
Definition of the Prognostic Role of MGMT Promoter Methylation Value by Pyrosequencing in Newly Diagnosed IDH Wild-Type Glioblastoma Patients Treated with Radiochemotherapy: A Large Multicenter Study
 , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
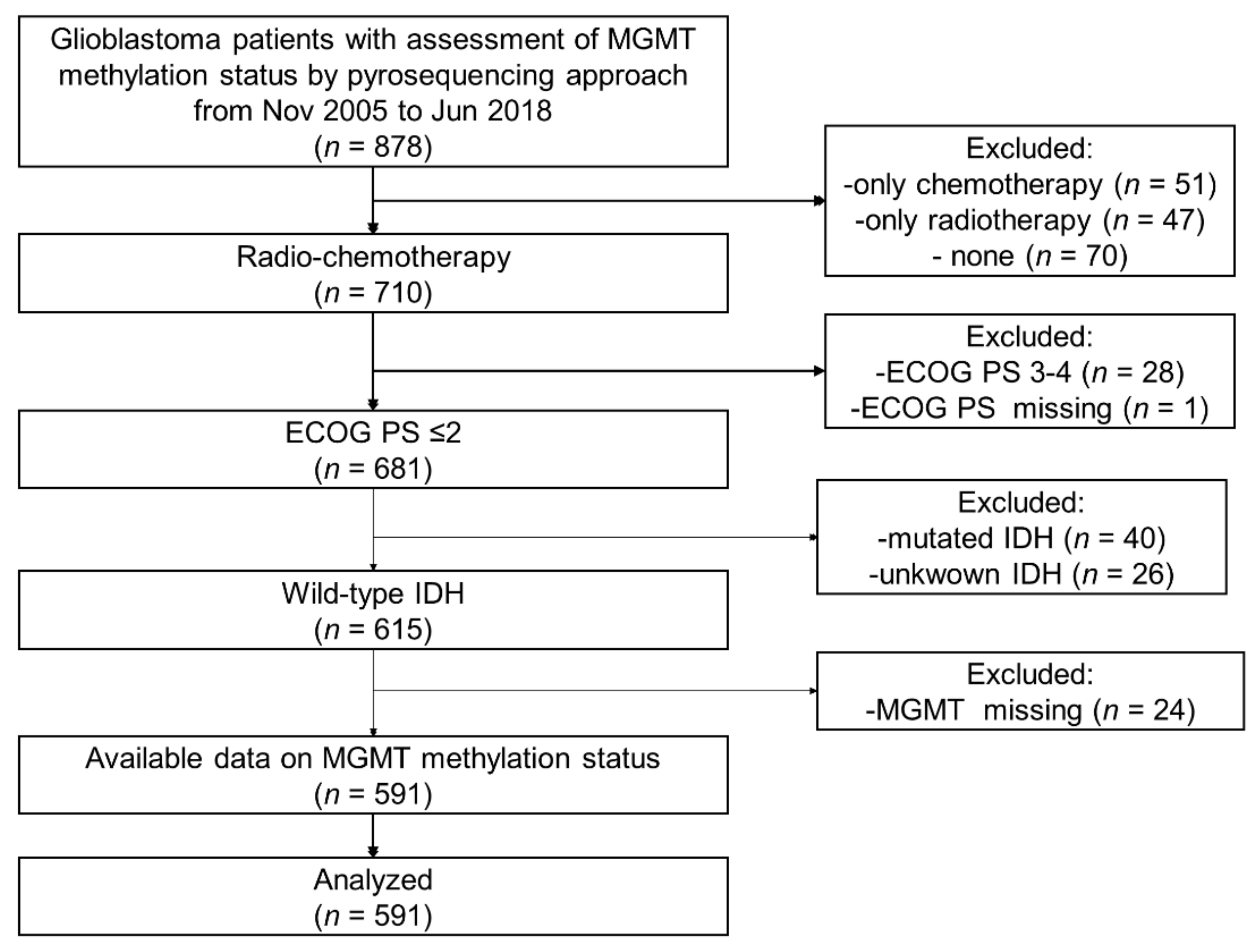
3.1. Patients
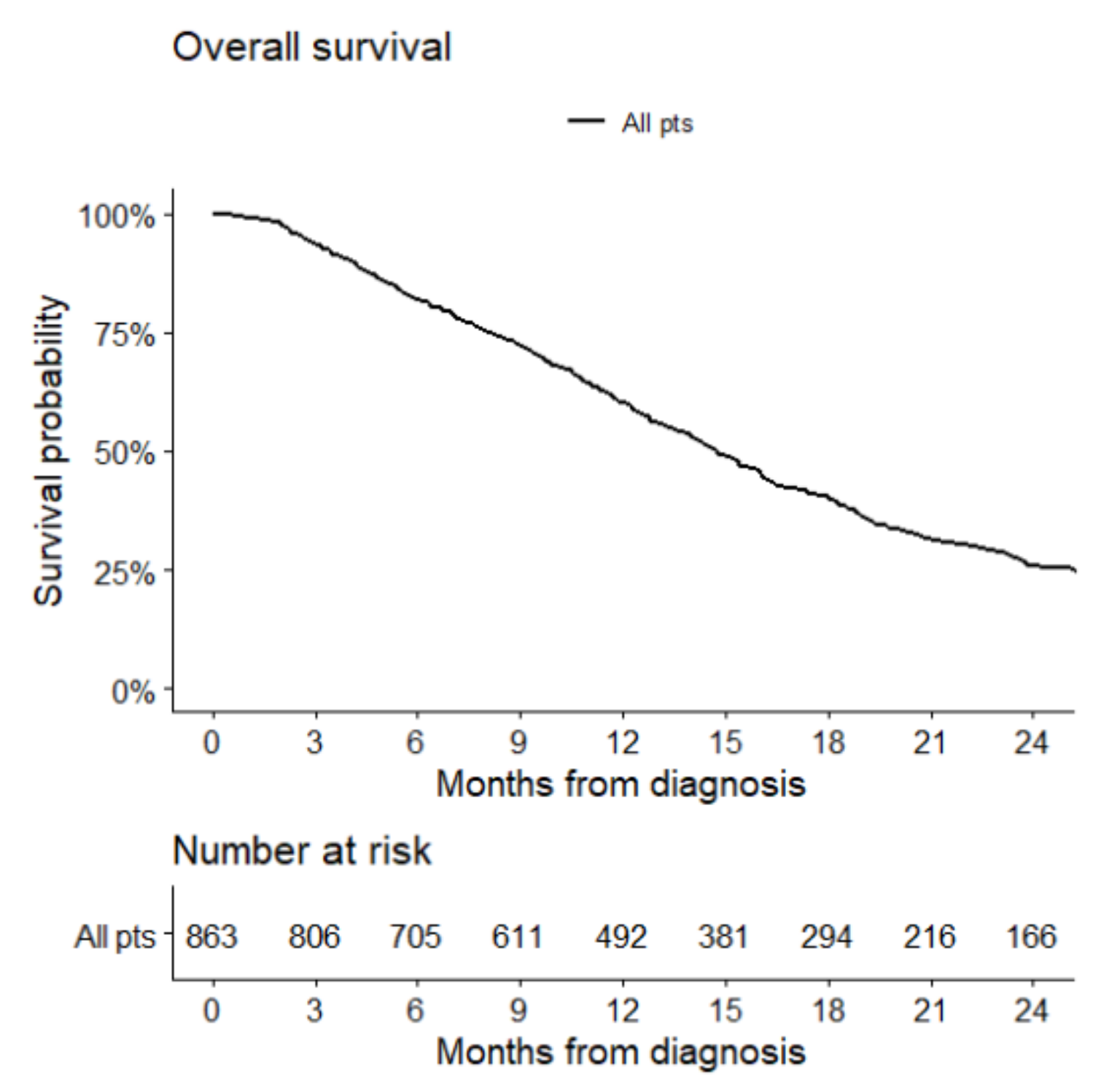
3.2. Overall Survival
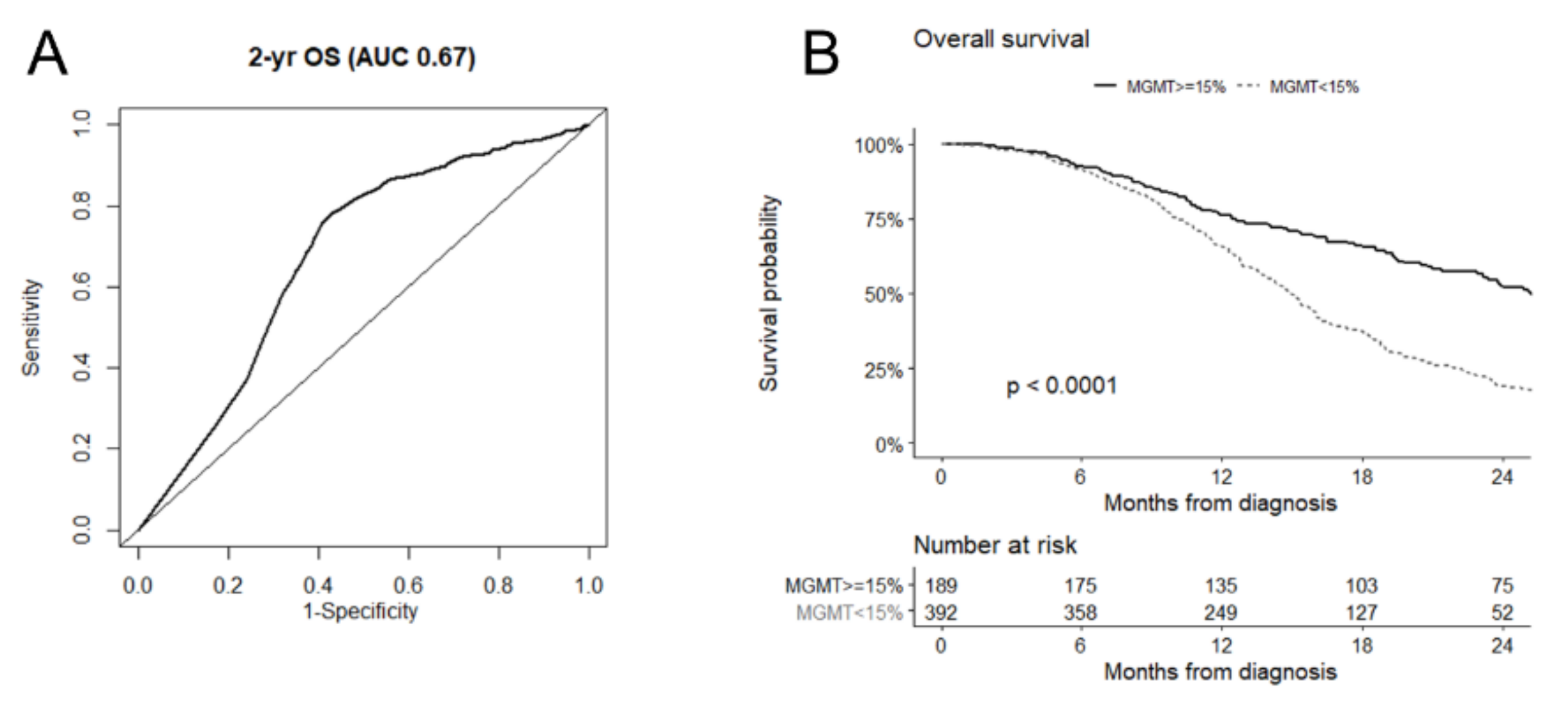
3.3. Prognostic Role of MGMT Promoter Methylation
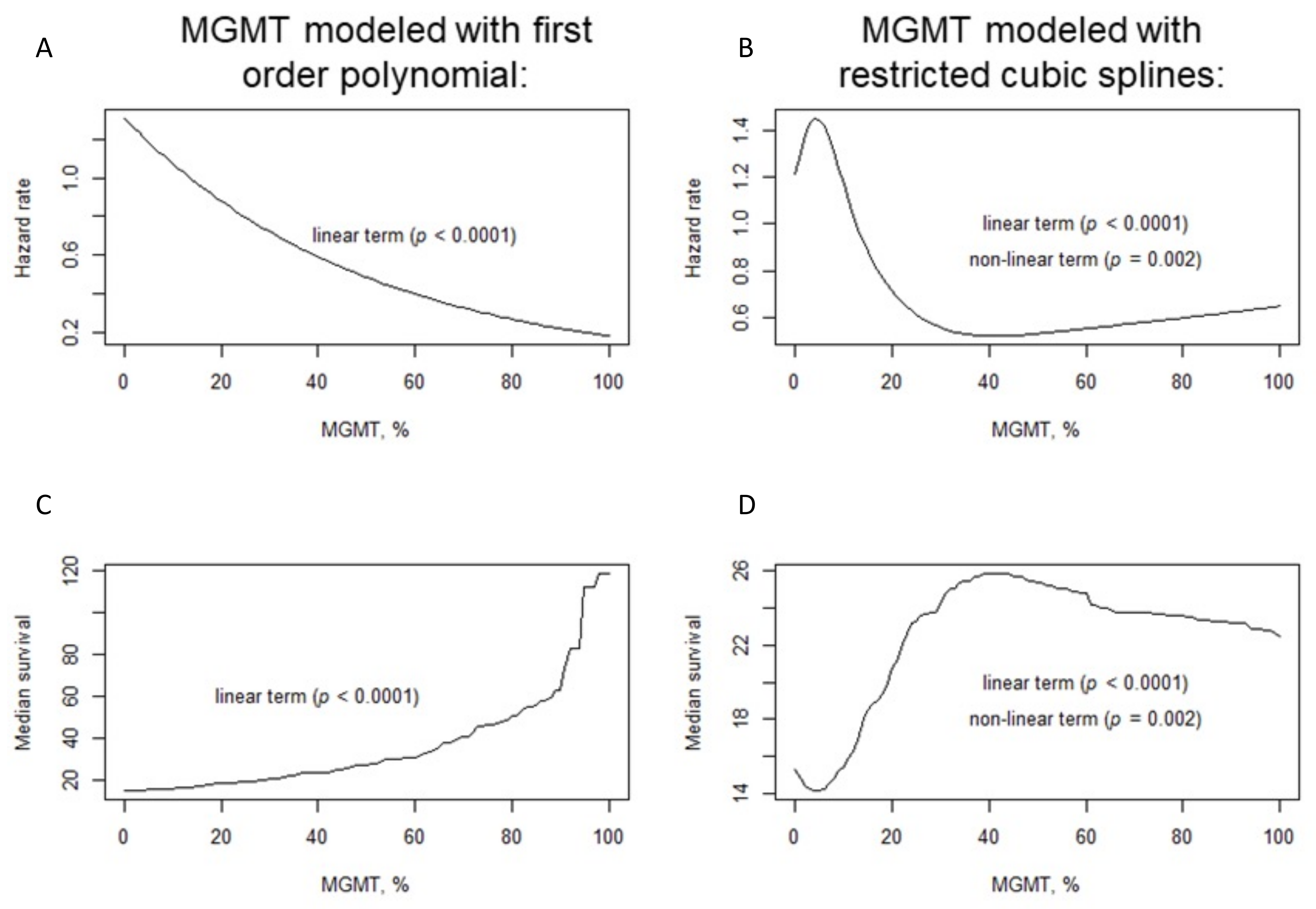
3.4. Non-Linear Association between Overall Survival and MGMT Promoter Methylation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| ECOG | Eastern Cooperative Oncology Group |
| EFS | Event-Free Survival |
| EORTC | European Organization for Research and Treatment of Cancer |
| FFPE | Formalin-Fixed Paraffin Embedded |
| GBM | Glioblastoma |
| HR | Hazard Ratio |
| IDH | Isocitrate Dehydrogenase |
| IQR | Interquartile Range |
| MGMT | O6-methylguanine (O6-MeG)-DNA Methyltransferase |
| MSP | Methylation-Specific PCR |
| NCIC | National Cancer Institute of Canada |
| NOA | Neuro-Oncology Working Group |
| OS | Overall Survival |
| PCR | Protein Chain Reaction |
| PS | Performance Status |
| PSQ | Pyrosequencing |
| ROC | Receiver Operating Characteristic |
| WHO | World Health Organization |
References
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013-2017. Neuro-Oncol. 2020, 22 (Suppl. S2), iv1–iv96. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Seyve, A.; Lozano-Sanchez, F.; Thomas, A.; Mathon, B.; Tran, S.; Mokhtari, K.; Giry, M.; Marie, Y.; Capelle, L.; Peyre, M.; et al. Initial surgical resection and long time to occurrence from initial diagnosis are independent prognostic factors in resected recurrent IDH wild-type glioblastoma. Clin. Neurol. Neurosurg. 2020, 196, 106006. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro-Oncol. 2020, 22, 1073–1113. Available online: https://academic.oup.com/neuro-oncology/article/doi/10.1093/neuonc/noaa106/5824407 (accessed on 19 July 2020). [CrossRef]
