
The Significance of Systemic Inflammation Markers in Intrahepatic Recurrence of Early-Stage Hepatocellular Carcinoma after Curative Treatment

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
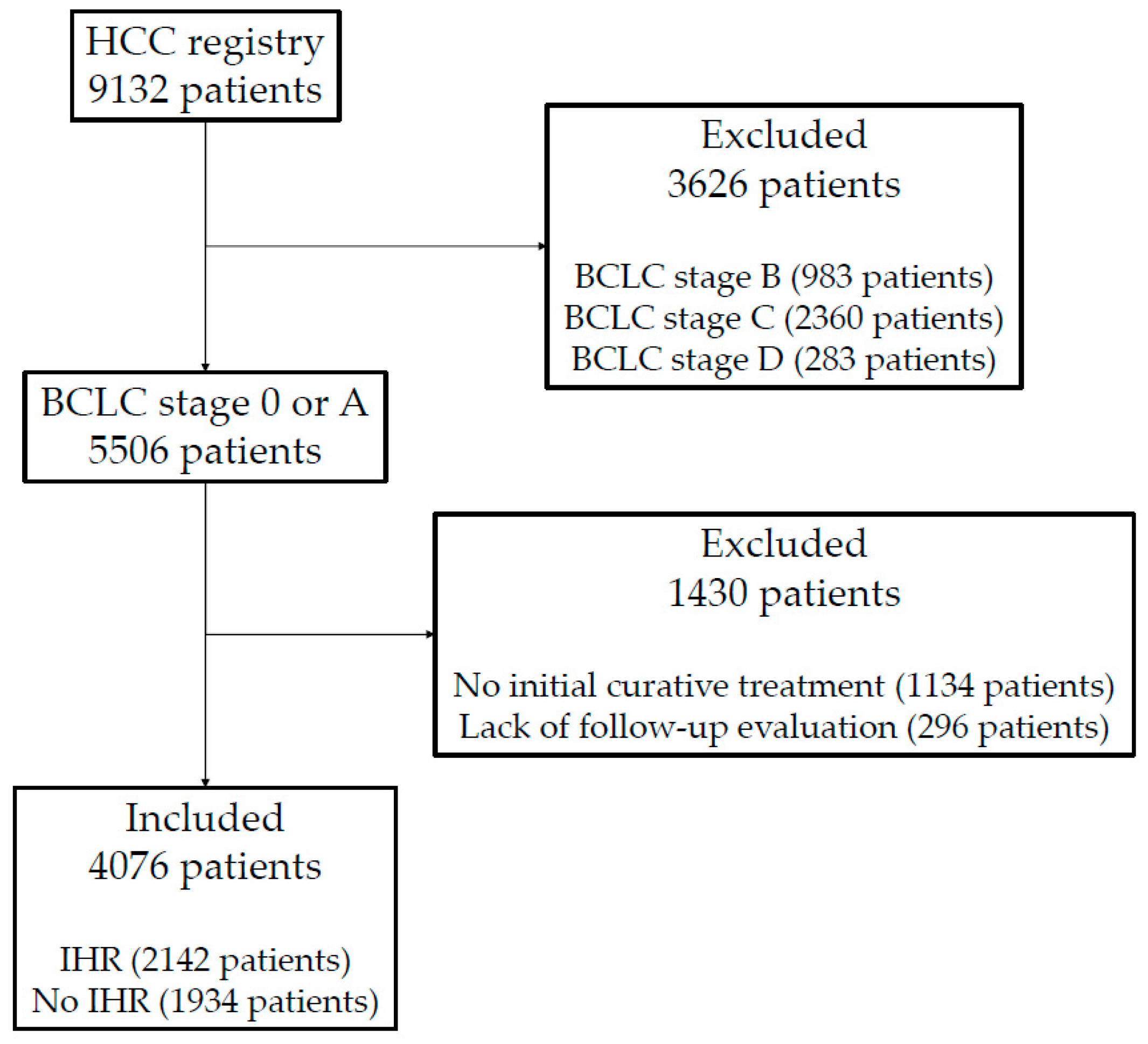
2.1. Patients
2.2. Data Collection
2.3. Follow-Up
2.4. Study Endpoints
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. 1), 4–13. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.C.; Preen, D.; Jeffrey, G.P.; Adams, L.A. The Evolving Epidemiology of Hepatocellular Carcinoma: A Global Perspective. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 765–779. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 871–873. [Google Scholar] [CrossRef] [PubMed]
- Dhir, M.; Melin, A.A.; Douaiher, J.; Lin, C.; Zhen, W.K.; Hussain, S.M.; Geschwind, J.F.; Doyle, M.B.; Abou-Alfa, G.K.; Are, C. A Review and Update of Treatment Options and Controversies in the Management of Hepatocellular Carcinoma. Ann. Surg. 2016, 263, 1112–1125. [Google Scholar] [CrossRef]
- Portolani, N.; Coniglio, A.; Ghidoni, S.; Giovanelli, M.; Benetti, A.; Tiberio, G.A.; Giulini, S.M. Early and late recurrence after liver resection for hepatocellular carcinoma: Prognostic and therapeutic implications. Ann. Surg. 2006, 243, 229–235. [Google Scholar] [CrossRef]
- Saito, A.; Toyoda, H.; Kobayashi, M.; Koiwa, Y.; Fujii, H.; Fujita, K.; Maeda, A.; Kaneoka, Y.; Hazama, S.; Nagano, H.; et al. Prediction of early recurrence of hepatocellular carcinoma after resection using digital pathology images assessed by machine learning. Mod. Pathol. 2021, 34, 417–425. [Google Scholar] [CrossRef]
- Wang, M.D.; Li, C.; Liang, L.; Xing, H.; Sun, L.Y.; Quan, B.; Wu, H.; Xu, X.F.; Wu, M.C.; Pawlik, T.M.; et al. Early and Late Recurrence of Hepatitis B Virus-Associated Hepatocellular Carcinoma. Oncologist 2020, 25, e1541–e1551. [Google Scholar] [CrossRef]
- Imamura, H.; Matsuyama, Y.; Tanaka, E.; Ohkubo, T.; Hasegawa, K.; Miyagawa, S.; Sugawara, Y.; Minagawa, M.; Takayama, T.; Kawasaki, S.; et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J. Hepatol. 2003, 38, 200–207. [Google Scholar] [CrossRef]
- Colecchia, A.; Schiumerini, R.; Cucchetti, A.; Cescon, M.; Taddia, M.; Marasco, G.; Festi, D. Prognostic factors for hepatocellular carcinoma recurrence. World J. Gastroenterol. 2014, 20, 5935–5950. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.; Karin, M. Obesity, inflammation, and liver cancer. J. Hepatol. 