
Treatment Pattern and Outcomes with Systemic Therapy in Men with Metastatic Prostate Cancer in the Real-World Patients in the United States

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
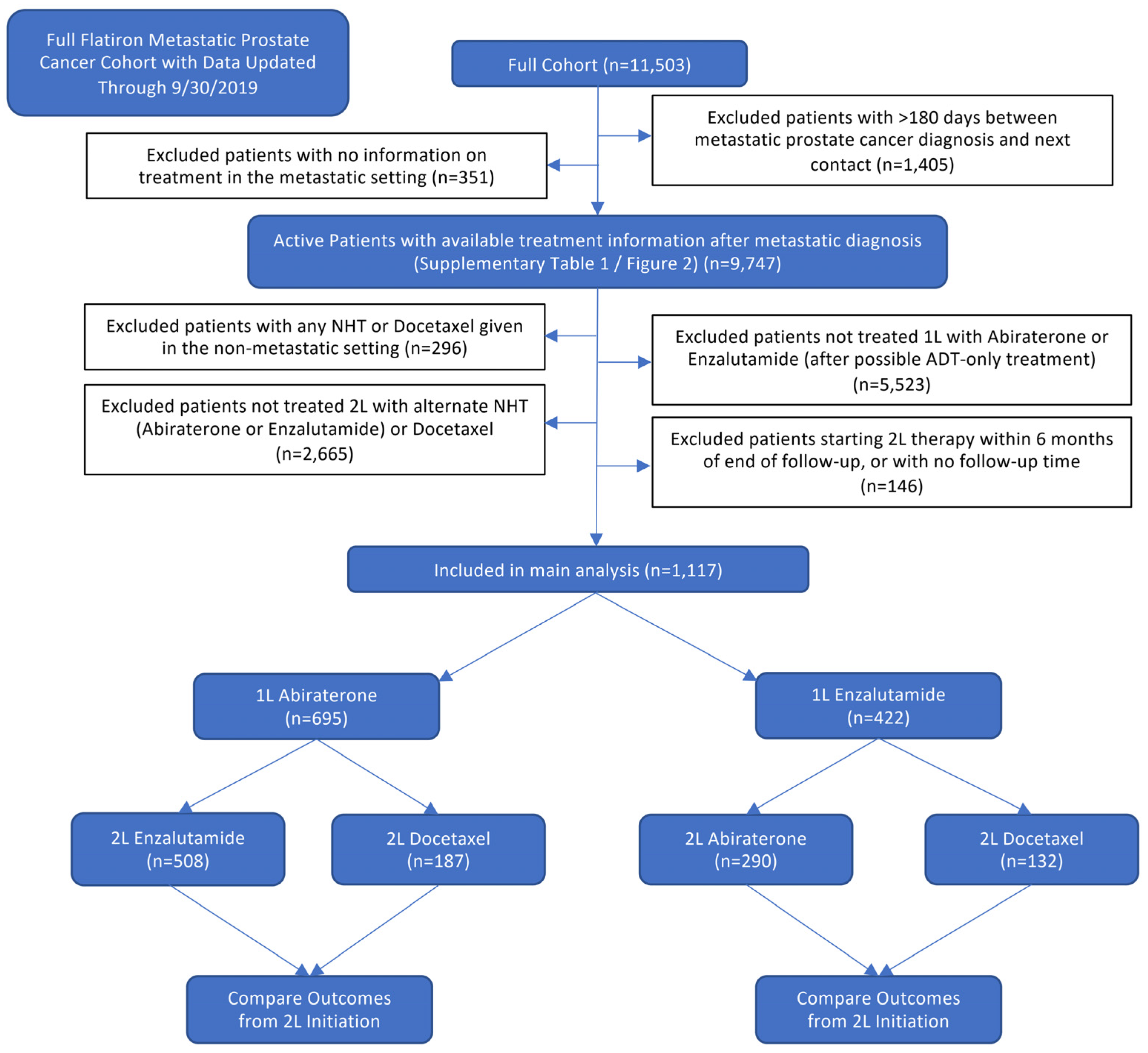
2.1. Study Population
