
Treatment-Related Adverse Events of Combination EGFR Tyrosine Kinase Inhibitor and Immune Checkpoint Inhibitor in EGFR-Mutant Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Study Objectives
2.4. Data Extraction
2.5. Assessment of Study Quality
2.6. Outcome Measures and Statistical Analysis
3. Results
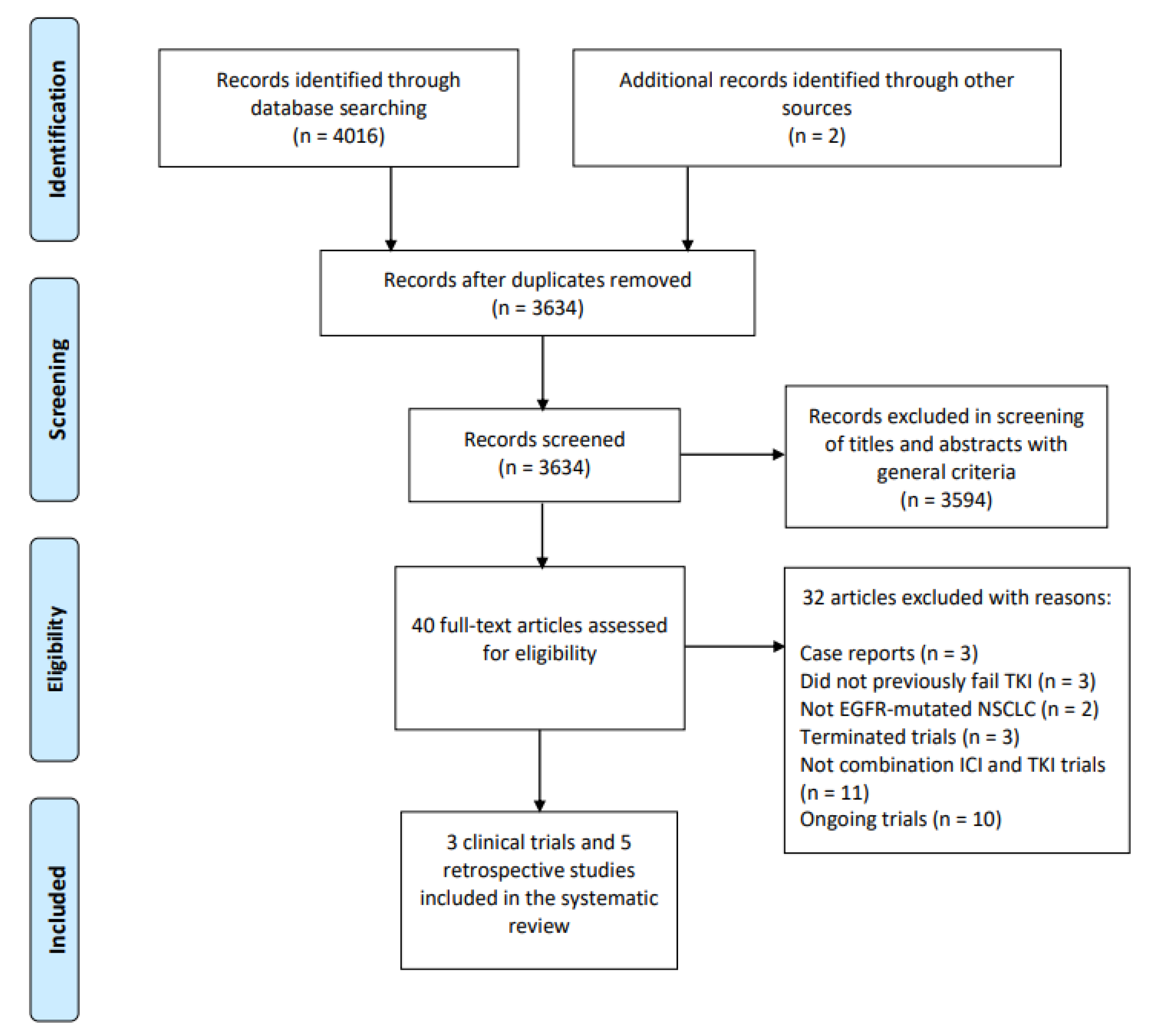
3.1. Search Strategy Results
3.2. Study Characteristics of Clinical Trials
3.3. Study Characteristics of Retrospective Studies
3.4. Nature of trAEs Reported in Retrospective Studies
3.5. Overall Incidence of trAEs
3.6. Incidence of Organ-Specific trAEs
3.7. Incidence of trAE Leading to Death and Drug Discontinuation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Soo, R.A.; Lim, S.M.; Syn, N.L.; Teng, R.; Soong, R.; Mok, T.S.; Cho, B.C. Immune checkpoint inhibitors in epidermal growth factor receptor mutant non-small cell lung cancer: Current controversies and future directions. Lung Cancer 2018, 115, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Au, J.S.-K.; Thongprasert, S.; Srinivasan, S.; Tsai, C.-M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.-C. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gahr, S.; Stoehr, R.; Geissinger, E.; Ficker, J.; Brueckl, W.; Gschwendtner, A.; Gattenloehner, S.; Fuchs, F.; Schulz, C.; Rieker, R. EGFR mutational status in a large series of Caucasian European NSCLC patients: Data from daily practice. Br. J. Cancer 2013, 109, 1821–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I. Gefitinib or chemotherapy for non–small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [Green Version]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): An open label, randomised phase 3 trial. Lancet Oncol. 2010, 11, 121–128. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Yang, J.; Hirsh, V.; Schuler, M.; Yamamoto, N.; O’Byrne, K.J.; Mok, T.S.-k.; Zazulina, V.; Shahidi, M.; Lungershausen, J.; Massey, D. Symptom control and quality of life in LUX-Lung 3: A phase III study of afatinib or cisplatin/pemetrexed in patients with advanced lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3342–3350. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Wu, Y.-L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.-P.; O’Byrne, K.; Feng, J. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Tan, E.-H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.-H.; Lee, K.H.; Lu, S. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): A phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): A randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef]