- Ostrom, Q.T.; Truitt, G.; Gittleman, H.; Brat, D.J.; Kruchko, C.; Wilson, R.; Barnholtz-Sloan, J.S. Relative survival after diagnosis with a primary brain or other central nervous system tumor in the National Program of Cancer Registries, 2004 to 2014. Neuro-Oncol. Pract. 2020, 7, 306–312. [Google Scholar] [CrossRef]
- Von Deimling, A.; Korshunov, A.; Hartmann, C. The Next Generation of Glioma Biomarkers: MGMT Methylation, BRAF Fusions and IDH1 Mutations: The Biomarkers MGMT, BRAF and IDH1. Brain Pathol. 2011, 21, 74–87. [Google Scholar] [CrossRef]
- Yu, W.; Zhang, L.; Wei, Q.; Shao, A. O6-Methylguanine-DNA Methyltransferase (MGMT): Challenges and New Opportunities in Glioma Chemotherapy. Front. Oncol. 2019, 9, 1547. [Google Scholar] [CrossRef]
- Ducray, F.; El Hallani, S.; Idbaih, A. Diagnostic and prognostic markers in gliomas. Curr. Opin. Oncol. 2009, 21, 537–542. [Google Scholar] [CrossRef]
- Hegi, M.E.; Diserens, A.C.; Gorlia, T.; Hamou, M.F.; de Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef]
- Berger, M.S.; Hervey-Jumper, S.; Wick, W. Astrocytic gliomas WHO grades II and III. Handb. Clin. Neurol. 2016, 134, 345–360. [Google Scholar]
- Wick, W.; Weller, M.; van den Bent, M.; Sanson, M.; Weiler, M.; von Deimling, A.; Plass, C.; Hegi, M.; Platten, M.; Reifenberger, G. MGMT testing-the challenges for biomarker-based glioma treatment. Nat. Rev. Neurol. 2014, 10, 372–385. [Google Scholar] [CrossRef]
- Christians, A.; Hartmann, C.; Benner, A.; Meyer, J.; von Deimling, A.; Weller, M.; Wick, W.; Weiler, M. Prognostic value of three different methods of MGMT promoter methylation analysis in a prospective trial on newly diagnosed glioblastoma. PLoS ONE 2012, 7, e33449. [Google Scholar] [CrossRef]
- Bienkowski, M.; Berghoff, A.S.; Marosi, C.; Wöhrer, A.; Heinzl, H.; Hainfellner, J.A.; Preusser, M. Clinical Neuropathology practice guide 5-2015: MGMT methylation pyrosequencing in glioblastoma: Unresolved issues and open questions. Clin. Neuropathol. 2015, 34, 250–257. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Preusser, M. Clinical neuropathology practice guide 06-2012: MGMT testing in elderly glioblastoma patients-yes, but how? Clin. Neuropathol. 2012, 31, 405–408. [Google Scholar] [CrossRef]