2.2. Outcome Definitions for Comparative Effective Analysis
2.3. Statistical Analysis
3. Results
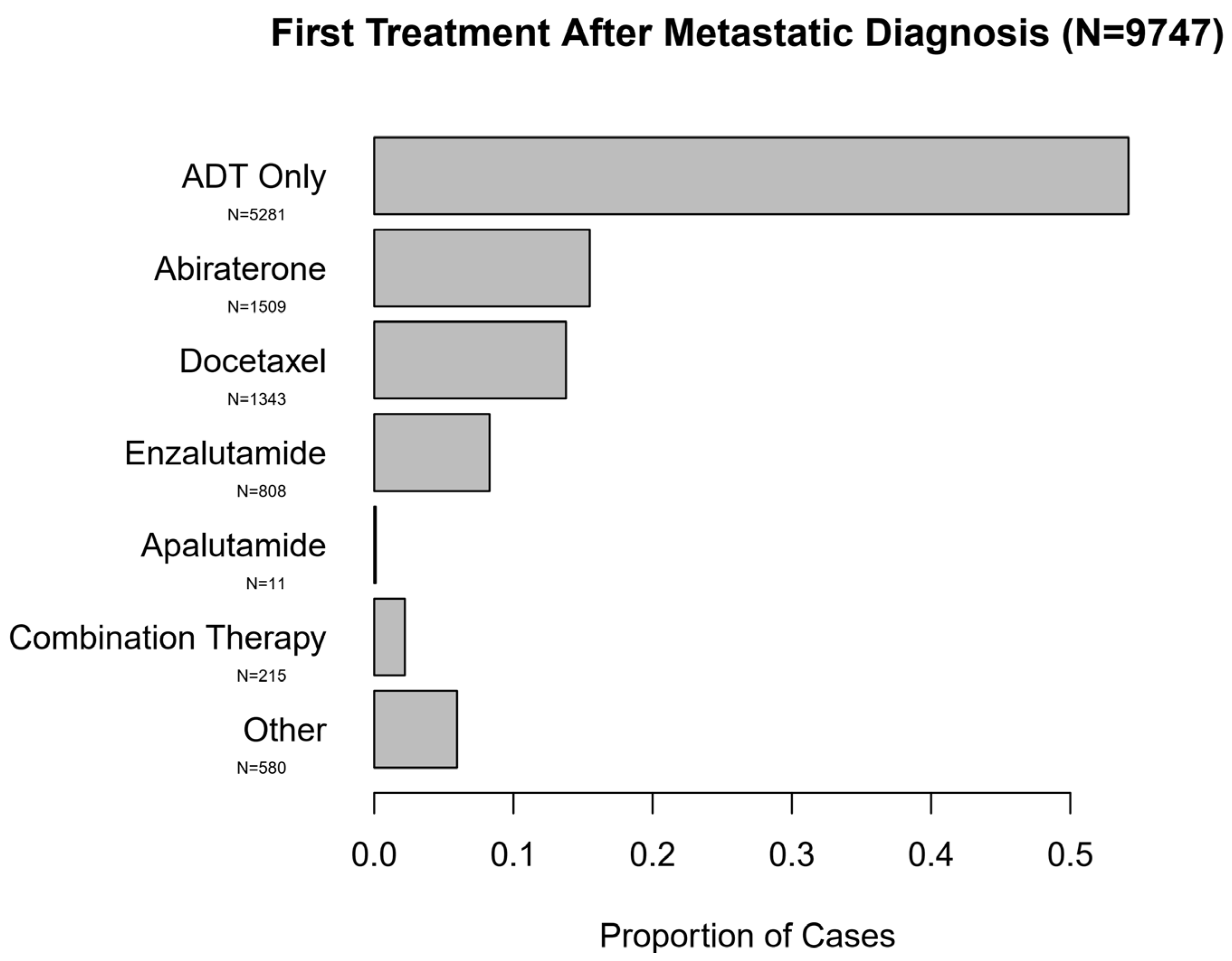