2012, 56, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mano, Y.; Shirabe, K.; Yamashita, Y.; Harimoto, N.; Tsujita, E.; Takeishi, K.; Aishima, S.; Ikegami, T.; Yoshizumi, T.; Yamanaka, T.; et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma: A retrospective analysis. Ann. Surg. 2013, 258, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Li, J.; Deng, H.; Li, H.; Su, C.; Guo, X. Neutrophil-to-lymphocyte ratio for the prognostic assessment of hepatocellular carcinoma: A systematic review and meta-analysis of observational studies. Oncotarget 2016, 7, 45283–45301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, W.K.; Chen, D.; Li, S.Q.; Fu, S.J.; Peng, B.G.; Liang, L.J. Prognostic significance of neutrophil-lymphocyte ratio in hepatocellular carcinoma: A meta-analysis. BMC Cancer 2014, 14, 117. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.I.; Park, H.C.; Yoo, G.S.; Paik, S.W.; Choi, M.S.; Kim, H.S.; Sohn, I.; Nam, H. Clinical Significance of Systemic Inflammation Markers in Newly Diagnosed, Previously Untreated Hepatocellular Carcinoma. Cancers 2020, 12, 1300. [Google Scholar] [CrossRef]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: A Meta-Analysis and Systematic Review. Cell Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Korean Liver Cancer, Association, and Goyang Korea National Cancer Center. 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Korean J. Radiol. 2019, 20, 1042–1113. [Google Scholar] [CrossRef] [Green Version]
- Korean Liver Cancer Study, Group, and Korea National Cancer Center. [Practice guidelines for management of hepatocellular carcinoma 2009]. Korean J. Hepatol. 2009, 15, 391–423. [Google Scholar] [CrossRef]
- Korean Liver Cancer Study, Group, and Korea National Cancer Center. 2014 KLCSG-NCC Korea Practice Guideline for the Management of Hepatocellular Carcinoma. Gut Liver 2015, 9, 267–317. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, M.; Shimizu, T.; Hirokawa, F.; Inoue, Y.; Komeda, K.; Asakuma, M.; Miyamoto, Y.; Takeshita, A.; Shibayama, Y.; Tanigawa, N. Clinicopathological risk factors for recurrence within one year after initial hepatectomy for hepatocellular carcinoma. Am. Surg. 2011, 77, 572–578. [Google Scholar] [CrossRef]
- Lu, X.; Zhao, H.; Yang, H.; Mao, Y.; Sang, X.; Miao, R.; Xu, Y.; Du, S.; Xu, H.; Chi, T.; et al. A prospective clinical study on early recurrence of hepatocellular carcinoma after hepatectomy. J. Surg. Oncol. 2009, 100, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Koh, K.C.; Choi, M.S.; Lee, J.H.; Yoo, B.C.; Paik, S.W.; Rhee, J.C.; Joh, J.W. Analysis of risk factors associated with early multinodular recurrences after hepatic resection for hepatocellular carcinoma. Am. J. Surg. 2006, 192, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Greig, P.D.; Gallinger, S.; Cattral, M.S.; Dixon, E.; Kim, R.D.; Taylor, B.R.; Grant, D.R.; Vollmer, C.M. Factors associated with early recurrence after resection for hepatocellular carcinoma and outcomes. J. Am. Coll. Surg. 2006, 202, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Ikoma, H.; Morimura, R.; Konishi, H.; Murayama, Y.; Komatsu, S.; Shiozaki, A.; Kuriu, Y.; Kubota, T.; Nakanishi, M.; et al. Optimal duration of the early and late recurrence of hepatocellular carcinoma after hepatectomy. World J. Gastroenterol. 2015, 21, 1207–1215. [Google Scholar] [CrossRef]
