
Non-Small Cell Lung Cancer (NSCLC) in Young Adults, Age < 50, Is Associated with Late Stage at Presentation and a Very Poor Prognosis in Patients That Do Not Have a Targeted Therapy Option: A Real-World Study
 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistics
3. Results
3.1. Clinical Characteristics
3.2. Molecular Diagnostics in Metastatic NSCLC Patients
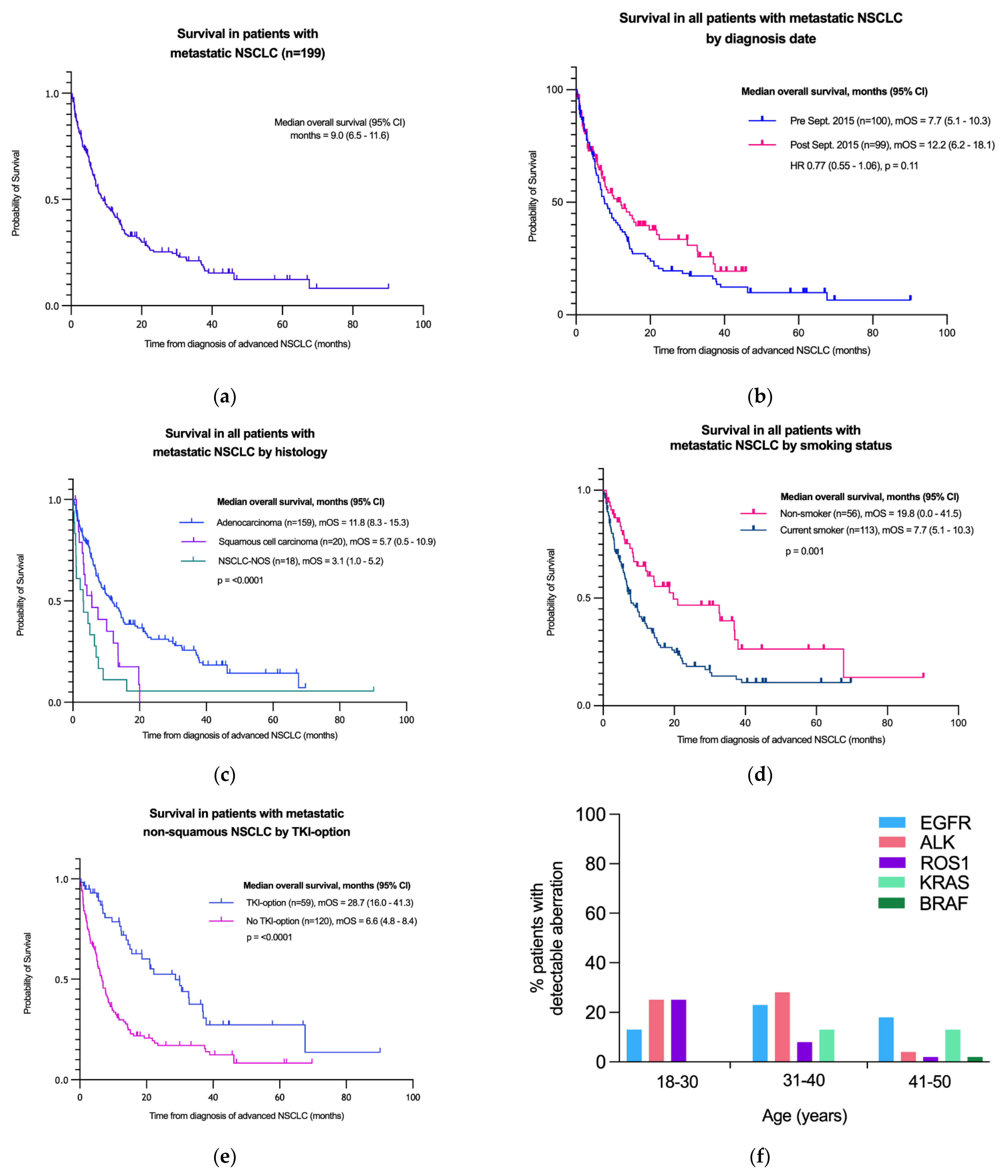
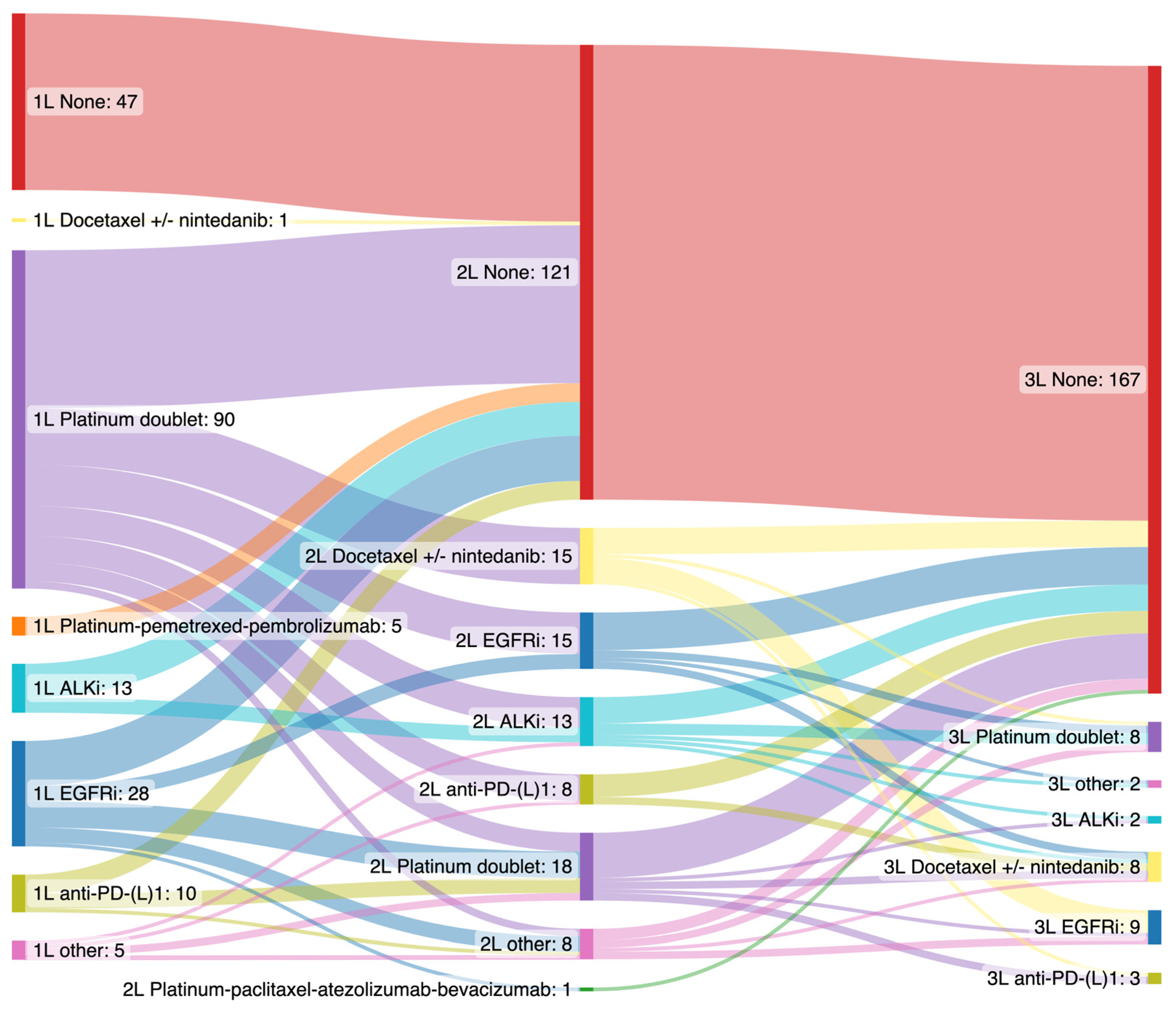
3.3. Treatment and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Lung Fact Sheet, Globocan 2020. Available online: https://gco.iarc.fr/today/fact-sheets-cancers (accessed on 26 August 2022).
- Office for National Statistics. Cancer Survival in England: National Estimates for Patients Followed up to 2017. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/cancersurvivalinengland/nationalestimatesforpatientsfollowedupto2017 (accessed on 26 August 2022).