- Mok, T.S.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Lee, M.; Linke, R.; Rosell, R.; Corral, J. Improvement in overall survival in a randomized study that compared dacomitinib with gefitinib in patients with advanced non-small-cell lung cancer and EGFR-activating mutations. J. Clin. Oncol. 2018, 36, 2244–2250. [Google Scholar] [CrossRef]
- Goss, G.; Tsai, C.-M.; Shepherd, F.A.; Bazhenova, L.; Lee, J.S.; Chang, G.-C.; Crino, L.; Satouchi, M.; Chu, Q.; Hida, T. Osimertinib for pretreated EGFR Thr790Met-positive advanced non-small-cell lung cancer (AURA2): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2016, 17, 1643–1652. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Patel, J.D.; Socinski, M.A.; Garon, E.B.; Reynolds, C.H.; Spigel, D.R.; Olsen, M.R.; Hermann, R.C.; Jotte, R.M.; Beck, T.; Richards, D.A. PointBreak: A randomized phase III study of pemetrexed plus carboplatin and bevacizumab followed by maintenance pemetrexed and bevacizumab versus paclitaxel plus carboplatin and bevacizumab followed by maintenance bevacizumab in patients with stage IIIB or IV nonsquamous non–small-cell lung cancer. J. Clin. Oncol. 2013, 31, 4349. [Google Scholar] [CrossRef] [PubMed]
- Barlesi, F.; Scherpereel, A.; Rittmeyer, A.; Pazzola, A.; Ferrer Tur, N.; Kim, J.-H.; Ahn, M.-J.; Aerts, J.G.; Gorbunova, V.; Vikström, A. Randomized phase III trial of maintenance bevacizumab with or without pemetrexed after first-line induction with bevacizumab, cisplatin, and pemetrexed in advanced nonsquamous non–small-cell lung cancer: AVAPERL (MO22089). J. Clin. Oncol. 2013, 31, 3004–3011. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Cho, B.-C.; Kim, J.-H.; Mazières, J.; Vansteenkiste, J.; Lena, H.; Jaime, J.C.; Gray, J.E.; Powderly, J.; Chouaid, C. Durvalumab as third-line or later treatment for advanced non-small-cell lung cancer (ATLANTIC): An open-label, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 521–536. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- Reck, M.; Mok, T.S.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): Key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir. Med. 2019, 7, 387–401. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.-G.; Daniel, D.; McCune, S.; Mekhail, T. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Study of Pemetrexed + Platinum Chemotherapy with or without Pembrolizumab (MK-3475) in Adults with Tyrosine Kinase Inhibitor- (TKI)-Resistant Epidermal Growth Factor Receptor- (EGFR)-Mutated Metastatic Non-Squamous Non-Small Cell Lung Cancer (NSCLC) (MK-3475-789/KEYNOTE-789). Available online: https://clinicaltrials.gov/ct2/show/NCT03515837 (accessed on 22 March 2022).
