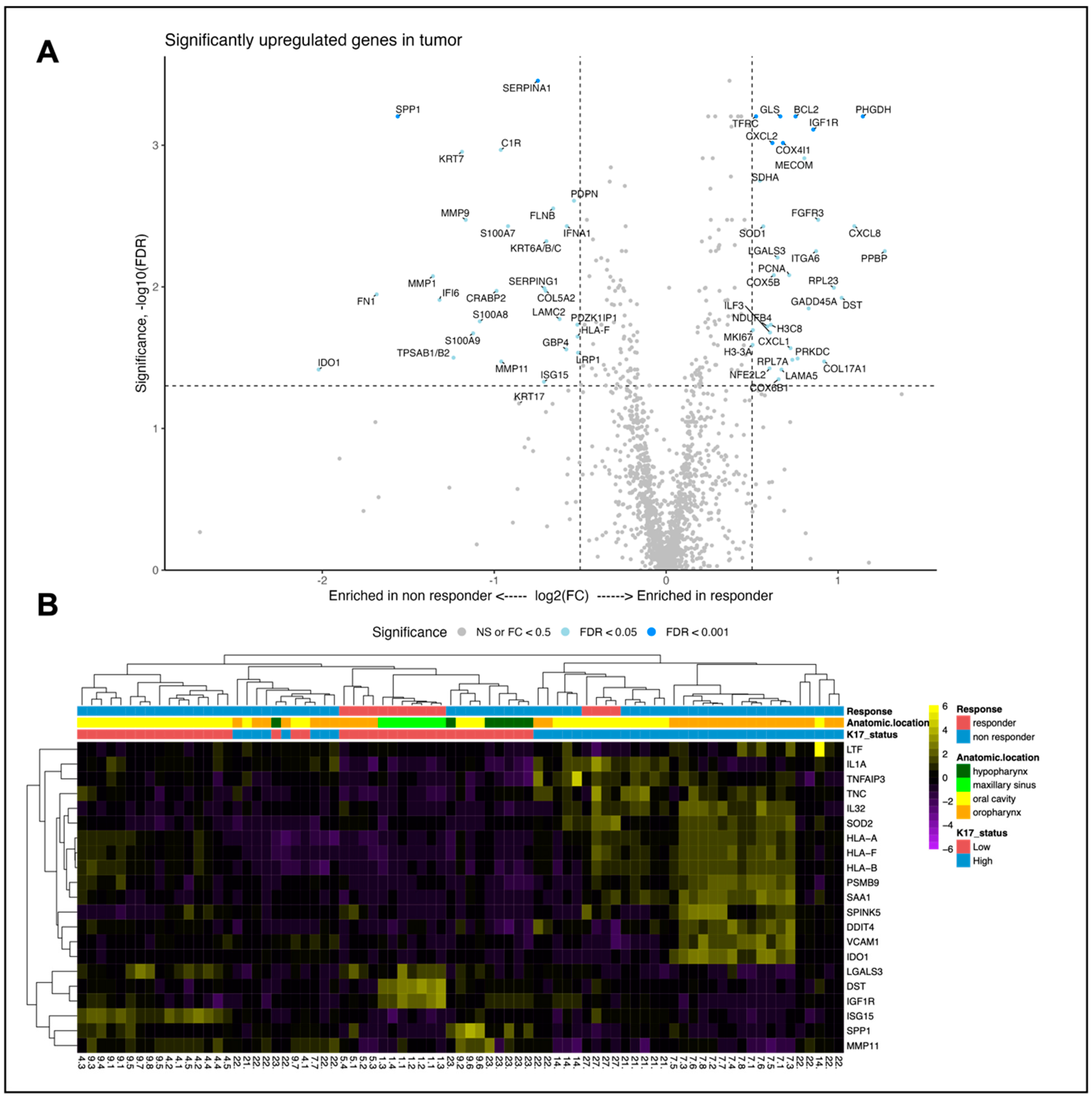
3.5. Spatial Transcriptomic Analysis Reveals Differentially Expressed Genes between Responders and Non-Responders
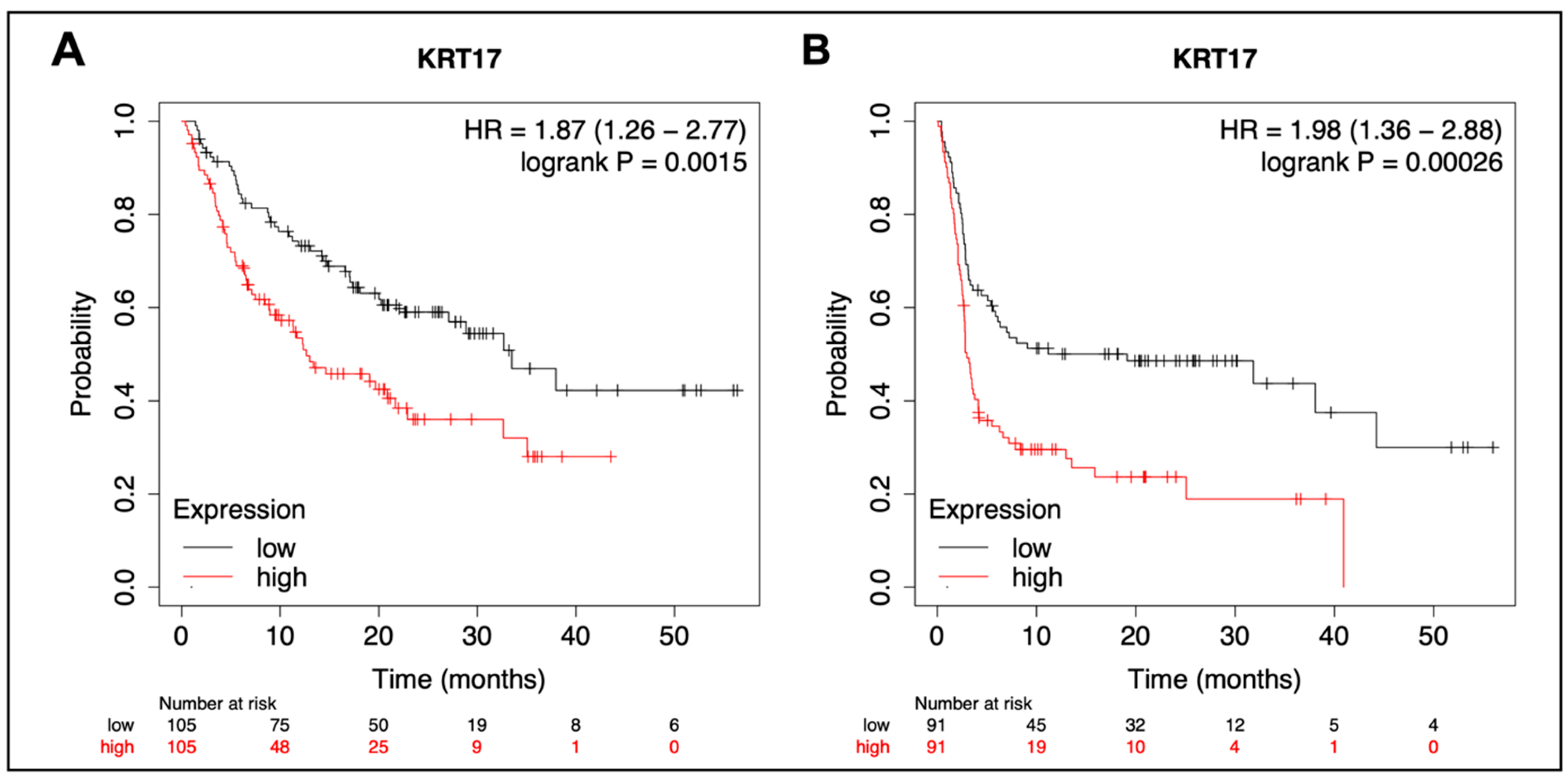
3.6. Pan-Cancer Analysis of KRT17 in Pembrolizumab-Treated Cancers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forster, M.D.; Devlin, M.J. Immune checkpoint inhibition in head and neck cancer. Front. Oncol. 2018, 8, 310. [Google Scholar] [CrossRef]
- Larkins, E.; Blumenthal, G.M.; Yuan, W.; He, K.; Sridhara, R.; Subramaniam, S.; Zhao, H.; Liu, C.; Yu, J.; Goldberg, K.B.; et al. FDA Approval Summary: Pembrolizumab for the Treatment of Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma with Disease Progression on or After Platinum-Containing Chemotherapy. Oncologist 2017, 22, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lozar, T.; Golfinos, A.E.; Lee, D.; Gronski, E.; Ward-Shaw, E.; Hayes, M.; Bruce, J.Y.; Kimple, R.J.; Hu, R.; et al. Stress Keratin 17 Expression in Head and Neck Cancer Contributes to Immune Evasion and Resistance to Immune-Checkpoint Blockade. Clin. Cancer Res. 2022, 28, 2953–2968. [Google Scholar] [CrossRef]
- Chu, P.G.; Weiss, L.M. Keratin expression in human tissues and neoplasms. Histopathology 2002, 40, 403–439. [Google Scholar] [CrossRef]
- Moll, R.; Franke, W.W.; Schiller, D.L.; Geiger, B.; Krepler, R. The catalog of human cytokeratins: Patterns of expression in normal epithelia, tumors and cultured cells. Cell 1982, 31, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, I.; Takahashi, K.; Moll, I.; Moll, R. Expression of keratins in cutaneous epithelial tumors and related disorders–distribution and clinical significance. Exp. Dermatol. 2011, 20, 217–228. [Google Scholar] [CrossRef]
- Proby, C.M.; Churchill, L.; Purkis, P.E.; Glover, M.T.; Sexton, C.J.; Leigh, I.M. Keratin 17 expression as a marker for epithelial transformation in viral warts. Am. J. Pathol. 1993, 143, 1667. [Google Scholar]
- Yang, L.; Zhang, S.; Wang, G. Keratin 17 in disease pathogenesis: From cancer to dermatoses. J. Pathol. 2019, 247, 158–165. [Google Scholar] [CrossRef]
- Rhodes, D.R.; Yu, J.; Shanker, K.; Deshpande, N.; Varambally, R.; Ghosh, D.; Barrette, T.; Pandey, A.; Chinnaiyan, A.M. ONCOMINE: A Cancer Microarray Database and Integrated Data-Mining Platform. Neoplasia 2004, 6, 1–6. [Google Scholar] [CrossRef]
- Li, C.; Teng, Y.; Wu, J.; Yan, F.; Deng, R.; Zhu, Y.; Li, X. A pan-cancer analysis of the oncogenic role of Keratin 17 (KRT17) in human tumors. Transl. Cancer Res. 2021, 10, 4489. [Google Scholar] [CrossRef]