- Quillien, V.; Lavenu, A.; Sanson, M.; Legrain, M.; Dubus, P.; Karayan-Tapon, L.; Mosser, J.; Ichimura, K.; Figarella-Branger, D. Outcome-based determination of optimal pyrosequencing assay for MGMT methylation detection in glioblastoma patients. J. Neuro-Oncol. 2014, 116, 487–496. [Google Scholar] [CrossRef]
- Karayan-Tapon, L.; Quillien, V.; Guilhot, J.; Wager, M.; Fromont, G.; Saikali, S.; Etcheverry, A.; Hamlat, A.; Loussouarn, D.; Campion, L.; et al. Prognostic value of O6-methylguanine-DNA methyltransferase status in glioblastoma patients, assessed by five different methods. J. Neuro-Oncol. 2010, 97, 311–322. [Google Scholar] [CrossRef]
- Preusser, M.; Berghoff, A.S.; Manzl, C.; Filipits, M.; Weinhäusel, A.; Pulverer, W.; Dieckmann, K.; Widhalm, G.; Wöhrer, A.; Knosp, E.; et al. Clinical Neuropathology practice news 1-2014: Pyrosequencing meets clinical and analytical performance criteria for routine testing of MGMT promoter methylation status in glioblastoma. Clin. Neuropathol. 2014, 33, 6–14. [Google Scholar] [CrossRef]
- Berghoff, A.S.; Hainfellner, J.A.; Marosi, C.; Preusser, M. Assessing MGMT methylation status and its current impact on treatment in glioblastoma. CNS Oncol. 2015, 4, 47–52. [Google Scholar] [CrossRef]
- McAleenan, A.; Kelly, C.; Spiga, F.; Kernohan, A.; Cheng, H.-Y.; Dawson, S.; Schmidt, L.; Robinson, T.; Brandner, S.; Faulkner, C.L.; et al. Prognostic value of test(s) for O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation for predicting overall survival in people with glioblastoma treated with temozolomide. Cochrane Database Syst. Rev. 2021, 3. Available online: http://doi.wiley.com/10.1002/14651858.CD013316.pub2 (accessed on 25 March 2021). [CrossRef]
