

An Indeterminate for Malignancy FNA Report Does Not Increase the Surgical Risk of Incidental Thyroid Carcinoma

 , ,
, ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pezzolla, A.; Marzaioli, R.; Lattarulo, S.; Docimo, G.; Conzo, G.; Ciampolillo, A.; Barile, G.; Anelli, F.M.; Madaro, A. Incidental Carcinoma of the Thyroid. Int. J. Surg. 2014, 12, S98–S102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evranos, B.; Polat, S.B.; Cuhaci, F.N.; Baser, H.; Topaloglu, O.; Kilicarslan, A.; Kilic, M.; Ersoy, R.; Cakir, B. A Cancer of Undetermined Significance: Incidental Thyroid Carcinoma. Diagn. Cytopathol. 2019, 47, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Bahl, M.; Sosa, J.A.; Nelson, R.C.; Esclamado, R.M.; Choudhury, K.R.; Hoang, J.K. Trends in Incidentally Identified Thyroid Cancers over a Decade: A Retrospective Analysis of 2,090 Surgical Patients. World J. Surg. 2014, 38, 1312–1317. [Google Scholar] [CrossRef]
- Papini, E.; Guglielmi, R.; Bianchini, A.; Crescenzi, A.; Taccogna, S.; Nardi, F.; Panunzi, C.; Rinaldi, R.; Toscano, V.; Pacella, C.M. Risk of Malignancy in Nonpalpable Thyroid Nodules: Predictive Value of Ultrasound and Color-Doppler Features. J. Clin. Endocrinol. Metab. 2002, 87, 1941–1946. [Google Scholar] [CrossRef] [PubMed]
- Pagni, F.; Jaconi, M.; Delitala, A.; Garancini, M.; Maternini, M.; Bono, F.; Giani, A.; Smith, A. San Gerardo Hospital collaborators group Incidental Papillary Thyroid Carcinoma: Diagnostic Findings in a Series of 287 Carcinomas. Endocr. Pathol. 2014, 25, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Garshell, J.; Neyman, N.; Altekruse, S.F.; Kosary, C.L.; Yu, M.; Ruhl, J.; Tatalovich, Z.; et al. SEER Cancer Statistics Review; National Cancer Institute: Bethesda, MD, USA, 2013; pp. 1975–2010.
- Sosa, J.A.; Hanna, J.W.; Robinson, K.A.; Lanman, R.B. Increases in Thyroid Nodule Fine-Needle Aspirations, Operations, and Diagnoses of Thyroid Cancer in the United States. Surgery 2013, 154, 1420–1426, discussion 1426–1427. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Vita, R.; Ieni, A.; Tuccari, G.; Benvenga, S. The Increasing Prevalence of Chronic Lymphocytic Thyroiditis in Papillary Microcarcinoma. Rev. Endocr. Metab. Disord. 2018, 19, 301–309. [Google Scholar] [CrossRef]
- Mazzaferri, E.L. Management of a Solitary Thyroid Nodule. N. Engl. J. Med. 1993, 328, 553–559. [Google Scholar]