- Escobar-Hoyos, L.F.; Yang, J.; Zhu, J.; Cavallo, J.A.; Zhai, H.; Burke, S.; Koller, A.; Chen, E.I.; Shroyer, K.R. Keratin 17 in premalignant and malignant squamous lesions of the cervix: Proteomic discovery and immunohistochemical validation as a diagnostic and prognostic biomarker. Mod. Pathol. 2014, 27, 621–630. [Google Scholar] [CrossRef]
- Regenbogen, E.; Mo, M.; Romeiser, J.; Shroyer, A.L.W.; Escobar-Hoyos, L.F.; Burke, S.; Shroyer, K.R. Elevated expression of keratin 17 in oropharyngeal squamous cell carcinoma is associated with decreased survival. Head Neck 2018, 40, 1788–1798. [Google Scholar] [CrossRef]
- Ide, M.; Kato, T.; Ogata, K.; Mochiki, E.; Kuwano, H.; Oyama, T. Keratin 17 expression correlates with tumor progression and poor prognosis in gastric adenocarcinoma. Ann. Surg. Oncol. 2012, 19, 3506–3514. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F.; Lang, H.Y.; Yuan, J.; Wang, J.; Wang, R.; Zhang, X.H.; Zhang, J.; Zhao, T.; Li, Y.R.; Liu, J.Y.; et al. Overexpression of keratin 17 is associated with poor prognosis in epithelial ovarian cancer. Tumor Biol. 2013, 34, 1685–1689. [Google Scholar] [CrossRef]
- Thike, A.A.; Cheok, P.Y.; Jara-Lazaro, A.R.; Tan, B.; Tan, P.; Tan, P.H. Triple-negative breast cancer: Clinicopathological characteristics and relationship with basal-like breast cancer. Mod. Pathol. 2010, 23, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Merkin, R.D.; Vanner, E.A.; Romeiser, J.L.; Shroyer, A.L.W.; Escobar-Hoyos, L.F.; Li, J.; Powers, R.S.; Burke, S.; Shroyer, K.R. Keratin 17 is overexpressed and predicts poor survival in estrogen receptor–negative/human epidermal growth factor receptor-2–negative breast cancer. Hum. Pathol. 2017, 62, 23–32. [Google Scholar] [CrossRef]
- Bai, J.D.K.; Babu, S.; Roa-Peña, L.; Hou, W.; Akalin, A.; Escobar-Hoyos, L.F.; Shroyer, K.R. Keratin 17 is a negative prognostic biomarker in high-grade endometrial carcinomas. Hum. Pathol. 2019, 94, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Roa-Peña, L.; Leiton, C.V.; Babu, S.; Pan, C.H.; Vanner, E.A.; Akalin, A.; Bandovic, J.; Moffitt, R.A.; Shroyer, K.R.; Escobar-Hoyos, L.F. Keratin 17 identifies the most lethal molecular subtype of pancreatic cancer. Sci. Rep. 2019, 9, 11239. [Google Scholar] [CrossRef]
- Baraks, G.; Tseng, R.; Pan, C.H.; Kasliwal, S.; Leiton, C.V.; Shroyer, K.R.; Escobar-Hoyos, L.F. Dissecting the Oncogenic Roles of Keratin 17 in the Hallmarks of Cancer. Cancer Res. 2022, 82, 1159–1166. [Google Scholar] [CrossRef]
