BERENICE Final Analysis: Cardiac Safety Study of Neoadjuvant Pertuzumab, Trastuzumab, and Chemotherapy Followed by Adjuvant Pertuzumab and Trastuzumab in HER2-Positive Early Breast Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Procedures
2.3. Assessments
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Cardiac Safety
3.2.1. Adjuvant Period
3.2.2. TFFU Period
3.2.3. Timing of Occurrence of Cardiac Events
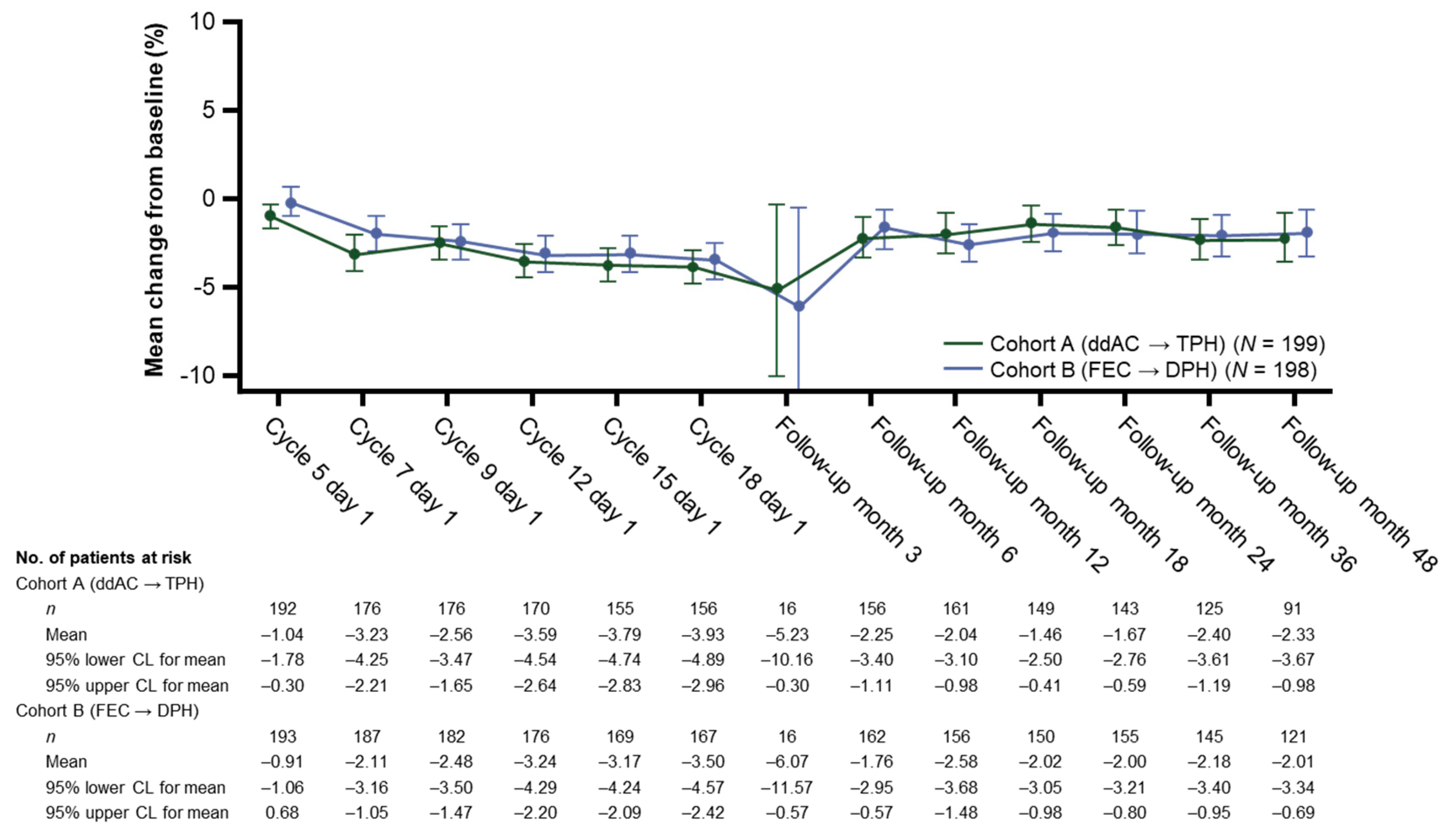
3.2.4. Mean Change in LVEF from Baseline