- Gurrieri, L.; De Carlo, E.; Gerratana, L.; De Maglio, G.; Macerelli, M.; Pisa, F.E.; Masiero, E.; Aprile, G.; Follador, A.; Puglisi, F.; et al. MGMT pyrosequencing-based cut-off methylation level and clinical outcome in patients with glioblastoma multiforme. Future Oncol. 2018, 14, 699–707. [Google Scholar] [CrossRef]
- Everhard, S.; Tost, J.; El Abdalaoui, H.; Crinière, E.; Busato, F.; Marie, Y.; Gut, I.G.; Sanson, M.; Mokhtari, K.; Laigle-Donadey, F.; et al. Identification of regions correlating MGMT promoter methylation and gene expression in glioblastomas. Neuro-Oncol. 2009, 11, 348–356. [Google Scholar] [CrossRef]
- Mulholland, S.; Pearson, D.M.; Hamoudi, R.A.; Malley, D.S.; Smith, C.M.; Weaver, J.M.J.; Jones, D.T.; Kocialkowski, S.; Bäcklund, L.M.; Collins, V.P.; et al. MGMT CpG island is invariably methylated in adult astrocytic and oligodendroglial tumors with IDH1 or IDH2 mutations. Int. J. Cancer 2012, 131, 1104–1113. [Google Scholar] [CrossRef]
- Collins, V.P.; Ichimura, K.; Di, Y.; Pearson, D.; Chan, R.; Thompson, L.C.; Gabe, R.; Brada, M.; Stenning, S.P. Prognostic and predictive markers in recurrent high grade glioma; results from the BR12 randomised trial. Acta Neuropathol. Commun. 2014, 2, 1–15. [Google Scholar] [CrossRef]
- Malley, D.S.; Hamoudi, R.A.; Kocialkowski, S.; Pearson, D.M.; Collins, V.P.; Ichimura, K. A distinct region of the MGMT CpG island critical for transcriptional regulation is preferentially methylated in glioblastoma cells and xenografts. Acta Neuropathol. 2011, 121, 651–661. [Google Scholar] [CrossRef]
- R Core Team. R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 1 January 2020).
- Malmstrom, A.; Gronberg, B.H.; Marosi, C.; Stupp, R.; Frappaz, D.; Schultz, H.; Abacioglu, U.; Tavelin, B.; Lhermitte, B.; Hegi, M.E.; et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: The Nordic randomised, phase 3 trial. Lancet Oncol. 2012, 13, 916–926. [Google Scholar] [CrossRef]
- Wick, W.; Platten, M.; Meisner, C.; Felsberg, J.; Tabatabai, G.; Simon, M.; Nikkhah, G.; Papsdorf, K.; Steinbach, J.P.; Sabel, M.; et al. Temozolomide chemotherapy alone versus radiotherapy alone for malignant astrocytoma in the elderly: The NOA-08 randomised, phase 3 trial. Lancet Oncol. 2012, 13, 707–715. [Google Scholar] [CrossRef]