- Lausen, B.; Hothorn, T.; Bretz, F.; Schumacher, M. Assessment of optimal selected prognostic factors. Biometrical J. 2004, 46, 364–374. [Google Scholar] [CrossRef]
- Cite European Association for the Study of the Liver. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- NCCNguidelines. Hepatobiliary Cancers (Version 4.2021). Available online: https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf (accessed on 8 September 2021).
- Surveillance Group; Diagnosis Group; Staging Group; Surgery Group; Local Ablation Group; TACE/TARE/HAI Group; Target Therapy/Systemic Therapy Group; Radiotherapy Group; Prevention Group; Drafting Group. Management consensus guideline for hepatocellular carcinoma: 2016 updated by the Taiwan Liver Cancer Association and the Gastroenterological Society of Taiwan. J. Formos Med. Assoc. 2018, 117, 381–403. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Elinav, E.; Nowarski, R.; Thaiss, C.A.; Hu, B.; Jin, C.; Flavell, R.A. Inflammation-induced cancer: Crosstalk between tumours, immune cells and microorganisms. Nat. Rev. Cancer 2013, 13, 759–771. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Song, W.; Tian, C.; Wang, K.; Zhang, R.J.; Zou, S.B. The pretreatment lymphocyte to monocyte ratio predicts clinical outcome for patients with hepatocellular carcinoma: A meta-analysis. Sci. Rep. 2017, 7, 46601. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Yuan, B.Y.; Hu, Y.; Chen, G.W.; Zhang, L.; Zhao, X.M.; Chen, Y.X.; Zeng, Z.C. Pre/Post-Treatment Dynamic of Inflammatory Markers Has Prognostic Value in Patients with Small Hepatocellular Carcinoma Managed by Stereotactic Body Radiation Therapy. Cancer Manag. Res. 2019, 11, 10929–10937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.X.; Wang, Z.K.; Huang, Y.Q.; Xie, J.W.; Wang, J.B.; Lu, J.; Chen, Q.Y.; Lin, M.; Tu, R.H.; Huang, Z.N.; et al. Dynamic Changes in Pre- and Postoperative Levels of Inflammatory Markers and Their Effects on the Prognosis of Patients with Gastric Cancer. J. Gastrointest. Surg. 2021, 25, 387–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khunger, M.; Patil, P.D.; Khunger, A.; Li, M.; Hu, B.; Rakshit, S.; Basu, A.; Pennell, N.; Stevenson, J.P.; Elson, P.; et al. Post-treatment changes in hematological parameters predict response to nivolumab monotherapy in non-small cell lung cancer patients. PLoS ONE 2018, 13, e0197743. [Google Scholar] [CrossRef]