- Bruni, D.; Angell, H.K.; Galon, J. The immune contexture and Immunoscore in cancer prognosis and therapeutic efficacy. Nat. Rev. Cancer 2020, 20, 662–680. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Uberoi, A.; Spurgeon, M.; Gronski, E.; Majerciak, V.; Lobanov, A.; Hayes, M.; Loke, A.; Zheng, Z.M.; Lambert, P.F. Stress keratin 17 enhances papillomavirus infection-induced disease by downregulating T cell recruitment. PLoS Pathog. 2020, 16, e1008206. [Google Scholar] [CrossRef]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting recommendations for tumor marker prognostic studies (REMARK): Explanation and elaboration. BMC Med. 2012, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- College of American Pathologists. CAP QCDR Measure Surgical Specimens CMS Measure ID/CMS QCDR ID: CAP 20 Measure Title: High Risk HPV Testing and p16 Scoring in Surgical Specimens for Patients with Oropharyngeal Squamous Cell Carcinoma (OPSCC) CAP QCDR Measure HR-HPV and p16 OPSCC; College of American Pathologists: Northfield, MN, USA, 2019; pp. 1–6. [Google Scholar]
- Mirghani, H.; Casiraghi, O.; Amen, F.; He, M.; Ma, X.J.; Saulnier, P.; Lacroix, L.; Drusch, F.; Lakdhar, A.B.; Saint Guily, J.L.; et al. Diagnosis of HPV-driven head and neck cancer with a single test in routine clinical practice. Mod. Pathol. 2015, 28, 1518–1527. [Google Scholar] [CrossRef] [PubMed]
- PD-L1 IHC 22C3 pharmDx Interpretation Manual—Head and Neck Squamous Cell Carcinoma (HNSCC). Available online: https://www.agilent.com/cs/library/usermanuals/public/29314_22c3_pharmDx_hnscc_interpretation_manual_us.pdf (accessed on 6 December 2022).
- Tomlins, S.A.; Hovelson, D.H.; Harms, P.; Drewery, S.; Falkner, J.; Fischer, A.; Hipp, J.; Kwiatkowski, K.; Lazo de la Vega, L.; Mitchell, K.; et al. Development and Validation of StrataNGS, a Multiplex PCR, Semiconductor Sequencing-Based Comprehensive Genomic Profiling Test. J. Mol. Diagn. 2021, 23, 1515–1533. [Google Scholar] [CrossRef]
- Frampton, G.M.; Fichtenholtz, A.; Otto, G.A.; Wang, K.; Downing, S.R.; He, J.; Schnall-Levin, M.; White, J.; Sanford, E.M.; An, P.; et al. Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing. Nat. Biotechnol. 2013, 31, 1023–1031. [Google Scholar] [CrossRef]
- Vogelzang, A.; McGuire, H.M.; Yu, D.; Sprent, J.; Mackay, C.R.; King, C. A Fundamental Role for Interleukin-21 in the Generation of T Follicular Helper Cells. Immunity 2008, 29, 127–137. [Google Scholar] [CrossRef]
- Andreatta, M.; Corria-Osorio, J.; Müller, S.; Cubas, R.; Coukos, G.; Carmona, S.J. Interpretation of T cell states from single-cell transcriptomics data using reference atlases. Nat. Commun. 2021, 12, 2965. [Google Scholar] [CrossRef]