- Wick, A.; Kessler, T.; Platten, M.; Meisner, C.; Bamberg, M.; Herrlinger, U.; Felsberg, J.; Weyerbrock, A.; Seidel, C.; Steinbach, J.P.; et al. P01.013 Long-term analyses of the NOA-08 randomized phase III trial of temozolomide versus radiotherapy for elderly patients with malignant astrocytomas. Neuro-Oncol. 2018, 20 (Suppl. S3), iii230–iii231. [Google Scholar] [CrossRef]
- Di Stefano, A.L.; Labussiere, M.; Lombardi, G.; Eoli, M.; Bianchessi, D.; Pasqualetti, F.; Farina, P.; Cuzzubbo, S.; Gallego-Perez-Larraya, J.; Boisselier, B.; et al. VEGFA SNP rs2010963 is associated with vascular toxicity in recurrent glioblastomas and longer response to bevacizumab. J. Neurooncol. 2015, 121, 499–504. [Google Scholar] [CrossRef]
- Birzu, C.; French, P.; Caccese, M.; Cerretti, G.; Idbaih, A.; Zagonel, V.; Lombardy, G. Recurrent Glioblastoma: From Molecular Landscape to New Treatment Perspectives. Cancers 2020, 13, 47. [Google Scholar] [CrossRef]
- Draaisma, K.; Chatzipli, A.; Taphoorn, M.; Kerkhof, M.; Weyerbrock, A.; Sanson, M.; Hoeben, A.; Lukacova, S.; Lombardi, G.; Leenstra, S.; et al. Molecular Evolution of IDH Wild-Type Glioblastomas Treated with Standard of Care Affects Survival and Design of Precision Medicine Trials: A Report From the EORTC 1542 Study. J. Clin. Oncol. 2020, 38, 81–99. [Google Scholar] [CrossRef]
- Malmström, A.; Łysiak, M.; Kristensen, B.W.; Hovey, E.; Henriksson, R.; Söderkvist, P. Do we really know who has an MGMT methylated glioma? Results of an international survey regarding use of MGMT analyses for glioma. Neuro-Oncol. Pract. 2020, 7, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Philteos, J.; Karmur, B.S.; Mansouri, A. MGMT Testing in Glioblastomas: Pitfalls and Opportunities. Am. J. Clin. Oncol. 2019, 42, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Wang, S.; Song, C.; Zha, Y.; Li, L. The prognostic value of MGMT promoter status by pyrosequencing assay for glioblastoma patients’ survival: A meta-analysis. World J. Surg. Oncol. 