- Centonze, L.; De Carlis, R.; Vella, I.; Carbonaro, L.; Incarbone, N.; Palmieri, L.; Sgrazzutti, C.; Ficarelli, A.; Valsecchi, M.G.; Dello Iacono, U. From LI-RADS Classification to HCC Pathology: A Retrospective Single-Institution Analysis of Clinico-Pathological Features Affecting Oncological Outcomes after Curative Surgery. Diagnostics 2022, 12, 160. [Google Scholar] [CrossRef]
- Hartke, J.; Johnson, M.; Ghabril, M. The diagnosis and treatment of hepatocellular carcinoma. Semin. Diagn. Pathol. 2017, 34, 153–159. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Z.X.; Cao, Y.; Zhang, G.; Chen, W.B.; Jiang, C.P. Preoperative inflammation-based markers predict early and late recurrence of hepatocellular carcinoma after curative hepatectomy. Hepatobiliary Pancreat. Dis. Int. 2016, 15, 266–274. [Google Scholar] [CrossRef]
- Yu, J.I.; Park, H.C.; Yoo, G.S.; Choi, C.; Choi, M.S.; Nam, H.; Baek, S.Y.; Park, M. Clinical importance of the absolute count of neutrophils, lymphocytes, monocytes, and platelets in newly diagnosed hepatocellular carcinoma. Sci. Rep. 2021, 11, 2614. [Google Scholar] [CrossRef]
- Lin, C.W.; Chen, Y.S.; Lo, G.H.; Hsu, Y.C.; Hsu, C.C.; Wu, T.C.; Yeh, J.H.; Hsiao, P.; Hsieh, P.M.; Lin, H.Y.; et al. Comparison of overall survival on surgical resection versus transarterial chemoembolization with or without radiofrequency ablation in intermediate stage hepatocellular carcinoma: A propensity score matching analysis. BMC Gastroenterol. 2020, 20, 99. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Chen, M.; Mei, J.; Xu, L.; Guo, R.; Lin, X.; Zhang, Y.; Peng, Z. Transarterial Chemoembolization Combined with Radiofrequency Ablation in the Treatment of Stage B1 Intermediate Hepatocellular Carcinoma. J. Oncol. 2019, 2019, 6298502. [Google Scholar] [CrossRef]
- Shimose, S.; Tanaka, M.; Iwamoto, H.; Niizeki, T.; Shirono, T.; Aino, H.; Noda, Y.; Kamachi, N.; Okamura, S.; Nakano, M.; et al. Prognostic impact of transcatheter arterial chemoembolization (TACE) combined with radiofrequency ablation in patients with unresectable hepatocellular carcinoma: Comparison with TACE alone using decision-tree analysis after propensity score matching. Hepatol. Res. 2019, 49, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Bholee, A.K.; Peng, K.; Zhou, Z.; Chen, J.; Xu, L.; Zhang, Y.; Chen, M. Radiofrequency ablation combined with transarterial chemoembolization versus hepatectomy for patients with hepatocellular carcinoma within Milan criteria: A retrospective case-control study. Clin. Transl. Oncol. 2017, 19, 844–852. [Google Scholar] [CrossRef]
- Liu, Y.; Xue, D.; Tan, S.; Zhang, Q.; Yang, X.; Li, Y.; Zhu, B.; Niu, S.; Jiang, L.; Wang, X. Comparison of macrovascular invasion-free survival in early-intermediate hepatocellular carcinoma after different interventions: A propensity score-based analysis. J. Cancer 2019, 10, 4063–4071. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.X.; Fu, Y.Z.; Hu, D.D.; Long, Q.; Wang, J.C.; Xi, M.; Liu, S.L.; Xu, L.; Liu, M.Z.; Chen, M.S.; et al. Stereotactic Body Radiotherapy vs. Radiofrequency Ablation in the Treatment of Hepatocellular Carcinoma: A Meta-Analysis. Front. Oncol. 2020, 10, 1639. [Google Scholar] [CrossRef]