3.2.5. Cardiac Event Resolution Rates
3.3. General Safety
3.3.1. Adjuvant Period
3.3.2. TFFU Period
3.4. Efficacy
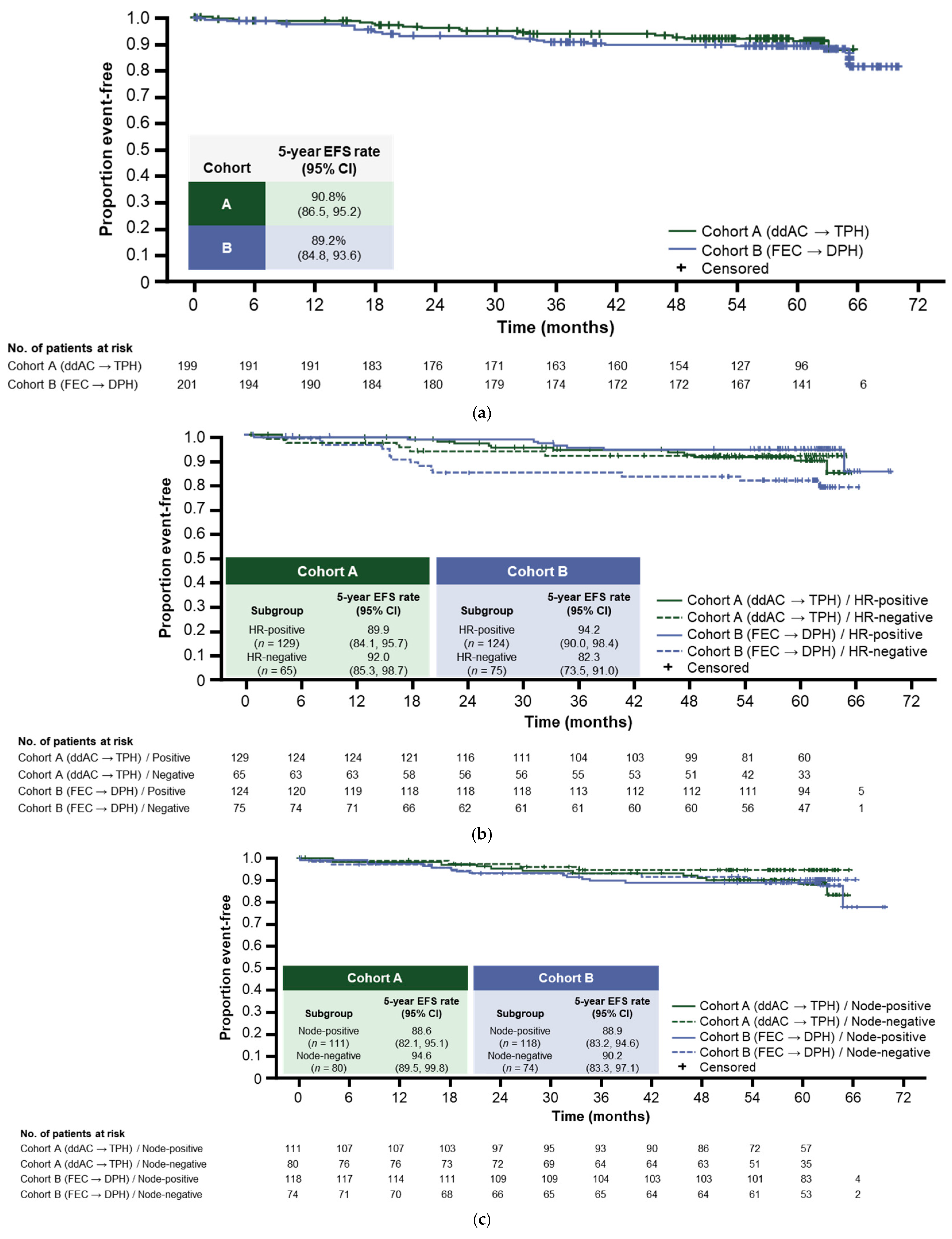
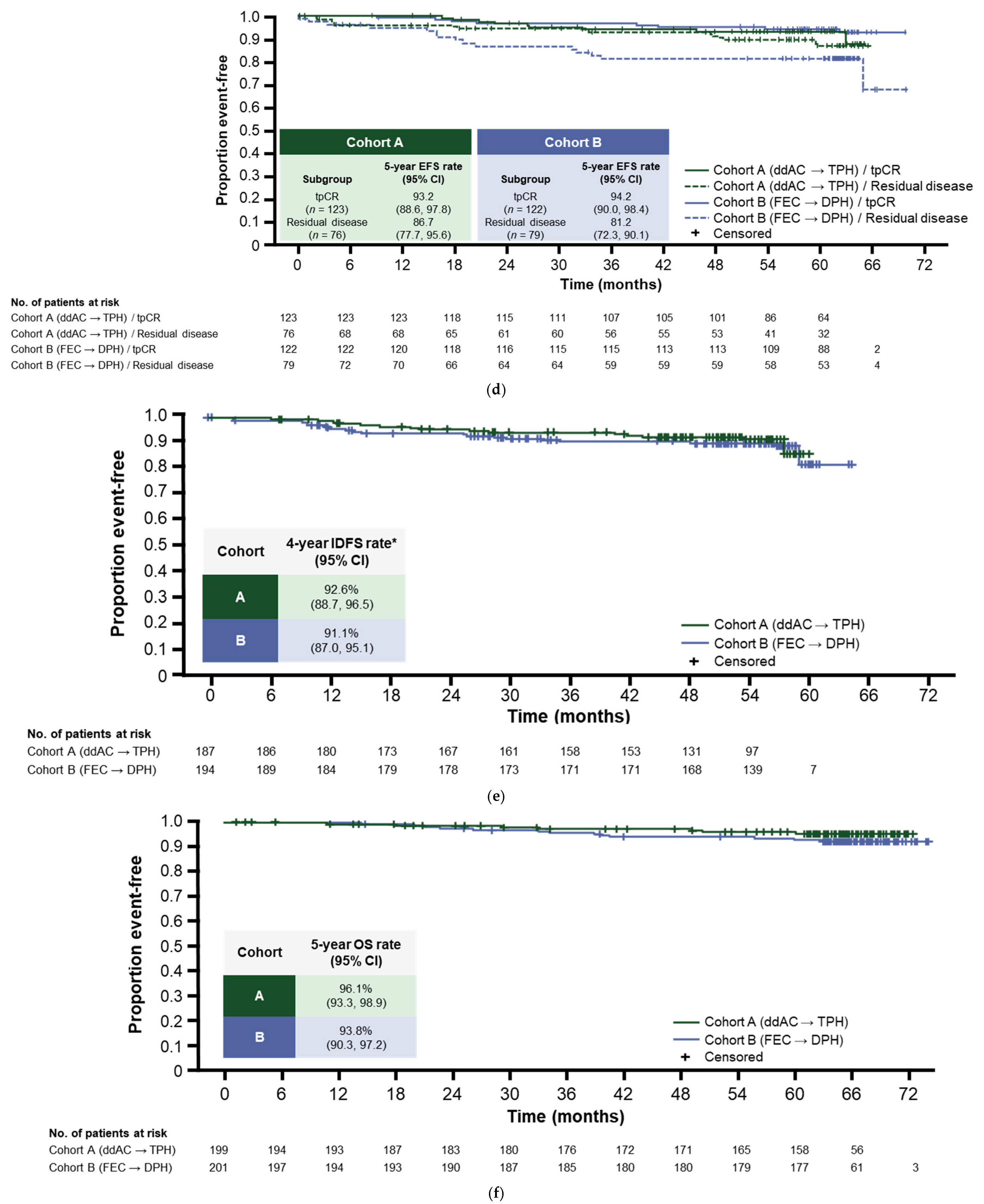
3.4.1. Five-Year EFS
3.4.2. Four-Year IDFS
3.4.3. Five-Year OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Bryant, S.E.; Mielke, M.M.; Rissman, R.A.; Lista, S.; Vanderstichele, H.; Zetterberg, H.; Lewczuk, P.; Posner, H.; Hall, J.; Johnson, L.; et al. Blood-based biomarkers in Alzheimer disease: Current state of the science and a novel collaborative paradigm for advancing from discovery to clinic. Alzheimers Dement. 2017, 13, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Genentech Inc. FDA Grants Genentech’s Perjeta Accelerated Approval for Use before Surgery in People with HER2-Positive Early Stage Breast Cancer [Press Release]. 30 September 2013. Available online: https://www.gene.com/media/press-releases/14548/2013-09-30/fda-grants-genentechs-perjeta-accelerate (accessed on 4 February 2022).