- Nguyen, X.V.; Job, J.; Fiorillo, L.E.; Sipos, J. Thyroid Incidentalomas: Practice Considerations for Radiologists in the Age of Incidental Findings. Radiol. Clin. North Am. 2020, 58, 1019–1031. [Google Scholar] [CrossRef]
- Ali, S.Z.; Cibas, E.S. The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria, and Explanatory Notes; Springer: Berlin/Heidelberg, Germany, 2017; ISBN 9783319605708. [Google Scholar]
- Seminati, D.; Capitoli, G.; Leni, D.; Fior, D.; Vacirca, F.; Di Bella, C.; Galimberti, S.; L’Imperio, V.; Pagni, F. Use of Diagnostic Criteria from ACR and EU-TIRADS Systems to Improve the Performance of Cytology in Thyroid Nodule Triage. Cancers 2021, 13, 5439. [Google Scholar] [CrossRef] [PubMed]
- Leni, D.; Seminati, D.; Fior, D.; Vacirca, F.; Capitoli, G.; Cazzaniga, L.; Di Bella, C.; L’Imperio, V.; Galimberti, S.; Pagni, F. Diagnostic Performances of the ACR-TIRADS System in Thyroid Nodules Triage: A Prospective Single Center Study. Cancers 2021, 13, 2230. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F.; Basolo, F.; Bellantone, R.; Boni, G.; Cannizzaro, M.A.; De Palma, M.; Durante, C.; Elisei, R.; Fadda, G.; Frasoldati, A.; et al. Italian Consensus on Diagnosis and Treatment of Differentiated Thyroid Cancer: Joint Statements of Six Italian Societies. J. Endocrinol. Investig. 2018, 41, 849–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs; International Agency for Research on Cancer: Lyon, France, 2017; ISBN 9789283244936. [Google Scholar]
- Institute, N.C. National Cancer Institute AJCC Cancer Staging Manual 8th Edition. Definitions 2020, 1, p873. [Google Scholar]
- Nabhan, F.; Ringel, M.D. Thyroid Nodules and Cancer Management Guidelines: Comparisons and Controversies. Endocr. Relat. Cancer 2017, 24, R13–R26. [Google Scholar] [CrossRef] [Green Version]
- Kamran, S.C.; Marqusee, E.; Kim, M.I.; Frates, M.C.; Ritner, J.; Peters, H.; Benson, C.B.; Doubilet, P.M.; Cibas, E.S.; Barletta, J.; et al. Thyroid Nodule Size and Prediction of Cancer. J. Clin. Endocrinol. Metab. 2013, 98, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Fisher, S.B.; Perrier, N.D. The Incidental Thyroid Nodule. CA Cancer J. Clin. 2018, 68, 97–105. [Google Scholar] [CrossRef]
- Kaliszewski, K.; Strutyńska-Karpińska, M.; Zubkiewicz-Kucharska, A.; Wojtczak, B.; Domosławski, P.; Balcerzak, W.; Łukieńczuk, T.; Forkasiewicz, Z. Should the Prevalence of Incidental Thyroid Cancer Determine the Extent of Surgery in Multinodular Goiter? PLoS ONE 2016, 11, e0168654. [Google Scholar] [CrossRef]