- Cillo, A.R.; Kürten, C.H.; Tabib, T.; Qi, Z.; Onkar, S.; Wang, T.; Liu, A.; Duvvuri, U.; Kim, S.; Soose, R.J.; et al. Immune Landscape of Viral- and Carcinogen-Driven Head and Neck Cancer. Immunity 2020, 52, 183–199. [Google Scholar] [CrossRef]
- Newman, A.M.; Liu, C.L.; Green, M.R.; Gentles, A.J.; Feng, W.; Xu, Y.; Hoang, C.D.; Diehn, M.; Alizadeh, A.A. Robust enumeration of cell subsets from tissue expression profiles. Nat. Methods 2015, 12, 453–457. [Google Scholar] [CrossRef]
- Győrffy, B. Discovery and ranking of the most robust prognostic biomarkers in serous ovarian cancer. GeroScience 2023, 45, 1889. [Google Scholar] [CrossRef]
- Kovács, S.A.; Fekete, J.T.; Győrffy, B. Predictive biomarkers of immunotherapy response with pharmacological applications in solid tumors. Acta Pharmacol. Sin. 2023, 44, 1879–1889. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, Y.; Feng, Z.; Lu, L.; Li, Y.; Liu, Y.; Chen, Y. Analysis of the Expression and Role of Keratin 17 in Human Tumors. Front. Genet. 2022, 13, 801698. [Google Scholar] [CrossRef] [PubMed]
- Sanguansin, S.; Kosanwat, T.; Juengsomjit, R.; Poomsawat, S. Diagnostic Value of Cytokeratin 17 during Oral Carcinogenesis: An Immunohistochemical Study. Int. J. Dent. 2021, 2021, 4089549. [Google Scholar] [CrossRef]
- Gyanchandani, A.; Shukla, S.; Vagha, S.; Acharaya, S.; Kadu, R.P. Diagnostic Utility of Cytokeratin 17 Expression in Oral Squamous Cell Carcinoma: A Review. Cureus 2022, 14, 10–14. [Google Scholar] [CrossRef]
- Wu, C.L.; Huang, C.C.; Wu, S.Y.; Jiang, S.S.; Tsai, F.Y.; Hsiao, J.R. A new scoring system facilitating diagnosis of oral squamous malignancy on biopsy specimens. BMC Oral Health 2022, 22, 165. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, R.; Toyoshima, T.; Tanaka, H.; Kawano, S.; Matsubara, R.; Goto, Y.; Jinno, T.; Maruse, Y.; Oobu, K.; Nakamura, S. Cytokeratin 17 mRNA as a prognostic marker of oral squamous cell carcinoma. Oncol. Lett. 2017, 14, 6735–6743. [Google Scholar] [CrossRef]
- Wang, J.; Lan, L.; Ma, B.; Ren, G.; Yin, C. KRT17 Accelerates Cell Proliferative and Invasive Potential of Laryngeal Squamous Cell Carcinoma (LSCC) through Regulating AKT/mTOR and Wnt/β-Catenin Pathways. Evid. Based Complement. Altern. Med 2022, 2022, 6176043. [Google Scholar] [CrossRef]
- Liang, W.; Liu, H.; Zeng, Z.; Liang, Z.; Xie, H.; Li, W.; Xiong, L.; Liu, Z.; Chen, M.; Jie, H.; et al. KRT17 Promotes T-lymphocyte Infiltration Through the YTHDF2-CXCL10 Axis in Colorectal Cancer. Cancer Immunol. Res. 2023, 11, 875–894. [Google Scholar] [CrossRef]