- Genentech Inc. PERJETA® (Pertuzumab). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125409s124lbl.pdf (accessed on 4 February 2022).
- Gianni, L.; Pienkowski, T.; Im, Y.H.; Tseng, L.M.; Liu, M.C.; Lluch, A.; Starosławska, E.; de la Haba-Rodriguez, J.; Im, S.A.; Pedrini, J.L.; et al. 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): A multicentre, open-label, phase 2 randomised trial. Lancet Oncol. 2016, 17, 791–800. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Waldron-Lynch, M.; Eng-Wong, J.; Kirk, S.; Cortés, J. Long-term efficacy analysis of the randomised, phase II TRYPHAENA cardiac safety study: Evaluating pertuzumab and trastuzumab plus standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer. Eur. J. Cancer 2018, 89, 27–35. [Google Scholar]
- Swain, S.M.; Ewer, M.S.; Viale, G.; Delaloge, S.; Ferrero, J.M.; Verrill, M.; Colomer, R.; Vieira, C.; Werner, T.L.; Douthwaite, H.; et al. Pertuzumab, trastuzumab, and standard anthracycline- and taxane-based chemotherapy for the neoadjuvant treatment of patients with HER2-positive localized breast cancer (BERENICE): A phase II, open-label, multicenter, multinational cardiac safety study. Ann. Oncol. 2018, 29, 646–653. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.H.; Roman, L.; Tseng, L.M.; Liu, M.C.; Lluch, A.; Staroslawska, E.; Haba-Rodriguez, J.; Im, S.A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Hegg, R.; Tausch, C.; Seo, J.H.; Tsai, Y.F.; Ratnayake, J.; et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: A randomized phase II cardiac safety study (TRYPHAENA). Ann. Oncol. 2013, 24, 2278–2284. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.S.; Mullins, M.; Cheang, M.C.; Leung, S.; Voduc, D.; Vickery, T.; Davies, S.; Fauron, C.; He, X.; Hu, Z.; et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. J. Clin. Oncol. 2009, 27, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.R.; Yu, J.; Lu, X.; Spoerke, J.M.; Xiao, Y.; O’Brien, C.; Savage, H.M.; Huw, L.Y.; Zou, W.; Koeppen, H.; et al. The molecular landscape of high-risk early breast cancer: Comprehensive biomarker analysis of a phase III adjuvant population. NPJ Breast Cancer 2016, 2, 16022. [Google Scholar] [CrossRef]
- Hudis, C.A.; Barlow, W.E.; Costantino, J.P.; Gray, R.J.; Pritchard, K.I.; Chapman, J.A.W.; Sparano, J.A.; Hunsberger, S.; Enos, R.A.; Gelber, R.D. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: The STEEP system. J. Clin. Oncol. 2007, 25, 2127–2132. [Google Scholar] [CrossRef]
- Lee, K.F.; Simon, H.; Chen, H.; Bates, B.; Hung, M.C.; Hauser, C. Requirement for neuregulin receptor erbB2 in neural and cardiac development. Nature 1995, 378, 394–398. [Google Scholar] [CrossRef]
- Timolati, F.; Ott, D.; Pentassuglia, L.; Giraud, M.-N.; Perriard, J.-C.; Suter, T.M.; Zuppinger, C. Neuregulin-1 beta attenuates doxorubicin-induced alterations of excitation–contraction coupling and reduces oxidative stress in adult rat cardiomyocytes. J. Mol. Cell Cardiol. 2006, 41, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Piccart, M.; Procter, M.; Fumagalli, D.; de Azambuja, E.; Clark, E.; Ewer, M.S.; Restuccia, E.; Jerusalem, G.; Dent, S.; Reaby, L.; et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer in the APHINITY trial: 6 years’ follow-up. J. Clin. Oncol. 2021, 39, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Valachis, A.; Nearchou, A.; Polyzos, N.P.; Lind, P. Cardiac toxicity in breast cancer patients treated with dual HER2 blockade. Int. J. Cancer 2013, 133, 2245–2252. [Google Scholar] [CrossRef]
- Eiger, D.; Pondé, N.F.; Agbor-Tarh, D.; Moreno-Aspitia, A.; Piccart, M.; Hilbers, F.S.; Werner, O.; Chumsri, S.; Dueck, A.; Kroep, J.R.; et al. Long-term cardiac outcomes of patients with HER2-positive breast cancer treated in the adjuvant lapatinib and/or trastuzumab Treatment Optimization Trial. Br. J. Cancer 2020, 122, 1453–1460. [Google Scholar] [CrossRef]