- Kaliszewski, K.; Diakowska, D.; Strutyńska-Karpińska, M.; Wojtczak, B.; Domosławski, P.; Balcerzak, W. Clinical and Histopathological Characteristics of Patients with Incidental and Nonincidental Thyroid Cancer. Arch. Med. Sci. 2017, 2, 390–395. [Google Scholar] [CrossRef]
- Maloney, E.; Dougherty, P.; Dighe, M.; Relyea-Chew, A. The Development of a Validated Checklist for Ultrasound-Guided Thyroid Nodule Fine-Needle Aspiration Biopsies. Ultrasound Q. 2015, 31, 159–165. [Google Scholar] [CrossRef]
- Yoo, F.; Chaikhoutdinov, I.; Mitzner, R.; Liao, J.; Goldenberg, D. Characteristics of Incidentally Discovered Thyroid Cancer. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 1181–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chooi, J.E.; Ravindiran, A.; Balasubramanian, S.P. The Influence of Incidental Detection of Thyroid Nodule on Thyroid Cancer Risk and Prognosis-a Systematic Review. J. Endocr. Soc. 2021, 5, A871. [Google Scholar] [CrossRef]
- Wagner, J.; Aron, D.C. Incidentalomas–A “disease” of Modern Imaging Technology. Best Pract. Res. Clin. Endocrinol. Metabolism 2012, 26, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Kwong, N.; Medici, M.; Angell, T.E.; Liu, X.; Marqusee, E.; Cibas, E.S.; Krane, J.F.; Barletta, J.A.; Kim, M.I.; Larsen, P.R.; et al. The Influence of Patient Age on Thyroid Nodule Formation, Multinodularity, and Thyroid Cancer Risk. J. Clin. Endocrinol. Metab. 2015, 100, 4434–4440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lombardi, C.P.; Bellantone, R.; De Crea, C.; Paladino, N.C.; Fadda, G.; Salvatori, M.; Raffaelli, M. Papillary Thyroid Microcarcinoma: Extrathyroidal Extension, Lymph Node Metastases, and Risk Factors for Recurrence in a High Prevalence of Goiter Area. World J. Surg. 2010, 34, 1214–1221. [Google Scholar] [CrossRef]
- Vasileiadis, I.; Karatzas, T.; Vasileiadis, D.; Kapetanakis, S.; Charitoudis, G.; Karakostas, E.; Kouraklis, G. Clinical and Pathological Characteristics of Incidental and Nonincidental Papillary Thyroid Microcarcinoma in 339 Patients. Head Neck 2014, 36, 564–570. [Google Scholar] [CrossRef]
- Huang, L.-Y.; Lee, Y.-L.; Chou, P.; Chiu, W.-Y.; Chu, D. Thyroid Fine-Needle Aspiration Biopsy and Thyroid Cancer Diagnosis: A Nationwide Population-Based Study. PLoS ONE 2015, 10, e0127354. [Google Scholar] [CrossRef]
- Ippolito, D.; Galimberti, S.; Leni, D.; Vacirca, F.; Nasr, A.; Bragazzi, N.L.; Spiga, S.; Schiavone, V.; Pincelli, A.I.; Garancini, M.; et al. Use of Shear Wave Elastography in the Sonographic Triage of Thyroid Nodules: Feasibility Study in a Series of Lesions Already Selected for Fine Needle Aspiration. J. Ultrasound Med. 2019, 38, 1713–1720. [Google Scholar] [CrossRef]
