
Exploring the Performance of Ultrasound Risk Stratification Systems in Thyroid Nodules of Pediatric Patients

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
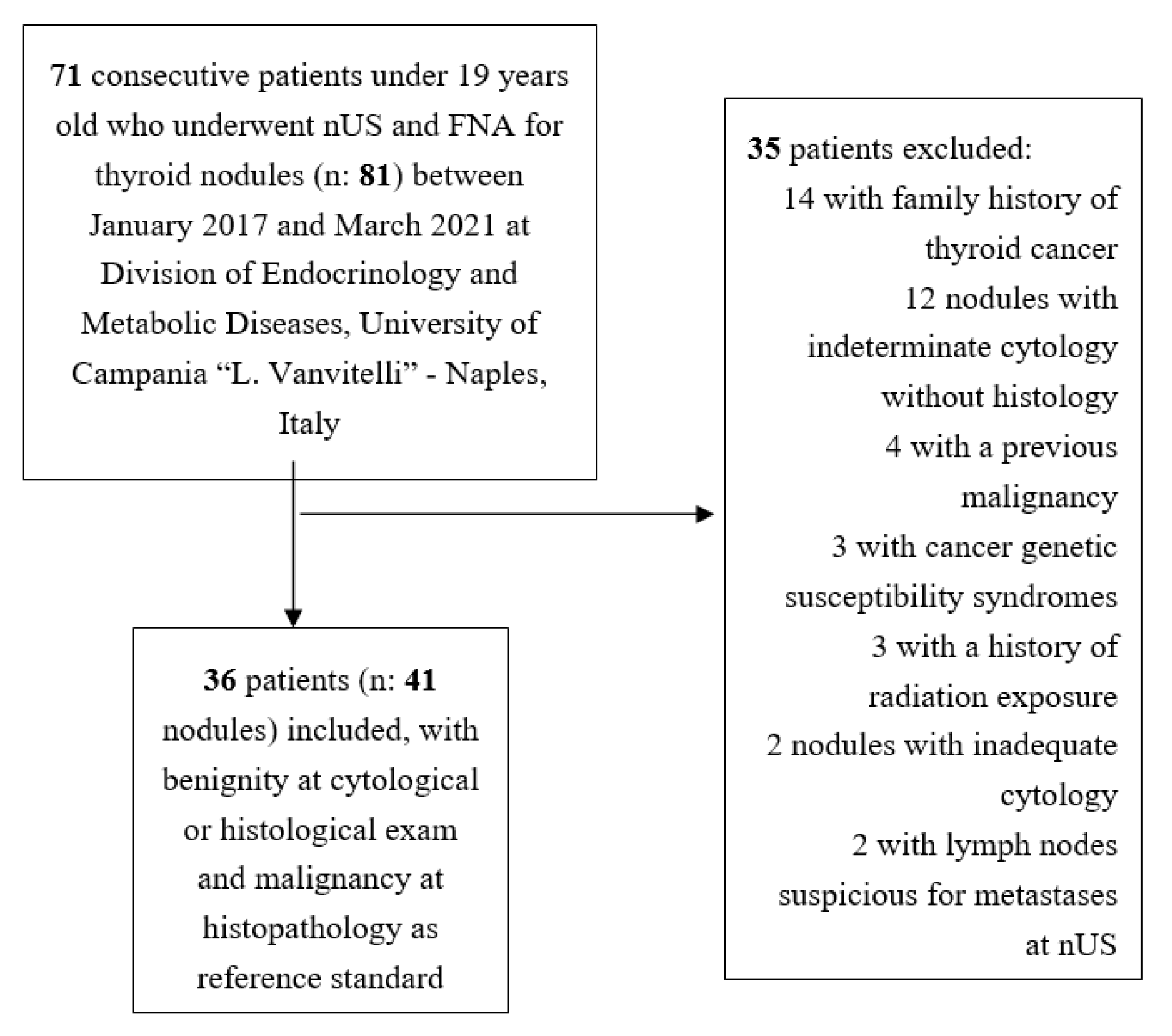
2.1. Study Design and Patients
2.2. Thyroid Ultrasonography
2.3. Thyroid Nodule Pathology
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Principal Findings
4.2. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M.; et al. Management guidelines for children with thyroid nodules and differentiated thyroid cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [Green Version]
- Lebbink, C.A.; Dekker, B.L.; Bocca, G.; Braat, A.; Derikx, J.; Dierselhuis, M.P.; de Keizer, B.; Kruijff, S.; Kwast, A.; van Nederveen, F.; et al. New national recommendations for the treatment of pediatric differentiated thyroid carcinoma in The Netherlands. Eur. J. Endocrinol. 2020, 183, P11–P18. [Google Scholar] [CrossRef] [PubMed]
- Niedziela, M.; Handkiewicz-Junak, D.; Małecka-Tendera, E.; Czarniecka, A.; Dedecjus, M.; Lange, D.; Kucharska, A.; Gawlik, A.; Pomorski, L.; Włoch, J. Diagnostics and treatment of differentiated thyroid carcinoma in children—Guidelines of Polish National Societies. Endokrynol. Polska 2016, 67, 628–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aghini-Lombardi, F.; Antonangeli, L.; Martino, E.; Vitti, P.; Maccherini, D.; Leoli, F.; Rago, T.; Grasso, L.; Valeriano, R.; Balestrieri, A.; et al. The spectrum of thyroid disorders in an iodine-deficient community: The Pescopagano survey. J. Clin. Endocrinol. Metab. 1999, 84, 561–566. [Google Scholar] [CrossRef]
- Taniguchi, N.; Hayashida, N.; Shimura, H.; Okubo, N.; Asari, Y.; Nigawara, T.; Midorikawa, S.; Kotani, K.; Nakaji, S.; Imaizumi, M.; et al. Ultrasonographic thyroid nodular findings in Japanese children. J. Med. Ultrason. 2001, 40, 219–224. [Google Scholar] [CrossRef]
- Bauer, A.J. Thyroid nodules in children and adolescents. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Cherella, C.E.; Angell, T.E.; Richman, D.M.; Frates, M.C.; Benson, C.B.; Moore, F.D.; Barletta, J.A.; Hollowell, M.; Smith, J.R.; Alexander, E.K.; et al. Differences in thyroid nodule cytology and malignancy risk between children and adults. Thyroid 2019, 29, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Al Nofal, A.; Gionfriddo, M.R.; Javed, A.; Haydour, Q.; Brito, J.P.; Prokop, L.J.; Pittock, S.T.; Murad, M.H. Accuracy of thyroid nodule sonography for the detection of thyroid cancer in children: Systematic review and meta-analysis. Clin. Endocrinol. 2016, 84, 423–430. [Google Scholar] [CrossRef]
- Essenmacher, A.C.; Joyce, P.H., Jr.; Kao, S.C.; Epelman, M.; Pesce, L.M.; D’Alessandro, M.P.; Sato, Y.; Johnson, C.M.; Podberesky, D.J. Sonographic evaluation of pediatric thyroid nodules. Radiographics 2017, 37, 1731–1752. [Google Scholar] [CrossRef]