- Kim, T.H.; Koh, Y.H.; Kim, B.H.; Kim, M.J.; Lee, J.H.; Park, B.; Park, J.W. Proton beam radiotherapy vs. radiofrequency ablation for recurrent hepatocellular carcinoma: A randomized phase III trial. J. Hepatol. 2021, 74, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.K.; Cheung, T.-T.; Pang, H.H.; Wong, T.C.; Dai, J.W.; Ma, K.-W.; She, W.-H.; Kotewall, C.N.; Lo, C.-M. A simplified prediction model for early intrahepatic recurrence after hepatectomy for patients with unilobar hepatocellular carcinoma without macroscopic vascular invasion: An implication for adjuvant therapy and postoperative surveillance. Surg. Oncol. 2019, 30, 6–12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| IHR (+) n = 2142 | IHR (−) n = 1934 | p-Value | |
|---|---|---|---|
| Sex | <0.001 * | ||
| Male | 1720 (80.3%) | 1465 (75.7%) | |
| Female | 422 (19.7%) | 469 (24.3%) | |
| Age | 0.949 ** | ||
| Mean (± SD) | 57.2 (± 9.8) | 57.3 (±10.4) | |
| Viral status | <0.001 * | ||
| Viral | 1874 (87.5%) | 1605 (83.0%) | |
| Non-viral | 268 (12.5%) | 329 (17.0%) | |
| ALBI grade | <0.001 * | ||
| 1 | 1388 (64.8%) | 1515 (78.3%) | |
| 2 | 710 (33.1%) | 382 (19.8%) | |
| 3 | 44 (2.1%) | 37 (1.9%) | |
| Child-Pugh Class | 0.290 * | ||
| A | 1975 (92.2%) | 1800 (93.1%) | |
| B | 167 (7.8%) | 134 (6.9%) | |
| BCLC stage | 0.551 * | ||
| 0 | 777 (36.3%) | 719 (37.2%) | |
| A | 1365 (63.7%) | 1215 (62.8%) | |
| AFP | <0.001 *** | ||
| Median (IQR) | 16 (5.7–90.75) | 11 (3.8–86.55) | |
| n of tumor | <0.001 * | ||
| 1 | 1881 (87.8%) | 1797 (92.9%) | |
| 2 | 236 (11.0%) | 125 (6.5%) | |
| 3 | 25 (1.2%) | 12 (0.6%) | |
| Tumor size | 0.039 ** | ||
| Mean (± SD) | 2.6 (± 1.7) | 2.7 (±1.8) | |
| T stage | <0.001 * | ||
| 1 | 856 (39.9%) | 783 (40.5%) | |
| 2 | 1171 (54.7%) | 1096 (56.7%) | |
| 3 | 115 (5.4%) | 55 (2.8%) | |
| Primary treatment | <0.001 * | ||
| Liver transplantation | 4 (0.2%) | 65 (3.4%) | |
| Resection | 1020 (47.6%) | 1241 (64.2%) | |
| Ablative treatment | 1118 (52.2%) | 628 (32.5%) | |
| RFA | 1021 (47.7%) | 576 (29.8%) | |
| TACE + RFA | 79 (3.7%) | 43 (2.2%) | |
| TACE + radiotherapy | 13 (0.6%) | 7 (0.4%) | |
| Curative radiotherapy | 7 (0.2%) | 2 (0.1%) |
| Factors | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Sex (Male) | 1.193 (1.073–1.327) | 0.001 | 1.211 (1.084–1.353) | 0.001 |
| Age (>60) | 1.108 (1.014–1.210) | 0.024 | 1.241 (1.129–1.365) | <0.001 |
| Viral status (Viral) | 1.158 (1.018–1.316) | 0.023 | ||
| AST (>40) | 1.546 (1.420–1.684) | <0.001 | ||
| ALT (>40) | 1.295 (1.187–1.413) | <0.001 | ||
