
Diagnostic Performance of Biomarkers for Bladder Cancer Detection Suitable for Community and Primary Care Settings: A Systematic Review and Meta-Analysis

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Sources
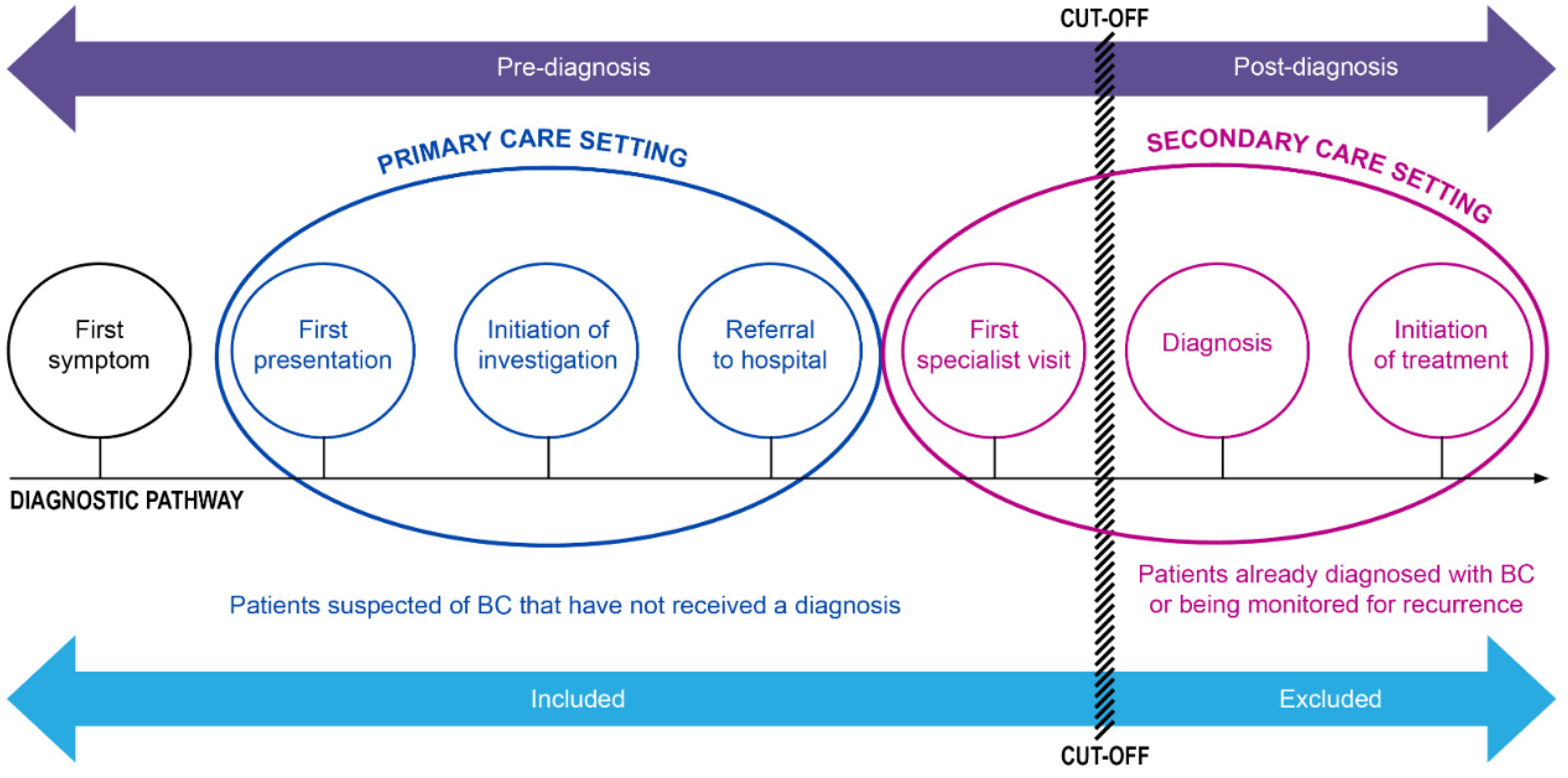
2.2. Inclusion & Exclusion Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Analysis
3. Results
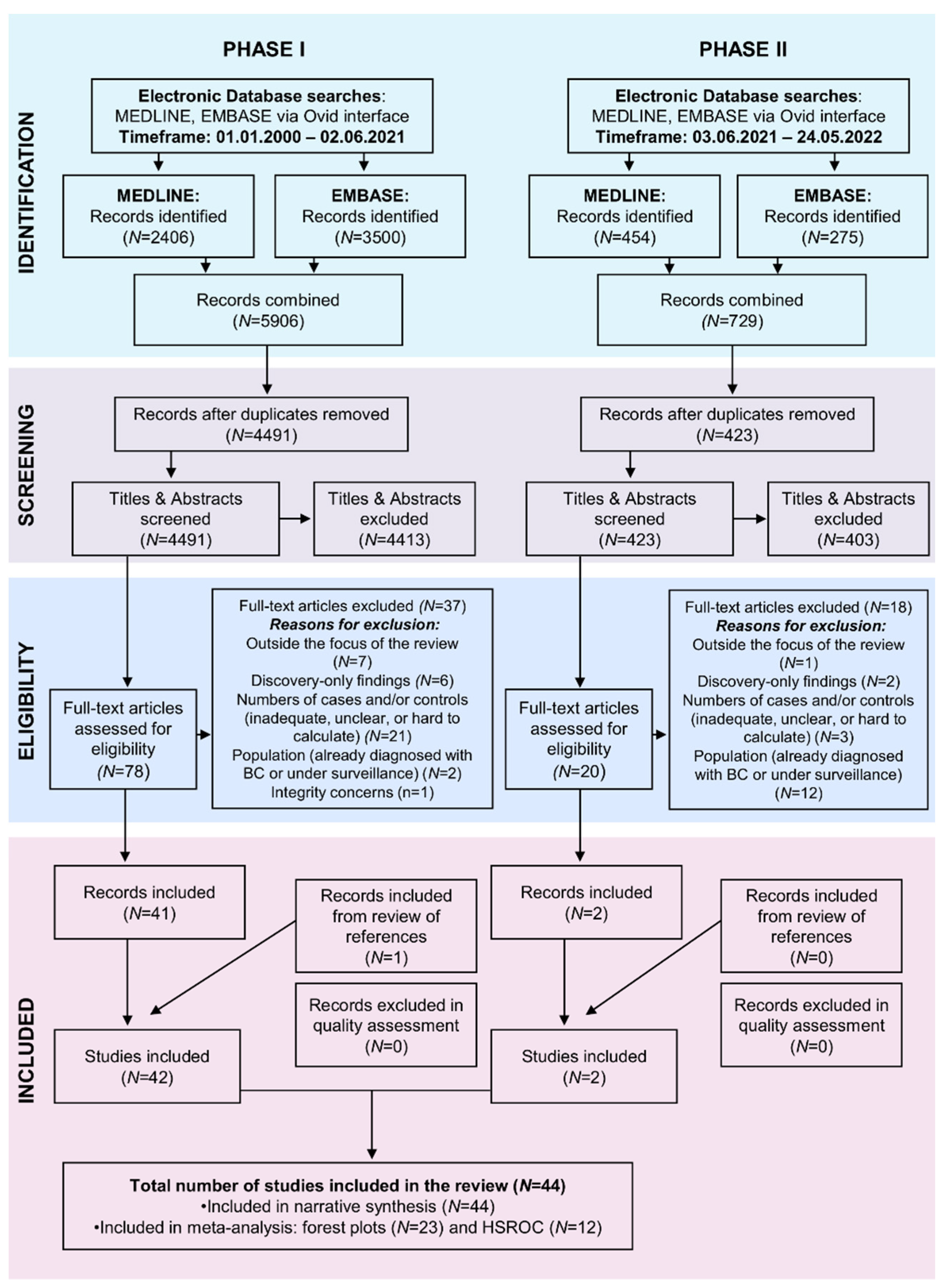
3.1. Selection Process
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Population Characteristics
3.5. Biomarker Characteristics
3.6. Meta-Analyses
3.6.1. Assessing Heterogeneity
3.6.2. Overall Performance and Sensitivity Analysis
3.7. Narrative Synthesis
3.7.1. For Biomarkers Reported in Three Studies or More
3.7.2. For Biomarkers with High Negative Predictive Value
4. Discussion
4.1. Summary of Main Findings
4.2. Comparison with Existing Literature
4.3. Strengths and Limitations
4.4. Implication for Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Van Valenberg, F.J.P.; Hiar, A.M.; Wallace, E.; Bridge, J.A.; Mayne, D.J.; Beqaj, S.; Sexton, W.J.; Lotan, Y.; Weizer, A.Z.; Jansz, G.K.; et al. Validation of an mRNA-based Urine Test for the Detection of Bladder Cancer in Patients with Haematuria. EAU 2021, 4, 93–101. [Google Scholar] [CrossRef]
- Rai, B.P.; Escrig, J.L.D.; Vale, L.; Kuusk, T.; Capoun, O.; Soukup, V.; Bruins, H.M.; Yuan, Y.; Violette, P.D.; Santesso, N.; et al. Systematic Review of the Incidence of and Risk Factors for Urothelial Cancers and Renal Cell Carcinoma Among Patients with Haematuria. Eur. Urol. 2022, 82, 182–192. [Google Scholar] [CrossRef]
- Zhou, Y.; Funston, G.; Lyratzopoulos, G.; Walter, F.M. Improving the Timely Detection of Bladder and Kidney Cancer in Primary Care. Adv. Ther. 2019, 36, 1778–1785. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Walter, F.M.; Singh, H.; Hamilton, W.; Abel, G.A.; Lyratzopoulos, G. Prolonged Diagnostic Intervals as Marker of Missed Diagnostic Opportunities in Bladder and Kidney Cancer Patients with Alarm Features: A Longitudinal Linked Data Study. Cancers 2021, 13, 156. [Google Scholar] [CrossRef]
- Tan, W.S.; Tan, W.P.; Tan, M.Y.; Khetrapal, P.; Dong, L.; deWinter, P.; Dong, L.; deWinter, P.; Feber, A.; Kelly, J.D. Novel urinary biomarkers for the detection of bladder cancer: A systematic review. Cancer Treat Rev. 2018, 69, 39–52. [Google Scholar] [CrossRef]
- Ng, K.; Stenzl, A.; Sharma, A.; Vasdev, N. Urinary biomarkers in bladder cancer: A review of the current landscape and future directions. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 41–51. [Google Scholar] [CrossRef]
- Zhu, C.Z.; Ting, H.N.; Ng, K.H.; Ong, T.A. A review on the accuracy of bladder cancer detection methods. J. Cancer 2019, 10, 4038–4044. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, E.; Ayaz-Shah, A.; Shinkins, B.; Jain, S.; Neal, R.D. A urine test for bladder cancer: Available soon in primary care? Trends Urol. Men’s Health 2020, 11, 18–21. [Google Scholar] [CrossRef]
- Giordano, A.; Soria, F. Role and efficacy of current biomarkers in bladder cancer. AME Med. J. 2020, 5, 6. [Google Scholar] [CrossRef]
- Dong, Y.; Zhang, T.; Li, X.; Yu, F.; Yu, H.; Shao, S. Urine biomarkers for the diagnosis of bladder cancer: A network meta-analysis. Urol. J. 2021, 18, 623–632. [Google Scholar]
- Hong, M.; He, G.; Goh, S.; Wei, A.; Low, X.; Tay, K.J.; Lim, T.K.H.; Yeong, J.; Khor, L.; Lim, T.S. Biomarkers for precision urothelial carcinoma diagnosis: Current approaches and the application of single-cell technologies. Cancers 2021, 13, 260. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, X.; Jiang, X.L.; Lu, D.; Yuan, Q.; Li, J. Diagnostic performance of nuclear matrix protein 22 and urine cytology for bladder cancer: A meta-analysis. Diagn. Cytopathol. 2022, 50, 300–312. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGarth, T.A.; Bossuyt, P.M.; PRISMA-DTA Group. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, P.ICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Walter, F.M.; Thompson, M.J.; Wellwood, I.; Abel, G.A.; Hamilton, W.; Johnson, M.; Lyratzopoulos, G.; Messenger, M.P.; Neal, R.D.; Rubin, G.; et al. Evaluating diagnostic strategies for early detection of cancer: The CanTest framework. BMC Cancer 2019, 19, 586. [Google Scholar] [CrossRef]
- Olesen, F.; Hansen, R.P.; Vedsted, P. Delay in diagnosis: The experience in Denmark. Br. J. Cancer 2009, 101, S5–S8. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, A.C.; Bossuyt, M.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Doebler, P.; Holling, H. Meta-Analysis of Diagnostic Accuracy with Mada. R Packag. 2015. Available online: https://bit.ly/36agmQy (accessed on 27 July 2022).