- Li, H.; Torabi, S.J.; Yarbrough, W.G.; Mehra, S.; Osborn, H.A.; Judson, B. Association of human papillomavirus status at head and neck carcinoma subsites with overall survival. JAMA Otolaryngol.—Head Neck Surg. 2018, 144, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Cerbelli, B.; Girolami, I.; Eccher, A.; Costarelli, L.; Taccogna, S.; Scialpi, R.; Benevolo, M.; Lucante, T.; Luigi Alò, P.; Stella, F.; et al. Evaluating programmed death-ligand 1 (PD-L1) in head and neck squamous cell carcinoma: Concordance between the 22C3 PharmDx assay and the SP263 assay on whole sections from a multicentre study. Histopathology 2022, 80, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Munari, E.; Zamboni, G.; Marconi, M.; Sommaggio, M.; Brunelli, M.; Martignoni, G.; Netto, G.J.; Moretta, F.; Mingari, M.C.; Salgarello, M.; et al. PD-L1 expression heterogeneity in non-small cell lung cancer: Evaluation of small biopsies reliability. Oncotarget 2017, 8, 90123. [Google Scholar] [CrossRef]
- Shabani, F.; Farasat, A.; Mahdavi, M.; Gheibi, N. Calprotectin (S100A8/S100A9): A key protein between inflammation and cancer. Inflamm. Res. 2018, 67, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.M.; Lee, H.J.; Kim, D.C. High expression of S100A8 and S100A9 is associated with poor disease-free survival in patients with cancer: A systematic review and meta-analysis. Transl. Cancer Res. 2021, 10, 3225. [Google Scholar] [CrossRef]
- Wagner, N.B.; Weide, B.; Gries, M.; Reith, M.; Tarnanidis, K.; Schuermans, V.; Kemper, C.; Kehrel, C.; Funder, A.; Lichtenberger, R.; et al. Tumor microenvironment-derived S100A8/A9 is a novel prognostic biomarker for advanced melanoma patients and during immunotherapy with anti-PD-1 antibodies. J. Immunother. Cancer 2019, 7, 343. [Google Scholar] [CrossRef] [PubMed]
- Butti, R.; Kumar, T.V.; Nimma, R.; Banerjee, P.; Kundu, I.G.; Kundu, G.C. Osteopontin Signaling in Shaping Tumor Microenvironment Conducive to Malignant Progression. Adv. Exp. Med. Biol. 2021, 1329, 419–441. [Google Scholar] [CrossRef]
- Bie, T.; Zhang, X. Higher Expression of SPP1 Predicts Poorer Survival Outcomes in Head and Neck Cancer. J. Immunol. Res. 2021, 2021, 8569575. [Google Scholar] [CrossRef]
- Kazakova, E.; Rakina, M.; Sudarskikh, T.; Iamshchikov, P.; Tarasova, A.; Tashireva, L.; Afanasiev, S.; Dobrodeev, A.; Zhuikova, L.; Cherdyntseva, N.; et al. Angiogenesis regulators S100A4, SPARC and SPP1 correlate with macrophage infiltration and are prognostic biomarkers in colon and rectal cancers. Front. Oncol. 2023, 13, 188. [Google Scholar] [CrossRef]
