
CANDIED: A Pan-Canadian Cohort of Immune Checkpoint Inhibitor-Induced Insulin-Dependent Diabetes Mellitus

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Data Collection
2.2. Oncological Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patient and ICI Therapy Characteristics
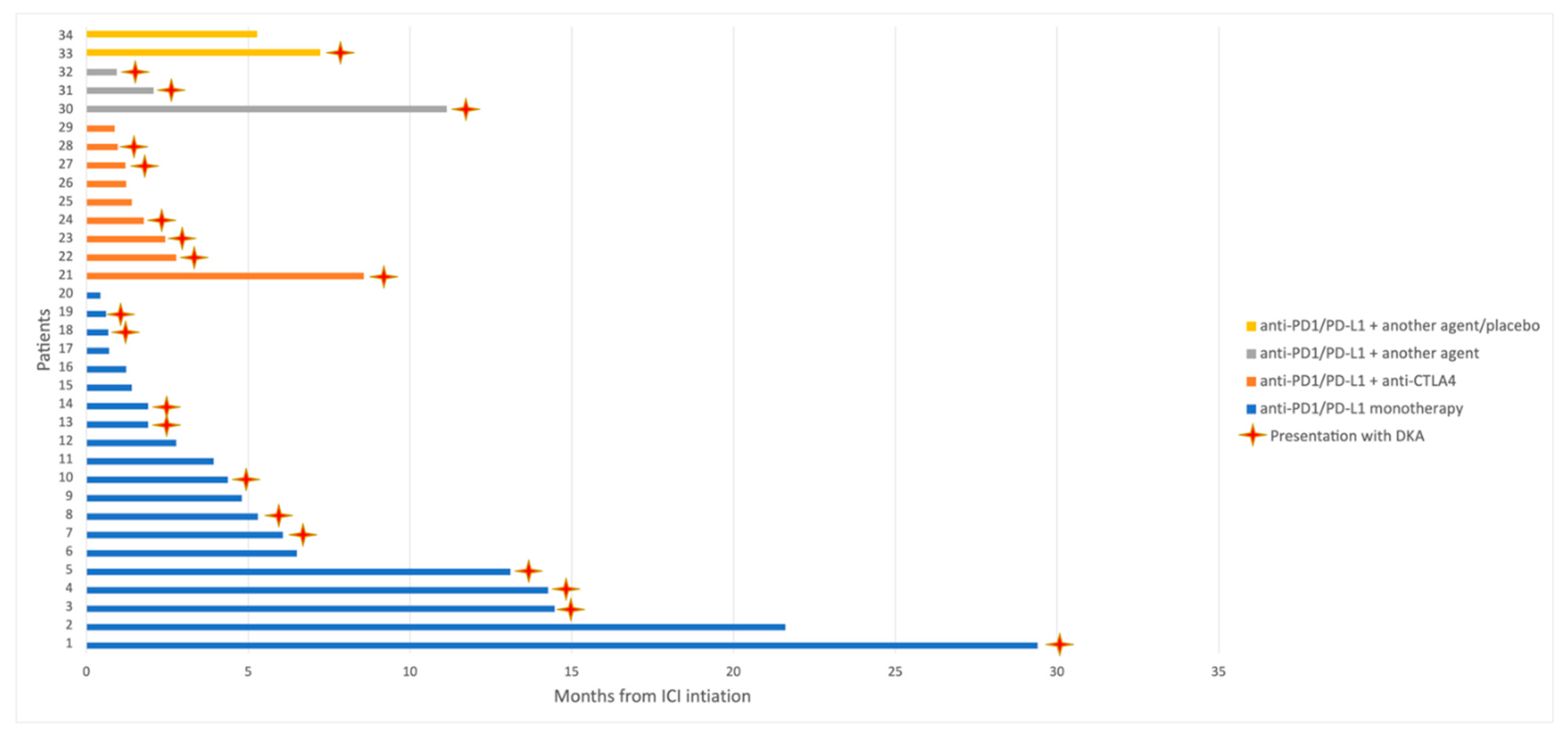
3.2. ICI-Induced IDDM
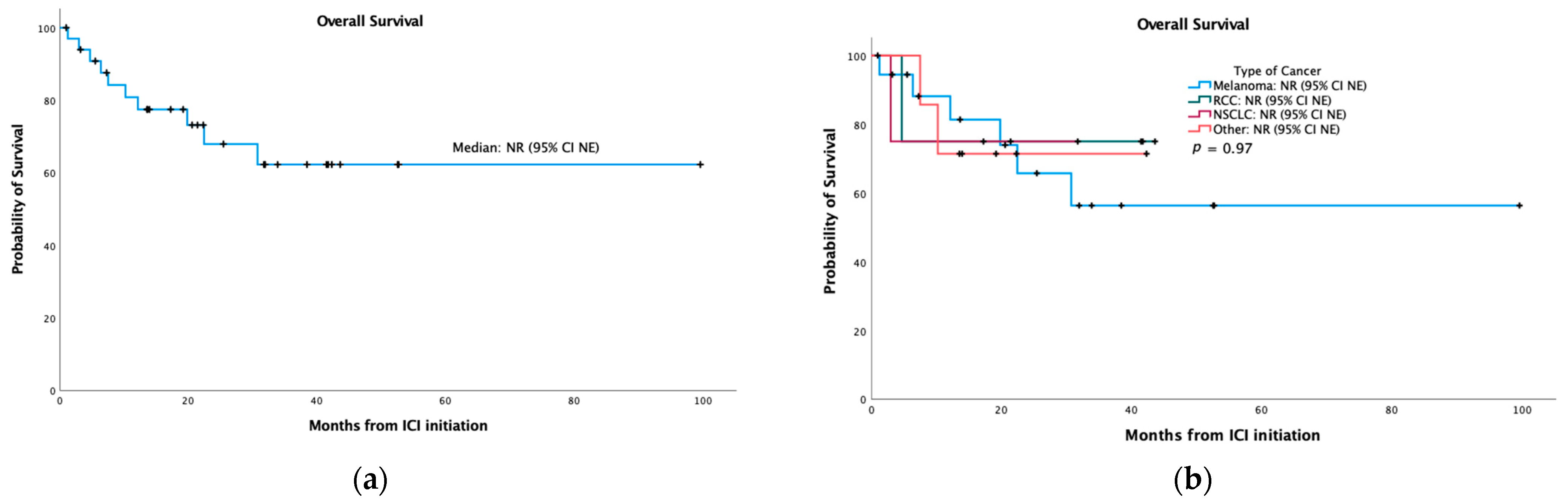
3.3. Response Assessment and Overall Survival
3.4. Princess Margaret Cancer Centre Cohort: Additional irAEs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Puzanov, I.; Diab, A.; Abdallah, K.; Bingham, C.O., 3rd; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; LeBoeuf, N.R.; et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.S.; Barroso-Sousa, R.; Tolaney, S.M.; Hodi, F.S.; Kaiser, U.B.; Min, L. Endocrine Toxicity of Cancer Immunotherapy Targeting Immune Checkpoints. Endocr. Rev. 2019, 40, 17–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barroso-Sousa, R.; Barry, W.T.; Garrido-Castro, A.C.; Hodi, F.S.; Min, L.; Krop, I.E.; Tolaney, S.M. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, A.; Haddox, C.; Block, M.; Kudva, Y.C. Immune checkpoint inhibitors: An emerging cause of insulin-dependent diabetes. BMJ Open Diabetes Res. Care 2019, 7, e000591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monami, M.; Naletto, L.; Nreu, B.; Dicembrini, I.; Sesti, G.; Mannucci, E. Immune checkpoints inhibitors and hyperglycemia: A Meta-analysis of randomized controlled trials. Diabetes Res. Clin. Pract. 2020, 162, 108115. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.J.; Salem, J.E.; Johnson, D.B.; Lebrun-Vignes, B.; Stamatouli, A.; Thomas, J.W.; Herold, K.C.; Moslehi, J.; Powers, A.C. Increased Reporting of Immune Checkpoint Inhibitor-Associated Diabetes. Diabetes Care 2018, 41, e150–e151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Zhou, H.; Zhang, Y.; Fang, W.; Yang, Y.; Huang, Y.; Zhang, L. Reporting of Immune Checkpoint Inhibitor Therapy–Associated Diabetes, 2015–2019. Diabetes Care 2020, 43, e79–e80. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gumus, M.; Mazieres, J.; Hermes, B.; Cay Senler, F.; Csoszi, T.; Fulop, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulieres, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulovic, S.; Demey, W.; Ullen, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Campos Bragagnoli, A.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Andre, T.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Stamatouli, A.M.; Quandt, Z.; Perdigoto, A.L.; Clark, P.L.; Kluger, H.; Weiss, S.A.; Gettinger, S.; Sznol, M.; Young, A.; Rushakoff, R.; et al. Collateral Damage: Insulin-Dependent Diabetes Induced with Checkpoint Inhibitors. Diabetes 2018, 67, 1471–1480. [Google Scholar] [CrossRef] [Green Version]