- ABC-Lung: Atezolizumab, Bevacizumab and Chemotherapy in EGFR-Mutant Non-Small Cell Lung Carcinoma (ABC-Lung). Available online: https://clinicaltrials.gov/ct2/show/NCT04245085 (accessed on 3 March 2022).
- Atezolizumab and Bevacizumab in Epidermal Growth Factor Receptor (EGFR) Mutant Non-Small Cell Lung Cancer in Patients with Progressive Disease after Receiving Osimertinib. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04099836 (accessed on 3 March 2022).
- A Phase II Study of Atezolizumab in Combination with Bevacizumab, Carboplatin or Cisplatin, and Pemetrexed for EGFR-mutant Metastatic Non-Small Cell Lung Cancer Patients after Failure of EGFR Tyrosine Kinase Inhibitors. Available online: https://clinicaltrials.gov/show/NCT04147351 (accessed on 22 March 2022).
- Atezolizumab in Combination with Bevacizumab, Carboplatin and Pemetrexed for EGFR-mutant Metastatic NSCLC Patients after Failure of EGFR Tyrosine Kinase Inhibitors. Available online: https://clinicaltrials.gov/show/NCT03647956 (accessed on 22 March 2022).
- Non Small Cell Lung Cancer Trial of Durvalumab and Tremelimumab in Advanced Epidermal Growth Factor Receptor (EGFR) Mutant Disease. (ILLUMINATE). Available online: https://clinicaltrials.gov/ct2/show/NCT03994393 (accessed on 22 March 2022).
- Study For Patients with NSCLC EGFR Mutations (Del 19 or L858R +/− T790M). Available online: https://clinicaltrials.gov/ct2/show/NCT02349633 (accessed on 3 March 2022).
- Testing Afatinib in Combination with Pembrolizumab in Patients with Squamous Cell Carcinoma of the Lung. Available online: https://clinicaltrials.gov/show/NCT03157089 (accessed on 22 March 2022).
- A Study of Nivolumab in Advanced Non-Small Cell Lung Cancer (NSCLC). Available online: https://clinicaltrials.gov/show/NCT02574078 (accessed on 22 March 2022).
- Study of Efficacy and Safety of Nivolumab in Combination with EGF816 and of Nivolumab in Combination with INC280 in Patients with Previously Treated Non-Small Cell Lung Cancer. Available online: https://clinicaltrials.gov/show/NCT02323126 (accessed on 22 March 2022).