- Bill, R.; Wirapati, P.; Messemaker, M.; Roh, W.; Zitti, B.; Duval, F.; Kiss, M.; Park, J.C.; Saal, T.M.; Hoelzl, J.; et al. CXCL9:SPP1 macrophage polarity identifies a network of cellular programs that control human cancers. Science 2023, 381, 515–524. [Google Scholar] [CrossRef]
- Khouja, M.H.; Baekelandt, M.; Sarab, A.; Nesland, J.M.; Holm, R. Limitations of tissue microarrays compared with whole tissue sections in survival analysis. Oncol. Lett. 2010, 1, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Torhorst, J.; Bucher, C.; Kononen, J.; Haas, P.; Zuber, M.; Köchli, O.R.; Mross, F.; Dieterich, H.; Moch, H.; Mihatsch, M.; et al. Tissue microarrays for rapid linking of molecular changes to clinical endpoints. Am. J. Pathol. 2001, 159, 2249–2256. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic, N (%) | All Patients N = 48 | Disease Control N = 17 | Progressive Disease N = 31 | p Value | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Age, median (years, IQR) | 64.0 | 11.8 | 66.0 | 7.5 | 61.0 | 14.0 | 0.295 |
| Sex | 0.885 | ||||||
| Female | 9 | 18.8 | 3 | 17.6 | 6 | 19.4 | |
| Male | 29 | 60.4 | 14 | 82.4 | 25 | 80.6 | |
| ECOG performance status ≥2 | 9 | 18.8 | 2 | 11.8 | 7 | 22.6 | 0.460 |
| Current or former smoker | 34 | 70.8 | 12 | 70.6 | 22 | 71.0 | 0.978 |
| Primary tumor location | 0.185 | ||||||
| Oral cavity | 16 | 33.3 | 3 | 17.6 | 13 | 41.9 | |
| Oropharynx | 21 | 43.8 | 9 | 52.9 | 12 | 38.7 | |
| Larynx | 2 | 4.2 | 1 | 5.9 | 1 | 3.2 | |
| Nasopharynx | 4 | 8.3 | 3 | 17.6 | 1 | 3.2 | |
| Other * | 5 | 10.4 | 1 | 5.9 | 4 | 12.9 | |
| Prior systemic therapy | 37 | 77.0 | 13 | 76.5 | 24 | 77.4 | 0.761 |
| HPV-positive tumor | 21 | 43.8 | 10 | 58.9 | 11 | 35.5 | 0.119 |
| PD-L1 expression (CPS) | 1.0 | ||||||
| <1 | 1 | 2.1 | 0 | 0 | 1 | 3.2 | |
| 1–19 | 24 | 50.0 | 9 | 52.9 | 15 | 48.4 | |
| ≥20 | 23 | 47.9 | 8 | 47.1 | 15 | 48.4 | |
| Front-line therapy | 0.089 | ||||||
| Surgery | 22 | 45.8 | 4 | 23.5 | 18 | 58.1 | |
| Chemoradiation | 18 | 37.5 | 10 | 58.8 | 8 | 25.8 | |
| Neoadjuvant Chemotherapy | 1 | 2.1 | 0 | 0 | 1 | 3.2 | |
| Palliative Chemotherapy | 3 | 6.3 | 2 | 11.8 | 1 | 3.2 | |
| Radiation only | 4 | 8.3 | 1 | 5.9 | 3 | 9.7 | |
| Single-agent pembrolizumab regimen | 39 | 81.3 | 14 | 82.4 | 25 | 80.6 | 1.0 |
| Concurrent radiation | 8 | 16.7 | 3 | 17.6 | 5 | 16.1 | 1.0 |
| Received ICB first line | 19 | 39.6 | 4 | 23.5 | 15 | 48.3 | 0.127 |
| Metastatic disease at initiation of ICB | 36 | 75.0 | 13 | 76.5 | 23 | 74.2 | 0.862 |
| Number of doses, mean (range) | 3.0 | (1–35) | 11.6 | (2–35) | 2.9 | (1–7) | <0.001 |