- Rich, A.L.; Khakwani, A.; Free, C.M.; Tata, L.; A Stanley, R.; Peake, M.D.; Hubbard, R.B.; Baldwin, D.R. Non-small cell lung cancer in young adults: Presentation and survival in the English National Lung Cancer Audit. QJM: Int. J. Med. 2015, 108, 891–897. [Google Scholar] [CrossRef] [Green Version]
- [Dataset] Health Quality Improvement Partnership. National Lung Cancer Audit Annual Audit Report 2020 England Data, Microsoft Excel. 2022. Available online: https://www.rcplondon.ac.uk/projects/outputs/nlca-annual-report-2022 (accessed on 1 October 2022).
- Cancer Research UK. Lung Cancer Incidence Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer/incidence (accessed on 26 August 2022).
- Swanton, C.; Hill, W.; Lim, E.; Lee, C.; Weeden, C.; Augustine, M.; Chen, K.; Kuan, F.-C.; Marongiu, F.; Rodrigues, F.; et al. Mechanism of action and an actionable inflammatory axis for air pollution induced non-small cell lung cancer: Towards molecular cancer prevention. Ann. Oncol. 2022, 33 (Suppl. S7), S1413. [Google Scholar] [CrossRef]
- Suidan, A.M.; Roisman, L.; Rozenblum, A.B.; Ilouze, M.; Dudnik, E.; Zer, A.; Peled, N. Lung Cancer in Young Patients: Higher Rate of Driver Mutations and Brain Involvement, but Better Survival. J. Glob. Oncol. 2019, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Quan, X.; Xu, C.; Lv, J.; Li, C.; Dong, L.; Liu, M. Lung cancer in young adults aged 35 years or younger: A full-scale analysis and review. J. Cancer 2019, 10, 3553–3559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacher, A.; Dahlberg, S.; Heng, J.; Mach, S.; Jänne, P.A.; Oxnard, G.R. Association Between Younger Age and Targetable Genomic Alterations and Prognosis in Non–Small-Cell Lung Cancer. JAMA Oncol. 2016, 2, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramanian, J.; Morgensztern, D.; Goodgame, B.; Baggstrom, M.Q.; Gao, F.; Piccirillo, J.; Govindan, R. Distinctive characteristics of non-small cell lung cancer (NSCLC) in the young: A surveillance, epidemiology, and end results (SEER) analysis. J. Thorac. Oncol. 2010, 5, 23–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosell, R.; Moran, T.; Queralt, C.; Porta, R.; Cardenal, F.; Camps, C.; Majem, M.; Lopez-Vivanco, G.; Isla, D.; Provencio, M.; et al. Screening for Epidermal Growth Factor Receptor Mutations in Lung Cancer. N. Engl. J. Med. 2009, 361, 958–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoneyama, R.; Saji, H.; Kato, Y.; Kudo, Y.; Shimada, Y.; Kimura, M.; Hagiwara, M.; Kakihana, M.; Miyajima, K.; Kajiwara, N.; et al. Clinicopathological characteristics and treatment strategies for young lung cancer patients. Ann. Transl. Med. 2019, 7, 100. [Google Scholar] [CrossRef] [PubMed]
- Moss, C.; Haire, A.; Cahill, F.; Enting, D.; Hughes, S.; Smith, D.; Sawyer, E.; Davies, A.; Zylstra, J.; Haire, K.; et al. Guy’s cancer cohort—real world evidence for cancer pathways. BMC Cancer 2020, 20, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.; Camidge, D.; Gadgeel, S.; Rosell, R.; Dziadziuszko, R.; Kim, D.-W.; Pérol, M.; Ou, S.-H.; Ahn, J.; Shaw, A.; et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann. Oncol. 2020, 31, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Taghizadeh-Hesary, F.; Akbari, H.; Bahadori, M.; Behnam, B. Targeted Anti-Mitochondrial Therapy: The Future of Oncology. Genes 2022, 13, 1728. [Google Scholar] [CrossRef] [PubMed]