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.; Scholten, R.J.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef]
- Arends, L.R.; Hamza, T.H.; van Houwelingen, J.C.; Heijenbrok-Kal, M.H.; Hunink, M.G.M.; Stijnen, T. Bivariate Random Effects Meta-Analysis of ROC Curves. Med. Decis. Mak. 2008, 28, 621–638. [Google Scholar] [CrossRef]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences; Blackwell: Oxford, UK, 2006. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme. 2006, p. 92. Available online: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf (accessed on 12 October 2022).
- Greenhalgh, T.; Robert, G.; Macfalane, F.; Bate, P.; Kyriakidou, O. Diffusion of Innovations in Service Organizations: Systematic Review and Recommendations. Millbank Q. 2004, 82, 581–629. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef] [Green Version]
- Jellema, P.; van der Windt, D.A.W.M.; Bruinvels, D.J.; Mallen, C.D.; van Weyenberg, S.J.B.; Mulder, C.J.; de Vet, H.C.W. Value of symptoms and additional diagnostic tests for colorectal cancer in primary care: Systematic review and meta-analysis. BMJ 2010, 340, c1269. [Google Scholar] [CrossRef] [Green Version]
- Baeyens, J.P.; Serrien, B.; Goossens, M.; Clijsen, R. Questioning the “SPIN and SNOUT” rule in clinical testing. Arch. Physiother. 2019, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Attallah, A.; El-Far, M.; Abdallah, S.O.; El-Waseef, A.M.; Omran, M.M.; Abdelrazek, M.A.; Attallah, A.A.; Saadh, M.J.; Radwan, M.; El-waffaey, K.A.; et al. Combined use of epithelial membrane antigen and nuclear matrix protein 52 as sensitive biomarker for detection of bladder cancer. Int. J. Biol. Markers 2015, 30, e407–e413. [Google Scholar] [CrossRef]
- Barbieri, C.E.; Cha, E.K.; Chromecki, T.F.; Dunning, A.; Lotan, Y.; Svatek, R.S.; Scherr, D.S.; Karakiewicz, P.I.; Sun, M.; Mazumdar, M.; et al. Decision curve analysis assessing the clinical benefir of NMP22 in the detection of bladder cancer: Secondary analysis of a prospective trial. BJUI 2011, 109, 685–690. [Google Scholar] [CrossRef] [Green Version]
- Bhuiyan, J.; Akhter, J.; O’Kane, D.J. Performance characteristics of multiple urinary tumor markers and sample collection techniques in the detection of transitional cell carcinoma of the bladder. Clin. Chim. Acta 2003, 331, 69–77. [Google Scholar] [CrossRef]
- Critselis, E.; Rava, M.; Marquez, M.; Lygirou, V.; Chatzicharalambous, D.; Liapi, P.; Lictinghagen, R.; Brand, K.; Cecchini, L.; Vlahou, A.; et al. Diagnostic and Prognostic Performance of Secreted Protein Acidic and Rich in Cysteine (SPARC) Assay for Detecting Primary and Recurrent Urinary Bladder Cancer. Proteom. Clin. Appl. 2019, 13, e1800148. [Google Scholar] [CrossRef]
- Dahmcke, C.M.; Steven, K.E.; Larsen, L.K.; Poulsen, A.L.; Abdul-Al, A.; Dahl, C.; Guldberg, P. A prospective blinded evaluation of urine-DNA testing for detection of urothelial bladder carcinoma in patients with gross hematuria. Eur. Urol. 2016, 70, 916–919. [Google Scholar] [CrossRef]
- Davidson, P.J.; McGeoch, G.; Shand, B. Assessment of a clinical pathway for investigation of haematuria that reduces the need for cystoscopy. NZMA 2020, 133, 71–82. [Google Scholar]
- Deininger, S.; Todenhöfer, T.; Hennenlotter, J.; Gerber, V.; Schwarz, J.; Bedke, J.; Schwentner, C.; Stenzl, A.; Rausch, S. Impact of variant microscopic interpretation of the uCyt+ immunocytological urine test for the detection of the bladder cancer. Diagn. Cytopathol. 2018, 46, 111–116. [Google Scholar] [CrossRef]
- Dudderidge, T.; Stockley, J.; Nabi, G.; Mom, J.; Uzem-Eronini, N.; Hrouda, D.; Cresswell, J.; McCracken, S.R.C. A novel, non-invasive test enabling bladder cancer detection in urine sediment of patients presenting with haematuria—A prospective multicentre performance evaluation of ADXBLADDER. Eur. Urol. Oncol. 2019, 3, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Eissa, S.; Swellam, M.; Ali-Labib, R.; Mansour, A.; El-Malt, O.; Tash, F.M. Detection of telomerase in urine by 3 methods: Evaluation of diagnostic accuracy for bladder cancer. J. Urol. 2007, 178 Pt 1, 1068–1072. [Google Scholar] [CrossRef] [PubMed]
- Eissa, S.; Ali-Labib, R.; Swellam, M.; Bassiony, M.; Tash, F.; El-Zayat, T.M. Noninvasive diagnosis of bladder cancer by detection of matrix metalloproteinases (MMP-2 and MMP-9) and their inhibitor (TIMP-2) in urine. Eur. Urol. 2007, 52, 1388–1396. [Google Scholar] [CrossRef]
- Eissa, S.; Salem, A.M.; Zohny, S.F.; Hegazy, M.G.A. The diagnostic efficacy of urinary TGF-β1 and VEGF in bladder cancer: Comparison with voided urine cytology. Cancer Biomark. 2007, 3, 275–285. [Google Scholar] [CrossRef]
- Eissa, S.; Swellam, M.; Ali-Labib, R.; El-Zayat, T.; El Ahmady, O. A panel of angiogenic factors for early bladder cancer detection: Enzyme immunoassay and western blot. J. Urol. 2009, 181, 1353–1360. [Google Scholar] [CrossRef]
- Eissa, S.; Swellam, M.; Shehata, H.; El-Khouly, I.M.; El-Zayat, T.; El-Ahmady, O. Expression of HYAL1 and Survivin, R.NA as diagnostic molecular markers for bladder cancer. J. Urol. 2010, 183, 493–498. [Google Scholar] [CrossRef]
- Eissa, S.; Swellam, M.; Amin, A.; Balbaa, M.E.; Yacout, G.A.; El-Zayat, T.M. The clinical relevance of urine-based markers for diagnosis of bladder cancer. Med. Oncol. 2011, 28, 513–518. [Google Scholar] [CrossRef]
- Eissa, S.; Zohny, F.S.; Shehata, H.H.; Hegazy, M.G.A.; Salem, A.M.; Esmat, M. Urinary retinoic acid receptor-β2 gene promoter methylation and hyaluronidase activity as noninvasive tests for diagnosis of bladder cancer. Clin. Biochem. 2012, 45, 402–407. [Google Scholar] [CrossRef]
- Eissa, S.; Matboli, M.; Mansour, A.; Mohamed, S.; Awad, N.; Kotb, Y.M. Evaluation of urinary HURP mRNA as a marker for detection of bladder cancer: Relation to bilharziasis. Med. Oncol. 2014, 31, 804. [Google Scholar] [CrossRef]
- Eissa, S.; Shawky, S.M.; Matboli, M.; Mohamed, S.; Azzazy, H.M. Direct detection of unamplified hepatoma upregulated protein RNA in urine using gold nanoparticles for bladder cancer diagnosis. Clin Biochem. 2014, 47, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Fu, F.; Zeng, F.; Sun, Z.; Jin, F. Head-to head comparison of serum and urine cytokeratin-19 fragnents (CYFRA 21-1) for bladder cancer diagnosis. Transl. Cancer Res. 2018, 7, 55–59. [Google Scholar] [CrossRef]
- Grossman, H.B.; Messing, E.; Soloway, M.; Tomera, K.; Katz, G.; Berger, Y.; Shen, Y. Detection of bladder cancer using a point-of-care proteomic assay. JAMA 2005, 293, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Horstmann, M.; Todenhöfer, T.; Hennenlotter, J.; Aufdeklamm, S.; Mischinger, J.; Kuehs, U.; Gakis, G.; Stenzl, A.; Schwentener, C. Influence of age on false positive rates of urine-based tumor markers. World J. Urol. 2013, 31, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Karnes, J.R.; Fernandez, C.A.; Shuber, A.P. A noninvasive multianalyte urine-based diagnostic assay for urothelial cancer of the bladder in the evaluation of haematuria. Mayo Clin. Proc. 2012, 87, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.D.; Dudderidge, T.J.; Wollenschlaeger, A.; Okoturo, O.; Burling, K.; Tulloch, F.; Halsall, I.; Prevost, T.; Prevost, A.T.; Vasconcelos, J.C.; et al. Bladder cancer diagnosis and identification of clinically significant disease by combined urinary detection of Mcm5 and Nuclear matric protein 22. PLoS ONE 2012, 7, e40305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Shi, B.; Hao, C.; Wang, Q.; Lv, Q.; Xing, N.; Shou, J.; Qu, L.; Gao, Y.; Qin, C.; et al. Urine gamma-synuclein as a biomarker for the diagnosis of bladder cancer. Oncotarget 2016, 7, 43432–43441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meiers, I.; Singh, H.; Hossain, D.; Lang, K.; Liu, L.; Qian, J.; Verhest, A.P.; Bostwick, D.G. Improved filter method for urine sediment detection of urothelial carcinoma by fluorescence in situ hybridization. Arch. Pathol. Lab. Med. 2007, 131, 1574–1577. [Google Scholar] [CrossRef]
- O’Sullivan, P.; Sharples, K.; Dalphin, M.; Davidson, P.; Gilling, P.; Cambridge, L.; Harvey, J.; Toro, T.; Giles, N.; Luxmanan, C.; et al. A multigene urine test for the detection and stratification of bladder cancer in patients presenting with haematuria. J. Urol. 2012, 188, 741–747. [Google Scholar] [CrossRef]
- Oertl, A.; Balan, S.; Okoński, P.K.; Jonas, D.; Oremek, G.M. Nuclear matrix protein 22 (NMP 22) a tumour marker for detection of bladder cancer. Clin. Exp. Med. Lett. 2007, 48, 15–17. [Google Scholar]