2016, 14, 261. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Gao, J.; Qin, C.; Liu, L.; Lin, H.; Shen, Y.; Gao, S.; Zhao, M.; Ding, H.; Pan, G. A High-Through Technique to Measure DNA Methylation. Genet. Epigenetics 2010, 3, GEG.S5035. [Google Scholar] [CrossRef]
- Mikeska, T.; Bock, C.; El-Maarri, O.; Hübner, A.; Ehrentraut, D.; Schramm, J.; Felsberg, J.; Kahl, P.; Büttner, R.; Pietsch, T.; et al. Optimization of quantitative MGMT promoter methylation analysis using pyrosequencing and combined bisulfite restriction analysis. J. Mol. Diagn. JMD 2007, 9, 368–381. [Google Scholar] [CrossRef]
- Nguyen, N.; Redfield, J.; Ballo, M.; Michael, M.; Sorenson, J.; Dibaba, D.; Wan, J.; Ramos, G.D.; Pandey, M. Identifying the optimal cutoff point for MGMT promoter methylation status in glioblastoma. CNS Oncol. 2021, 10, CNS74. [Google Scholar] [CrossRef]
- Dunn, J.; Baborie, A.; Alam, F.; Joyce, K.; Moxham, M.; Sibson, R.; Crooks, D.; Husband, D.; Shenoy, A.; Brodbelt, A.; et al. Extent of MGMT promoter methylation correlates with outcome in glioblastomas given temozolomide and radiotherapy. Br. J. Cancer 2009, 101, 124–131. [Google Scholar] [CrossRef]
- Rapkins, R.W.; Wang, F.; Nguyen, H.N.; Cloughesy, T.F.; Lai, A.; Ha, W.; Nowak, A.K.; Hitchins, M.P.; McDonald, K.L. The MGMT promoter SNP rs16906252 is a risk factor for MGMT methylation in glioblastoma and is predictive of response to temozolomide. Neuro-Oncol. 2015, 17, 1589–1598. [Google Scholar] [CrossRef]
- Quillien, V.; Lavenu, A.; Karayan-Tapon, L.; Carpentier, C.; Labussière, M.; Lesimple, T.; Chinot, O.; Wager, M.; Honnorat, J.; Saikali, S.; et al. Comparative assessment of 5 methods (methylation-specific polymerase chain reaction, MethyLight, pyrosequencing, methylation-sensitive high-resolution melting, and immunohistochemistry) to analyze O6-methylguanine-DNA-methyltranferase in a series of 100 glioblastoma patients. Cancer 2012, 118, 4201–4211. [Google Scholar]