- Papadimitrakopoulou, V.; Wistuba, I.I.; Lee, J.J.; Tsao, A.S.; Kalhor, N.; Fossella, F.V.; Heymach, J.; Alden, C.M.; Gettinger, S.N.; Coombes, K.R. BATTLE-2 program: A biomarker-integrated targeted therapy study in previously treated patients with advanced non-small cell lung cancer (NSCLC). Am. Soc. Clin. Oncol. 2013, 34, 3638–3647. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.; Yang, J.-H.; Yu, H.; Kim, S.-W.; Saka, H.; Horn, L.; Goto, K.; Ohe, Y.; Mann, H.; Thress, K. TATTON: A multi-arm, phase Ib trial of osimertinib combined with selumetinib, savolitinib or durvalumab in EGFR-mutant lung cancer. Ann. Oncol. 2020, 31, 507–516. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.; Shepherd, F.A.; Kim, D.W.; Lee, G.W.; Lee, J.S.; Chang, G.C.; Lee, S.S.; Wei, Y.F.; Lee, Y.G.; Laus, G.; et al. Osimertinib Plus Durvalumab versus Osimertinib Monotherapy in EGFR T790M-Positive NSCLC following Previous EGFR TKI Therapy: CAURAL Brief Report. J. Thorac. Oncol. 2019, 14, 933–939. [Google Scholar] [CrossRef] [Green Version]
- Oshima, Y.; Tanimoto, T.; Yuji, K.; Tojo, A. EGFR-TKI-Associated Interstitial Pneumonitis in Nivolumab-Treated Patients with Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 1112–1115. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, A.J.; Arbour, K.C.; Rizvi, H.; Iqbal, A.N.; Gadgeel, S.M.; Girshman, J.; Kris, M.G.; Riely, G.J.; Yu, H.A.; Hellmann, M.D. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann. Oncol. 2019, 30, 839–844. [Google Scholar] [CrossRef]
- Kotake, M.; Murakami, H.; Kenmotsu, H.; Naito, T.; Takahashi, T. High incidence of interstitial lung disease following practical use of osimertinib in patients who had undergone immediate prior nivolumab therapy. Ann. Oncol. 2017, 28, 669–670. [Google Scholar] [CrossRef]
- Uchida, T.; Kaira, K.; Yamaguchi, O.; Mouri, A.; Shiono, A.; Miura, Y.; Hashimoto, K.; Nishihara, F.; Murayama, Y.; Kobayashi, K. Different incidence of interstitial lung disease according to different kinds of EGFR-tyrosine kinase inhibitors administered immediately before and/or after anti-PD-1 antibodies in lung cancer. Thorac. Cancer 2019, 10, 975–979. [Google Scholar] [CrossRef]
- Jänne, P.A.; Yang, J.C.; Kim, D.W.; Planchard, D.; Ohe, Y.; Ramalingam, S.S.; Ahn, M.J.; Kim, S.W.; Su, W.C.; Horn, L.; et al. AZD9291 in EGFR inhibitor–resistant non–small-cell lung cancer. N. Engl. J. Med. 2015, 372, 1689–1699. [Google Scholar] [CrossRef]
- Osa, A.; Uenami, T.; Koyama, S.; Fujimoto, K.; Okuzaki, D.; Takimoto, T.; Hirata, H.; Yano, Y.; Yokota, S.; Kinehara, Y. Clinical implications of monitoring nivolumab immunokinetics in non–small cell lung cancer patients. JCI Insight 2018, 3, e59125. [Google Scholar] [CrossRef] [PubMed]
- Lizotte, P.H.; Hong, R.L.; Luster, T.A.; Cavanaugh, M.E.; Taus, L.J.; Wang, S.; Dhaneshwar, A.; Mayman, N.; Yang, A.; Kulkarni, M.; et al. A high-throughput immune-oncology screen identifies EGFR inhibitors as potent enhancers of antigen-specific cytotoxic T-lymphocyte tumor cell killing. Cancer Immunol. Res. 2018, 6, 1511–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, Y.; Li, X.; Jiang, T.; Zhao, S.; Zhao, C.; Zhang, L.; Liu, X.; Shi, J.; Qiao, M.; Luo, J. EGFR-targeted therapy alters the tumor microenvironment in EGFR-driven lung tumors: Implications for combination therapies. Int. J. Cancer 2019, 145, 1432–1444. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 105906. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.-L.; Ahn, M.-J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.M.E.; et al. Osimertinib or Platinum–Pemetrexed in EGFR T790M–Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Nie, K.; Zhang, Z.; Zhang, C.; Geng, C.; Zhang, L.; Xu, X.; Liu, S.; Wang, S.; Zhuang, X.; Lan, K. Osimertinib compared docetaxel-bevacizumab as third-line treatment in EGFR T790M mutated non-small-cell lung cancer. Lung Cancer 2018, 121, 5–11. [Google Scholar] [CrossRef]