- Piaton, E.; Daniel, L.; Verriele, V.; Dalifard, I.; Zimmermann, U.; Renaudin, K.; Gobet, F.; Caratero, A.; Desvaux, D.; Pouille, Y.; et al. Improved detection of urothelial carcinomas with fluorescence immunocytochemistry (uCyt+ Assay) and urinary cytology: Results of a French prospective multicenter study. Lab. Investig. 2003, 83, 845–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulakis, V.; Witzsch, U.; De Vries, R.; Altmannsberger, H.M.; Manyak, M.J.; Becht, E. A comparison of urinary nuclear matrix protein-22 and bladder tumour antigen tests with voided urinary cytology in detecting and following bladder cancer: The prognostic value of false-positive results. BJU Int. 2001, 88, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Saad, A.; Hanbury, D.C.; McNicholas, T.A.; Boustead, G.B.; Morgan, S.; Woodman, A.C. A study comparing various noninvasive methods of detecting bladder cancer in urine. BJU Int. 2002, 89, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Sajid, M.T.; Zafar, M.R.; Ahmad, H.; Ullah, S.; Mirza, Z.I.; Shahzad, K. Diagnostic accuracy of the NMP 22 and urine cytology for detection of transitional cell carcinoma urine bladder taking cystoscopy as gold standard. Pak. J. Med. Sci. 2020, 36, 705–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Carbayo, M.; Urrutia, M.; González de Buitrago, J.M.; Navajo, J.A. Evaluation of two urinary tumor markers: Bladder tumor fibronectin and cytokeratin 18 for the diagnosis of bladder cancer. Clin. Cancer Res. 2000, 6, 3585–3594. [Google Scholar]
- Sarosdy, M.F.; Kahn, P.R.; Ziffer, M.D.; Love, M.R.; Barkin, J.; Abara, E.O.; Jansz, K.; Bridge, J.A.; Johansson, S.L.; Person, D.L.; et al. Use of a multitarget fluorescence in situ hybridization assay to diagnose bladder cancer in patients with haematuria. J. Urol. 2006, 176, 44–47. [Google Scholar] [CrossRef]
- Shang, D.; Liu, Y.; Xu, X.; Chen, Z.; Wang, D. Diagnostic value comparison of CellDetect, fluorescent in situ hybridization (FISH), and cytology in urothelial carcinoma. Cancer Cell Int. 2021, 21, 465. [Google Scholar] [CrossRef]
- Todenhöfer, T.; Hennenlotter, J.; Esser, M.; Mohrhardt, S.; Tews, V.; Aufderklamm, S.; Gakis, G.; Kuehs, U.; Stenzl, A.; Schwentner, C. Combined application of cytology and molecular urine markers to improve the detection of urothelial carcinoma. Cancer Cytopathol. 2013, 121, 252–260. [Google Scholar] [CrossRef]
- Todenhöfer, T.; Hennenlotter, J.; Aufderklamm, S.; Kühs, U.; Gakis, G.; Germann, M.; Stenzl, A.; Schwentner, C. Individual risk assessment in bladder cancer patients based on a multi-marker panel. J. Cancer Res. Clin. Oncol. 2013, 139, 49–56. [Google Scholar] [CrossRef]
- Todenhöfer, T.; Hennenlotter, J.; Tews, V.; Gakis, G.; Aufderklamm, S.; Kuehs, U.; Stenzl, A.; Schwenter, C. Impact of different grades of microscopic hematuria on the performance of urine-based markers for the detection of urothelial carcinoma. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 1148–1154. [Google Scholar] [CrossRef] [PubMed]
- Van Kessel, K.E.M.; Van neste, L.; Lurkin, I.; Zwarthoff, E.C.; Criekinge, W.V. Evaluation of an epigenetic profile for the detection of bladder cancer in patients with hematuria. J. Urol. 2016, 195, 601–607. [Google Scholar] [CrossRef]
- Van Kessel, K.E.M.; Beukers, W.; Lurkin, I.; Ziel-van der Made, A.; van der Keur, K.A.; Boormans, J.L.; Dyrskjøt, L.; Márquez, M.; Ørntoft, T.F.; Real, F.X.; et al. Validation of a DNA methylation-mutation urine assay to select patients with hematuria for cystoscopy. J. Urol. 2017, 197 Pt 1, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Van Kessel, K.E.M.; de Jong, J.J.; Ziel-van der Made, A.C.J.; Roshani, H.; Haensel, S.M.; Wolterbeek, J.H.; Boevé, E.R.; Oomens, E.H.G.M.; van Casteren, N.J.; Krispin, M.; et al. A urine based genomic assay to triage patients with hematuria for cystoscopy. J. Urol. 2020, 204, 50–57. [Google Scholar] [CrossRef]
- Virk, R.K.; Abro, S.; Muus Martinez de Ubago, J.; Pambuccian, S.E.; Quek, M.L.; Wojcik, E.M.; Mehrotra, S.; Chatt, G.U.; Barkan, G.A. The value of the UroVysion® FISH assay in the risk-stratification of patients with “atypical urothelial cells” in urinary cytology specimens. Diagn. Cytopathol. 2017, 45, 481–500. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.G.; Baxter, L.; Ott, S.; Gordon, N.S.; Wang, J.; Patel, P.; Piechocki, K.; Silcock, L.; Sale, C.; Zeegers, M.P.; et al. Highly Sensitive and Specific Detection of Bladder Cancer via Targeted Ultra-deep Sequencing of Urinary, D.NA. Eur. Urol. Oncol. 2022. [Google Scholar] [CrossRef]
- Wu, Y.; Jiang, G.; Zhang, N.; Liu, S.; Lin, X.; Perschon, C.; Zheng, L.S.; Ding, Q.; Wang, X.; Na, R.; et al. HOXA9, P.CDH17, P.OU4F2, and ONECUT2 as a Urinary Biomarker Combination for the Detection of Bladder Cancer in Chinese Patients with Hematuria. Eur. Urol. Focus 2020, 15, 284–291. [Google Scholar] [CrossRef]
- Zhou, L.; Yang, K.; Li, X.; Ding, Y.; Mu, D.; Li, H.; Yan, Y.; Li, J.; Wang, D.; Li, W.; et al. Application of fluorescence in situ hybridization in the detection of bladder transitional-cell carcinoma: A multi-center clinical study based on Chinese population. Asian J. Urol. 2019, 6, 114–121. [Google Scholar] [CrossRef]
- Guo, A.; Wang, X.; Gao, L.; Shi, J.; Sun, C.; Wan, Z. Bladder tumour antigen (BTA stat) test compared to the urine cytology in the diagnosis of bladder cancer: A meta-analysis. Can. Urol. Assoc. J. 2014, 8, e347–e352. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Gore, J.L.; Buckley, D.; Fu, R.; Gustafon, K.; Griffin, J.C.; Grusing, S.; Selph, S. Urinary biomarkers for diagnosis of bladder cancer. Ann. Intern. Med. 2015, 163, 922–931. [Google Scholar] [CrossRef] [Green Version]
- He, H.; Han, C.; Hao, L.; Zang, G. ImmunoCyt test compared to cytology in the diagnosis of bladder cancer: A meta-analysis. Oncol. Lett. 2016, 12, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Que, H.; Suo, C.; Han, Z.; Tao, J.; Huang, Z.; Ju, X.; Tan, R.; Gu, M. Evaluation of the NMP22 BladderChek test for detecting bladder cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 100648–100656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willis, B.H. Spectrum bias—Why clinicians need to be cautious when applying diagnostic test studies. Fam. Pract. 2008, 25, 390–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usher-Smith, J.A.; Sharp, S.J.; Griffin, S.J. The spectrum effect in tests for risk prediction, screening, and diagnosis. BMJ 2016, 353, i3139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciarra, A.; Di Lascio, G.; Del Giudice, F.; Leoncini, P.P.; Salciccia, S.; Gentilucci, A.; Porreca, A.; Chung, B.I.; Di Pierro, G.; Busetto, G.M.; et al. Comparison of the clinical usefulness of different urinary tests for the initial detection of bladder cancer: A systematic review. Curr. Urol. 2021, 15, 22–32. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Butaney, M.; Weight, C.J.; Kumar, R.; Konety, B.R. Urinary biomarkers in the evaluation of primary hematuria: A systematic review and meta-analysis. Bladder Cancer 2018, 4, 353–363. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, N.; Hicks, G.; Benton, S.C.; Abulafi, M. The diagnostic accuracy of the faecal immunochemical test for colorectal cancer in risk-stratified symptomatic patients. Ann. R. Coll. Surg. Engl. 2020, 102, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.E.R.; Abel, G.A.; Atkins, A.; Byford, R.; Davies, S.J.; Mays, J.; McDonald, T.J.; Miller, J.; Neck, C.; Renninson, J.; et al. Diagnostic performance of a faecal immunochemical test for patients with low-risk symptoms of colorectal cancer in primary care: An evaluation in the South West of England. Br. J. Cancer 2021, 124, 1231–1236. [Google Scholar] [CrossRef]
- Booth, R.; Carten, R.; D’Souza, N.; Westwood, M.; Kleijnen, J.; Abulafi, M. Role of the faecal immunochemical test in patients with risk-stratified suspected colorectal cancer symptoms: A systematic review and meta-analysis to inform the ACPGBI/BSG guidelines. Lancet Reg. Health Eur. 2022, 23, 100518. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Context | Population | Intervention | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Country | Recruitment Timeline | Design | Clinical Setting: (Hospital (H), Community (Co), Unclear (U)) | Cases | Controls | Age | Gender (M/F) | Risk Factors | Symptoms | Biomarker/Test | |||||||||
| Cases (C) | All (Con) | Non-Malignant (NM) | Healthy Controls (HC) | Range | Mean (SD) or Median 1 | Smoking (N) | Other (N) | Haematuria | UTIs | Other | ||||||||||
| VH | NVH | |||||||||||||||||||
| Attallah et al. 2015 [30] | Egypt | NA | Prospective | Single centre | NA | H | 66 | 94 | 54 | 40 | C (44–81) NM (45–70) HC (45–65) | C (60.6 ± 10.6) NM (58.6 ± 11.2) HC (56.2 ± 8.2) | 106M:54F | - | - | x | - | - | Cystitis | EMA |
| NMP-52 | ||||||||||||||||||||
| EMA + NMP-52 | ||||||||||||||||||||
| Barbieri et al. 2011 [31] | USA | 2001–2002 | Retrospective | Multi-centre | Cohort | H&Co | 72 | 1231 | - | - | - | 66 ± 13.6 | 738M:565F | 474Y:829N | - | x | - | - | Base model (age, gender, smoker, race, haematuria) + NMP-22 | |
| Base model (age, gender, smoker, race, haematuria) + NMP-22 + Cytology | ||||||||||||||||||||
| Bhuiyan et al. 2003 [32] | NA | NA | NA | NA | NA | U | 70 | 163 | - | - | - | - | - | - | - | - | - | - | - | Telomerase |
| BTAstat | ||||||||||||||||||||
| NMP-22 | ||||||||||||||||||||
| Telomerase + Hb Dipstick | ||||||||||||||||||||