| Median TTF, months (95% CI) | 1.9 | 1.4–3.3 | 8.3 | 5.9–10.7 | 1.4 | 1.1–1.7 | <0.001 |
| Median PFS, months (95% CI) | 2.0 | 1.3–3.4 | 6.5 | 0.1–13.0 | 1.9 | 1.5–2.3 | <0.001 |
| Median OS, months (95% CI) | 6.1 | 2.1–10.1 | 8.3 | 5.9–10.8 | 4.6 | 1.1–8.2 | 0.168 |
| Discontinuation due to AEs | 4 | 8.3 | 3 | 17.6 | 1 | 3.2 | 0.084 |
| Characteristic | All Cases N = 48 | CK17 Protein Expression | |||||
|---|---|---|---|---|---|---|---|
| CK17 High N = 21 | CK17 Low N = 27 | p Value | |||||
| N | % | N | % | N | % | ||
| Tumor stage at diagnosis | 0.683 | ||||||
| T0 | 1 | 2.1 | 0 | 0 | 1 | 3.7 | |
| T1 | 6 | 12.5 | 2 | 9.5 | 4 | 14.8 | |
| T2 | 9 | 18.8 | 5 | 23.8 | 4 | 14.8 | |
| T3 | 5 | 10.4 | 1 | 4.8 | 4 | 14.8 | |
| T4 | 27 | 56.3 | 13 | 61.9 | 14 | 51.9 | |
| Lymph node stage at diagnosis | 0.149 | ||||||
| 0 | 7 | 14.6 | 3 | 14.3 | 4 | 14.8 | |
| 1 | 2 | 4.2 | 1 | 4.8 | 1 | 3.7 | |
| 2 | 25 | 52.1 | 14 | 66.7 | 11 | 40.7 | |
| 3 | 14 | 29.2 | 3 | 14.3 | 11 | 40.7 | |
| Primary tumor location | 0.274 | ||||||
| oral cavity | 16 | 33.3 | 8 | 38.1 | 8 | 29.6 | |
| oropharynx | 21 | 43.8 | 10 | 47.6 | 11 | 40.7 | |
| larynx | 2 | 4.2 | 1 | 4.8 | 1 | 3.7 | |
| nasopharynx | 4 | 8.3 | 1 | 4.8 | 3 | 11.1 | |
| other * | 5 | 10.4 | 0 | 0 | 5 | 18.5 | |
| Histologic subtype ** | 0.003 | ||||||
| keratinizing | 27 | 56.3 | 17 | 80.9 | 10 | 37.0 | |
| non-keratinizing | 21 | 43.8 | 4 | 19.1 | 17 | 62.9 | |
| Sample type | 0.769 | ||||||
| biopsy | 31 | 64.6 | 13 | 61.9 | 18 | 66.7 | |
| resection | 17 | 35.4 | 8 | 38.1 | 9 | 33.3 | |
| Tissue type | 0.462 | ||||||
| primary tumor | 19 | 39.6 | 7 | 33.3 | 12 | 44.4 | |
| local recurrence | 16 | 33.3 | 10 | 47.6 | 6 | 22.2 | |
| locoregional lymph node metastasis | 5 | 10.4 | 2 | 9.5 | 3 | 11.1 | |
| distant metastasis | 8 | 16.7 | 6 | 28.6 | 2 | 7.4 | |
| Received radiation before obtaining study tissue | 24 | 50.0 | 10 | 47.6 | 14 | 51.9 | 1.0 |
| HPV-positive tumor | 21 | 43.8 | 10 | 47.6 | 11 | 40.7 | 0.771 |
| PD-L1 expression (CPS) | NC | ||||||
| <1 | 1 | 2.1 | 1 | 4.8 | 0 | 0 | |
| 1–19 | 24 | 50.0 | 9 | 42.9 | 15 | 55.6 | |
| ≥20 | 23 | 47.9 | 11 | 52.4 | 12 | 44.4 | |
| Received chemotherapy before obtaining study tissue | 22 | 45.8 | 10 | 47.6 | 12 | 44.4 | 0.624 |
| Received radiation before obtaining study tissue | 24 | 50.0 | 10 | 47.6 | 14 | 51.9 | 1.0 |
| Concurrent chemotherapy while on ICB | 8 | 16.7 | 6 | 28.6 | 2 | 7.4 | 0.115 |
| Concurrent radiation while on ICB | 8 | 16.7 | 6 | 28.6 | 2 | 7.4 | 0.115 |