- De Carlos, J.; Ernaga, A.; Irigaray, A.; Pineda, J.J.; Echegoyen, A.; Salvador, P.; Anda, E. Incidentally Discovered Papillary Thyroid Microcarcinoma in Patients Undergoing Thyroid Surgery for Benign Disease. Endocrine 2022, 77, 325–332. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Increasing Incidence of Thyroid Cancer in the United States, 1973-2002. JAMA 2006, 295, 2164–2167. [Google Scholar] [CrossRef] [Green Version]
- John, A.M.; Jacob, P.M.; Oommen, R.; Nair, S.; Nair, A.; Rajaratnam, S. Our Experience with Papillary Thyroid Microcancer. Indian J. Endocrinol. Metab. 2014, 18, 410–413. [Google Scholar] [PubMed]
- Trimboli, P.; Ferrarazzo, G.; Cappelli, C.; Piccardo, A.; Castellana, M.; Barizzi, J. Thyroid Nodules with Indeterminate FNAC According to the Italian Classification System: Prevalence, Rate of Operation, and Impact on Risk of Malignancy. An Updated Systematic Review and Meta-Analysis. Endocr. Pathol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-H.; Chen, C.-Y. Clinicopathologic Characteristics of Incidental Thyroid Carcinoma in Euthyroid Patients Receiving Total Thyroidectomy for Multinodular Goiter: A Retrospective Cohort Study. J. Chin. Med. Assoc. 2022, 85, 839. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.G.; da Silva, L.F.F.; Araujo-Filho, V.J.F.d.; Mosca, L.d.M.; Araujo-Neto, V.J.F.d.; Kowalski, L.P.; Carneiro, P.C. Incidental Thyroid Carcinoma: Correlation between FNAB Cytology and Pathological Examination in 1093 Cases. Clinics 2022, 77, 100022. [Google Scholar] [CrossRef] [PubMed]
- Provenzale, M.A.; Fiore, E.; Ugolini, C.; Torregrossa, L.; Morganti, R.; Molinaro, E.; Miccoli, P.; Basolo, F.; Vitti, P. “Incidental” and “non-Incidental” Thyroid Papillary Microcarcinomas Are Two Different Entities. Eur. J. Endocrinol. 2016, 174, 813–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Uruno, T.; Nakano, K.; Takamura, Y.; Miya, A.; Kobayashi, K.; Yokozawa, T.; Matsuzuka, F.; Kuma, S.; Kuma, K.; et al. An Observation Trial without Surgical Treatment in Patients with Papillary Microcarcinoma of the Thyroid. Thyroid 2003, 13, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malandrino, P.; Pellegriti, G.; Attard, M.; Violi, M.A.; Giordano, C.; Sciacca, L.; Regalbuto, C.; Squatrito, S.; Vigneri, R. Papillary Thyroid Microcarcinomas: A Comparative Study of the Characteristics and Risk Factors at Presentation in Two Cancer Registries. J. Clin. Endocrinol. Metab. 2013, 98, 1427–1434. [Google Scholar] [CrossRef] [Green Version]