- Takakuwa, O.; Oguri, T.; Uemura, T.; Sone, K.; Fukuda, S.; Okayama, M.; Kanemitsu, Y.; Ohkubo, H.; Takemura, M.; Ito, Y. Osimertinib-induced interstitial lung disease in a patient with non-small cell lung cancer pretreated with nivolumab: A case report. Mol. Clin. Oncol. 2017, 7, 383–385. [Google Scholar] [CrossRef] [Green Version]
- Shinno, Y.; Goto, Y.; Ohuchi, M.; Hamada, A.; Nokihara, H.; Fujiwara, Y.; Ohe, Y. The Long Half-Life of Programmed Cell Death Protein 1 Inhibitors May Increase the Frequency of Immune-Related Adverse Events after Subsequent EGFR Tyrosine Kinase Inhibitor Therapy. JTO Clin. Res. Rep. 2020, 1, 100008. [Google Scholar] [CrossRef]
- Mamesaya, N.; Kenmotsu, H.; Takahashi, T. Successful osimertinib rechallenge in a patient with advanced non-small cell lung cancer following osimertinib-induced interstitial lung disease after treatment with nivolumab. Investig. New Drugs. 2017, 35, 839–841. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.-H.; Gadgeel, S.M.; Sequist, L.V.; Wu, C.-L.; Papadimitrakopoulou, V.A.; Su, W.-C.; Fiore, J.; Saraf, S.; Raftopoulos, H.; Patnaik, A. Pembrolizumab in combination with Erlotinib or Gefitinib as first-line therapy for advanced NSCLC with sensitizing EGFR mutation. J. Thorac. Oncol. 2019, 14, 553–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creelan, B.C.; Yeh, T.C.; Kim, S.W.; Nogami, N.; Kim, D.W.; Chow, L.Q.M.; Kanda, S.; Taylor, R.; Tang, W.; Tang, M.; et al. A Phase 1 study of gefitinib combined with durvalumab in EGFR TKI-naive patients with EGFR mutation-positive locally advanced/metastatic non-small-cell lung cancer. Br. J. Cancer 2021, 124, 383–390. [Google Scholar] [CrossRef]
- Levy, B.; Paz-Ares, L.; Bennouna, J.; Felip, E.; Abreu, D.R.; Isla, D.; Barlesi, F.; Molinier, O.; Madelaine, J.; Audigier-Valette, C. Afatinib with Pembrolizumab for Treatment of Patients with Locally Advanced/Metastatic Squamous Cell Carcinoma of the Lung: The LUX-Lung IO/KEYNOTE 497 Study Protocol. Clin. Lung Cancer 2019, 20, e407–e412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenschein, G.; Chandler, J.; Garon, E.B.; Waterhouse, D.; Goldman, J.W.; Gunuganti, V.K.; Boccia, R.; Spigel, D.; Glaspy, J.; Berry, D.A. PS01. 59: CheckMate 370: A Master Protocol of Phase 1/2 Studies of Nivolumab as Maintenance or First-Line±Standard-of-Care Therapies in Advanced NSCLC: Topic: Medical Oncology. J. Thorac. Oncol. 2016, 11, S307. [Google Scholar] [CrossRef] [Green Version]
- Leighl, N.B.; Hellmann, M.D.; Hui, R.; Carcereny, E.; Felip, E.; Ahn, M.J.; Eder, J.P.; Balmanoukian, A.S.; Aggarwal, C.; Horn, L.; et al. Pembrolizumab in patients with advanced non-small-cell lung cancer (KEYNOTE-001): 3-year results from an open-label, phase 1 study. Lancet Respir. Med. 2019, 7, 347–357. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Riudavets, M.; Naigeon, M.; Texier, M.; Dorta, M.; Barlesi, F.; Mazieres, J.; Varga, A.; Cassard, L.; Boselli, L.; Grivel, J.; et al. Gefitinib plus tremelimumab combination in refractory non-small cell lung cancer patients harbouring EGFR mutations: The GEFTREM phase I trial. Lung Cancer 2021, 166, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Reinmuth, N.; Orlov, S.; Fischer, J.R.; Sugawara, S.; Mandziuk, S.; Marquez-Medina, D.; Novello, S.; Takeda, Y.; Soo, R. ARCTIC: Durvalumab with or without tremelimumab as third-line or later treatment of metastatic non-small-cell lung cancer. Ann. Oncol. 2020, 31, 609–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pembrolizumab and Afatinib in Patients with Non-small Cell Lung Cancer with Resistance to Erlotinib. Available online: https://clinicaltrials.gov/ct2/show/NCT02364609 (accessed on 3 March 2022).