- Shen, D.; Liu, T.; Lin, Q.; Lu, X.; Wang, Q.; Lin, F.; Mao, W. MGMT promoter methylation correlates with an overall survival benefit in Chinese high-grade glioblastoma patients treated with radiotherapy and alkylating agent-based chemotherapy: A single-institution study. PLoS ONE 2014, 9, e107558. [Google Scholar] [CrossRef]
- Reifenberger, G.; Hentschel, B.; Felsberg, J.; Schackert, G.; Simon, M.; Schnell, O.; Westphal, M.; Wick, W.; Pietsch, T.; Loeffler, M.; et al. Predictive impact of MGMT promoter methylation in glioblastoma of the elderly. Int. J. Cancer 2012, 131, 1342–1350. [Google Scholar] [CrossRef]
- Li, M.; Dong, G.; Zhang, W.; Ren, X.; Jiang, H.; Yang, C.; Zhao, X.; Zhu, Q.; Li, M.; Chen, H.; et al. Combining MGMT promoter pyrosequencing and protein expression to optimize prognosis stratification in glioblastoma. Cancer Sci. 2021, 112, 3699–3710. [Google Scholar] [CrossRef]
- Hsu, C.-Y.; Ho, H.-L.; Lin, S.-C.; Chang-Chien, Y.-C.; Chen, M.-H.; Hsu, S.P.-C.; Yen, Y.S.; Guo, W.Y.; Ho, D.M. Prognosis of glioblastoma with faint MGMT methylation-specific PCR product. J. Neurooncol. 2015, 122, 179–188. [Google Scholar] [CrossRef]
- McDonald, K.L.; Rapkins, R.W.; Olivier, J.; Zhao, L.; Nozue, K.; Lu, D.; Tiwari, S.; Kuroiwa-Trzmielina, J.; Brewer, J.; Wheeler, H.R.; et al. The T genotype of the MGMT C>T (rs16906252) enhancer single-nucleotide polymorphism (SNP) is associated with promoter methylation and longer survival in glioblastoma patients. Eur. J. Cancer 2013, 49, 360–368. [Google Scholar] [CrossRef]
- Xie, H.; Tubbs, R.; Yang, B. Detection of MGMT promoter methylation in glioblastoma using pyrosequencing. Int. J. Clin Exp. Pathol. 2015, 8, 636–642. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Summary |
|---|---|
| n patients | 591 |
| Age at diagnosis, years a | 60 (52–67) |
| Females Males | 202 (34.1) 389 (65.9) |
| ECOG PS: 0 1 2 | 255 (43.2) 266 (45.0) 70 (11.8) |
| Type of surgery: b Radical Non-radical | 343 (58.2) 246 (41.8) |