- Hurvitz, S.A.; Martin, M.; Jung, K.H.; Huang, C.S.; Harbeck, N.; Valero, V.; Stroyakovskiy, D.; Wildiers, H.; Campone, M.; Boileau, J.F.; et al. Neoadjuvant trastuzumab emtansine and pertuzumab in human epidermal growth factor receptor 2-positive breast cancer: Three-year outcomes from the phase III KRISTINE study. J. Clin. Oncol. 2019, 37, 2206–2216. [Google Scholar] [CrossRef]
- Shao, Z.; Pang, D.; Yang, H.; Li, W.; Wang, S.; Cui, S.; Liao, N.; Wang, Y.; Wang, C.; Chang, Y.C.; et al. Efficacy, safety, and tolerability of pertuzumab, trastuzumab, and docetaxel for patients with early or locally advanced ERBB2-positive breast cancer in asia: The PEONY phase 3 randomized clinical trial. JAMA Oncol. 2020, 6, e193692. [Google Scholar] [CrossRef]
- Tan, A.R.; Im, S.-A.; Mattar, A.; Colomer, R.; Stroyakovskii, D.; Nowecki, Z.; De Laurentiis, M.; Pierga, J.-Y.; Jung, K.H.; Schem, C.; et al. Fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection plus chemotherapy in HER2-positive early breast cancer (FeDeriCa): A randomised, open-label, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2021, 22, 85–97. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Procter, M.; de Azambuja, E.; Zardavas, D.; Benyunes, M.; Viale, G.; Suter, T.; Arahmani, A.; Rouchet, N.; Clark, E.; et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. N. Engl. J. Med. 2017, 377, 122–131. [Google Scholar] [CrossRef]
- De Azambuja, E.; Eiger, D.; Procter, M.J.; Ponde, N.F.; Guillaume, S.; Parlier, D.; Lambertini, M.; Desmet, A.; Caballero, C.A.; Aguila, C.; et al. Cardiac safety of dual anti-HER2 blockade with pertuzumab plus trastuzumab (P+T) in the APHINITY trial. J. Clin. Oncol. 2021, 39, 510. [Google Scholar] [CrossRef]
- Ewer, M.S.; Herson, J. False positive cardiotoxicity events in cancer-related clinical trials: Risks related to imperfect noninvasive parameters. Chemotherapy 2018, 63, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G., Jr.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: Final analysis of the HERceptin Adjuvant (HERA) trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.H.; Sledge, G.; Geyer, C.E., Jr.; Martino, S.; Rastogi, P.; Gralow, J.; Swain, S.M.; et al. Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2–positive breast cancer: Planned joint analysis of overall survival from NSABP B-31 and NCCTG N9831. J. Clin. Oncol. 2014, 32, 3744–3752. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: A patient-level meta-analysis of 37,298 women with early breast cancer in 26 randomised trials. Lancet 2019, 393, 1440–1452. [Google Scholar] [CrossRef]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef]
- Van Ramshorst, M.S.; van der Voort, A.; van Werkhoven, E.D.; Mandjes, I.A.; Kemper, I.; Dezentjé, V.O.; Oving, I.M.; Honkoop, A.H.; Tick, L.W.; van de Wouw, A.J.; et al. Neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2 blockade for HER2-positive breast cancer (TRAIN-2): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1630–1640. [Google Scholar] [CrossRef]
- Van der Voort, A.; van Ramshorst, M.S.; van Werkhoven, E.D.; Mandjes, I.A.; Kemper, I.; Vulink, A.J.; Oving, I.M.; Honkoop, A.H.; Tick, L.W.; van de Wouw, A.J.; et al. Three-year follow-up of neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2-blockade for HER2-positive breast cancer (TRAIN-2): A randomized phase III trial. J. Clin. Oncol. 2020, 38, 501. [Google Scholar] [CrossRef]
- Cortes, J.; Gebhart, G.; Ruiz Borrego, M.; Stradella, A.; Bermejo, B.; Escrivá, S.; Calvo Martínez, L.; Ribelles, N.; Martinez, N.; Albacar, C.; et al. Chemotherapy (CT) de-escalation using an FDG-PET/CT (F-PET) and pathological response-adapted strategy in HER2[+] early breast cancer (EBC): PHERGain Trial. J. Clin. Oncol. 2020, 38, 503. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Breast Cancer. Version 2.2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 4 February 2022).
