

Radiomics-Based Inter-Lesion Relation Network to Describe [18F]FMCH PET/CT Imaging Phenotypes in Prostate Cancer
 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Image Analysis
2.3. Data Analysis and Statistics
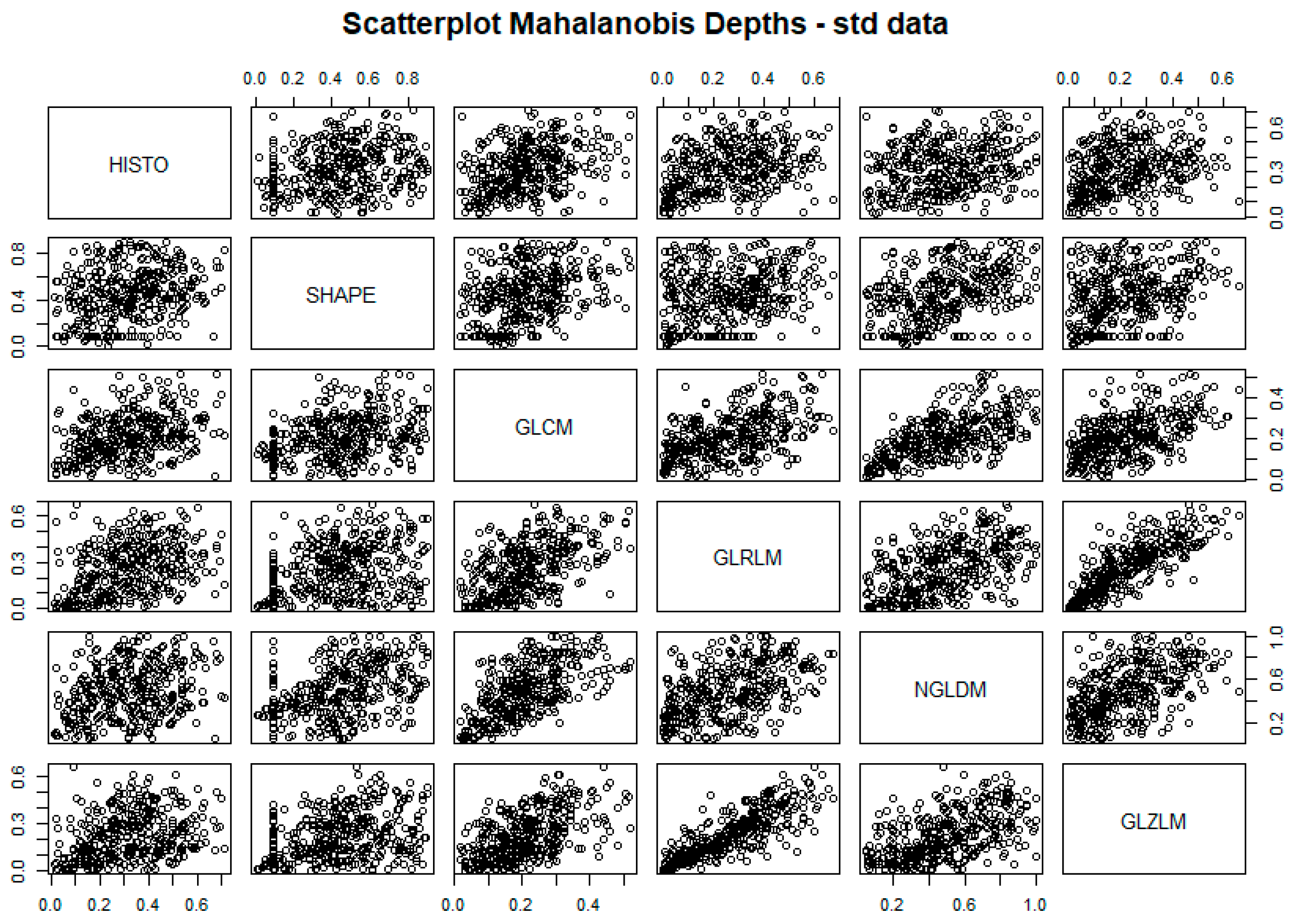
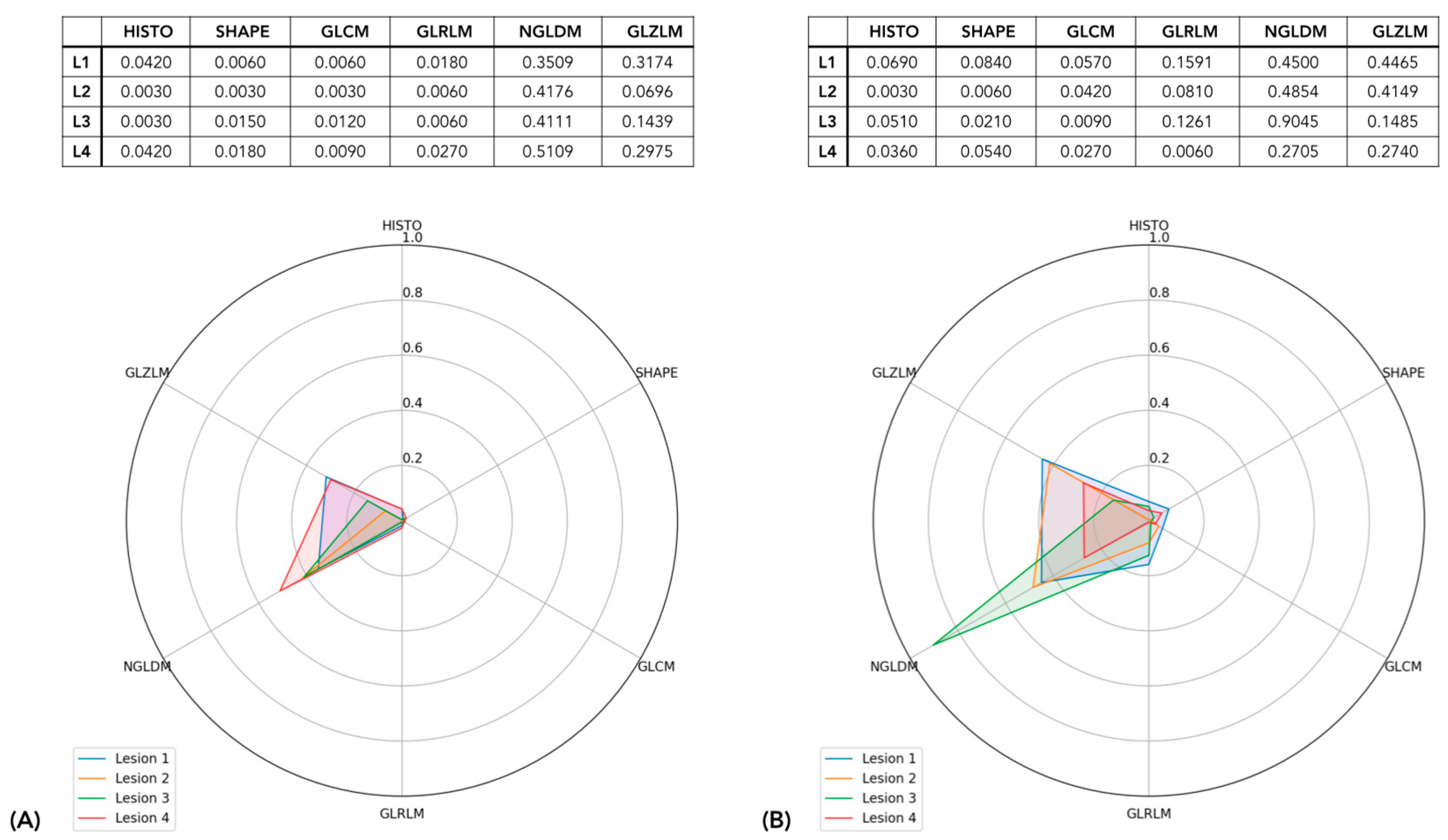
2.3.1. Lesion Textural Profile
2.3.2. Qualitative Assessment of Intra-Tumor Heterogeneity
- patients exhibiting lesions with homogeneous radiomic phenotypes—i.e., their lesions fell into the same group of lesions—were labelled as patients with homogenous disease;
- patients featuring lesions with heterogeneous radiomic phenotypes—i.e., their lesions fell into more than one group of lesions—were labelled as patients with heterogeneous disease.