| Critselis et al. 2019 [33] | Spain | 2009–2012 | Prospective | Single centre | Cross-sectional | H | 179 | 85 | 85 | 0 | - | 69.4 ± 12.2 | 218M:46F | - | - | x | - | - | SPARC | |
| Dahmcke et al. 2016 [34] | Denmark | 2013–2015 | Prospective | Single centre | Evaluation | H | 99 | 376 | - | - | C (26–91) Con (18–91) | C 69 Con 64 | 355M:120F | - | - | x | - | - | - | TERT, FGFR3 and SALL3, ONECUT2, CCNA1, BCL2, EOMES, and VIM |
| TERT | ||||||||||||||||||||
| ONECUT2 | ||||||||||||||||||||
| VIM | ||||||||||||||||||||
| SALL3 | ||||||||||||||||||||
| CCNA1 | ||||||||||||||||||||
| BCL2 | ||||||||||||||||||||
| EOMES | ||||||||||||||||||||
| FGFR3 | ||||||||||||||||||||
| TERT + FGFR3 | ||||||||||||||||||||
| CCNA1 + ONECUT2 + BCL2 + EOMES + SALL3 + VIM | ||||||||||||||||||||
| TERT + FGFR3 + CCNA1 + ONECUT2 + BCL2 + EOMES + SALL3 + VIM | ||||||||||||||||||||
| TERT + FGFR3 + N + A1 + ONECUT2 + BCL2 + EOMES + SALL3 | ||||||||||||||||||||
| TERT + FGFR3 + CCNA1 + ONECUT2 + BCL2 + EOMES | ||||||||||||||||||||
| TERT + FGFR3 + CCNA1 + ONECUT2 + BCL2 | ||||||||||||||||||||
| TERT + FGFR3 + CCNA1 + ONECUT2 | ||||||||||||||||||||
| TERT + FGFR3 + CCNA1 | ||||||||||||||||||||
| TERT + ONECUT2 | ||||||||||||||||||||
| Davidson et al. 2020 [35] | New Zealand | 2018-2019 | Prospective | Multi-centre | Cohort | H&Co | 51 | 833 | 833 | 0 | (14–97) | 63.1 ± 16.2; median:65 | 71 Current: 293 Former: 520 Never | 1 Previous cancer diagnosis; 1 Radiation therapy of pelvis | x | x | x | Cystitis; Upper tract stones; vascular Prostate; Anticoagulation; Renal disease; Primary amyloidosis | CxBladder Triage (CxbT) | |
| CxbT + Imaging | ||||||||||||||||||||
| Deininger et al. 2017 [36] | Germany | 2006–2009 | Retrospective | Single centre | Cohort | H | 68 | 376 | - | - | (18–93) | median:67 | 376M:68F | 61 Current: 82 Former: 274 Never: 27 n/a | - | x | x | Benign prostatic hyperplasia; Prostate cancer | uCyt+ 7 | |
| Dudderidge et al. 2020 [37] | UK | 2016–2017 | Prospective | Multi-centre | Cohort | H | 74 | 782 | 782 | - | (54–73) | median:64 | 487M:369F | - | - | x | x | x | - | ADXBLADDER |
| Eissa et al. 2007 [38] | Egypt | NA | Prospective | Single centre | NA | H | 200 | 115 | 85 | 30 | C (37–78) NM (34–70) HC (30–78) | C (57.8 ± 10) NM (51 ± 11.8) HC (54.1 ± 9.7) | - | 136Y:64N 2 | 85 Benign schistosomal urological lesions | - | - | - | - | RTA |
| hRT | ||||||||||||||||||||
| hTERT | ||||||||||||||||||||
| RTA + hRT | ||||||||||||||||||||
| RTA + hTERT | ||||||||||||||||||||
| hTR + hTERT | ||||||||||||||||||||
| RTA + hRT + hTERT | ||||||||||||||||||||
| HRT + Cytology | ||||||||||||||||||||
| hRT + Cytology | ||||||||||||||||||||
| RTA + hRT + Cytology | ||||||||||||||||||||
| RTA + hTERT + Cytology | ||||||||||||||||||||
| RTA + hRT + HTERT + Cytology | ||||||||||||||||||||
| Eissa et al. 2007 [39] | Egypt | NA | Prospective | Single centre | NA | H | 154 | 90 | 60 | 30 | C (25–82) NM (25–79) HC (27–50) | C (57 ± 12) NM (51± 14) HC (45.36 ± 5.2) | 164M:80F | - | 60 Benign schistosomal urologic lesions | - | - | - | - | MMP-2 |
| MMP-9 | ||||||||||||||||||||
| TIMP-2 | ||||||||||||||||||||
| MMP-2 + TIMP-2 | ||||||||||||||||||||
| MMP-9 + TIMP2 | ||||||||||||||||||||
| MMP zymography | ||||||||||||||||||||
| MMP-2 + Cytology | ||||||||||||||||||||
| MMP-9 + Cytology | ||||||||||||||||||||
| TIMP-2 + Cytology | ||||||||||||||||||||
| MMP-2+ TIMP-2 ratio + Cytology | ||||||||||||||||||||
| MMP-9+ TIMP-2 ratio + Cytology | ||||||||||||||||||||
| MMP zymography + Cytology | ||||||||||||||||||||
| Eissa et al. 2007 [40] | Egypt | NA | Prospective | Single centre | NA | H | 120 | 109 | 54 | 55 | C (40–80) NM (17–80) HC (17–50) | C (55.0 ± 7.76) NM (49.8 ± 15.75) HC (21.8 ± 8.47) | - | - | - | - | - | - | Cystitis; Ureteral stone; Renal stone; Nephritis; Combined disorders | TGF-β1 |
| VEGF | ||||||||||||||||||||
| TGF-β1 + VEGF | ||||||||||||||||||||
| TGF-β1 + VEGF + Cytology | ||||||||||||||||||||
| TGF-β1 + Cytology | ||||||||||||||||||||
| VEGF + Cytology | ||||||||||||||||||||
| Eissa et al. 2009 [41] | Egypt | NA | Prospective | Single centre | Case-control | H | 240 | 218 | 108 | 110 | 182 <45: 276 >45 | - | 278M:180F | 217Y:241N | 70 Schistosomal dysplasia; 28 schistosomal cystitis | - | - | - | benign prostatic hyperplasia | VEGF |
| bFGF | ||||||||||||||||||||
| ANG | ||||||||||||||||||||
| HGF | ||||||||||||||||||||
| Eissa et al. 2010 [42] | Egypt | NA | NA | NA | NA | U | 166 | 212 | 112 | 100 | C (26–83) NM (18–75) HC (25–60) | C (60 ± 11) NM (48 ± 15) HC (49 ± 10) | - | - | - | - | - | - | - | HYAL-1 Qual |
| HYAL-1 Semi-quant | ||||||||||||||||||||
| Survivin Qual | ||||||||||||||||||||
| Survivin Semi-quant | ||||||||||||||||||||
| HYAL-1 + Survivin Qual | ||||||||||||||||||||
| HYAL-1 + Survivin Semi-quant | ||||||||||||||||||||
| HYAL-1 Qual + Cytology | ||||||||||||||||||||
| HYAL-1 Semi-quant + Cytology | ||||||||||||||||||||
| Survivin Qual + Cytology | ||||||||||||||||||||
| Survivin Semi-quant + Cytology | ||||||||||||||||||||
| HYAL-1 Qual + Survivin Qual + Cytology | ||||||||||||||||||||
| HYAL-1 Semi-quant + Survivin Semi-quant + Cytology | ||||||||||||||||||||
| Eissa et al. 2011 [43] | Egypt | NA | Prospective | Single centre | NA | H | 132 | 108 | 60 | 48 | C (30–78) NM (25–72) HC (25–45) | C (56.60 ± 9.60) NM (51.30 ± 14.0) HC (29.20 ± 10.60) | - | - | - | - | - | - | - | FN |
| RTA | ||||||||||||||||||||
| CK20 | ||||||||||||||||||||
| CK20 + RTA | ||||||||||||||||||||
| CK20 + FN + RTA | ||||||||||||||||||||
| FN + Cytology | ||||||||||||||||||||
| CK20 + Cytology | ||||||||||||||||||||
| RTA+ Cytology | ||||||||||||||||||||
| FN+ CK20+ Cytology | ||||||||||||||||||||
| CK20 + RTA + Cytology | ||||||||||||||||||||
| FN + CK20 + RTA + Cytology | ||||||||||||||||||||
| Eissa et al. 2012 [44] | Egypt | NA | Prospective | Single centre | NA | H | 100 | 116 | 65 | 51 | C (37–78) NM (31–75) HC (29–67) | C (57.40 ± 9.60) NM (52.6 ± 13.8) HC (46.9 ± 9.87) | - | 64Y:36N2 | 65 Schistosomiasis positive | - | - | - | Cystitis; Ureteral stone; Renal stone; Nephritis; Combined disorders | RAR-B2 |
| HYAL-1 | ||||||||||||||||||||
| RAR-β2 + HYAL-1 | ||||||||||||||||||||
| RAR-β2 + Cytology | ||||||||||||||||||||
| HYAL-1 + Cytology | ||||||||||||||||||||
| RAR-β2 + HYAL-1 + Cytology | ||||||||||||||||||||
| Eissa et al. 2014 [45] | Egypt | 2011-2012 | Prospective | Single centre | NA | H | 211 | 133 | 71 | 62 | C (25–79) NM (25–66) HC (29–76) | C (52 ± 10) NM (50 ± 8) HC (51 ± 10) | 252M:91F 1 Unknown | 101Y:243N | 193 Schistosomiasis positive | - | - | - | - | HURP |
| HURP + Cytology | ||||||||||||||||||||
| Eissa et al. 2014 [46] | Egypt | 2011–2012 | Prospective | Single centre | NA | H | 50 | 50 | 25 | 25 | C (37–79) NM (25–68) HC (28–79) | C (59.8 ± 9.3) NM (52.88 ± 9.4) HC (45.44 ± 11.9) | 78M:22F | 38Y:62N | Schistosomiasis dysplastic lesions | x | - | Renal stone; Urethral stricture; Chronic irritative symptoms | HURP | |
| HURP + Cytology | ||||||||||||||||||||
| Fu et al. 2018 [47] | China | 2016 | Prospective | Single centre | NA | H | 152 | 82 | 82 | 0 | - | C (63 ± 13) Con (64 ± 13) | 179M:55F | - | - | - | - | x | Cystitis; urolithiasis; kidney carcinoma; benign bladder tumor 3 | CYFRA21-1 |
| Grossman et al. 2005 [48] | USA | 2001-2002 | Prospective | Multi-centre | Trial | H&Co | 79 | 1252 | 685 | 567 | (18–96) | 58.7 ± 14.3 | 759M:572F | - | 120 Black non-Hispanic; 1089 White non-Hispanic; 84 Hispanic; 26 Asian;6 Other;6 Unknown | x | - | x | Benign prostatic hypertrophy; prostatitis; cystitis; inflammation; trigonitis; urinary tract infection; erythema; hyperplasia; squamous; metaplasia; cysts and polyps; calculi; trabeculations; other benign disease; kidney and genitourinary; other cancer history; non bladder; other active cancer; non bladder | NMP-22 |
| Horstmann et al. 2012 [49] | Germany | NA | Prospective | Single centre | Cohort | U | 377 | 1177 | - | - | (23–96) | 67 | 1169M:385F | - | 605 with previous bladder cancer diagnosis4 | x | - | x | UroVysion | |
| uCyt+ | ||||||||||||||||||||
| NMP-22 | ||||||||||||||||||||
| Karnes et al. 2012 [50] | NA | 2009–2011 | Prospective | Multi-centre | Observational | H&C | 58 | 690 | - | - | - | C (71 ± 10.0) Con (64 ± 9.6) | 450M:298F | 444Y:300N: 4 Unknown | - | x | - | - | MADR Assay | |
| FGFR3 | ||||||||||||||||||||
| FGFR3 + Cytology | ||||||||||||||||||||
| Kelly et al. 2012 [51] | UK | NA | Prospective | Multi-centre | Observational | H | 222 | 1455 | 755 | 700 | (49–73) | 60.7 ± 16.3 median:63 | 1040M:637F | - | - | x | x | x | Urolithiasis; other malignancies; other benign conditions 3 | Mcm5 |
| NMP-22 | ||||||||||||||||||||
| Mcm5 + NMP-22 | ||||||||||||||||||||
| Liu et al. 2016 [52] | China | 2010–2014 | Prospective | Multi-centre | Cohort | H | 141 | 135 | - | 135 | - | - | - | - | - | - | - | - | - | Gamma-synuclein (SNCG) |
| Meiers et al. 2007 [53] | Belgium | NA | NA | NA | NA | U | 170 | 454 | 454 | 0 | - | - | - | - | - | - | - | - | - | UroVysion |