- Ogle, S.; Merz, A.; Parina, R.; Alsayed, M.; Milas, M. Ultrasound and the evaluation of pediatric thyroid malignancy: Current recommendations for diagnosis and follow-up. J. Ultrasound Med. 2018, 37, 2311–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim-Dunham, J.E. Ultrasound guidelines for pediatric thyroid nodules: Proceeding with caution. Pediatr. Radiol. 2019, 49, 851–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iakovou, I.; Giannoula, E.; Sachpekidis, C. Imaging and imaging-based management of pediatric thyroid nodules. J. Clin. Med. 2020, 9, 384. [Google Scholar] [CrossRef] [Green Version]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrias, A.; Mussa, A.; Baronio, F.; Arrigo, T.; Salerno, M.; Segni, M.; Vigone, M.C.; Gastaldi, R.; Zirilli, G.; Tuli, G.; et al. Diagnostic features of thyroid nodules in pediatrics. Arch. Pediatr. Adolesc. Med. 2010, 164, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Clement, S.C.; Lebbink, C.A.; Klein Hesselink, M.S.; Teepen, J.C.; Links, T.P.; Ronckers, C.M.; van Santen, H.M. Presentation and outcome of subsequent thyroid cancer among childhood cancer survivors compared to sporadic thyroid cancer: A matched national study. Eur. J. Endocrinol. 2020, 183, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P. Ultrasound: The extension of our hands to improve the management of thyroid patients. Cancers 2021, 13, 567. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Castellana, M.; Piccardo, A.; Romanelli, F.; Grani, G.; Giovanella, L.; Durante, C. The ultrasound risk stratification systems for thyroid nodule have been evaluated against papillary carcinoma. A meta-analysis. Rev. Endocr. Metab. Disord. 2021, 22, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Castellana, M.; Piccardo, A.; Virili, C.; Scappaticcio, L.; Grani, G.; Durante, C.; Giovanella, L.; Trimboli, P. Can ultrasound systems for risk stratification of thyroid nodules identify follicular carcinoma? Cancer Cytopathol. 2020, 128, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, H.; Yang, Y.; Zhang, X.; Qian, L. The KWAK TI-RADS and 2015 ATA guidelines for medullary thyroid carcinoma: Combined with cell block-assisted ultrasound-guided thyroid fine-needle aspiration. Clin. Endocrinol. 2020, 92, 450–460. [Google Scholar] [CrossRef]
- Matrone, A.; Gambale, C.; Biagini, M.; Prete, A.; Vitti, P.; Elisei, R. Ultrasound features and risk stratification systems to identify medullary thyroid carcinoma. Eur. J. Endocrinol. 2021, 185, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Scappaticcio, L.; Virili, C.; Castellana, M.; Paone, G.; Centanni, M.; Trimboli, P.; Giovanella, L. An unsuspicious thyroid nodule with fatal outcome. Hormones 2019, 18, 321–324. [Google Scholar] [CrossRef]