- A Phase 1b Study of Atezolizumab in Combination with Erlotinib or Alectinib in Participants with Non-Small Cell Lung Cancer (NSCLC). Available online: https://www.clinicaltrials.gov/ct2/show/NCT02013219 (accessed on 3 March 2022).
- Immune-Modulated Study of Selected Small Molecules (Gefitinib, AZD9291, or Selumetinib + Docetaxel) or a 1st Immune-Mediated Therapy (IMT.; Tremelimumab) with a Sequential Switch to a 2nd IMT (MEDI4736) in Patients with Locally Advanced or Metastatic Non-Small-Cell Lung Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02179671 (accessed on 3 March 2022).
- A Study Evaluating Platinum-Pemetrexed-Atezolizumab (+/-Bevacizumab) for Patients with Stage IIIB/IV Non-squamous Non-small Cell Lung Cancer with EGFR Mutations, ALK Rearrangement or ROS1 Fusion Progressing after Targeted Therapies (GFPC 06-2018). Available online: https://clinicaltrials.gov/ct2/show/NCT04042558 (accessed on 22 March 2022).
- A Study of Toripalimab+ Pemetrexed Plus Carboplatin in Patients with EGFR-mutation Positive and T790M Negative after Progression on EGFR-TKI Treatment (JS001). Available online: https://clinicaltrials.gov/ct2/show/NCT03513666 (accessed on 22 March 2022).
- Phase 2 Platform Study in Patients with Advanced Non-Small Lung Cancer Who Progressed on First-Line Osimertinib Therapy (ORCHARD). Available online: https://www.clinicaltrials.gov/ct2/show/NCT03944772 (accessed on 22 March 2022).
- Gettinger, S.; Hellmann, M.D.; Chow, L.Q.; Borghaei, H.; Antonia, S.; Brahmer, J.R.; Goldman, J.W.; Gerber, D.E.; Juergens, R.A.; Shepherd, F.A. Nivolumab plus erlotinib in patients with EGFR-mutant advanced NSCLC. J. Thorac. Oncol. 2018, 13, 1363–1372. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Nagashima, H.; Akiyama, M.; Utsumi, Y.; Sato, H.; Chiba, S.; Sugai, M.; Ube, K.; Mori, Y.; Watanabe, K.; et al. Treatment with immune checkpoint inhibitors after EGFR-TKIs in EGFR-mutated lung cancer. Thorac. Cancer 2022, 13, 386–393. [Google Scholar] [CrossRef]
- Gibbons, D.L.; Chow, L.; Kim, D.-W.; Kim, S.; Yeh, T.; Song, X.; Jiang, H.; Taylor, R.; Karakunnel, J.; Creelan, B. 57O Efficacy, safety and tolerability of MEDI4736 (durvalumab [D]), a human IgG1 anti-programmed cell death-ligand-1 (PD-L1) antibody, combined with gefitinib (G): A phase I expansion in TKI-naive patients (pts) with EGFR mutant NSCLC. J. Thorac. Oncol. 2016, 11, S79. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Trial | Author | Phase | Key Eligibility Criteria | Treatment Arms | Primary Objective | Treatment Line | Median Age (Range), Years) | Sample Size (Female%) | Grade 3/4 trAE | Discontinuation Due to Adverse Events | ORR | PFS (Months) | DOR (Months) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TATTON/NCT02143466 | Oxnard et al. | Ib | Advanced EGFR-mutant NSCLC and disease progression to a prior TKI | Arm 1: osimertinib 80 mg daily + durvalumab 3 mg/kg every 2 weeks (n = 10) Arm 2: osimertinib 80 mg daily + durvalumab 10 mg/kg every 2 weeks (dose escalation) | Safety, tolerability | ≥s | Arm 1: 67 (46–78) Arm 2: 58 (44–73) | Arm 1: 10 (70%) Arm 2: 13 (54%) | Arm 1: 60%, Arm 2: 38.5% | Arm 1: 30% a, 40% b Arm 2: 23.1% a, 38.5% b | Arm 1: 40%, Arm 2: 39% | NA | NA |