| ALBI grade (2–3) | 1.528 (1.398–1.670) | <0.001 | 1.157 (1.051–1.275) | 0.003 |
| Child-Pugh score (6–9) | 1.302 (1.176–1.441) | <0.001 | ||
| AFP (>100) | 1.036 (0.938–1.143) | 0.488 | ||
| n of tumor (2–3) | 1.562 (1.372–1.778) | <0.001 | 1.342 (1.177–1.532) | <0.001 |
| Tumor size (>5 cm) | 1.102 (0.957–1.268) | 0.184 | 1.314 (1.112–1.552) | 0.001 |
| BCLC stage (A) | 1.119 (1.025–1.222) | 0.012 | ||
| Platelet (≤150,000) | 1.493 (1.366–1.632) | <0.001 | ||
| ANC (≤2500) | 1.265 (1.162–1.377) | <0.001 | ||
| ALC (>1200) | 1.094 (0.985–1.215) | 0.097 | ||
| AMC (≤500) | 1.093 (0.993–1.203) | 0.073 | 1.206 (1.088–1.337) | <0.001 |
| NLR (>1.0) | 1.019 (0.921–1.127) | 0.718 | ||
| PLR (≤65.0) | 1.174 (1.078–1.278) | <0.001 | 1.297 (1.187–1.417) | <0.001 |
| LMR (≤4.0) | 1.082 (0.971–1.206) | 0.159 | ||
| ALRI (>15.0) | 1.612 (1.458–1.782) | <0.001 | 1.550 (1.384–1.735) | <0.001 |
| Change in NLR (>1.1 fold) | 2.294 (2.107–2.498) | <0.001 | 1.416 (1.280–1.566) | <0.001 |
| Change in PLR (>1 fold) | 2.514 (2.307–2.740) | <0.001 | 1.889 (1.706–2.092) | <0.001 |
| Change in LMR (<1 fold) | 2.252 (2.066–2.455) | <0.001 | 1.687 (1.530–1.860) | <0.001 |
| Change in ALRI (>1.1 fold) | 1.217 (1.118–1.325) | <0.001 | ||
| Factors | Early IHR | Late IHR | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Sex (Male) | 1.351 (1.120–1.630) | 0.001 | 1.426 (1.162–1.749) | 0.001 | 1.265 (1.058–1.513) | 0.010 | 1.397 (1.122–1.738) | 0.003 |
| Age (>60) | 0.936 (0.799–1.095) | 0.408 | 0.931 (0.799–1.084) | 0.355 | ||||
| Viral status (Viral) | 1.425 (1.144–1.776) | 0.002 | 1.441 (1.164–1.783) | 0.001 | ||||
| AST (>40) | 2.130 (1.821–2.490) | <0.001 | 1.673 (1.436–1.950) | <0.001 | ||||
| ALT (>40) | 1.684 (1.437–1.975) | <0.001 | 1.466 (1.254–1.713) | <0.001 | ||||
| ALBI grade (2–3) | 2.136 (1.807–2.524) | <0.001 | 1.456 (1.199–1.768) | <0.001 | 1.818 (1.542–2.142) | <0.001 | 1.605 (1.235–2.086) | <0.001 |
| Child-Pugh score (6–9) | 1.536 (1.273–1.853) | <0.001 | 1.374 (1.141–1.654) | 0.001 | 1.365 (1.019–1.829) | 0.037 | ||
| AFP (>100) | 1.224 (1.029–1.454) | 0.022 | 1.171 (0.981–1.399) | 0.081 | ||||
| n of tumor (2–3) | 2.196 (1.716–2.811) | <0.001 | 1.729 (1.314–2.274) | <0.001 | 1.495 (1.153–1.938) | 0.002 | ||
| Tumor size (>5 cm) | 1.089 (0.838–1.416) | 0.524 | 1.385 (1.035–1.855) | 0.029 | 0.867 (0.738–1.121) | 0.648 | ||
| BCLC stage (A) | 1.279 (1.089–1.503) | 0.003 | 0.870 (0.748–1.012) | 0.070 | ||||
| Platelet (≤150,000) | 1.797 (1.537–2.101) | <0.001 | 1.874 (1.610–2.181) | <0.001 | ||||
| ANC (≤2500) | 1.497 (1.284–1.745) | <0.001 | 1.386 (1.194–1.608) | <0.001 | 1.339 (1.088–1.647) | 0.006 | ||
| ALC (>1200) | 0.918 (0.759–1.110) | 0.378 | 0.911 (0.758–1.095) | 0.323 | ||||
| AMC (>500) | 1.028 (0.863–1.223) | 0.760 | 1.101 (0.931–1.301) | 0.261 | ||||