2.3.3. Quantitative Assessment of Intra-Tumor Heterogeneity
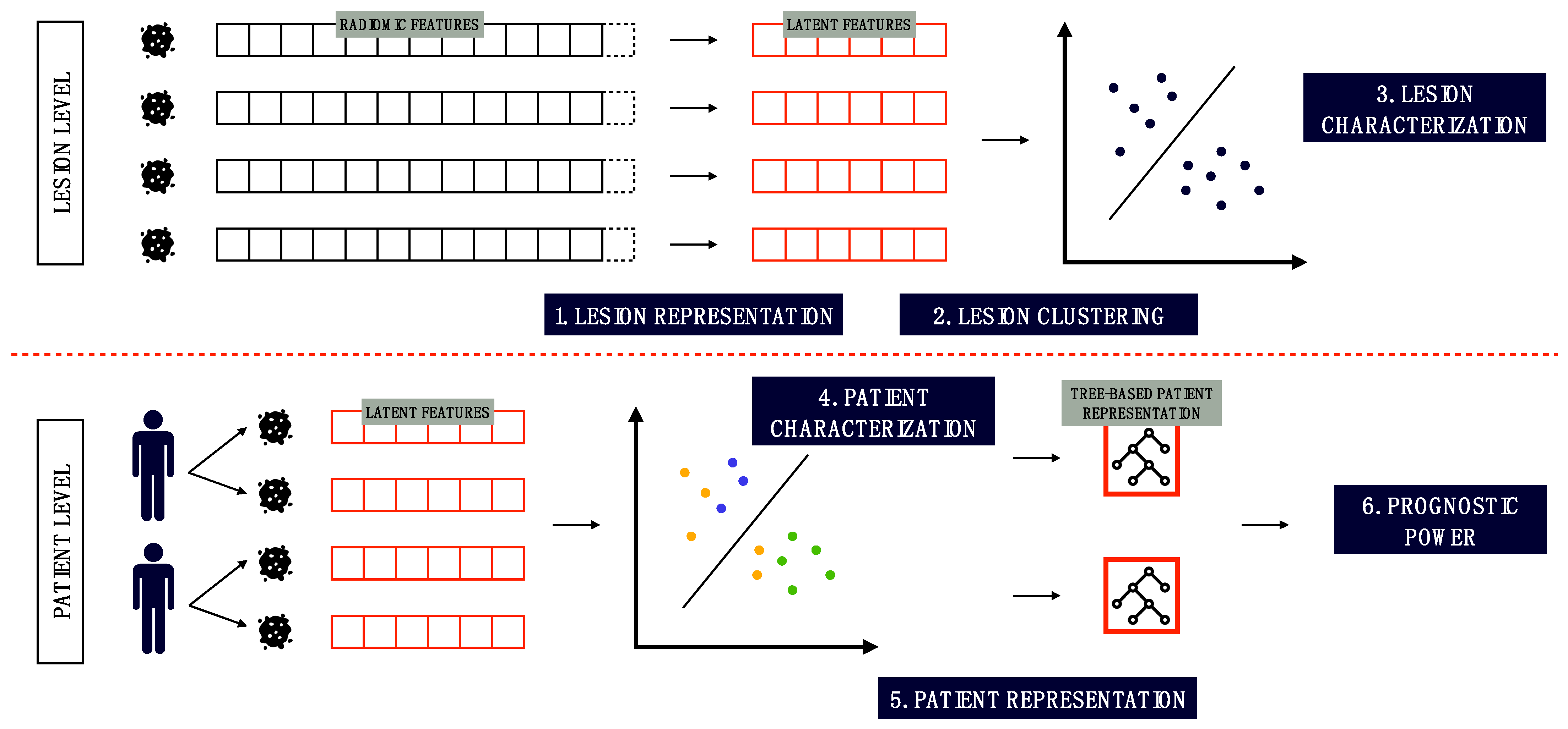
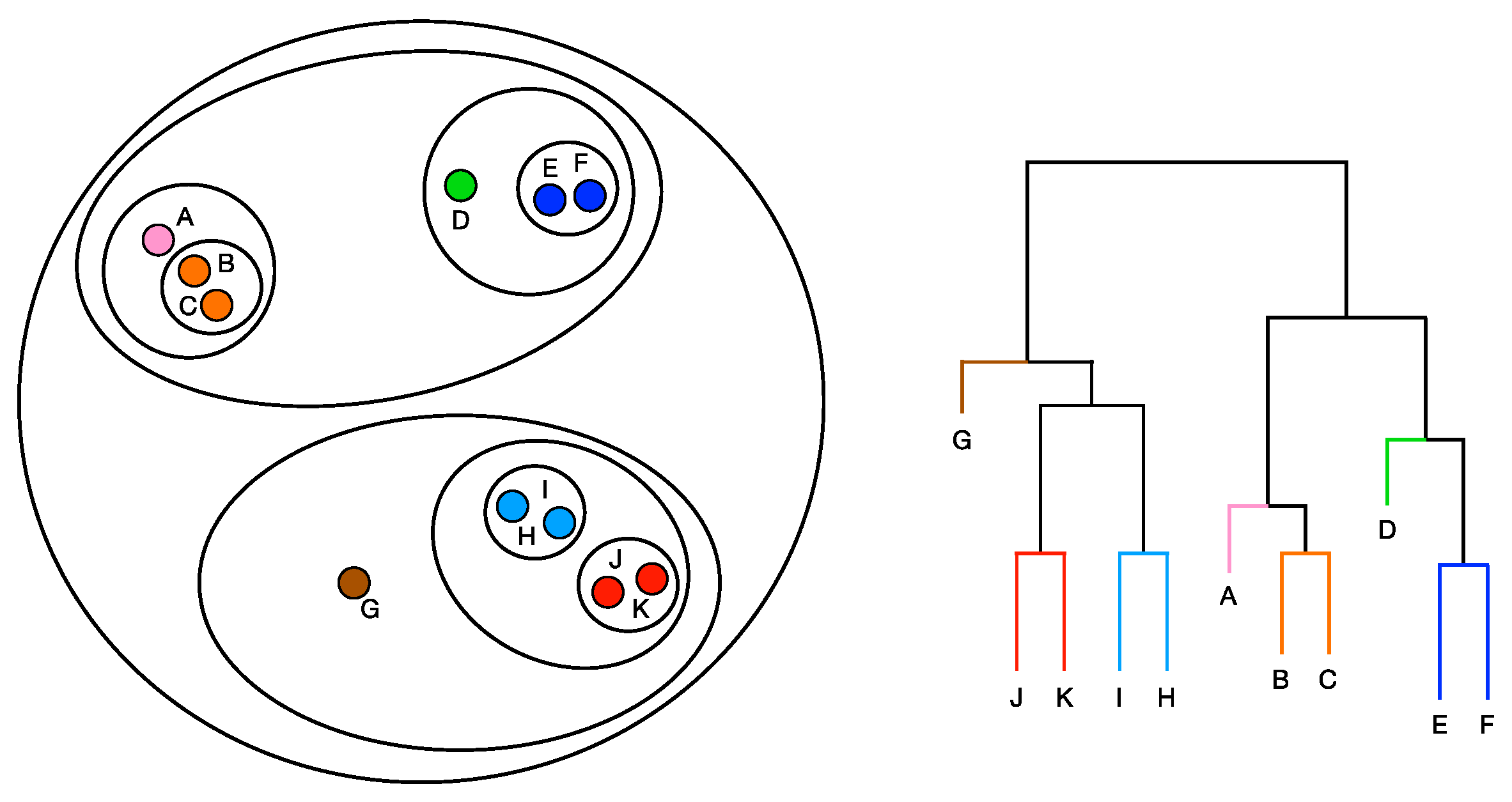
2.3.4. Perspective Modeling
3. Results
3.1. Lesion Textural Profile
3.2. Qualitative Assessment of Intra-Tumor Heterogeneity
3.3. Quantitative Assessment of Intra-Tumor Heterogeneity
3.4. Perspective Modelling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sollini, M.; Bandera, F.; Kirienko, M. Quantitative imaging biomarkers in nuclear medicine: From SUV to image mining studies. Highlights from annals of nuclear medicine 2018. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2737–2745. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Bartoli, F.; Marciano, A.; Zanca, R.; Slart, R.H.J.A.; Erba, P.A. Artificial intelligence and hybrid imaging: The best match for personalized medicine in oncology. Eur. J. Hybrid Imaging 2020, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Antunovic, L.; Chiti, A.; Kirienko, M. Towards clinical application of image mining: A systematic review on artificial intelligence and radiomics. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2656–2672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—“how-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef]
- Hatt, M.; Krizsan, A.K.; Rahmim, A.; Bradshaw, T.J.; Costa, P.F.; Forgacs, A.; Seifert, R.; Zwanenburg, A.; El Naqa, I.; Kinahan, P.E.; et al. Joint EANM/SNMMI guideline on radiomics in nuclear medicine: Jointly supported by the EANM Physics Committee and the SNMMI Physics, Instrumentation and Data Sciences Council. Eur. J. Nucl. Med. Mol. Imaging 2022, 50, 352–375. [Google Scholar] [CrossRef]
- Sollini, M.; Cozzi, L.; Ninatti, G.; Antunovic, L.; Cavinato, L.; Chiti, A.; Kirienko, M. PET/CT radiomics in breast cancer: Mind the step. Methods 2021, 188, 122–132. [Google Scholar] [CrossRef]