| O’Sullivan et al. 2012 [54] | Australasia (NZ/Australia) | NA | Prospective | Multi-centre | Cohort | H | 66 | 419 | 255 | 164 | (59–77) | median:69 | 389M:96F | 76 Current: 215 Former: 194 Never | 423 European; 33 Māori; 29 Other | x | x | - | - | uRNA-D |
| NMP-22 | ||||||||||||||||||||
| NMP-22 BladderChek | ||||||||||||||||||||
| Cxbladder | ||||||||||||||||||||
| Oertl et al. 2007 [55] | NA | NA | Prospective | NA | NA | U | 56 | 51 | 51 | 0 | - | - | - | - | Benign bladder tumour | - | - | - | Cystitis; pyelonephritis; urethritis | NMP-22 |
| Piaton et al. 2003 [56] | France | NA | Prospective | Multi-centre | NA | H | 59 | 156 | 156 | 0 | (32–92) | 66.2 ± 12.8 | 550M:144F 5 | - | - | x | x | x | Dysuria; pollakiuria; cystitis; cystalgia; other condition | uCyt+ |
| uCyt+ (+) Cytology | ||||||||||||||||||||
| Poulakis et al. 2001 [57] | NA | NA | Prospective | NA | NA | U | 406 | 333 | 212 | 121 | (67–90) | 66.7 | 485M:254F | - | 386 with previous bladder carcinoma 4 | x | - | - | NMP-22 | |
| BTAstat | ||||||||||||||||||||
| Saad et al. 2002 [58] | UK | NA | Prospective | Single centre | NA | H | 52 | 68 | 53 | 15 | (30–88) | 69.5 ± 11.1 | 100M:20F | - | - | - | - | x | Benign prostatic hyperplasia; urethral strictures; renal stone; cystodistension; 12 prostate cancer; 2 renal cell carcinoma | BTAstat |
| NMP-22 | ||||||||||||||||||||
| Sajid et al. 2020 [59] | Pakistan | 2018–2019 | NA | Single centre | Cross-sectional | H | 215 | 165 | - | - | (24–75) | 53.08 ± 12.41 | 300M:80F | - | - | - | - | - | - | NMP-22 |
| NMP-22 + Cytology | ||||||||||||||||||||
| Sanchez-Carbayo et al. 2000 [60] | Spain | NA | Prospective | Single centre | NA | H | 52 | 137 | 45 | 32 | - | - | 311M:90F 5 | - | - | - | x | x | Benign diseases; lithiasis; Stenosis; benign prostate hyperplasia | BTF |
| BTF normalised | ||||||||||||||||||||
| CK18 | ||||||||||||||||||||
| CK18 normalised | ||||||||||||||||||||
| Sarosdy et al. 2006 [61] | NA | NA | Prospective | Multi-centre | Trial | U | 51 | 422 | - | - | (40–97) | 63 | 298M:199F 6 | 265 Current or former: 207 Never: 1 Unknown | 440 White; 26 Black; 15 Hispanic; 4 Asian; 12 Other race 6 | x | - | Inflammation or infection; benign prostatic hyperplasia; stones; urethral stricture; bladder polyp | UroVysion | |
| Shang et al. 2021 [62] | China | 2020–2021 | Prospective | Single centre | NA | H | 128 | 136 | 136 | 0 | C (32–89) Con (35–84) | C (67.5 ± 10.2) Con (68.9 ± 13) | 190M:74F | - | - | x | - | Irritative bladder symptoms, abdominal pain, hydronephrosis on the affected side | UroVysion | |
| Todenhöfer et al. 2013 [63] | Germany | NA | NA | Single centre | Cohort | U | 115 | 693 | - | - | (21–92) | median:67 | 645M:163F | - | - | x | x | Irritative voiding symptoms | UroVysion | |
| uCyt+ | ||||||||||||||||||||
| NMP-22 | ||||||||||||||||||||
| UroVysion + uCyt+ | ||||||||||||||||||||
| UroVysion + NMP-22 | ||||||||||||||||||||
| uCyt+ (+) NMP-22 | ||||||||||||||||||||
| UroVysion + uCyt+ (+) NMP-22 | ||||||||||||||||||||
| UroVysion + Cytology | ||||||||||||||||||||
| uCyt+ (+) Cytology | ||||||||||||||||||||
| NMP-22 + Cytology | ||||||||||||||||||||
| uCyt+ (+) UroVysion + Cytology | ||||||||||||||||||||
| UroVysion + NMP-22+ Cytology | ||||||||||||||||||||
| uCyt+ (+) NMP-22 + Cytology | ||||||||||||||||||||
| UroVysion + uCyt+ (+) NMP22+ Cytology | ||||||||||||||||||||
| Base model (age and grade of haematuria) + UroVysion | ||||||||||||||||||||
| Base model (age and grade of haematuria) + UroVysion + Cytology | ||||||||||||||||||||
| Base model (age and grade of haematuria) + UroVysion + uCyt+ | ||||||||||||||||||||
| Base model (age and grade of haematuria) + UroVysion + uCyt+ (+) Cytology) | ||||||||||||||||||||
| Todenhöfer et al. 2013 [64] | Germany | 2004–2009 | NA | Single centre | Cohort | U | 502 | 1611 | 1611 | 0 | (23–96) | median:66 | 1599M:514F | - | - | - | - | x | - | UroVysion |
| uCyt+ | ||||||||||||||||||||
| NMP-22 | ||||||||||||||||||||
| Todenhöfer et al. 2013 [65] | Germany | 2004–2009 | Retrospective | Single centre | Cohort | U | 543 | 1822 | - | - | (18–97) | median:65 | 1776M:589F | - | - | x | - | Irritative voiding symptoms | UroVysion | |
| uCyt+ | ||||||||||||||||||||
| NMP-22 | ||||||||||||||||||||
| van Kessel et al. 2016 [66] | The Netherlands | 2006–2013 | Prospective | Single centre | Cohort | H | 74 | 80 | 80 | 0 | C (38–91) Con (21–86) | C 68 Con 58 | 109M:45F | - | - | x | - | - | FGFR3 | |
| TERT | ||||||||||||||||||||
| FGFR3, TERT, HRAS | ||||||||||||||||||||
| TWIST1 | ||||||||||||||||||||
| OTX1 probe 1 | ||||||||||||||||||||
| OTX1 probe 2 | ||||||||||||||||||||
| OTX1 probe 3 | ||||||||||||||||||||
| OTX1 probe 4 | ||||||||||||||||||||
| ONECUT 2 probe 1 | ||||||||||||||||||||
| ONECUT 2 probe 2 | ||||||||||||||||||||
| ONECUT 2 probe 3 | ||||||||||||||||||||
| ONECUT 2 probe 4 | ||||||||||||||||||||
| ONECUT 2 probe 5 | ||||||||||||||||||||
| OTX1 all combined | ||||||||||||||||||||
| ONECUT2 all combined | ||||||||||||||||||||
| ONECUT probes 1 + 4 | ||||||||||||||||||||
| Optimal (age, FGFR3, TERT, HRAS, ONECUT2 probes 1 + 4, OTX1 probe 2, Twist) | ||||||||||||||||||||
| van Kessel et al. 2017 [67] | Sweden, Spain, The Netherlands | NA | Prospective | Multi-centre | Cohort | H | 97 | 103 | 103 | 0 | C (38–110) Con (50–82) | C 71 Con 62 | 181M:19F | - | - | x | - | - | FGFR3, TERT, HRAS and OTX1, ONECUT2, TWIST1 | |
| van Kessel et al. 2020 [68] | The Netherlands | 2015–2017 | Prospective | Multi-centre | Cohort | H | 112 | 726 | - | - | (19–96) | median:66 | 485M:353F | 221 Current: 185 Former: 258 Never: 174 Not reported | - | x | x | - | - | FGFR3, TERT, Harvey HRAS and OTX1, ONECUT2, TWIST1 |
| Extended Model consisting of: Existing model (univariate analysis incl. age, mutation, methylation) + type of haematuria + gender | ||||||||||||||||||||
| Optimal model consisting of: Existing model (univariate analysis incl. age, mutation, methylation) + type of haematuria | ||||||||||||||||||||
| van Valenberg et al. 2021 [2] | USA | 2015 | Prospective | Multi-centre | Cohort | U | 59 | 769 | - | - | (23–84) | 65 ± 13 | 467M:361F | 139 Current: 288 Former: 401 Never | 698 Caucasian; 80 Black; 32 Hispanic; 18 Other | x | x | - | - | Xpert |
| UroVysion | ||||||||||||||||||||
| Virk et al. 2017 [69] | USA | 2008–2014 | Retrospective | Single centre | Cohort | H | 181 | 196 | 196 | 0 | (24–93) | mean & median: 67 | 259M:118F | - | - | x | - | Other Symptoms; miscellaneous indications | UroVysion | |
| Ward et al. 2022 [70] | UK | NA | Prospective | Multi-centre | NA | H | 68 | 147 | - | - | - | median: C 72.5: Con 60 | 137M:78F | - | - | - | - | - | Calculi, benign prostatic hyperplasia, cystitis, inflammation, prostate cancer, and kidney cancer | TERT (promoter), FGFR3, PIK3CA, TP53, ERCC2, RHOB, ERBB2, HRAS, RXRA, ELF3, CDKN1A, KRAS, KDM6A, AKT1, FBXW7, ERBB3, SF3B1, CTNNB1, BRAF, C3orf70, CREBBP, CDKN2A, and NRAS |
| Wu et al. 2020 [71] | China | 2015–2016 | Prospective | Single centre | Case-control | H | 53 | 58 | 58 | 0 | C (61.5–74): Con (48–63.3) | median: C 68: Con 55.5 | 83M:28F | - | - | x | x | Urinary calculi; benign prostatic hyperplasia | HOXA9 | |
| PCDH17 | ||||||||||||||||||||
| POU4F2 | ||||||||||||||||||||
| ONECUT2 | ||||||||||||||||||||
| HOXA9 + PCDH17 + POU4F2 + ONECUT2 | ||||||||||||||||||||
| Zhou et al. 2019 [72] | China | 2007–2008 | Prospective | Multi-centre | Trial | H | 3640 | 319 | (15–97) | 63.04 ± 13.31 | 3021M:938F | - | - | x | - | - | Inflammation; Renal tumor; benign bladder tumor; bladder tumor with non-transitional cell origin 3 | UroVysion | ||
| No | Biomarker/Test | Biomarker Category | Description | Study | Test Platform | Report | Sample Source | Threshold Used (Where Available/Appropriate) | Performance Measures Reported | Included in Meta-Analysis | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Proteins | mRNA | DNA | Individual Markers | Multiple Markers | Urine | Serum | ||||||||
| INDIVIDUAL MARKERS | ||||||||||||||
| 1 | ADXBLADDER/Mcm5 | x | Protein expression of Minichromosome Maintenance protein 5 | [37] | ELISA 1 | x | x | SN, SP, NPV, AUC, Accuracy, FP, FN | No | |||||
| [51] | Immunofluorometric Assay | x | x | 2150-cell;8500-cell | SN, SP, PPV, NPV | No | ||||||||
| 2 | ANG | x | Protein expression of Angiogenin | [41] | ELISA | x | x | 425 pg/mg | SN, SP, PPV, NPV, Accuracy | No | ||||
| 3 | BCL2 | x | Methylation of BCL2 gene | [34] | qPCR 2 | x | x | SN, SP, PPV, NPV | No | |||||
| 4 | bFGF | x | Protein expression of Basic Fibroblast Growth Factor | [41] | ELISA | x | 19,444 fmol/mg | SN, SP, PPV, NPV, Accuracy | No | |||||
| 5 | BTAstat | x | Protein expression of Complement factor H-related protein | [32] | Lateral Flow Test | x | x | SN, SP, FP | Yes | |||||
| [57] | Lateral Flow Test | x | x | SN, SP, PPV, NPV, Accuracy | ||||||||||
| [58] | Lateral Flow Test | x | x | SN, SP, PPV, Accuracy, FP, FN | ||||||||||