- Tafani, M.; Sansone, L.; Limana, F.; Arcangeli, T.; De Santis, E.; Polese, M.; Fini, M.; Russo, M.A. The Interplay of Reactive Oxygen Species, Hypoxia, Inflammation, and Sirtuins in Cancer Initiation and Progression. Oxidative Med. Cell. Longev. 2015, 2016, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, C.; Black, J.R.M.; Reading, J.L.; Litchfield, K.; Turajlic, S.; McGranahan, N.; Jamal-Hanjani, M.; Swanton, C. Tracking cancer evolution through the disease course. Cancer Discov. 2021, 11, 916–932. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.L.; Milan, M.S.D.; Tamen, R.M.; Bertram, A.A.; Michael, K.S.; Ricciuti, B.; Kehl, K.L.; Awad, M.M.; Sholl, L.M.; Paweletz, C.P.; et al. Plasma cfDNA Genotyping in Hospitalized Patients With Suspected Metastatic NSCLC. JCO Precis. Oncol. 2021, 5, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Leighl, N.B.; Page, R.D.; Raymond, V.M.; Daniel, D.B.; Divers, S.G.; Reckamp, K.L.; Villalona-Calero, M.A.; Dix, D.; Odegaard, J.I.; Lanman, R.B.; et al. Clinical Utility of Comprehensive Cell-free DNA Analysis to Identify Genomic Biomarkers in Patients with Newly Diagnosed Metastatic Non–small Cell Lung Cancer. Clin. Cancer Res. 2019, 25, 4691–4700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, W.; Milner-Watts, C.; McVeigh, T.P.; Minchom, A.; Bholse, J.; Davidson, M.; Yousaf, N.; MacMahon, S.; Mugalaasi, H.; Gunapala, R.; et al. A pilot of Blood-First diagnostic cell free DNA (cfDNA) next generation sequencing (NGS) in patients with suspected advanced lung cancer. Lung Cancer 2022, 165, 34–42. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Characteristic | Total n = 248 |
|---|---|
| Age at diagnosis, n (%) | |
| 18–30 | 9 (4) |
| 31–40 | 52 (21) |
| 41–50 | 187 (75) |
| Mean (yrs) | 44 |
| Median (yrs) | 46 |
| Range (yrs) | 26–50 |
| Sex, n (%) | |
| Female | 125 (50) |
| Male | 123 (50) |
| Smoking history, n (%) | |
| Never smoker | 64 (26) |
| Ex-smoker | 51 (21) |
| Smoker | 95 (38) |
| Unknown | 38 (15) |
| Ethnic background, n (%) | |
| White (British, Irish, other) | 145 (58) |
| Black (African, Caribbean, British) | 45 (18) |
| Asian (Asian, British) | 10 (4) |
| Mixed | 3 (1) |
| Other | 7 (3) |
| Not stated | 38 (15) |
| Stage at diagnosis, n (%) | |
| I | 24 (10) |
| II | 15 (6) |
| III | 43 (17) |
| IV | 166 (67) |
| Histopathology, n (%) | |
| Adenocarcinoma | 191 (77) |
| Squamous cell carcinoma | 33 (13) |
| Large cell carcinoma | 3 (1) |
| NSCLC-NOS | 21 (8) |
| Clinical Characteristic | All, n (% of Total) | 18–30 Years | 31–40 Years | 41–50 Years |
|---|---|---|---|---|
| Age at diagnosis, n (%) | 199 (100) | 9 (5) | 44 (22) | 146 (73) |
| Mean (yrs) | 44 | |||
| Median (yrs) | 45 | |||
| Range (yrs) | 26–50 | |||
| Sex, n (%) | ||||
| Female | 97 (49) | 5 (56) | 23 (52) | 69 (47) |