- Baloch, Z.W.; Asa, S.L.; Barletta, J.A.; Ghossein, R.A.; Juhlin, C.C.; Jung, C.K.; LiVolsi, V.A.; Papotti, M.G.; Sobrinho-Simões, M.; Tallini, G.; et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr. Pathol. 2022, 33, 27–63. [Google Scholar] [CrossRef]
- Wartofsky, L. Management of Papillary Microcarcinoma: Primum Non Nocere? J. Clin. Endocrinol. Metab. 2012, 97, 1169–1172. [Google Scholar] [CrossRef] [Green Version]
- Tuttle, R.M.; Alzahrani, A.S. Risk Stratification in Differentiated Thyroid Cancer: From Detection to Final Follow-Up. J. Clin. Endocrinol. Metab. 2019, 104, 4087–4100. [Google Scholar] [CrossRef]
- Maturo, A.; Tromba, L.; De Anna, L.; Carbotta, G.; Livadoti, G.; Donello, C.; Falbo, F.; Galiffa, G.; Esposito, A.; Biancucci, A.; et al. Incidental Thyroid Carcinomas. A Retrospective Study. G. Chir. 2017, 38, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Wada, N.; Duh, Q.-Y.; Sugino, K.; Iwasaki, H.; Kameyama, K.; Mimura, T.; Ito, K.; Takami, H.; Takanashi, Y. Lymph Node Metastasis from 259 Papillary Thyroid Microcarcinomas: Frequency, Pattern of Occurrence and Recurrence, and Optimal Strategy for Neck Dissection. Ann. Surg. 2003, 237, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Jaconi, M.; Manzoni, M.; Pincelli, A.I.; Giardini, V.; Scardilli, M.; Smith, A.; Fellegara, G.; Pagni, F. The Impact of the Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Feature Terminology in the Routine Diagnosis of Thyroid Tumours. Cytopathology 2017, 28, 495–502. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Classes III–IV Patient Parameters | Results | |
|---|---|---|
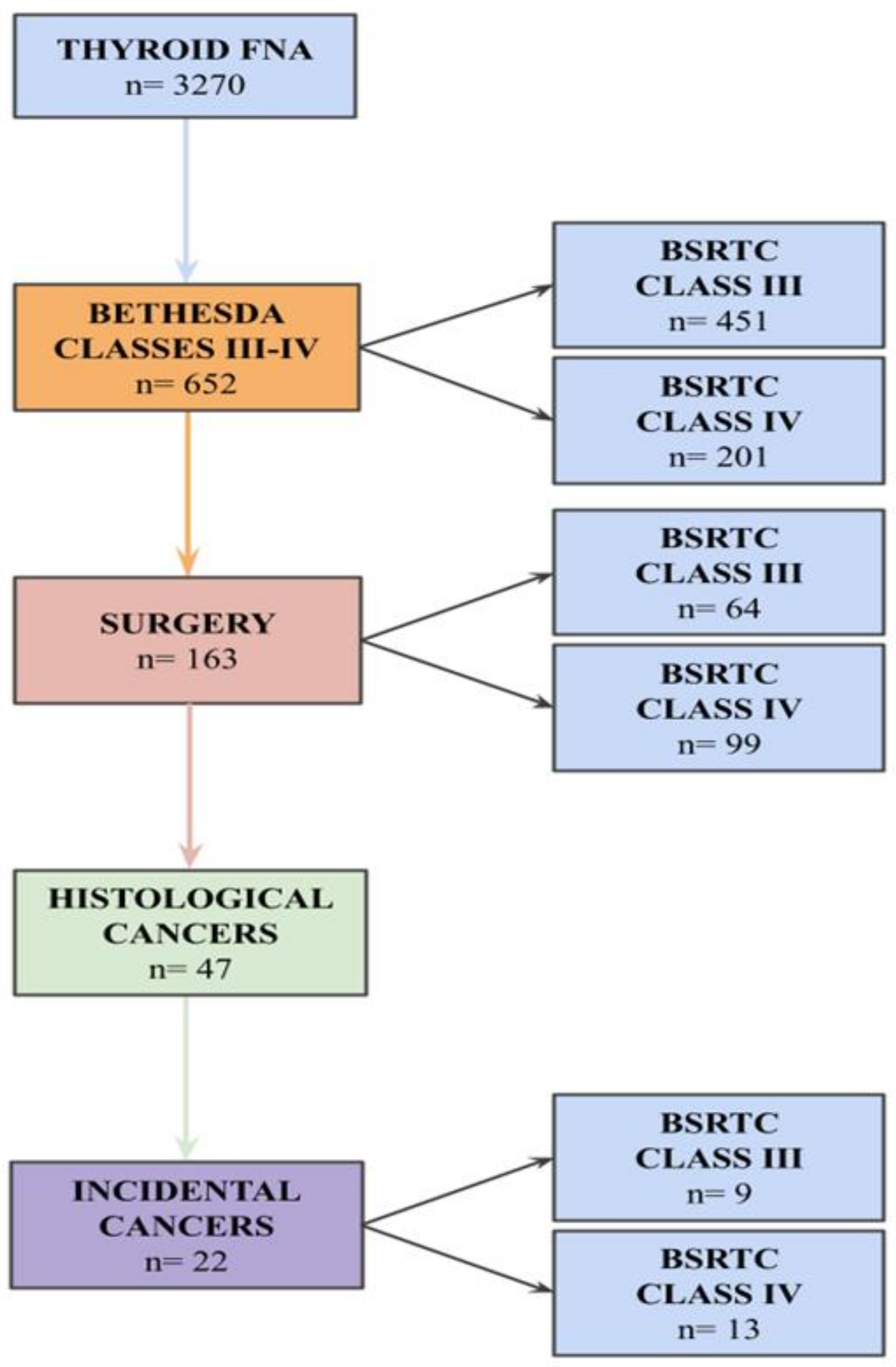
| Number of Patients | 652 | |
| AJCC AGE GROUPS (years) | <55 | 39.8% (260) |
| ≥55 | 60.2% (392) | |
| SEX | Male | 30.8% (201) |
| Female | 69.2% (451) | |
| FNA NODULE SIZE (mm) | ≤10 | 17% (111) |
| 11–20 | 40.9% (267) | |
| 21–30 | 21.9% (143) | |
| 31–40 | 13% (85) | |
| >40 | 7% (46) | |
| FNA RESULT | Bethesda III | 69.2% (451) |
| Bethesda IV | 30.8% (201) | |
| SURGICAL RESECTION | Yes | 25% (163) |
| No | 75% (489) | |
| BETHESDA CLASS III SURGICAL REASON | Symptomatic or unaesthetic | 48.4% (31) |
| Multinodularity | 51.5% (33) | |
| ITC Patient Parameters | Results | |
|---|---|---|