| CheckMate012/NCT01454102 | Gettinger et al. | I | EGFR-mutant chemotherapy-naïve, EGFR-TKI naïve or TKI treated stage IIIB/IV NSCLC | Nivolumab 3 mg/kg every 2 weeks and erlotinib 150 mg/d | Safety, tolerability | ≥s | 63 (41–80) | 21 (62%) | 24% | 10% | 15% | 48 | 5.1 c, 5.7 d |
| CAURAL/NCT02454933 | Yang et al. | III | EGFR T790M-positive, TKI-treated NSCLC | Arm 1: Osimertinib (80 mg once daily) Arm 2: osimertinib (80 mg once daily) + durvalumab (10 mg/kg IV every 2 weeks) | Safety, tolerability | ≥s | Arm 1: 65 (41–80) Arm2: 56 (41–78) | Arm 1: 17 (76%) Arm 2: 12 (50%) | 34% | 17% | 80% a, 64% e | NA | NA |
| Author | Year | Title | Study Design | Inclusion Criteria | EGFR Mutant (%) | Treatment Line | Treatment Arms | Time between ICI and TKI (Days) | Median Age (Range), Years | Sample Size (Female %) | Adverse Event Reported |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ito et al. | 2022 | Treatment with immune checkpoint inhibitors after EGFR-TKIs in EGFR-mutated lung cancer | Multiple institutions (Iwate Medical University Hospital, Iwate Prefectural Central Hospital, and Miyagi Cancer Center) retrospective study | EGFR mutant NSCLC previously treated with TKI | Ex19del/ L858R (25%) T790M (8%) | ≥s | G/E/Af/O followed by N/P/At | 139 (1–707) | 67 (38–80) | 25 (40%) | ILD |
| Schoenfeld et al. | 2019 | Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib | Single institution (Memorial Sloan Kettering Cancer Center) retrospective study | EGFR mutant NSCLC treated with PD-(L)1 blockers and EGFR-TKI irrespective of drug sequence | NA | s | Arm 1: N/P/At/D followed by O Arm 2: sequential osimertinib followed by N/P/At/D | Arm 1: 61 (12–1446) Arm 2: 5 (1–256) | Arm 1: 61 (30–79) Arm 2: 56 (36–85) | Arm 1: 41 (66%)Arm 2: 29 (83% | Severe immune related adverse events (4 G3 pneumonitis, 1 G3 colitis, 1 G4 hepatitis) |
| Uchida et al. | 2019 | Different incidence of interstitial lung disease according to different kinds of EGFR-tyrosine kinase inhibitors administered immediately before and/or after anti-PD-1 antibodies in lung cancer | Single institution (Saitama medical university international medical center) retrospective study | Advanced EGFR mutant patients who receive TKI immediately before and/or after N or P | Ex19del/ L858R (100%) | ≥s | O or Af before or after N or P | NA | 69 (44–80) | 26 (62%) | ILD |