| Male | 102 (51) | 4 (44) | 21 (48) | 77 (53) |
| Smoking history, n (%) | ||||
| Never smoker | 56 (28) | 5 (56) | 20 (45) | 31 (21) |
| Ex-smoker | 38 (19) | 1 (11) | 11 (25) | 26 (18) |
| Smoker | 75 (38) | 1 (11) | 11 (25) | 63 (43) |
| Unknown | 30 (15) | 2 (22) | 2 (5) | 26 (18) |
| Ethnic background, n (%) | ||||
| White (British, Irish, other) | 109 (55) | 7 (78) | 24 (55) | 78 (53) |
| Black (African, Caribbean, British) | 41 (21) | 0 (0) | 6 (14) | 35 (24) |
| Asian (Asian, British) | 10 (5) | 2 (22) | 5 (11) | 3 (2) |
| Mixed | 3 (2) | 0 (0) | 2 (5) | 1 (1) |
| Other | 4 (2) | 0 (0) | 1 (2) | 3 (2) |
| Not stated | 32 (16) | 0 (0) | 6 (14) | 26 (18) |
| Stage at diagnosis, n (%) | ||||
| I | 6 (3) | 0 (0) | 0 (0) | 6 (4) |
| II | 2 (1) | 0 (0) | 0 (0) | 2 (1) |
| III | 25 (13) | 2 (22) | 2 (5) | 21 (14) |
| IV | 166 (83) | 7 (78) | 42 (95) | 117 (80) |
| Number of metastatic sites *, n (%) | ||||
| 1 | 69 (35) | 1 (11) | 11(25) | 57 (39) |
| 2 | 73 (37) | 4 (44) | 18 (41) | 51 (35) |
| >3 | 57 (29) | 4 (44) | 15 (34) | 38 (26) |
| Metastatic sites *, n (%) | ||||
| Intrathoracic | 98 (49) | 6 (67) | 31 (70) | 61 (42) |
| Extrathoracic | ||||
| Brain | 65 (33) | 3 (33) | 12 (28) | 50 (34) |
| Bone | 82 (41) | 6 (67) | 14 (32) | 62 (42) |
| Liver | 37 (19) | 3 (33) | 10 (23) | 24 (16) |
| Adrenal | 35 (18) | 1 (11) | 6 (14) | 28 (19) |
| Distal lymph nodes | 34 (17) | 4 (44) | 7 (16) | 23 (16) |
| other | 21 (11) | 2 (22) | 3 (7) | 16 (11) |
| Performance status at diagnosis, n (%) | ||||
| 0 | 39 (20) | 0 (0) | 10 (23) | 29 (20) |
| 1 | 101 (51) | 9 (100) | 26 (59) | 66 (45) |
| 2 | 18 (9) | 0 (0) | 2 (5) | 16 (11) |
| 3 | 12 (6) | 0 (0) | 2 (5) | 10 (7) |
| 4 | 4 (2) | 0 (0) | 0 (0) | 4 (3) |
| unknown | 25 (13) | 0 (0) | 4 (9) | 21 (14) |
| Histopathology, n (%) | ||||
| Adenocarcinoma | 159 (80) | 8 (89) | 38 (86) | 113 (77) |
| Squamous cell carcinoma | 20 (10) | 1 (11) | 4 (9) | 15 (10) |
| Large cell carcinoma | 2 (1) | 0 (0) | 1 (2) | 1 (1) |
| NSCLC-NOS | 18 (9) | 0 (0) | 1 (2) | 17 (12) |
| PD-L1 score, n (%) | ||||
| <1 | 32 (16) | 0 (0) | 12 (27) | 20 (14) |
| 1–49 | 18 (9) | 0 (0) | 5 (11) | 13 (9) |
| ≥50 | 32 (16) | 3 (33) | 11 (25) | 18 (12) |
| Unknown | 117 (59) | 6 (67) | 16 (36) | 95 (65) |
| EGFR status in Non-squamous, n (%) | ||||
| Mutant | 34 (19) | 1 (13) | 9 (23) | 24 (18) |
| Wild type | 123 (69) | 7 (88) | 28 (70) | 88 (67) |
| Unknown | 22 (12) | 0 (0) | 3 (8) | 19 (15) |
| ALK status in Non-squamous, n (%) | ||||
| Rearranged | 18 (10) | 2 (25) | 11 (28) | 5 (4) |
| Not rearranged | 100 (56) | 4 (50) | 24 (60) | 72 (55) |
| Unknown | 61 (34) | 2 (25) | 5 (13) | 54 (41) |
| ROS1 status in Non-squamous, n (%) | ||||
| Rearranged | 8 (4) | 2 (25) | 3 (8) | 3 (2) |
| Not rearranged | 94 (53) | 4 (50) | 28 (70) | 62 (47) |
| Unknown | 77 (43) | 2 (25) | 9 (23) | 66 (50) |
| KRAS status in Non-squamous, n (%) | ||||
| Mutant | 22 (12) | 0 (0) | 5 (13) | 17 (13) |
| Wild type | 97 (54) | 4 (50) | 24 (60) | 69 (53) |
| Unknown | 60 (34) | 4 (50) | 11 (28) | 45 (34) |
| BRAF status in Non-squamous, n (%) | ||||
| Mutant | 2 (1) | 0 (0) | 0 (0) | 2 (2) |