- Porenta, G. Is There Value for Artificial Intelligence Applications in Molecular Imaging and Nuclear Medicine? J. Nucl. Med. 2019, 60, 1347–1349. [Google Scholar] [CrossRef]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A Postreconstruction Harmonization Method for Multicenter Radiomic Studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef] [Green Version]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Sollini, M.; Gelardi, F.; Matassa, G.; Delgado Bolton, R.C.; Chiti, A.; Kirienko, M. Interdisciplinarity: An essential requirement for translation of radiomics research into clinical practice–a systematic review focused on thoracic oncology. Rev. Española Med. Nucl. Imagen Mol. Engl. Ed. 2020, 39, 146–156. [Google Scholar] [CrossRef]
- Gelardi, F.; Kirienko, M.; Sollini, M. Climbing the steps of the evidence-based medicine pyramid: Highlights from Annals of Nuclear Medicine 2019. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Kirienko, M.; Cavinato, L.; Ricci, F.; Biroli, M.; Ieva, F.; Calderoni, L.; Tabacchi, E.; Nanni, C.; Zinzani, P.L.; et al. Methodological framework for radiomics applications in Hodgkin’s lymphoma. Eur. J. Hybrid Imaging 2020, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Bartoli, F.; Cavinato, L.; Ieva, F.; Ragni, A.; Marciano, A.; Zanca, R.; Galli, L.; Paiar, F.; Pasqualetti, F.; et al. [18F]FMCH PET/CT biomarkers and similarity analysis to refine the definition of oligometastatic prostate cancer. EJNMMI Res. 2021, 11, 119. [Google Scholar] [CrossRef] [PubMed]
- Artibani, W.; Porcaro, A.B.; De Marco, V.; Cerruto, M.A.; Siracusano, S. Management of Biochemical Recurrence after Primary Curative Treatment for Prostate Cancer: A Review. Urol. Int. 2018, 100, 251–262. [Google Scholar] [CrossRef]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuze, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. Lifex: A freeware for radiomic feature calculation in multimodality imaging to accelerate advances in the characterization of tumor heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Lee, S.M.S. Depth functions as measures of representativeness. Stat. Pap. 2014, 55, 1079–1105. [Google Scholar] [CrossRef] [Green Version]
- Pokotylo, O.; Mozharovskyi, P.; Dyckerhoff, R. Depth and depth-based classification with R package ddalpha. J. Stat. Softw. 2019, 91, 1–46. [Google Scholar] [CrossRef] [Green Version]