| NLR (> 1.0) | 0.996 (0.828–1.200) | 0.970 | 0.845 (0.709–1.006) | 0.058 | 1.430 (1.130–1.809) | 0.003 | ||
| PLR (≤ 65.0) | 1.232 (1.055–1.439) | 0.008 | 1.428 (1.190–1.714) | <0.001 | 1.769 (1.494–2.095) | <0.001 | 1.607 (1.326–1.946) | <0.001 |
| LMR (≤4.0) | 1.013 (0.836–1.227) | 0.897 | 1.096 (0.908–1.324) | 0.338 | ||||
| ALRI (>15.0) | 2.100 (1.783–2.472) | <0.001 | 2.304 (1.880–2.825) | <0.001 | 1.697 (1.423–2.025) | <0.001 | 1.990 (1.599–2.476) | <0.001 |
| Change in NLR (>1.1 fold) | 3.808 (3.233–4.486) | <0.001 | 2.165 (1.786–2.623) | <0.001 | 3.081 (2.626–3.613) | <0.001 | 1.977 (1.588–2.461) | <0.001 |
| Change in PLR (>1 fold) | 4.370 (3.714–5.141) | <0.001 | 2.940 (2.443–3.537) | <0.001 | 3.583 (3.063–4.191) | <0.001 | 2.832 (2.315–3.466) | <0.001 |
| Change in LMR (<1 fold) | 3.588 (3.060–4.207) | <0.001 | 2.543 (2.120–3.051) | <0.001 | 2.735 (2.348–3.186) | <0.001 | 2.345 (1.921–2.863) | <0.001 |
| Change in ALRI (>1.1 fold) | 1.332 (1.154–1.537) | <0.001 | 1.118 (0.953–1.312) | 0.171 | ||||
| Factors | IHRFS | OS | ||||
|---|---|---|---|---|---|---|
| 2-Year | 5-Year | p-Value | 2-Year | 5-Year | p-Value | |
| Pre-treatment PLR | <0.001 | 0.096 | ||||
| >65.0 | 69.2% | 52.0% | 93.8% | 81.1% | ||
| ≤65.0 | 67.0% | 45.8% | 93.3% | 81.8% | ||
| Pre-treatment ALRI | <0.001 | <0.001 | ||||
| ≤15.0 | 76.9% | 61.2% | 96.1% | 87.8% | ||
| >15.0 | 64.7% | 44.5% | 92.5% | 79.0% | ||
| Post-treatment change in NLR | <0.001 | <0.001 | ||||
| ≤1.1 fold | 76.0% | 60.0% | 95.6% | 86.1% | ||
| >1.1 fold | 54.7% | 31.0% | 89.8% | 73.6% | ||
| Post-treatment change in PLR | <0.001 | <0.001 | ||||
| ≤1 fold | 77.4% | 62.8% | 95.1% | 85.4% | ||
| >1 fold | 55.1% | 30.7% | 91.2% | 76.1% | ||
| Post-treatment change in LMR | <0.001 | <0.001 | ||||
| >1 fold | 77.1% | 61.5% | 95.4% | 86.0% | ||
| ≤1 fold | 57.4% | 34.7% | 91.2% | 76.1% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, B.K.; Park, H.C.; Yoo, G.S.; Choi, M.S.; Oh, J.H.; Yu, J.I. The Significance of Systemic Inflammation Markers in Intrahepatic Recurrence of Early-Stage Hepatocellular Carcinoma after Curative Treatment. Cancers 2022, 14, 2081. https://doi.org/10.3390/cancers14092081
Bae BK, Park HC, Yoo GS, Choi MS, Oh JH, Yu JI. The Significance of Systemic Inflammation Markers in Intrahepatic Recurrence of Early-Stage Hepatocellular Carcinoma after Curative Treatment. Cancers. 2022; 14(9):2081. https://doi.org/10.3390/cancers14092081
Chicago/Turabian StyleBae, Bong Kyung, Hee Chul Park, Gyu Sang Yoo, Moon Seok Choi, Joo Hyun Oh, and Jeong Il Yu. 2022. "The Significance of Systemic Inflammation Markers in Intrahepatic Recurrence of Early-Stage Hepatocellular Carcinoma after Curative Treatment" Cancers 14, no. 9: 2081. https://doi.org/10.3390/cancers14092081