- Castellana, M.; Virili, C.; Paone, G.; Scappaticcio, L.; Piccardo, A.; Giovanella, L.; Trimboli, P. Ultrasound systems for risk stratification of thyroid nodules prompt inappropriate biopsy in autonomously functioning thyroid nodules. Clin. Endocrinol. 2020, 93, 67–75. [Google Scholar] [CrossRef]
- Castellana, M.; Castellana, C.; Treglia, G.; Giorgino, F.; Giovanella, L.; Russ, G.; Trimboli, P. Performance of five ultrasound risk stratification systems in selecting thyroid nodules for FNA. J. Clin. Endocrinol. Metab. 2020, 105, 1659–1669. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.H.; Yoon, H.M.; Hwang, J.; Lee, J.S.; Jung, A.Y.; Cho, Y.A.; Baek, J.H. Diagnostic performance of adult-based ATA and ACR-TIRADS ultrasound risk stratification systems in pediatric thyroid nodules: A systematic review and meta-analysis. Eur. Radiol. 2021, 31, 7450–7463. [Google Scholar] [CrossRef]
- Grani, G.; Brenta, G.; Trimboli, P.; Falcone, R.; Ramundo, V.; Maranghi, M.; Lucia, P.; Filetti, S.; Durante, C. Sonographic risk stratification systems for thyroid nodules as rule-out tests in older adults. Cancers 2020, 12, 2458. [Google Scholar] [CrossRef] [PubMed]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR thyroid imaging, reporting and data system (TI-RADS): White paper of the ACR TI-RADS committee. JACR 2017, 14, 587–595. [Google Scholar] [CrossRef] [Green Version]
- Russ, G.; Bonnema, S.J.; Erdogan, M.F.; Durante, C.; Ngu, R.; Leenhardt, L. European thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: The EU-TIRADS. Eur. Thyroid J. 2017, 6, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.H.; Baek, J.H.; Chung, J.; Ha, E.J.; Kim, J.H.; Lee, Y.H.; Lim, H.K.; Moon, W.J.; Na, D.G.; Park, J.S.; et al. Ultrasonography diagnosis and imaging-based management of thyroid nodules: Revised korean society of thyroid radiology consensus statement and recommendations. Korean J. Radiol. 2016, 17, 370–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef] [Green Version]
- Nardi, F.; Basolo, F.; Crescenzi, A.; Fadda, G.; Frasoldati, A.; Orlandi, F.; Palombini, L.; Papini, E.; Zini, M.; Pontecorvi, A.; et al. Italian consensus for the classification and reporting of thyroid cytology. J. Endocrinol. Investig. 2014, 37, 593–599. [Google Scholar] [CrossRef]
- Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J.; World Health Organization. International Agency for Research on Cancer. WHO Classification of Tumours of Endocrine Organs. 2017. Available online: https://www.iarc.who.int/news-events/who-classification-of-tumours-of-endocrine-organs/ (accessed on 28 August 2021).