| Number of Patients | 22 | |
| AJCC AGE GROUPS (years) | <55 | 31.9% (7) |
| ≥55 | 68.1% (15) | |
| SEX | Male | 27.3% (6) |
| Female | 72.7% (16) | |
| HASHIMOTO’S THYROIDITIS | Present | 13.6% (3) |
| Absent | 86.3% (19) | |
| GRAVES’ DISEASE | Present | 0% (0) |
| Absent | 100% (22) | |
| FNA NODULE SIZE (mm) | ≤10 | 27.2% (6) |
| 11–20 | 22.7% (5) | |
| 21–30 | 18.2% (4) | |
| 31–40 | 31.8% (7) | |
| >40 | 0% (0) | |
| MEAN NODULE SIZE (mm) | 24 (SD: 11.6) | |
| FNAB RESULT | Bethesda III | 40.9% (9) |
| Bethesda IV | 59.1% (13) | |
| HISTOLOGY | Papillary (PTC) | 100% (22) |
| Follicular | 0% (0) | |
| PTC HISTOLOGICAL SUBTYPE | Conventional | 50% (11) |
| Follicular | 31.8% (7) | |
| Conventional and follicular | 18.2% (4) | |
| DOMINANT SITE | Right lobe | 45.4% (10) |
| Left lobe | 55.6% (12) | |
| TUMOR SIZE (mm) | ≤10 | 100% (22) |
| >10 | 0% (0) | |
| MEAN TUMOR SIZE (mm) | 3.7 (SD: 2.7) | |
| CANCER FOCI | 1 | 63.6% (14) |
| ≥2 | 36.4% (8) | |
| CAPSULAR INVASION | Present | 4.5% (1) |
| Absent | 95.4% (21) | |
| VASCULAR INVASION | Present | 0% (0) |
| Absent | 100% (22) | |
| EXTRATHYROIDAL EXTENSION | Present | 0% (0) |
| Absent | 100% (22) | |
| RESECTION | Complete | 100% (22) |
| Non-complete | 0% (0) | |
| LYMPH NODE METASTASIS | Present | 0% (0) |
| Absent | 100% (22) | |
| DISTANT METASTASIS | Present | 0% (0) |
| Absent | 100% (22) | |
| AJCC TUMOR STAGE | I | 100% (22) |
| II | 0% (0) | |
| III | ||
| IV | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seminati, D.; Mane, E.; Ceola, S.; Casati, G.; Putignano, P.; Garancini, M.; Gatti, A.; Leni, D.; Pincelli, A.I.; Fusco, N.; et al. An Indeterminate for Malignancy FNA Report Does Not Increase the Surgical Risk of Incidental Thyroid Carcinoma. Cancers 2022, 14, 5427. https://doi.org/10.3390/cancers14215427
Seminati D, Mane E, Ceola S, Casati G, Putignano P, Garancini M, Gatti A, Leni D, Pincelli AI, Fusco N, et al. An Indeterminate for Malignancy FNA Report Does Not Increase the Surgical Risk of Incidental Thyroid Carcinoma. Cancers. 2022; 14(21):5427. https://doi.org/10.3390/cancers14215427
Chicago/Turabian StyleSeminati, Davide, Eltjona Mane, Stefano Ceola, Gabriele Casati, Pietro Putignano, Mattia Garancini, Andrea Gatti, Davide Leni, Angela Ida Pincelli, Nicola Fusco, and et al. 2022. "An Indeterminate for Malignancy FNA Report Does Not Increase the Surgical Risk of Incidental Thyroid Carcinoma" Cancers 14, no. 21: 5427. https://doi.org/10.3390/cancers14215427