| Wild type | 51 (29) | 3 (38) | 11 (28) | 37 (28) |
| Unknown | 126 (70) | 5 (62) | 29 (72) | 92 (70) |
| Radiotherapy Received | All, n (% of Total) | 18–30 Years | 31–40 Years | 41–50 Years |
|---|---|---|---|---|
| Palliative | ||||
| yes | 70 (35) | 4 (44) | 12 (27) | 54 (37) |
| no | 129 (65) | 5 (56) | 32 (73) | 92 (63) |
| Whole brain | ||||
| yes | 44 (22) | 2 (22) | 7 (16) | 35 (24) |
| no | 155 (78) | 7 (78) | 37 (84) | 111 (76) |
| Stereotactic brain | ||||
| yes | 11 (6) | 0 (0) | 4 (9) | 7 (5) |
| no | 188 (94) | 9 (100) | 40 (91) | 139 (95) |
| Variable | Hazard Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Age (yrs) | |||
| 18–30 | 1.0 | -- | -- |
| 31–40 | 0.70 | 0.29–2.12 | 0.483 |
| 41–50 | 0.60 | 0.25–1.80 | 0.305 |
| Sex | |||
| Female | 1.0 | -- | -- |
| Male | 1.03 | 0.72–1.48 | 0.855 |
| Smoking history | |||
| Never smoker | 0.59 | 0.34–1.00 | 0.052 |
| Ex-smoker | 1.19 | 0.72–1.91 | 0.488 |
| Smoker | 1.0 | -- | -- |
| Ethnic background | |||
| White (British, Irish, other) | 1.0 | -- | -- |
| Black (African, Caribbean, British) | 0.83 | 0.53–1.28 | 0.406 |
| Asian (Asian, British) | 0.84 | 0.32–1.86 | 0.700 |
| Mixed | 1.01 | 0.16–3.31 | 0.991 |
| Other | 2.89 | 0.65–9.03 | 0.105 |
| Number of metastatic sites *, n (%) | |||
| 1 | 0.38 | 0.24–0.62 | <0.001 |
| 2 | 0.70 | 0.45–1.10 | 0.113 |
| >3 | 1.0 | -- | -- |
| Intracranial mets | |||
| Yes | 1.0 | -- | -- |
| No | 1.0 | 0.69–1.47 | 0.986 |
| Histopathology | |||
| Adenocarcinoma | 1.0 | -- | -- |
| Squamous cell carcinoma | 1.69 | 0.95–2.84 | 0.060 |
| Large cell carcinoma | 2.28 | 1.92–52.58 | 0.004 |
| NSCLC-NOS | 13.02 | 1.26–3.94 | 0.001 |
| TKI-option | |||
| Yes No | 0.42 | 0.24–0.69 | <0.001 |
| 1.0 | -- | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hughes, D.J.; Kapiris, M.; Podvez Nevajda, A.; McGrath, H.; Stavraka, C.; Ahmad, S.; Taylor, B.; Cook, G.J.R.; Ghosh, S.; Josephs, D.; et al. Non-Small Cell Lung Cancer (NSCLC) in Young Adults, Age < 50, Is Associated with Late Stage at Presentation and a Very Poor Prognosis in Patients That Do Not Have a Targeted Therapy Option: A Real-World Study. Cancers 2022, 14, 6056. https://doi.org/10.3390/cancers14246056
Hughes DJ, Kapiris M, Podvez Nevajda A, McGrath H, Stavraka C, Ahmad S, Taylor B, Cook GJR, Ghosh S, Josephs D, et al. Non-Small Cell Lung Cancer (NSCLC) in Young Adults, Age < 50, Is Associated with Late Stage at Presentation and a Very Poor Prognosis in Patients That Do Not Have a Targeted Therapy Option: A Real-World Study. Cancers. 2022; 14(24):6056. https://doi.org/10.3390/cancers14246056
Chicago/Turabian StyleHughes, Daniel Johnathan, Matthaios Kapiris, Andreja Podvez Nevajda, Harriet McGrath, Chara Stavraka, Shahreen Ahmad, Benjamin Taylor, Gary J. R. Cook, Sharmistha Ghosh, Debra Josephs, and et al. 2022. "Non-Small Cell Lung Cancer (NSCLC) in Young Adults, Age < 50, Is Associated with Late Stage at Presentation and a Very Poor Prognosis in Patients That Do Not Have a Targeted Therapy Option: A Real-World Study" Cancers 14, no. 24: 6056. https://doi.org/10.3390/cancers14246056