- Galen, R.S.; Gambino, S.R. Beyond Normality: The Predictive Value and Efficiency of Medical Diagnoses; John and Wiley and Sons: New York, NY, USA, 1975. [Google Scholar]
- Richman, D.M.; Benson, C.B.; Doubilet, P.M.; Wassner, A.J.; Asch, E.; Cherella, C.E.; Smith, J.R.; Frates, M.C. Assessment of American College of Radiology Thyroid Imaging Reporting and Data System (TI-RADS) for pediatric thyroid nodules. Radiology 2020, 294, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Bi Lee, S.; Jin Cho, Y.; Lee, S.; Hun Choi, Y.; Cheon, J.E.; Sun Kim, W. Korean Society of Thyroid Radiology Guidelines for the Management of Pediatric Thyroid Nodules: Suitability and Risk Factors. Thyroid 2021. [Google Scholar] [CrossRef]
- Martinez-Rios, C.; Daneman, A.; Bajno, L.; van der Kaay, D.; Moineddin, R.; Wasserman, J.D. Utility of adult-based ultrasound malignancy risk stratifications in pediatric thyroid nodules. Pediatr. Radiol. 2018, 48, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.M.; Baek, J.H.; Na, D.G.; Suh, C.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Diagnostic performance of practice guidelines for thyroid nodules: Thyroid nodule size versus biopsy rates. Radiology 2019, 291, 92–99. [Google Scholar] [CrossRef]
- Kim, P.H.; Suh, C.H.; Baek, J.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Unnecessary thyroid nodule biopsy rates under four ultrasound risk stratification systems: A systematic review and meta-analysis. Eur. Radiol. 2021, 31, 2877–2885. [Google Scholar] [CrossRef]
- Radetti, G.; Loche, S.; D’Antonio, V.; Salerno, M.; Guzzetti, C.; Aversa, T.; Cassio, A.; Cappa, M.; Gastaldi, R.; Deluca, F.; et al. Influence of hashimoto thyroiditis on the development of thyroid nodules and cancer in children and adolescents. J. Endocr. Soc. 2019, 3, 607–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacFarland, S.P.; Bauer, A.J.; Adzick, N.S.; Surrey, L.F.; Noyes, J.; Kazahaya, K.; Mostoufi-Moab, S. Disease burden and outcome in children and young adults with concurrent graves disease and differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2018, 103, 2918–2925. [Google Scholar] [CrossRef]
- Gharib, H.; Papini, E.; Garber, J.R.; Duick, D.S.; Harrell, R.M.; Hegedüs, L.; Paschke, R.; Valcavi, R.; Vitti, P.; AACE/ACE/AME Task Force on Thyroid Nodules. American Association of Clinical Endocrinologists, American College Of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines For Clinical Practice For The Diagnosis And Management Of Thyroid Nodules--2016 update. Endocr. Pract. 2016, 22, 622–639. [Google Scholar] [CrossRef] [Green Version]
- Russ, G.; Trimboli, P.; Buffet, C. The new era of TIRADSs to stratify the risk of malignancy of thyroid nodules: Strengths, weaknesses and pitfalls. Cancers 2021, 13, 4316. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | |
|---|---|
| Age at diagnosis, years (IQR) | 15 (11–17) |
| Females/males (n) | 26/10 |
| Reasons to perform nUS | |
| 17 (47.2) |
| 9 (25) |
| 6 (16.7) |
| 4 (11.1) |
| Nodules | |
| 13 (10–16) |
| 28 (77.8) |
| 8 (22.2) |
| Benign nodules/malignant nodules, n (%) | 29/12 (70.7/29.3) |
| 6/29 (20.7) |
| 10 (7–13) |
| 10 (83.3) |
| 2 (16.7) |
| ACR-TIRADS | Benign Nodules (n) | Malignant Nodules (n) | Total Nodules (n) | Cancer Prevalence (%) |
|---|---|---|---|---|
| 4 | 0 | 4 | 0 |
| 4 | 1 | 5 | 20 |
| 7 | 3 | 10 | 30 |
| 14 | 2 | 16 | 12.5 |
| 0 | 6 | 6 | 100 |
| EU-TIRADS | ||||
| 7 | 1 | 8 | 12.5 |
| 8 | 3 | 11 | 27.3 |