- Velasco-Forero, S.; Angulo, J. Mathematical Morphology for Vector Images Using Statistical Depth. In Mathematical Morphology and Its Applications to Image and Signal Processing; Lecture Notes in Computer Science (including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2011; Volume 6671, pp. 355–366. [Google Scholar]
- Ekstrøm, C.T.; Alexander, T.; Maintainer, G. Package “SuperRanker” Title Sequential Rank Agreement; Version 1.2.0; CRAN: Vienna, Austria, 2021. [Google Scholar]
- Newling, J.; Fleuret, F. Nested Mini-Batch K-Means. arXiv 2016, arXiv:1602.02934. [Google Scholar]
- Ganeshan, B.; Skogen, K.; Pressney, I.; Coutroubis, D.; Miles, K. Tumour heterogeneity in oesophageal cancer assessed by CT texture analysis: Preliminary evidence of an association with tumour metabolism, stage, and survival. Clin. Radiol. 2012, 67, 157–164. [Google Scholar] [CrossRef]
- Rousseeuw, P.J. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J. Comput. Appl. Math. 1987, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Davies, D.L.; Bouldin, D.W. A Cluster Separation Measure. IEEE Trans. Pattern Anal. Mach. Intell. 1979, PAMI-1, 224–227. [Google Scholar] [CrossRef]
- Caliñski, T.; Harabasz, J. A Dendrite Method Foe Cluster Analysis. Commun. Stat. 1974, 3, 1–27. [Google Scholar]
- Pihur, M.V. Package “RankAggreg” Type Package Title Weighted Rank Aggregation; Version 0.6.6; CRAN: Vienna, Austria, 2020. [Google Scholar]
- Tateishi, U.; Terauchi, T.; Akashi-Tanaka, S.; Kinoshita, T.; Kano, D.; Daisaki, H.; Murano, T.; Tsuda, H.; Macapinlac, H.A. Comparative study of the value of dual tracer PET/CT in evaluating breast cancer. Cancer Sci. 2012, 103, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Sghedoni, R.; Erba, P.A.; Cavuto, S.; Froio, A.; De Berti, G.; Pisanello, A.; Fraternali, A.; Iori, M.; Iaccarino, C.; et al. Diagnostic performances of [18F]fluorocholine positron emission tomography in brain tumors. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Fiz, F.; Costa, G.; Gennaro, N.; la Bella, L.; Boichuk, A.; Sollini, M.; Politi, L.S.; Balzarini, L.; Torzilli, G.; Chiti, A.; et al. Contrast administration impacts CT-based radiomics of colorectal liver metastases and non-tumoral liver parenchyma revealing the “radiological” tumour microenvironment. Diagnostics 2021, 11, 1162. [Google Scholar] [CrossRef] [PubMed]
- Fiz, F.; Masci, C.; Costa, G.; Sollini, M.; Chiti, A.; Ieva, F.; Torzilli, G.; Viganò, L. PET/CT-based radiomics of mass-forming intrahepatic cholangiocarcinoma improves prediction of pathology data and survival. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3387–3400. [Google Scholar] [CrossRef] [PubMed]
- Fournier, L.; Costaridou, L.; Bidaut, L.; Michoux, N.; Lecouvet, F.E.; de Geus-Oei, L.F.; Boellaard, R.; Oprea-Lager, D.E.; Obuchowski, N.A.; Caroli, A.; et al. Incorporating radiomics into clinical trials: Expert consensus endorsed by the European Society of Radiology on considerations for data-driven compared to biologically driven quantitative biomarkers. Eur. Radiol. 2021, 31, 6001–6012. [Google Scholar] [CrossRef] [PubMed]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef]
- Sollini, M.; Cozzi, L.; Antunovic, L.; Chiti, A.; Kirienko, M. PET Radiomics in NSCLC: State of the art and a proposal for harmonization of methodology. Sci. Rep. 2017, 7, 358. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Marron, J.S. Object oriented data analysis: Sets of trees. Ann. Stat. 2007, 35, 1849–1873. [Google Scholar] [CrossRef]
- Georgina, F.A. Multiclass classification of tree structured objects: The k-nn case. BIOMAT 2013, 323–343. [Google Scholar] [CrossRef]
- Flesia, A.G. Unsupervised Classification of Tree Structured Objects. BIOMAT 2009, 280–299. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number of Patients (%) | |
|---|---|---|
| Number of metastases | Oligo (<3) | 15 (27%) |
| Multi (≥3) | 40 (73%) | |
| Oligo (<5) | 26 (47%) | |
| Multi (≥5) | 29 (53%) | |
| Intermediate (3 ≤ n < 5) | 11 (20%) | |
| Gleason Score (dichotomous) | <7 | 7 (13%) |
| =7 | 24 (44%) | |
| >7 | 18 (33%) | |
| Missing | 6 (10%) | |