| 6 | BTF | x | Protein expression of Bladder Tumour Fibronectin | [60] | Chemiluminescence Immunoassay | x | x | 52.8 µg/L | SN, SP, PPV, NPV, Accuracy | No | ||||
| 77 µg/g (when normalising with urine CREA) | ||||||||||||||
| 7 | CCNA1 | x | Methylation of CCNA1 gene | [34] | qPCR | x | x | SN, SP, PPV, NPV | No | |||||
| 8 | CK18 | x | Protein expression of Cytokeratin 18 | [60] | Chemiluminescence Immunoassay | x | x | 7.4 µg/L | SN, SP, PPV, NPV, Accuracy | No | ||||
| 7 µg/g (when normalising with urine CREA) | ||||||||||||||
| 9 | CK20 | x | mRNA expression of Cytokeratin 20 | [43] | RT-PCR 3 | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 10 | CYFRA21-1 | x | Protein expression of Cytokeratin 19 fragments | [47] | Chemiluminescence Immunoassay | x | x | 2.28 ng/mL | SN, SP, AUC | No | ||||
| x | 62.74 ng/mL | SN, SP, AUC | ||||||||||||
| x | x | 0.66 ng/mL | SN, SP, AUC | |||||||||||
| 11 | EMA | x | Protein expression of Epithelial Membrane Antigen | [30] | ELISA | x | x | 1.8 Ug/mL | SN, SP, PPV, NPV, AUC, Efficiency | No | ||||
| 12 | EOMES | x | Methylation of EOMES gene | [34] | qPCR | x | x | SN, SP, PPV, NPV | No | |||||
| 13 | FGFR3 | x | Mutation of FGFR3 gene | ddPCR 4 | x | x | 3 | SN, SP, PPV, NPV | ||||||
| [50] | qPCR | x | x | “negative” | SN, SP, NPV | |||||||||
| [66] | SNaPshot assay | x | x | SN, SP, Accuracy, FP, FN | ||||||||||
| 14 | FN | x | Protein expression of Fibronectin | [43] | ELISA | x | x | 41.7 ng/mg | SN, SP, PPV, NPV, Accuracy | No | ||||
| 15 | HGF | x | Protein expression of Hepatocyte Growth Factor | [41] | ELISA | x | x | 1820 pg/mg | SN, SP, PPV, NPV, Accuracy | No | ||||
| 16 | HOXA9 | x | Methylation of HOXA9 gene | [71] | High Resolution Melting | x | x | SN, SP, PPV, NPV | No | |||||
| 17 | HURP | x | mRNA expression of Hepatoma Up-regulated Protein | [45] | RT-PCR | x | x | 0.0132 | SN, SP, PPV, NPV | No | ||||
| [46] | RT-PCR & AuNP 5 assay | x | x | SN, SP, PPV, NPV, Accuracy, FP, FN | ||||||||||
| 18 | HYAL-1 | x | Hyaluronidase 1 activity | [44] | Zymography | x | x | 13.8 µU/mg | SN, SP, PPV, NPV, AUC, Accuracy | No | ||||
| x | mRNA expression of Hyaluronidase 1 (Qual/Semi-quant) | [42] | RT-PCR | x | x | 0.25 (Qual) | SN, SP, PPV, NPV, Accuracy | |||||||
| 19 | MMP-2 | x | Protein expression of Matrix metalloproteinase 2 | [39] | ELISA | x | x | 1.9 ng/mg | SN, SP | No | ||||
| 20 | MMP-9 | x | Protein expression of Matrix metalloproteinase 9 | ELISA | x | x | 8.7 ng/mg | SN, SP | No | |||||
| 21 | NMP-22 | x | Protein expression of Nuclear Matrix Protein 22 | [48] | Lateral Flow Test (BladderChek) | x | x | 10 IU/mL | SN, SP, PPV, NPV | Yes | ||||
| [54] | Lateral Flow Test (BladderChek) | x | x | SN, SP | ||||||||||
| [59] | Lateral Flow Test (BladderChek) | x | x | SN, SP, PPV, NPV, AUC, Accuracy, FP, FN | ||||||||||
| [32] | ELISA | x | x | 3.6 IU/mL | SN, SP, FP | |||||||||
| [49] | ELISA | x | x | 10 IU/mL | SN, SP, Accuracy, FP | |||||||||
| [51] | ELISA | x | x | 10 IU/mL | SN, SP, PPV, NPV, AUC, Accuracy | |||||||||
| [54] | ELISA | x | x | 7.5 IU/mL | SN, SP, AUC | |||||||||
| [55] | ELISA | x | x | 7.5 IU/mL | SN | |||||||||
| [57] | ELISA | x | x | 8.25 IU/mL | SN, SP, PPV, NPV, Accuracy | |||||||||
| [63] | ELISA | x | x | ≥10 IU/mL | SN, SP, PPV, NPV, AUC | |||||||||
| [64] | ELISA | x | x | ≥10 IU/mL | SN, SP | |||||||||
| [65] | ELISA | x | x | ≥10 IU/mL | SN, SP | |||||||||
| [58] | Unclear | x | x | ≥10 IU/mL | SN, SP, PPV, Accuracy, FP, FN | |||||||||
| 22 | NMP-52 | x | Protein expression of Nuclear Matrix Protein 52 | [30] | ELISA | x | x | 2.8 Ug/mL | SN, SP, PPV, NPV, AUC, Efficiency | No | ||||
| 23 | OTX1 | x | Methylation of OTX1 gene (probe 1/probe 2/probe 3/probe 4/all combined) | [66] | SNaPshot assay | x | x | SN, SP, AUC | No | |||||
| 24 | ONECUT2 | x | Methylation of ONECUT2 gene | [34] | qPCR | x | x | SN, SP, PPV, NPV | No | |||||
| [71] | High Resolution Melting | x | x | SN, SP, PPV, NPV | No | |||||||||
| Methylation of ONECUT2 gene (probe 1/probe 2/probe 3/probe 4/probe 5/probe 1 + 4/all combined) | [66] | SNaPshot assay | x | x | SN, SP, AUC | No | ||||||||
| 25 | PCDH17 | x | Methylation of PCDH17 gene | [71] | High Resolution Melting | x | x | SN, SP, PPV, NPV | No | |||||
| 26 | POU4F2 | x | Methylation of POU4F2 gene | High Resolution Melting | x | x | SN, SP, PPV, NPV | No | ||||||
| 27 | RAB-B2 | x | Methylation of RAB-B2 gene | [44] | PCR | x | x | 0.065 | SN, SP, PPV, NPV, AUC, Accuracy | No | ||||
| 28 | SALL3 | x | Methylation of SALL3 gene | [34] | qPCR | x | x | 0.5 | SN, SP, PPV, NPV | No | ||||
| 29 | SNCG | x | Protein expression of Gamma-Synuclein | [52] | ELISA | x | 1.874 ng/mL | SN, SP, PPV, NPV, AUC, Accuracy | No | |||||
| 30 | SPARC | x | Protein expression of Secreted Protein Acidic and Rich in Cysteine | [33] | ELISA | x | x | >0 ng/mL−1 | SN, SP, PPV, NPV, AUC | No | ||||
| 31 | Survivin | x | mRNA expression of Survivin (Qual/Semi-quant) | [42] | RT-PCR | x | x | 0.25 (Qual) | SN, SP, PPV, NPV, Accuracy | No | ||||
| 32 | Telomerase (TERT; hRT; hTERT; RTA) | x | Mutation of TERT gene | [34] | ddPCR | x | x | 5 (TERT C250T)/3 (TERT C228T) | SN, SP, PPV, NPV | No | ||||
| [66] | SNaPshot assay | x | x | SN, SP, AUC | ||||||||||
| x | mRNA expression of Telomerase (hRT/hTERT) | [38] | RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy, FP, FN | No | |||||||
| x | Telomerase activity (RTA) | qPCR | x | x | 18.08 copies per 2µl | SN, SP, PPV, NPV, AUC, Accuracy, FP, FN | ||||||||
| TRAP 6 assay | x | x | 0.046 | SN, SP, PPV, NPV, AUC, Accuracy, FP, FN | ||||||||||
| Telomerase activity | [43] | TRAP assay | x | SN, SP, PPV, NPV, Accuracy | No | |||||||||
| [32] | TRAP assay | x | x | SN, SP, FP | ||||||||||
| 33 | TGF-β1 | x | Protein expression of Transforming Growth Factor Beta 1 | [40] | ELISA | x | 25 pg/mg | SN, SP, PPV, NPV, AUC, Accuracy | No | |||||
| 34 | TIMP-2 | x | Protein expression of Tissue Inhibitor of Metalloproteinase 2 | [39] | ELISA | x | x | 4.49 ng/mg | SN, SP | No | ||||
| 35 | TWIST1 | x | Methylation of TWIST1 gene | [66] | qPCR | x | x | SN, SP, AUC | No | |||||
| 36 | VEGF | x | Protein expression of Vascular Endothelial Growth Factor | [40] | ELISA | x | x | 38 pg/mg | SN, SP, PPV, NPV, AUC, Accuracy | No | ||||
| [41] | ELISA | x | x | 52ng/mg | SN, SP, AUC, FP, FN | No | ||||||||
| 37 | VIM | x | Methylation of VIM gene | [34] | qPCR | x | x | 2 | SN, SP, PPV, NPV | No | ||||
| MULTIPLE MARKERS | ||||||||||||||
| 1 | CCNA1 + ONECUT2 + BCL2 + EOMES + SALL3 + VIM | x | Methylation of CCNA1, ONECUT2, BCL2, EOMES, SALL3 and VIM genes | [34] | qPCR | x | x | SN, SP | No | |||||
| 2 | CK20 + RTA | x | x | mRNA expression of Cytokeratin 20 + telomerase activity | [43] | RT-PCR + TRAP assay | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||
| 3 | CK20 + FN + RTA | x | x | mRNA expression of Cytokeratin 20 + protein expression of Fibronectin + telomerase activity | RT-PCR + ELISA + TRAP assay | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 4 | CxBladder | x | mRNA expression of CDK1, HOXA13, MDK, IGFBP5 and CXCR2 genes | [35] | qPCR | x | x | <4 | SN, SP, NPV, Accuracy | No | ||||
| [54] | predefined as the classifier scores which gave 85% to 90% SP in this cohort | SN, SP, AUC | ||||||||||||
| 5 | EMA + NMP-52 | x | Protein expression of Epithelial Membrane Antigen and Nuclear matrix protein 52 | [30] | ELISA | x | x | 4.0 Ug/mL | SN, SP, PPV, NPV, AUC, Efficiency | No | ||||
| 6 | FGFR3, TERT, HRAS | x | Mutation of FGFR3, TERT and HRAS genes | [66] | SNaPshot assay | x | x | SN, SP, AUC | No | |||||
| 7 | FGFR3, TERT, HRAS and OTX1, ONECUT2, TWIST1 | x | Mutation of FGFR3, TERT and HRAS genes and methylation of OTX1, ONECUT2 and TWIST1 genes | [67] | SNaPshot assay and qPCR | x | x | 0.1917196 | SN, SP | No | ||||
| [68] | SNaPshot assay and qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||||
| 8 | HOXA9 + PCDH17 + POU4F2 + ONECUT2 | x | Methylation of HOXA9, PCDH17, POU4F2 and ONECUT2 gene | [71] | High Resolution Melting | x | SN, SP, PPV, NPV, AUC | No | ||||||
| 9 | HYAL-1 + Survivin | x | mRNA expression of Hyaluronidase 1 + Survivin (Qual/Semi-quant) | [42] | RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 10 | MADR Assay | x | x | Methylation of TWIST1 and NID2 genes, mutation of FGFR3 gene and protein expression of matrix metalloproteinase 2 | [50] | PCR + qPCR + ELISA | x | x | TWIST1 < 139K; NID2 < 680; MMP-2 < 1.100 ng/mL; FGF3 negative | SN, SP, NPV | No | |||
| 11 | Mcm5 + NMP-22 | x | Protein expression of Minichromosome Maintenance protein 5 and Nuclear Matrix Protein 22 | [51] | Immunofluorometric Assay + ELISA | x | x | 4200-cell; 2800-cell; 1900-cell; 1000-cell + 10 IU/mL | SN, SP | No | ||||
| 12 | MMP-2 + TIMP-2 | x | Protein expression of Matrix metalloproteinase 2 + Tissue inhibitor of metalloproteinase 2 | [39] | ELISA | x | x | 0.93 ng/mg | SN, SP | No | ||||
| 13 | MMP-9 + TIMP-2 | x | Protein expression of Matrix metalloproteinase 9 + Tissue inhibitor of metalloproteinase 2 | [39] | ELISA | x | x | 3.81 ng/mg | SN, SP | No | ||||