| Oshima et al. | 2018 | EGFR–TKI-associated interstitial pneumonitis in nivolumab-treated patients with non–small cell lung cancer | Database study of US FDA Adverse Event Reporting System | EGFR mutant NSCLC | NA | NA | N/P/At in combination with Af/E/G/O | NA | Without N and TKI: 63 (NA) Without N, with TKI: 69 (NA). With N, without TKI: 66 (NA) With N and TKI: 64 (NA) | 20516 | ILD |
| Kotake et al. | 2017 | High incidence of interstitial lung disease following practical use of osimertinib in patients who had undergone immediate prior nivolumab therapy | Single institution (Shizuoka Cancer center) retrospective study | Advanced EGFR mutant NSCLC and disease progression on or after EGFR TKI | T790M (100%) | ≥s | N followed by O | In patients with ILD: 14 (7–28) In patients without ILD: 49 (28–119) | Median age NA In patients with ILD: 4 < 70 In patients without ILD: 10 < 70, 5 > 70 | 19 | ILD |
| trAEs | Combination of TKI and ICI | TKI Monotherapy | Odds Ratio (Combined vs. Monotherapy) | p |
|---|---|---|---|---|
| Overall | ||||
| Any grade | 100.0 (96.3, 100.0) a,b | 87.7 (68.1, 99.0) b,c | 1.27 (0.75, 1.66) | 0.077 |
| Grade ≥ 3 | 30.0 (12.0, 51.6) b,c | 13.8 (0.1, 40.4) b,c | 1.23 (0.85, 1.76) | 0.271 |
| Skin | ||||
| Any grade | 61.1 (47.3, 74.1) a | 42.6 (25.5, 61.2) c | 1.19 (0.95, 1.49) | 0.012 |
| Grade ≥ 3 | 1.7 (0.0, 8.5) a | 0.2 (0.0, 0.9) a | 1.13 (0.96, 1.29) | 0.082 |
| Gastrointestinal | ||||
| Any grade | 44.0 (21.2, 68.1) c | 40.3 (22.5, 59.5) c | 1.04 (0.77, 1.40) | 0.790 |
| Grade ≥ 3 | 3.6 (0.0, 11.6) a | 1.0 (0.2, 2.1) a | 1.13 (0.99, 1.02) | 0.076 |
| Interstitial lung disease (ILD) | ||||
| Any grade | 16.3 (6.7, 28.6) a | 2.8 (1.5, 4.3) a | 1.28 (1.11, 1.48) | 0.001 |
| Grade ≥ 3 | 4.4 (0.8, 9.8) a | 0.5 (0.0, 1.5) a | 1.16 (1.05, 1.28) | 0.003 |
| Sensitivity analysis (on studies of sample size >40) | ||||
| Any grade | 30.5 (23.1, 38.3) a | 3.4 (2.0, 5.0) a | 1.48 (1.34, 1.62) | < 0.001 |
| Grade ≥ 3 | 9.6 (2.7, 23.1) a | 1.0 (0.3, 2.1) a | 1.24 (1.06, 1.45) | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, D.W.-K.; Choi, H.C.-W.; Lee, V.H.-F. Treatment-Related Adverse Events of Combination EGFR Tyrosine Kinase Inhibitor and Immune Checkpoint Inhibitor in EGFR-Mutant Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2157. https://doi.org/10.3390/cancers14092157
Chan DW-K, Choi HC-W, Lee VH-F. Treatment-Related Adverse Events of Combination EGFR Tyrosine Kinase Inhibitor and Immune Checkpoint Inhibitor in EGFR-Mutant Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(9):2157. https://doi.org/10.3390/cancers14092157
Chicago/Turabian StyleChan, Daisy Wai-Ka, Horace Cheuk-Wai Choi, and Victor Ho-Fun Lee. 2022. "Treatment-Related Adverse Events of Combination EGFR Tyrosine Kinase Inhibitor and Immune Checkpoint Inhibitor in EGFR-Mutant Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis" Cancers 14, no. 9: 2157. https://doi.org/10.3390/cancers14092157