| 14 | 2 | 16 | 12.5 |
| 0 | 6 | 6 | 100 |
| K-TIRADS | ||||
| 7 | 1 | 8 | 12.5 |
| 8 | 3 | 11 | 27.3 |
| 14 | 2 | 16 | 12.5 |
| 0 | 6 | 6 | 100 |
| ATA US RSS | ||||
| 0 | 0 | 0 | 0 |
| 5 | 0 | 5 | 0 |
| 10 | 4 | 14 | 28.6 |
| 14 | 2 | 16 | 12.5 |
| 0 | 6 | 6 | 100 |
| Management Per ACR TIRADS Criteria | Benign Nodules (n) | Malignant Nodules (n) | Total Nodules (n) | Cancer Prevalence (%) | Unnecessary FNA Prevalence (%) |
|---|---|---|---|---|---|
| 7 | 5 | 12 | 41.7 | 58.3 |
| 22 | 7 | 29 | 24.1 | |
| Management per EU-TIRADS criteria | |||||
| 7 | 5 | 12 | 41.7 | 58.3 |
| 22 | 7 | 29 | 24.1 | |
| Management per K-TIRADS criteria | |||||
| 19 | 6 | 25 | 24 | 76 |
| 10 | 6 | 16 | 37.5 | |
| Management per ATA US RSS criteria | |||||
| 19 | 6 | 25 | 24 | 76 |
| 10 | 6 | 16 | 37.5 |
| Sensitivity (%) (CI) | Specificity (%) (CI) | PPV (%) (CI) | NPV (%) (CI) | Accuracy (%) | |
|---|---|---|---|---|---|
| ACR TIRADS | 41.7 (27–58) | 75.9 (60–87) | 41.7 (27–58) | 75.9 (60–87) | 65.9 |
| EU-TIRADS | 41.7 (27–58) | 75.9 (60–87) | 41.7 (60–87) | 75.9 (60–87) | 65.9 |
| K-TIRADS | 50.0 (32–68) | 34.5 (0.3–14) | 24.0 (11–43) | 62.5 (0.3–14) | 39.0 |
| ATA US RSS | 50.0 (32–68) | 34.5 (0.3–14) | 24.0 (11–43) | 62.5 (0.3–14) | 39.0 |
| ID | Age (Years) | Gender | Number | Location | Composition | Echogenicity | Taller Than Wide | Margin | Echogenic Foci | Maximum Dimension (mm) | TI-RADS Risk Level | Cytology | Histology | Preexisting Thyroid Disease |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 17 | F | single | lower left pole | solid | hypoechoic | no | ill-defined | punctate | 7 | TR5, EU5, K5, High | TIR4 | mCPTC | no |
| 2 | 15 | M | multiple | mid right lobe | solid | isoechoic | no | smooth | no | 10 | TR3, EU3, K3, Low | TIR5 | CPTC | no |
| 3 | 18 | F | single | isthmus | solid | hypoechoic | no | smooth | no | 13 | TR4, EU4 | TIR3A | FV-PTC | ACT |
| 4 | 17 | F | single | upper right lobe | mixed cystic and solid | isoechoic | no | smooth | no | 7 | TR2, EU2, K2, Low | TIR5 | CPTC | GD |
| 5 | 7 | M | multiple | mid right lobe | solid | isoechoic | no | smooth | no | 10 | TR3, EU3, K3, Low | TIR3B | FTC | ACT |
| 6 | 12 | M | single | upper left lobe | solid | isoechoic | no | smooth | no | 12 | TR3, EU3, K3, Low | TIR3B | FTC | ACT |
| 7 | 13 | F | single | upper right lobe | solid | hypoechoic | no | ill-defined | punctate | 7 | TR5, EU5, K5, High | TIR5 | CPTC | ACT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scappaticcio, L.; Maiorino, M.I.; Iorio, S.; Docimo, G.; Longo, M.; Grandone, A.; Luongo, C.; Cozzolino, I.; Piccardo, A.; Trimboli, P.; et al. Exploring the Performance of Ultrasound Risk Stratification Systems in Thyroid Nodules of Pediatric Patients. Cancers 2021, 13, 5304. https://doi.org/10.3390/cancers13215304
Scappaticcio L, Maiorino MI, Iorio S, Docimo G, Longo M, Grandone A, Luongo C, Cozzolino I, Piccardo A, Trimboli P, et al. Exploring the Performance of Ultrasound Risk Stratification Systems in Thyroid Nodules of Pediatric Patients. Cancers. 2021; 13(21):5304. https://doi.org/10.3390/cancers13215304
Chicago/Turabian StyleScappaticcio, Lorenzo, Maria Ida Maiorino, Sergio Iorio, Giovanni Docimo, Miriam Longo, Anna Grandone, Caterina Luongo, Immacolata Cozzolino, Arnoldo Piccardo, Pierpaolo Trimboli, and et al. 2021. "Exploring the Performance of Ultrasound Risk Stratification Systems in Thyroid Nodules of Pediatric Patients" Cancers 13, no. 21: 5304. https://doi.org/10.3390/cancers13215304