| 14 | MMP-2/MMP-9 | x | MMP-2/MMP-9 activity | [39] | Zymography | x | x | SN, SP | No | |||||
| 15 | RAB-B2 + HYAL-1 | x | x | Methylation of RAB-B2 + Hyaluronidase 1 activity | [44] | PCR + Zymography | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||
| 16 | Telomerase (RTA + hRT; RTA + hTERT; hTR + hTERT; RTA + hRT + hTERT) | x | x | Telomerase activity (RTA) + telomerase mRNA expression (hRT) | [38] | TRAP assay + RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||
| Telomerase activity (RTA) + telomerase mRNA expression (hTERT) | TRAP assay + qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||||
| x | Telomerase mRNA expression (hTR + hTERT) | RT-PCR + qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||||||
| x | x | Telomerase activity (RTA) + telomerase mRNA expression (hTR + hTERT) | TRAP assay + RT-PCR + qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||
| 17 | TERT (promoter), FGFR3, PIK3CA, TP53, ERCC2, RHOB, ERBB2, HRAS, RXRA, ELF3, CDKN1A, KRAS, KDM6A, AKT1, FBXW7, ERBB3, SF3B1, CTNNB1, BRAF, C3orf70, CREBBP, CDKN2A, and NRAS | x | Mutation of TERT (promoter), FGFR3, PIK3CA, TP53, ERCC2, RHOB, ERBB2, HRAS, RXRA, ELF3, CDKN1A, KRAS, KDM6A, AKT1, FBXW7, ERBB3, SF3B1, CTNNB1, BRAF, C3orf70, CREBBP, CDKN2A, and NRAS | [70] | NGS 7 | x | x | a positive test was defined as detection of any one of the 443 mutations in a cpDNA sample at >0.9% VAF for chr5:129528A/G or >0.5% VAF for all other coordinates. | SN, SP | No | ||||
| 18 | TERT, FGFR3, SALL3, ONECUT2, CCNA1, BCL2, EOMES, and VIM | x | Mutation of TERT and FGFR3 genes plus methylation of SALL3, ONECUT2, CCNA1, BCL2, EOMES, and VIM genes | [34] | ddPCR/qPCR | x | x | SN, SP, PPV, NPV, AUC | No | |||||
| 19 | TERT + ONECUT2 | x | Mutation of TERT gene plus methylation of ONECUT2 genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 20 | TERT + FGFR3 | x | Mutation of TERT and FGFR3 genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 21 | TERT + FGFR3 + CCNA1 | x | Mutation of TERT and FGFR3 genes plus methylation of CCNA1 genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 22 | TERT + FGFR3 + CCNA1 + ONECUT2 | x | Mutation of TERT and FGFR3 genes plus methylation of CCNA1 and ONECUT2 genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 23 | TERT + FGFR3 + CCNA1+ ONECUT2 + BCL2 | x | Mutation of TERT and FGFR3 genes plus methylation of CCNA1, ONECUT2 and BCL2 genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 24 | TERT + FGFR3 + CCNA1 + ONECUT2 + BCL2 + EOMES | x | Mutation of TERT and FGFR3 genes plus methylation of CCNA1, ONECUT2, BCL2 and EOMES genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 25 | TERT + FGFR3 + CCNA1 + ONECUT2 + BCL2 + EOMES + SALL3 | x | Mutation of TERT and FGFR3 genes plus methylation of CCNA1, ONECUT2, BCL2, EOMES and SALL3 genes | ddPCR/qPCR | x | x | SN, SP | No | ||||||
| 26 | TGF-β1 + VEGF | x | Protein expression of Transforming growth factor beta 1 + Vascular endothelial growth factor | [40] | ELISA | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 27 | uCyt+9 | x | Protein expression of Carcinoembryonic antigen and sulphate mucin glycoproteins | [36] | Immunofluorescence | x | x | SN, SP, FP, FN | Yes | |||||
| [49] | Immunofluorescence | x | x | at least 1 clear positive cell | SN, SP, Accuracy, FP | |||||||||
| [56] | Immunofluorescence | x | x | SN, SP, FP | ||||||||||
| [63] | Immunofluorescence | x | x | at least 1 clear positive cell | SN, SP, PPV, NPV, AUC | |||||||||
| [64] | Immunofluorescence | x | x | at least 1 clear positive cell | SN, SP | |||||||||
| [65] | Immunofluorescence | x | x | at least 1 clear positive cell | SN, SP, Accuracy, FP, FN | |||||||||
| 28 | uCyt+ (+) NMP-22 | x | Protein expression of Carcinoembryonic antigen and Sulphate mucin glycoproteins and nuclear matrix protein 22 | [63] | Immunofluorescence + ELISA | x | x | uCyt+ => 1 clear positive cell/NMP22 = > 10 IU/mL | SN, SP, PPV, NPV, AUC | No | ||||
| 29 | uRNA-D | x | mRNA expression of CDC2, HOXA13, MDK and IGFBP5 genes | [54] | qPCR | x | x | predefined as the classifier scores which gave 85% SP in this cohort | SN, SP, AUC | No | ||||
| 30 | UroVysion | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 | [49] | FISH 8 | x | x | SN, SP, Accuracy, FP | Yes | |||||
| [53] | FISH | x | x | SN, SP | ||||||||||
| [61] | FISH | x | x | SN, SP, PPV, NPV, Accuracy | ||||||||||
| [62] | FISH | x | x | SN, SP | ||||||||||
| [63] | FISH | x | x | SN, SP, PPV, NPV, AUC | ||||||||||
| [64] | FISH | x | x | SN, SP | ||||||||||
| [65] | FISH | x | x | SN. SP, | ||||||||||
| [2] | FISH | x | x | SN, SP, PPV, NPV, Accuracy | ||||||||||
| [69] | FISH | x | x | SN, SP, PPV, NPV, Accuracy | ||||||||||
| [72] | FISH | x | x | SN, SP, PPV, NPV, AUC, FP, FN | ||||||||||
| 31 | UroVysion + uCyt+ | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen and Sulphate mucin glycoproteins | [63] | FISH + Immunofluorescence | x | x | SN, SP, PPV, NPV, AUC | No | ||||
| 32 | UroVysion + NMP-22 | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of nuclear matrix protein 22 | [63] | FISH + ELISA | x | x | NMP-22 => ≥10IU/mL | SN, SP, PPV, NPV, AUC | No | |||
| 33 | UroVysion + uCyt+ (+) NMP-22 | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen and Sulphate mucin glycoproteins and nuclear matrix protein 22 | [63] | FISH + Immunofluorescence + ELISA | x | x | SN, SP, PPV, NPV, AUC | No | ||||
| 34 | Xpert | x | mRNA expression of ABL1, CRH, IGF2, UPK1B and ANXA10 | [2] | qPCR | x | x | SN, SP, PPV, NPV, AUC, Accuracy | No | |||||
| BIOMARKER/TESTS and CYTOLOGY | ||||||||||||||
| 1 | CK20 + Cytology | x | mRNA expression of Cytokeratin 20 + Cytology | [43] | RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 2 | CK20 + RTA + Cytology | x | x | mRNA expression of Cytokeratin 20 + telomerase activity + Cytology | RT-PCR + TRAP assay | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 3 | FGFR3 + Cytology | x | Mutation of FGFR3 gene + Cytology | [50] | qPCR | x | x | SN, SP, PPV | No | |||||
| 4 | FN + Cytology | x | Protein expression of Fibronectin + Cytology | [43] | ELISA | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 5 | FN + CK20 + Cytology | x | x | Protein expression of Fibronectin + mRNA expression of Cytokeratin 20 + Cytology | ELISA + RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 6 | FN + CK20 + RTA + Cytology | x | x | Protein expression of Fibronectin + mRNA expression of Cytokeratin 20 + telomerase activity + Cytology | ELISA + RT-PCR + TRAP assay | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 7 | HURP + Cytology | x | mRNA expression of Hepatoma Up-regulated Protein + Cytology | [45] | RT-PCR | x | x | 0.0132 | SN, SP, PPV, NPV, Accuracy | No | ||||
| [46] | RT-PCR & AuNP assay | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||||
| 9 | HYAL-1 + Cytology | x | mRNA expression of Hyaluronidase 1 + Cytology (Qual/Semi-quant) | [42] | RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| x | Hyaluronidase activity + Cytology | [44] | Zymography | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||
| 10 | HYAL-1 + Survivin + Cytology | x | mRNA expression of Hyaluronidase 1 and Survivin + Cytology (Qual/Semi-quant) | [42] | RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 11 | MMP-2 and MMP-9 zymography + Cytology | x | Activity of Matrix metalloproteinase 2 and Matrix metalloproteinase 9 + Cytology | [39] | Zymography | x | x | SN, SP | No | |||||
| 12 | MMP-2 + Cytology | x | Protein expression of Matrix metalloproteinase 2 + Cytology | ELISA | x | x | 1.9 ng/mg | SN, SP | No | |||||
| 13 | MMP-9 + Cytology | x | Protein expression of Matrix metalloproteinase 9 + Cytology | ELISA | x | x | 8.7 ng/mg | SN, SP | No | |||||
| 14 | MMP-2 + TIMP-2 ratio + Cytology | x | Protein expression of Matrix metalloproteinase 2 and Tissue inhibitor of metalloproteinase 2 + Cytology | ELISA | x | x | 0.93 ng/mg | SN, SP | No | |||||
| 15 | MMP-9 + TIMP-2 ratio + Cytology | x | Protein expression of Matrix metalloproteinase 9 + Tissue inhibitor of metalloproteinase 2 + Cytology | ELISA | x | x | 3.81 ng/mg | SN, SP | No | |||||
| 16 | NMP-22 + Cytology | x | Protein expression of Nuclear Matrix Protein 22 + Cytology | [59] | Lateral Flow Test (BladderChek) | x | x | SN, SP, PPV, NPV, AUC, Accuracy, FP, FN | No | |||||
| [63] | ELISA | x | x | ≥10 IU/mL | SN, SP, PPV, NPV, AUC | No | ||||||||
| 17 | RAB-B2 + Cytology | x | Methylation of RAB-B2 gene + Cytology | [44] | PCR | x | x | 0.065 | SN, SP, PPV, NPV, Accuracy | No | ||||
| 18 | RAB-B2 + HYAL-1 + Cytology | x | x | Methylation of RAB-B2 gene + Hyaluronidase activity + Cytology | PCR + Zymography | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 19 | Survivin + Cytology | x | mRNA expression of Survivin + Cytology | [42] | RT- PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 20 | Telomerase + Cytology (RTA + Cytology; hRT + Cytology; hTERT + Cytology; RTA + hRT + Cytology; RTA + hTERT + Cytology; hTR + hTERT + Cytology; RTA + hRT + HTERT + Cytology) | x | Telomerase activity (RTA) + Cytology | [38] | TRAP assay | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| [43] | TRAP assay | x | SN, SP, PPV, NPV, Accuracy | No | ||||||||||