| Second surgery | 98 (17.2) |
| Study | Samples | Material | Cut-Off (%) | CpGs |
|---|---|---|---|---|
| Our Study | 591 | FFPE | 15 | 75–84 |
| Dunn et al. [38] | 109 | Frozen-FFPE | 9, 29 | 72–83 |
| Rapkins et al. [39] | 303 | FFPE | 9 | 74–78 |
| Quillien et al. [40] | 100 | Frozen | 8 | 74–78 |
| Shen et al. [41] | 128 | Frozen | 10 | 72–83 |
| Mulholland et al. [22] | 182 | Frozen | 10 | 74–89 |
| Collins et al. [23] | 225 | FFPE | 10 | 74–89 |
| Reifenberger et al. [42] | 166 | Frozen | 8, 25 | 74–78 |
| Nguyen et al. [37] | 109 | FFPE | 21 | 74–78 |
| Li et al. [43] | 312 | FFPE | 5–11 | 74–81 |
| Hsu et al. [44] | 99 | FFPE | 8 | 76–79 |
| McDonald et al. [45] | 78 | FFPE | 8 | 74–78 |
| Xie et al. [46] | 43 | FFPE | 10 | 74–89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caccese, M.; Simonelli, M.; Villani, V.; Rizzato, S.; Ius, T.; Pasqualetti, F.; Russo, M.; Rudà, R.; Amoroso, R.; Bellu, L.; et al. Definition of the Prognostic Role of MGMT Promoter Methylation Value by Pyrosequencing in Newly Diagnosed IDH Wild-Type Glioblastoma Patients Treated with Radiochemotherapy: A Large Multicenter Study. Cancers 2022, 14, 2425. https://doi.org/10.3390/cancers14102425
Caccese M, Simonelli M, Villani V, Rizzato S, Ius T, Pasqualetti F, Russo M, Rudà R, Amoroso R, Bellu L, et al. Definition of the Prognostic Role of MGMT Promoter Methylation Value by Pyrosequencing in Newly Diagnosed IDH Wild-Type Glioblastoma Patients Treated with Radiochemotherapy: A Large Multicenter Study. Cancers. 2022; 14(10):2425. https://doi.org/10.3390/cancers14102425
Chicago/Turabian StyleCaccese, Mario, Matteo Simonelli, Veronica Villani, Simona Rizzato, Tamara Ius, Francesco Pasqualetti, Marco Russo, Roberta Rudà, Rosina Amoroso, Luisa Bellu, and et al. 2022. "Definition of the Prognostic Role of MGMT Promoter Methylation Value by Pyrosequencing in Newly Diagnosed IDH Wild-Type Glioblastoma Patients Treated with Radiochemotherapy: A Large Multicenter Study" Cancers 14, no. 10: 2425. https://doi.org/10.3390/cancers14102425