- Quandt, Z.; Young, A.; Anderson, M. Immune checkpoint inhibitor diabetes mellitus: A novel form of autoimmune diabetes. Clin. Exp. Immunol. 2020, 200, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Akturk, H.K.; Kahramangil, D.; Sarwal, A.; Hoffecker, L.; Murad, M.H.; Michels, A.W. Immune checkpoint inhibitor-induced Type 1 diabetes: A systematic review and meta-analysis. Diabet. Med. 2019, 36, 1075–1081. [Google Scholar] [CrossRef] [Green Version]
- Baden, M.Y.; Imagawa, A.; Abiru, N.; Awata, T.; Ikegami, H.; Uchigata, Y.; Oikawa, Y.; Osawa, H.; Kajio, H.; Kawasaki, E.; et al. Characteristics and clinical course of type 1 diabetes mellitus related to anti-programmed cell death-1 therapy. Diabetol. Int. 2019, 10, 58–66. [Google Scholar] [CrossRef]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 306. [Google Scholar] [CrossRef]
- Deshpande, R.P.; Sharma, S.; Watabe, K. The Confounders of Cancer Immunotherapy: Roles of Lifestyle, Metabolic Disorders and Sociological Factors. Cancers 2020, 12, 2938. [Google Scholar] [CrossRef] [PubMed]
- Dai, X.; Bu, X.; Gao, Y.; Guo, J.; Hu, J.; Jiang, C.; Zhang, Z.; Xu, K.; Duan, J.; He, S.; et al. Energy status dictates PD-L1 protein abundance and anti-tumor immunity to enable checkpoint blockade. Mol. Cell 2021, 81, 2317–2331.e6. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S15–S33. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef] [PubMed]
- Common Terminolgy Criteria for Adverse Events (CTCAE). Version 5.0. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 1 November 2021).
- Colli, M.L.; Hill, J.L.E.; Marroqui, L.; Chaffey, J.; Dos Santos, R.S.; Leete, P.; Coomans de Brachene, A.; Paula, F.M.M.; Op de Beeck, A.; Castela, A.; et al. PDL1 is expressed in the islets of people with type 1 diabetes and is up-regulated by interferons-alpha and-gamma via IRF1 induction. EBioMedicine 2018, 36, 367–375. [Google Scholar] [CrossRef] [Green Version]