| x | mRNA expression of Telomerase (hRT/hTERT) + Cytology | [38] | RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||
| qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||||||||
| x | x | Telomerase activity (RTA) + mRNA expression of Telomerase (hRT/hTERT) + Cytology | TRAP assay + RT-PCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||
| TRAP assay + qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||||||||
| x | mRNA expression of Telomerase (hTR + hTERT) + Cytology | RT-PCR + qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||||||
| x | x | Telomerase activity (RTA) + mRNA expression of Telomerase (hTR + hTERT) + Cytology | TRAP assay + RT-PCR + qPCR | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||||
| 21 | TGF-β1 + Cytology | x | Protein expression of Transforming Growth Factor Beta 1 + Cytology | [40] | ELISA | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| 22 | TGF-β1 + VEGF + Cytology | x | Protein expression of Transforming Growth Factor Beta 1 + Vascular Endothelial Growth Factor + Cytology | ELISA | x | x | SN, SP, PPV, NPV, Accuracy | No | ||||||
| 23 | TIMP-2 + Cytology | x | Protein expression of Tissue inhibitor of metalloproteinase 2 + Cytology | [39] | ELISA | x | x | 4.49 ng/mg | SN, SP | No | ||||
| 24 | uCyt+ + Cytology | x | Protein expression of Carcinoembryonic Antigen and Sulphate Mucin Glycoproteins + Cytology | [56] | Immunofluorescence | x | x | SN | No | |||||
| [63] | Immunofluorescence | x | x | SN, SP, PPV, NPV, AUC | No | |||||||||
| 25 | uCyt+ (+) NMP-22 + Cytology | x | Protein expression of Carcinoembryonic antigen, Sulphate mucin glycoproteins and Nuclear matrix protein 22 + Cytology | Immunofluorescence + ELISA | x | x | SN, SP, PPV, NPV, AUC | No | ||||||
| 26 | UroVysion + Cytology | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 | FISH | x | x | SN, SP, PPV, NPV, AUC | No | ||||||
| 27 | UroVysion + uCyt+ (+) Cytology | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen and sulphate mucin glycoproteins + Cytology | FISH + Immunofluorescence | x | x | SN, SP, PPV, NPV, AUC | No | |||||
| 28 | UroVysion + NMP-22 + Cytology | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of nuclear matrix protein 22 + Cytology | FISH + ELISA | x | x | SN, SP, PPV, NPV, AUC | No | |||||
| 29 | UroVysion + uCyt+ (+) NMP-22 + Cytology | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen, Sulphate mucin glycoproteins and nuclear matrix protein 22 + Cytology | FISH + Immunofluorescence + ELISA | x | x | SN, SP, PPV, NPV, AUC | No | |||||
| 30 | VEGF + Cytology | x | protein expression of Vascular endothelial growth factor + Cytology | [40] | ELISA | x | x | SN, SP, PPV, NPV, Accuracy | No | |||||
| BIOMARKER/TESTS and PREDICTION MODELS | ||||||||||||||
| 1 | Base model (age and grade of haematuria) + UroVysion | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 | [63] | FISH | x | AUC | No | ||||||
| 2 | Base model (age and grade of haematuria) + UroVysion + uCyt+ | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen and Sulphate mucin glycoproteins | FISH + Immunofluorescence | x | AUC | No | ||||||
| 3 | Base model (age and grade of haematuria) + UroVysion + Cytology | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen and Sulphate mucin glycoproteins | Immunofluorescence | x | AUC | No | |||||||
| 4 | Optimal (age + FGFR3, TERT, HRAS, ONECUT2 probes 1 + 4, OTX1 probe 2, TWIST) | x | Methylation of ONECUT2 and OXT1 genes and mutation of FGFR3, TERT and HRAS genes | [66] | SNaPshot assay | x | x | Various cut-offs: 0.1213372; 0.1917196; 0.3547327; 0.4975214 | SN, SP, PPV, NPV | No | ||||
| 5 | Extended Model consisting of: Existing model (univariate analysis incl. age, mutation, methylation) + type of haematuria + gender | x | Mutation of FGFR3, TERT and HRAS and methylation of OTX1, ONECUT2 and TWIST1 | [68] | SNaPshot assay and qPCR | x | x | AUC | No | |||||
| 6 | Optimal model consisting of: Existing model (univariate analysis incl. age, mutation, methylation) + type of haematuria | x | Mutation of FGFR3, TERT and HRAS and methylation of OTX1, ONECUT2 and TWIST2 | SNaPshot assay and qPCR | x | x | SN, SP, PPV, NPV, AUC, FP, FN | No | ||||||
| BIOMARKER/TESTS, PREDICTION MODELS and CYTOLOGY | ||||||||||||||
| 1 | Base model (age, gender, smoker, race, haematuria) + NMP-22 | x | Protein expression of Nuclear Matrix Protein 22 | [31] | Lateral Flow Test (BladderChek) | x | x | AUC, Accuracy | No | |||||
| 2 | Base model (age, gender, smoker, race, haematuria) + NMP-22+ Cytology | x | Protein expression of Nuclear Matrix Protein 22 + Cytology | Lateral Flow Test (BladderChek) | x | x | AUC, Accuracy | No | ||||||
| 3 | Base model (age, gender, smoker, race, haematuria) + UroVysion + uCyt+ (+) Cytology | x | x | Aneuploidy of Chromosomes 3, 7 and 17 and loss of chromosome locus 9p21 + protein expression of Carcinoembryonic antigen and sulphate mucin glycoproteins + Cytology | [63] | FISH + Immunofluorescence | x | AUC | No | |||||
| BIOMARKER/TESTS and OTHER | ||||||||||||||
| 1 | CxBladder Triage (CxBT) + Imaging | x | mRNA expression of CDK1, HOXA13, MDK, IGFBP5, CXCR2 | [35] | qPCR | x | x | <4.0 to indicate specialist assessment was required | SN, SP, NPV, Accuracy | No | ||||
| 2 | Telomerase + Hb Dipstick | x | Telomerase activity and haematuria | [32] | PCR | x | SN, SP | No | ||||||
| Biomarker Category | Biomarkers/Tests | Studies Identified | Country of Research, Total Population (N) 1 | Clinical Features | Risk Factors | Short Term Outcomes | Authors’ Conclusions (Applicable in the Health System Where the Biomarker Was Evaluated) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Haematuria | UTIs | Other | Smoking (N) 1 | Other (N) 1 | SN | SP | PPV | NPV | ||||||
| VH | NVH | |||||||||||||
| PROTEINS | ADXBLADDER/Mcm5 | Kelly 2012 [51] | UK, 1677 | x | x | x | Urolithiasis; other malignancies; other benign conditions | NA | NA | 73.0% | 68.4% | NA | 96.4% |
|
| Dudderidge 2020 [37] | UK, 856 | x | x | x | NA | NA | NA | 36.0–85.0% 2 | 47.0–96.0% 2 | 17.0–65.0% 2 | 90.0–96.0% 2 |
| ||
| EMA + NMP-52 | Attallah 2015 [30] | Egypt, 160 | x | NA | Cystitis | NA | NA | 94.0% | 80.0% | 75.0% | 95.0% | NA | ||
| uCyt+ + NMP-22 | Todenhöfer 2013 [63] | Germany, 808 | x | x | Irritative voiding symptoms | NA | NA | 90.4% | 35.9% | 19.0% | 95.8% | NA | ||
| mRNAs | CxBladder Triage | Davidson 2020 [35] | New Zealand, 884 | x | x | x | Cystitis; upper tract stones; vascular prostate; anticoagulation; renal disease; primary amyloidosis | NA | Previous cancer diagnosis N = 1; Radiation therapy of pelvis N = 1 | 89.4% | 59.0% | NA | 98.9% |
|
| CxBladder Triage + Imaging | Davidson2020 [35] | 98.1% | 98.4% | NA | 99.9% | |||||||||
| Xpert | van Valenberg 2021 [2] | USA, 828 | x | x | NA | NA | Current N = 139; Former N = 288; Never; N = 401 | Caucasian N = 698; Black N = 80; Hispanic N = 32; Other N = 18 | 78.0% | 84.0% | 27.0% | 98.0% 97.0% 3 99.0% 4 |
| |
| DNAs | FGFR3 + TERT + HRAS + OXT1 + ONECUT2 + TWIST | van Kessel 2017 [67] | Sweden, Spain, Netherlands, 200 | x | NA | NA | NA | NA | 93.2% | 85.6% | 42.2% | 99.2% |
| |
| van Kessel 2020 [68] | Netherlands, 838 | x | x | NA | NA | Current N = 221; Former N = 185; Never N = 258; Not reported N = 174 | NA | 92.0% | 73.0% | 34.0% | 98.0% | |||
| PROTEIN + DNA | UroVysion + NMP-22 + uCyt+ | Todenhöfer 2013 [63] | Germany, 808 | x | x | Irritative voiding symptoms | NA | NA | 83.5% | 74.1% | 34.9% | 96.4% |
| |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papavasiliou, E.; Sills, V.A.; Calanzani, N.; Harrison, H.; Snudden, C.; di Martino, E.; Cowan, A.; Behiyat, D.; Boscott, R.; Tan, S.; et al. Diagnostic Performance of Biomarkers for Bladder Cancer Detection Suitable for Community and Primary Care Settings: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 709. https://doi.org/10.3390/cancers15030709
Papavasiliou E, Sills VA, Calanzani N, Harrison H, Snudden C, di Martino E, Cowan A, Behiyat D, Boscott R, Tan S, et al. Diagnostic Performance of Biomarkers for Bladder Cancer Detection Suitable for Community and Primary Care Settings: A Systematic Review and Meta-Analysis. Cancers. 2023; 15(3):709. https://doi.org/10.3390/cancers15030709
Chicago/Turabian StylePapavasiliou, Evie, Valerie A. Sills, Natalia Calanzani, Hannah Harrison, Claudia Snudden, Erica di Martino, Andy Cowan, Dawnya Behiyat, Rachel Boscott, Sapphire Tan, and et al. 2023. "Diagnostic Performance of Biomarkers for Bladder Cancer Detection Suitable for Community and Primary Care Settings: A Systematic Review and Meta-Analysis" Cancers 15, no. 3: 709. https://doi.org/10.3390/cancers15030709