| Ongoing therapy (ADT) | Y | 24 (44%) |
| N | 31 (56%) | |
| Primary treatment (initial therapy) | RP | 15 (27%) |
| RP+RT | 30 (54%) | |
| RT | 7 (13%) | |
| Missing | 3 (6%) | |
| PSA (dichotomous) | ≤1.93 * | 11 (20%) |
| >1.93 | 33 (40%) | |
| Missing | 11 (20%) | |
| Parameter | Cluster 1 | Cluster 2 | p-Value | |
|---|---|---|---|---|
| SUV_max | Median | 9.8350 | 10.8707 | 0.0187 * |
| Std. Dev. | 3.9163 | 7.8156 | ||
| Q3 | 12.4980 | 16.7168 | ||
| TLA (mL) | Median | 4.6851 | 6.0573 | <0.001 *** |
| Std. Dev. | 14.4136 | 90.1964 | ||
| Q3 | 14.1085 | 65.8136 | ||
| GLCM Entropy | Median | 1.4224 | 1.4524 | 0.0517 . |
| Std. Dev. | 0.4507 | 0.6868 | ||
| Q3 | 1.8524 | 2.2928 | ||
| Organ | Regional lymph nodes | 24 (15.4%) | 32 (18.1%) | 0.4202 |
| Distant lymph nodes | 40 (25.6%) | 36 (20.3%) | ||
| Skeleton | 92 (59%) | 109 (61.6%) | ||
| Parameter | Homogeneous | Heterogeneous | p-Value | |
|---|---|---|---|---|
| PSA | Median | 2.81 | 3.99 | 0.3189 |
| Std. Dev. | 1.5036 | 105.6279 | ||
| Q3 | 3.81 | 14.4974 | ||
| GS | Median | 7.0 | 7.0 | 0.7047 |
| Std. Dev. | 0.8314 | 1.2447 | ||
| Q3 | 8.0 | 8.0 | ||
| Nodal lesions | Median | 2.0 | 7.0 | 0.0001 *** |
| Std. Dev. | 0.8314 | 3.1359 | ||
| Q3 | 2.0 | 10.0 | ||
| Total Tumor Volume (mL) | Median | 1.9114 | 15.3200 | 0.0651 . |
| Std. Dev. | 5.7938 | 44.7814 | ||
| Q3 | 7.0262 | 31.1022 | ||
| Gleason Category | ≤7 | 5 (55%) | 26 (65%) | 0.5954 |
| >7 | 4 (45%) | 14 (35%) | ||
| Oligo or Multi (>3) | Oligo | 7 (70%) | 37 (82%) | <0.0001 *** |
| Multi | 3 (30%) | 8 (18%) | ||
| Oligo or Multi (>5) | Oligo | 10 (100%) | 29 (64%) | 0.0004 ** |
| Multi | 0 (0%) | 16 (36%) | ||
| 3 < Lesions ≤ 5 | <3 | 7 (70%) | 29 (64%) | 0.0001 *** |
| 3 < Lesions ≤ 5 | 3 (30%) | 8 (18%) | ||
| > 5 | 0 (0%) | 8 (18%) | ||
| Initial Therapy | RP + RT | 5 (55%) | 25 (58%) | 0.6293 |
| RP | 3 (33%) | 12 (28%) | ||
| RT | 1 (12%) | 6 (14%) | ||
| Ongoing Therapy | N | 6 (60%) | 25 (55%) | 0.7976 |
| Y | 4 (40%) | 20 (35%) | ||
| Combined therapy | N | 7 (78%) | 26 (66%) | 0.8810 |
| Y | 2 (22%) | 13 (34%) | ||