- Delitala, A.P.; Fanciulli, G.; Zoledziewska, M.; Pitzalis, M.; Pusceddu, P.; Frongia, P.; Puddu, L.; Errigo, A.; Maioli, M.; Delitala, G.; et al. Allelic variant in CTLA4 is associated with thyroid failure and faster beta-cell exhaustion in latent autoimmune diabetes in adults. J. Diabetes 2015, 7, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Lin, S.; Yuan, X.; Lin, Z.; Huang, Z. HLA-DQB1 and HLA-DRB1 Variants Confer Susceptibility to Latent Autoimmune Diabetes in Adults: Relative Predispositional Effects among Allele Groups. Genes 2019, 10, 710. [Google Scholar] [CrossRef] [Green Version]
- Ashton, J.J.; Latham, K.; Beattie, R.M.; Ennis, S. Review article: The genetics of the human leucocyte antigen region in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2019, 50, 885–900. [Google Scholar] [CrossRef]
- Fawwad, A.; Govender, D.; Ahmedani, M.Y.; Basit, A.; Lane, J.A.; Mack, S.J.; Atkinson, M.A.; Henry Wasserfall, C.; Ogle, G.D.; Noble, J.A. Clinical features, biochemistry and HLA-DRB1 status in youth-onset type 1 diabetes in Pakistan. Diabetes Res. Clin. Pract. 2019, 149, 9–17. [Google Scholar] [CrossRef]
- Morris, D.L.; Fernando, M.M.; Taylor, K.E.; Chung, S.A.; Nititham, J.; Alarcon-Riquelme, M.E.; Barcellos, L.F.; Behrens, T.W.; Cotsapas, C.; Gaffney, P.M.; et al. MHC associations with clinical and autoantibody manifestations in European SLE. Genes Immun. 2014, 15, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Levet, S.; Charvet, B.; Bertin, A.; Deschaumes, A.; Perron, H.; Hober, D. Human Endogenous Retroviruses and Type 1 Diabetes. Curr. Diabetes Rep. 2019, 19, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchinson, J.A.; Kronenberg, K.; Riquelme, P.; Wenzel, J.J.; Glehr, G.; Schilling, H.L.; Zeman, F.; Evert, K.; Schmiedel, M.; Mickler, M.; et al. Virus-specific memory T cell responses unmasked by immune checkpoint blockade cause hepatitis. Nat. Commun. 2021, 12, 1439. [Google Scholar] [CrossRef]
- Nathan, D.M.; The DCCT/EDIC Research Group. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: Overview. Diabetes Care 2014, 37, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, D.M.; Turgeon, H.; Regan, S. Relationship between glycated haemoglobin levels and mean glucose levels over time. Diabetologia 2007, 50, 2239–2244. [Google Scholar] [CrossRef] [Green Version]
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [Green Version]
- Gauci, M.L.; Boudou, P.; Squara, P.A.; Delyon, J.; Allayous, C.; Mourah, S.; Resche-Rigon, M.; Lebbe, C.; Baroudjian, B.; Gautier, J.F.; et al. Checkpoint inhibitor treatment induces an increase in HbA1c in nondiabetic patients. Melanoma Res. 2019, 29, 328–332. [Google Scholar] [CrossRef]