- Abou, R.; van der Bijl, P.; Bax, J.J.; Delgado, V. Global longitudinal strain: Clinical use and prognostic implications in contemporary practice. Heart 2020, 106, 1438–1444. [Google Scholar] [CrossRef]
- Cikes, M.; Solomon, S.D. Beyond ejection fraction: An integrative approach for assessment of cardiac structure and function in heart failure. Eur. Heart J. 2016, 37, 1642–1650. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cardiac Safety Event | Cohort A (ddAC ➝ TPH) | Cohort B (FEC ➝ DPH) |
|---|---|---|
| Class III/IV cardiac failure n, (%) | 3 (1.5) | 2 (1.0) |
| Neoadjuvant period 1 | 3 (1.5) | 0 |
| Adjuvant period 2 | 0 | 1 (0.5) |
| TFFU period 3 | 0 | 1 (0.5) |
| LVEF declines of ≥10% points from baseline to <50% n, (%); 4 (confirmed events n, (%)) 5 | 27 (13.6) | 24 (12.1) |
| Neoadjuvant period | 13 (6.5); (2 (1.0)) | 4 (2.0); (1 (0.5)) |
| Adjuvant period | 14 (7.7); (5 (2.8)) | 20 (10.5); (6 (3.2)) |
| TFFU period | 12 (6.0); (6 (3.0)) | 7 (3.5); (2 (1.0)) |
| Adjuvant Phase | ||
|---|---|---|
| Total number of patients, n (%) | Cohort A (ddAC ➝ TPH) n = 181 | Cohort B (FEC ➝ DPH) n = 190 |
| ≥1 AE | 171 (94.5) | 171 (90.0) |
| Total AEs, n | 1165 | 1237 |
| Deaths 1 | 0 | 0 |
| Withdrawn due to an AE | ||
| Pertuzumab or trastuzumab | 9 (5.0) | 11 (5.8) |
| Pertuzumab | 8 (4.4) | 10 (5.3) |
| Any study drug | 9 (5.0) | 11 (5.8) |
| Dose interruption/delay due to an AE | ||
| Pertuzumab or trastuzumab | 23 (12.7) | 30 (15.8) |
| Pertuzumab | 22 (12.2) | 28 (14.7) |
| Grade ≥ 3 AE | 23 (12.7) | 40 (21.1) |
| Serious AE | 15 (8.3) | 17 (8.9) |
| AE suspected to be caused by pertuzumab or trastuzumab | 105 (58.0) | 122 (64.2) |
| AE suspected to be caused by pertuzumab | 104 (57.5) | 120 (63.2) |
| AE during pertuzumab or trastuzumab infusion | 3 (1.7) | 1 (0.5) |
| AE during pertuzumab infusion | 2 (1.1) | 1 (0.5) |
| AEs to monitor | ||
| Heart failure | 0 | 1 (0.5) |
| Grade ≥ 3 | 0 | 0 |
| Ejection fraction decreased | 15 (8.3) | 20 (10.5) |
| Grade ≥ 3 | 5 (2.8) | 6 (3.2) |
| Diarrhea | 26 (14.4) | 45 (23.7) |
| Grade ≥ 3 | 0 | 2 (1.1) |
| Rash | 59 (32.6) | 61 (32.1) |
| Grade ≥ 3 | 0 | 2 (1.1) |
| Hypersensitivity/anaphylaxis | 2 (1.1) | 1 (0.5) |
| Grade ≥ 3 | 0 | 0 |
| Mucositis | 10 (5.5) | 23 (12.1) |
| Grade ≥ 3 | 1 (0.6) | 4 (2.1) |
| Leukopenia | 12 (6.6) | 12 (6.3) |
| Grade ≥ 3 | 0 | 1 (0.5) |
| Leukopenic infection | 0 | 1 (0.5) |
| Grade ≥ 3 | 0 | 0 |
| Febrile neutropenia | 0 | 0 |
| Grade ≥ 3 | 0 | 0 |
| Febrile neutropenic infection | 0 | 0 |
| Grade ≥ 3 | 0 | 0 |
| Interstitial lung disease | 1 (0.6) | 0 |
| Grade ≥ 3 | 0 | 0 |
| Infusion-related reactions 2 | 7 (3.9) | 14 (7.4) |