| Characteristic | All Patients N = 22 | Disease Control N = 14 | Progressive Disease N = 8 | p Value | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Age, median (years, IQR) | 63.1 | 13.6 | 63.1 | 16.4 | 61.2 | 14.9 | 1.0 |
| Sex | 1.0 | ||||||
| Female | 1 | 4.5 | 1 | 7.1 | 0 | / | |
| Male | 21 | 95.4 | 13 | 92.9 | 8 | 100.0 | |
| Current or former smoker | 17 | 77.3 | 11 | 78.6 | 6 | 75.0 | 1.0 |
| Primary tumor location | NC | ||||||
| Oral cavity | 2 | 9.1 | 1 | 7.1 | 1 | 12.5 | |
| Oropharynx | 12 | 54.5 | 7 | 50.0 | 5 | 62.5 | |
| Larynx | 3 | 13.6 | 2 | 14.3 | 1 | 12.5 | |
| Other * | 5 | 22.7 | 4 | 28.6 | 1 | 12.5 | |
| HPV Status | NC | ||||||
| Positive | 11 | 50.0 | 6 | 42.9 | 5 | 62.5 | |
| Negative | 9 | 40.1 | 6 | 42.9 | 3 | 37.5 | |
| Missing | 2 | 9.1 | 2 | 14.2 | 0 | 0 | |
| PD-L1 expression (CPS) | 0.086 | ||||||
| <1 | 5 | 22.7 | 4 | 28.6 | 1 | 12.5 | |
| 1–19 | 9 | 40.9 | 3 | 21.4 | 6 | 75.0 | |
| ≥20 | 8 | 36.4 | 7 | 50.0 | 1 | 12.5 | |
| Single-agent pembrolizumab regimen | 9 | 40.1 | 4 | 28.6 | 5 | 62.5 | 0.187 |
| Concurrent radiation | 7 | 31.8 | 5 | 35.7 | 2 | 25.0 | 0.671 |
| Received ICB first line | 14 | 63.6 | 8 | 57.1 | 6 | 75.0 | 0.649 |
| Metastatic disease at initiation of ICB | 18 | 81.8 | 11 | 78.6 | 7 | 87.5 | 1.0 |
| Median PFS, months (95% CI) | 7.3 | 1.8–12.8 | 15.1 | 3.2–27.0 | 1.3 | 0.5–2.1 | <0.001 |
| Median OS, months (95% CI) | 18.8 | 4.5–33.1 | 31.1 | 4.6–57.6 | 4.0 | 0.1–8.6 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lozar, T.; Laklouk, I.; Golfinos, A.E.; Gavrielatou, N.; Xu, J.; Flynn, C.; Keske, A.; Yu, M.; Bruce, J.Y.; Wang, W.; et al. Stress Keratin 17 Is a Predictive Biomarker Inversely Associated with Response to Immune Check-Point Blockade in Head and Neck Squamous Cell Carcinomas and Beyond. Cancers 2023, 15, 4905. https://doi.org/10.3390/cancers15194905
Lozar T, Laklouk I, Golfinos AE, Gavrielatou N, Xu J, Flynn C, Keske A, Yu M, Bruce JY, Wang W, et al. Stress Keratin 17 Is a Predictive Biomarker Inversely Associated with Response to Immune Check-Point Blockade in Head and Neck Squamous Cell Carcinomas and Beyond. Cancers. 2023; 15(19):4905. https://doi.org/10.3390/cancers15194905
Chicago/Turabian StyleLozar, Taja, Israa Laklouk, Athena E. Golfinos, Niki Gavrielatou, Jin Xu, Christopher Flynn, Aysenur Keske, Menggang Yu, Justine Y. Bruce, Wei Wang, and et al. 2023. "Stress Keratin 17 Is a Predictive Biomarker Inversely Associated with Response to Immune Check-Point Blockade in Head and Neck Squamous Cell Carcinomas and Beyond" Cancers 15, no. 19: 4905. https://doi.org/10.3390/cancers15194905