- Akturk, H.K.; Michels, A.W. Adverse events associated with immune checkpoint inhibitors: A new era in autoimmune diabetes. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 187–193. [Google Scholar] [CrossRef]
- Marchand, L.; Thivolet, A.; Dalle, S.; Chikh, K.; Reffet, S.; Vouillarmet, J.; Fabien, N.; Cugnet-Anceau, C.; Thivolet, C. Diabetes mellitus induced by PD-1 and PD-L1 inhibitors: Description of pancreatic endocrine and exocrine phenotype. Acta Diabetol. 2019, 56, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Imagawa, A.; Hanafusa, T. Fulminant type 1 diabetes---An important subtype in East Asia. Diabetes Metab. Res. Rev. 2011, 27, 959–964. [Google Scholar] [CrossRef]
- Maddaloni, E.; Moretti, C.; Mignogna, C.; Buzzetti, R. Adult-onset autoimmune diabetes in 2020: An update. Maturitas 2020, 137, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Trinh, B.; Donath, M.Y.; Laubli, H. Successful Treatment of Immune Checkpoint Inhibitor-Induced Diabetes With Infliximab. Diabetes Care 2019, 42, e153–e154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galligan, A.; Krishnamurthy, B.; Kay, T.W. Comment on Trinh et al. Successful Treatment of Immune Checkpoint Inhibitor–Induced Diabetes With Infliximab. Diabetes Care 2019; 42: E153–e154. Diabetes Care 2020, 43, e10. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 15. Diabetes Care in the Hospital: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S211–S220. [Google Scholar] [CrossRef]
- American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44, S111–S124. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, C.; Fuca, G.; Ligorio, F.; Huber, V.; Vingiani, A.; Iannelli, F.; Raimondi, A.; Rinchai, D.; Frige, G.; Belfiore, A.; et al. Fasting-mimicking diet is safe and reshapes metabolism and antitumor immunity in cancer patients. Cancer Discov. 2021. [Google Scholar] [CrossRef] [PubMed]
- Teulings, H.E.; Limpens, J.; Jansen, S.N.; Zwinderman, A.H.; Reitsma, J.B.; Spuls, P.I.; Luiten, R.M. Vitiligo-like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: A systematic review and meta-analysis. J. Clin. Oncol. 2015, 33, 773–781. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Population | 34 Patients |
|---|---|
| Median Age (Range) | 60.5 (39–79) |
| Sex | n (%) |
| Male | 25 (74%) |
| Female | 9 (26%) |
| Primary Tumor | n (%) |
| Melanoma | 19 (56%) |
| Renal cell carcinoma | 4 (12%) |
| Non-small cell lung cancer | 4 (12%) |
| Other 1 | 7 (20%) |
| Comorbidities | n (%) |