| Grade ≥ 3 | 0 | 1 (0.5) |
| Patients, n (%) | Cohort A (ddAC ➝ TPH) n = 199 | Cohort B (FEC ➝ DPH) n = 198 |
|---|---|---|
| Deaths | 7 (3.5) | 13 (6.6) |
| Disease recurrence | 0 | 1 (0.5) |
| Disease progression | 4 (2.0) | 12 (6.1) |
| Adverse event | 1 (0.5) | 0 |
| Other 1 | 2 (1.0) | 0 |
| Patients, n (%) | Cohort A (ddAC ➝ TPH) n = 199 | Cohort B (FEC ➝ DPH) n = 198 |
|---|---|---|
| Patients with a recurrence | 15 (7.5) | 25 (12.6) |
| Local recurrence | 2 (1.0) | 4 (2.0) |
| Ipsilateral after previous lumpectomy | 0 | 2 (1.0) |
| Ipsilateral after previous mastectomy | 1 (0.5) | 2 (1.0) |
| Regional recurrence | 2 (1.0) | 4 (2.0) |
| Ipsilateral internal mammary lymph nodes | 0 | 2 (1.0) |
| Ipsilateral axillary lymph nodes | 2 (1.0) | 2 (1.0) |
| Ipsilateral supraclavicular lymph nodes | 0 | 1 (0.5) |
| Distant recurrence | 13 (6.5) | 13 (6.6) |
| Skin, subcutaneous tissue, and lymph nodes | 3 (1.5) | 2 (1.0) |
| Bone | 4 (2.0) | 1 (0.5) |
| Lung | 1 (0.5) | 3 (1.5) |
| Liver | 1 (0.5) | 1 (0.5) |
| CNS | 4 (2.0) | 7 (3.5) |
| Other | 2 (1.0) | 0 |
| Second primary invasive breast cancer | 2 (1.0) | 2 (1.0) |
| Right | 2 (1.0) | 0 |
| Left | 0 | 2 (1.0) |
| Second primary malignancy (nonbreast) | 1 (0.5) | 6 (3.0) |
| Lung cancer | 0 | 1 (0.5) |
| Colon cancer | 0 | 2 (1.0) |
| Non-Hodgkin’s lymphoma | 0 | 1 (0.5) |
| Other | 1 (0.5) | 2 (1.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, C.; Ewer, M.S.; Delaloge, S.; Ferrero, J.-M.; Colomer, R.; de la Cruz-Merino, L.; Werner, T.L.; Dadswell, K.; Verrill, M.; Eiger, D.; et al. BERENICE Final Analysis: Cardiac Safety Study of Neoadjuvant Pertuzumab, Trastuzumab, and Chemotherapy Followed by Adjuvant Pertuzumab and Trastuzumab in HER2-Positive Early Breast Cancer. Cancers 2022, 14, 2596. https://doi.org/10.3390/cancers14112596
Dang C, Ewer MS, Delaloge S, Ferrero J-M, Colomer R, de la Cruz-Merino L, Werner TL, Dadswell K, Verrill M, Eiger D, et al. BERENICE Final Analysis: Cardiac Safety Study of Neoadjuvant Pertuzumab, Trastuzumab, and Chemotherapy Followed by Adjuvant Pertuzumab and Trastuzumab in HER2-Positive Early Breast Cancer. Cancers. 2022; 14(11):2596. https://doi.org/10.3390/cancers14112596
Chicago/Turabian StyleDang, Chau, Michael S. Ewer, Suzette Delaloge, Jean-Marc Ferrero, Ramon Colomer, Luis de la Cruz-Merino, Theresa L. Werner, Katherine Dadswell, Mark Verrill, Daniel Eiger, and et al. 2022. "BERENICE Final Analysis: Cardiac Safety Study of Neoadjuvant Pertuzumab, Trastuzumab, and Chemotherapy Followed by Adjuvant Pertuzumab and Trastuzumab in HER2-Positive Early Breast Cancer" Cancers 14, no. 11: 2596. https://doi.org/10.3390/cancers14112596