| Response to therapy | N | 9 (100%) | 29 (74%) | 0.4255 |
| Y | 0 (0%) | 10 (26%) | ||
| Parameter | # Phentypes_Silhouette | # Phentypes_ch | # Phentypes_db | Dispersion | Sum Branches |
|---|---|---|---|---|---|
| PSA | 0.0214 | 0.0234 | 0.0210 | 0.4953 | 0.0433 |
| GS | 0.0736 | 0.1976 | 0.3403 | 0.4672 | 0.1909 |
| Nodal Lesions | <0.0001 | <0.0001 | <0.0001 | 0.0016 | <0.0001 |
| Total Tumor Volume | 0.0002 | <0.0001 | 0.0004 | 0.4010 | 0.0020 |
| Gleason Category | 0.0004 | 0.0006 | 0.0086 | 0.0050 | 0.0061 |
| Oligo or Multi (>3) | 0.0002 | 0.0003 | 0.0003 | 0.0008 | 0.0003 |
| Oligo or Multi (>5) | 0.0088 | 0.0098 | 0.0119 | 0.6702 | 0.2933 |
| 3 < Lesions ≤ 5 | 0.0014 | 0.0016 | 0.0020 | 0.0344 | 0.0070 |
| Initial Therapy | 0.1931 | 0.2040 | 0.1908 | 0.1503 | 0.1444 |
| Ongoing Therapy | 0.6647 | 0.7010 | 0.6760 | 0.7529 | 0.8379 |
| Combined therapy | 0.6245 | 0.2221 | 0.5707 | 0.7968 | 0.6055 |
| Radiotherapy | 0.0003 | 0.0001 | 0.0003 | 0.0207 | <0.0001 |
| Hormonotherapy | 0.0783 | 0.6348 | 0.8975 | 0.7963 | 0.0717 |
| Difosfonate | 0.1608 | 0.2336 | 0.1212 | 0.1444 | 0.0727 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavinato, L.; Sollini, M.; Ragni, A.; Bartoli, F.; Zanca, R.; Pasqualetti, F.; Marciano, A.; Ieva, F.; Erba, P.A. Radiomics-Based Inter-Lesion Relation Network to Describe [18F]FMCH PET/CT Imaging Phenotypes in Prostate Cancer. Cancers 2023, 15, 823. https://doi.org/10.3390/cancers15030823
Cavinato L, Sollini M, Ragni A, Bartoli F, Zanca R, Pasqualetti F, Marciano A, Ieva F, Erba PA. Radiomics-Based Inter-Lesion Relation Network to Describe [18F]FMCH PET/CT Imaging Phenotypes in Prostate Cancer. Cancers. 2023; 15(3):823. https://doi.org/10.3390/cancers15030823
Chicago/Turabian StyleCavinato, Lara, Martina Sollini, Alessandra Ragni, Francesco Bartoli, Roberta Zanca, Francesco Pasqualetti, Andrea Marciano, Francesca Ieva, and Paola Anna Erba. 2023. "Radiomics-Based Inter-Lesion Relation Network to Describe [18F]FMCH PET/CT Imaging Phenotypes in Prostate Cancer" Cancers 15, no. 3: 823. https://doi.org/10.3390/cancers15030823