| Hypertension | 10 (29%) |
| Dyslipidemia | 10 (29%) |
| Obesity | 3 (9%) |
| NIDDM | 3 (9%) |
| Pre-DM | 4 (12%) |
| Hypothyroidism | 5 (15%) |
| Autoimmune disease 2 | 5 (15%) |
| ICI Regimen | n (%) |
| Anti-PD1/PD-L1 monotherapy | 20 (59%) |
| Anti-PD1/PD-L1 + anti-CTLA4 | 9 (26%) |
| Anti-PD1/PD-L1 + another agent | 3 (9%) |
| Anti-PD1/PD-L1 + another agent/placebo | 2 (6%) |
| Line of Therapy | n (%) |
| First | 16 (47%) |
| Second | 7 (21%) |
| Third or beyond | 6 (17%) |
| Adjuvant | 4 (12%) |
| Consolidation | 1 (3%) |
| Symptom | n (%) |
|---|---|
| Polydipsia | 19 (56%) |
| Polyuria | 14 (41%) |
| Dehydration | 9 (26%) |
| Weight loss | 6 (17%) |
| Abdominal pain | 4 (12%) |
| Confusion | 4 (12%) |
| Immune-Related Adverse Events | All Grades a | G1 | G2 | G3 | G4 |
|---|---|---|---|---|---|
| AST increased | 7 | 6 | 0 | 1 | 0 |
| ALT increased | 8 | 5 | 3 | 0 | 0 |
| Troponin increased | 1 | 1 | 0 | 0 | 0 |
| CPK increased | 1 | 0 | 0 | 0 | 1 |
| Pancreatic enzymes decreased | 1 | 0 | 1 | 0 | 0 |
| Amylase increased | 1 | 0 | 1 | 0 | 0 |
| Lipase increased | 1 | 0 | 0 | 1 | 0 |
| Hypothyroidism | 6 | 0 | 6 | 0 | 0 |
| Hyperthyroidism | 3 | 2 | 1 | 0 | 0 |
| Diarrhea | 2 | 0 | 1 | 1 | 0 |
| Colitis | 2 | 0 | 2 | 0 | 0 |
| Rash | 3 | 1 | 2 | 0 | 0 |
| Pruritus | 1 | 1 | 0 | 0 | 0 |
| Vitiligo-like skin depigmentation | 2 | 0 | 2 | 0 | 0 |
| Hyperkeratosis | 1 | 0 | 0 | 1 | 0 |
| Guillain–Barré syndrome | 1 | 0 | 1 | 0 | 0 |
| Total | 41 | 16 | 20 | 4 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muniz, T.P.; Araujo, D.V.; Savage, K.J.; Cheng, T.; Saha, M.; Song, X.; Gill, S.; Monzon, J.G.; Grenier, D.; Genta, S.; et al. CANDIED: A Pan-Canadian Cohort of Immune Checkpoint Inhibitor-Induced Insulin-Dependent Diabetes Mellitus. Cancers 2022, 14, 89. https://doi.org/10.3390/cancers14010089
Muniz TP, Araujo DV, Savage KJ, Cheng T, Saha M, Song X, Gill S, Monzon JG, Grenier D, Genta S, et al. CANDIED: A Pan-Canadian Cohort of Immune Checkpoint Inhibitor-Induced Insulin-Dependent Diabetes Mellitus. Cancers. 2022; 14(1):89. https://doi.org/10.3390/cancers14010089
Chicago/Turabian StyleMuniz, Thiago P., Daniel V. Araujo, Kerry J. Savage, Tina Cheng, Moumita Saha, Xinni Song, Sabrina Gill, Jose G. Monzon, Debjani Grenier, Sofia Genta, and et al. 2022. "CANDIED: A Pan-Canadian Cohort of Immune Checkpoint Inhibitor-Induced Insulin-Dependent Diabetes Mellitus" Cancers 14, no. 1: 89. https://doi.org/10.3390/cancers14010089