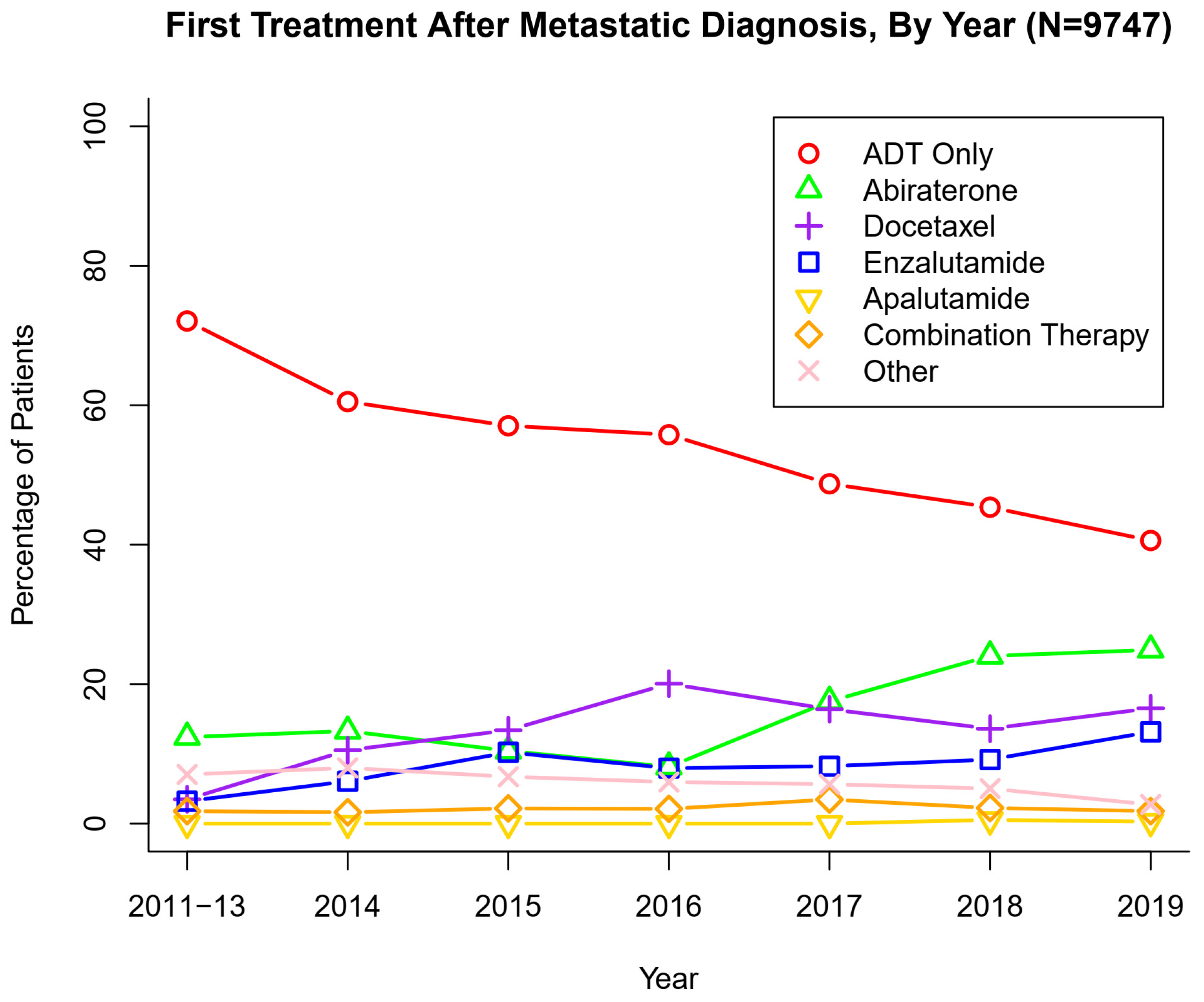
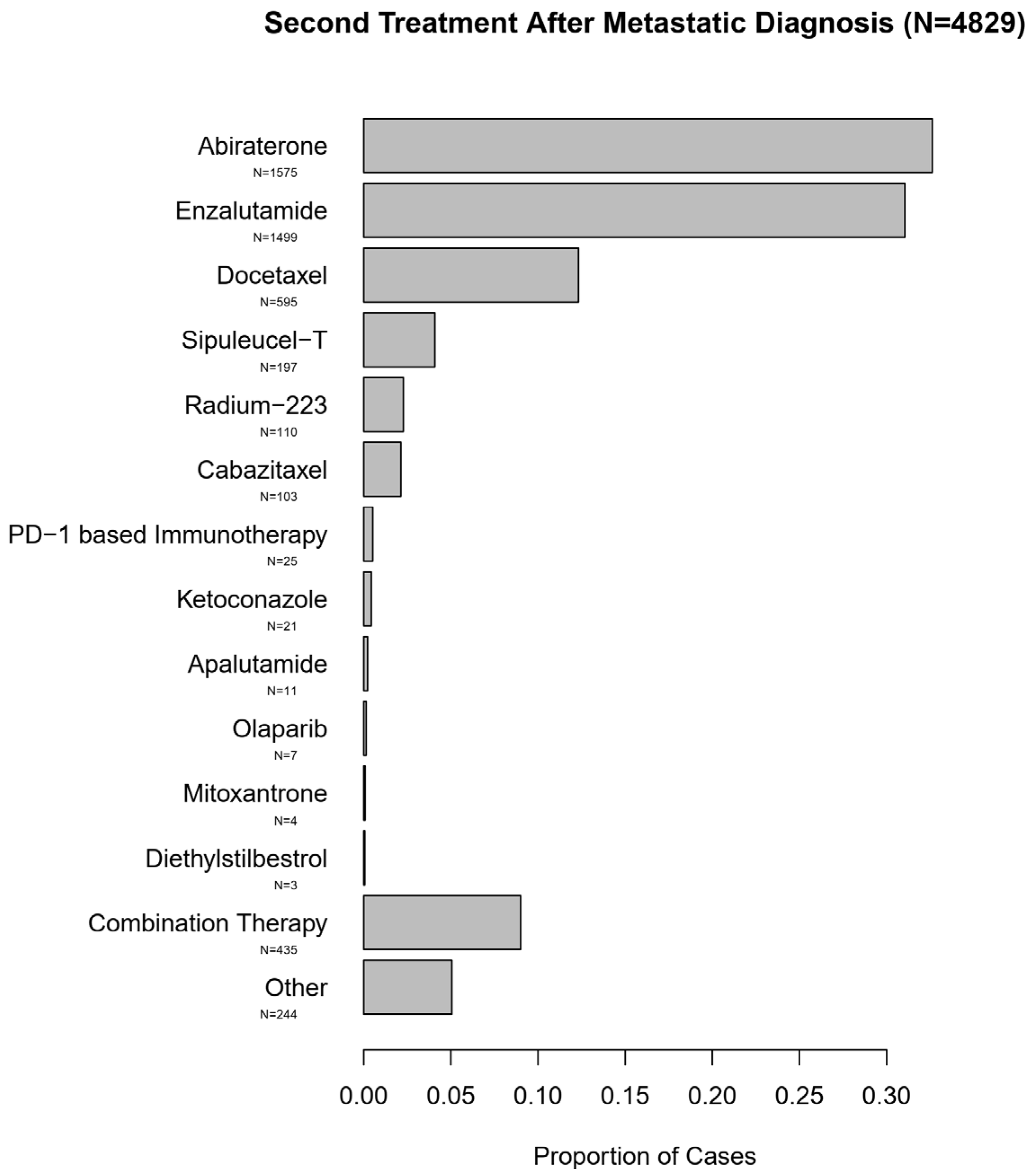
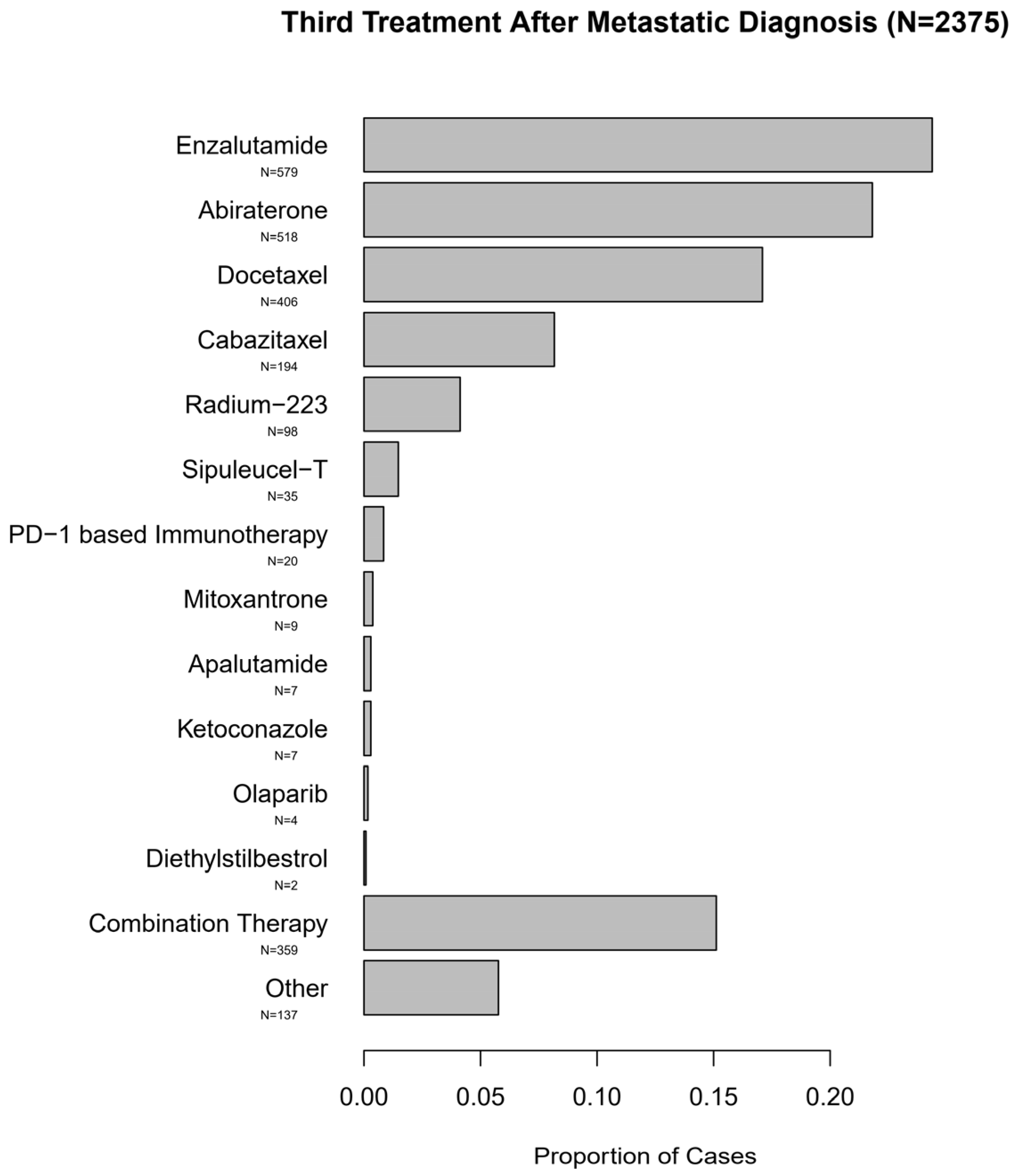
3.1. Treatment Patterns in Patients with Metastatic Prostate Cancer
3.2. Comparison of Effectiveness of NHT versus Docetaxel after a Prior NHT
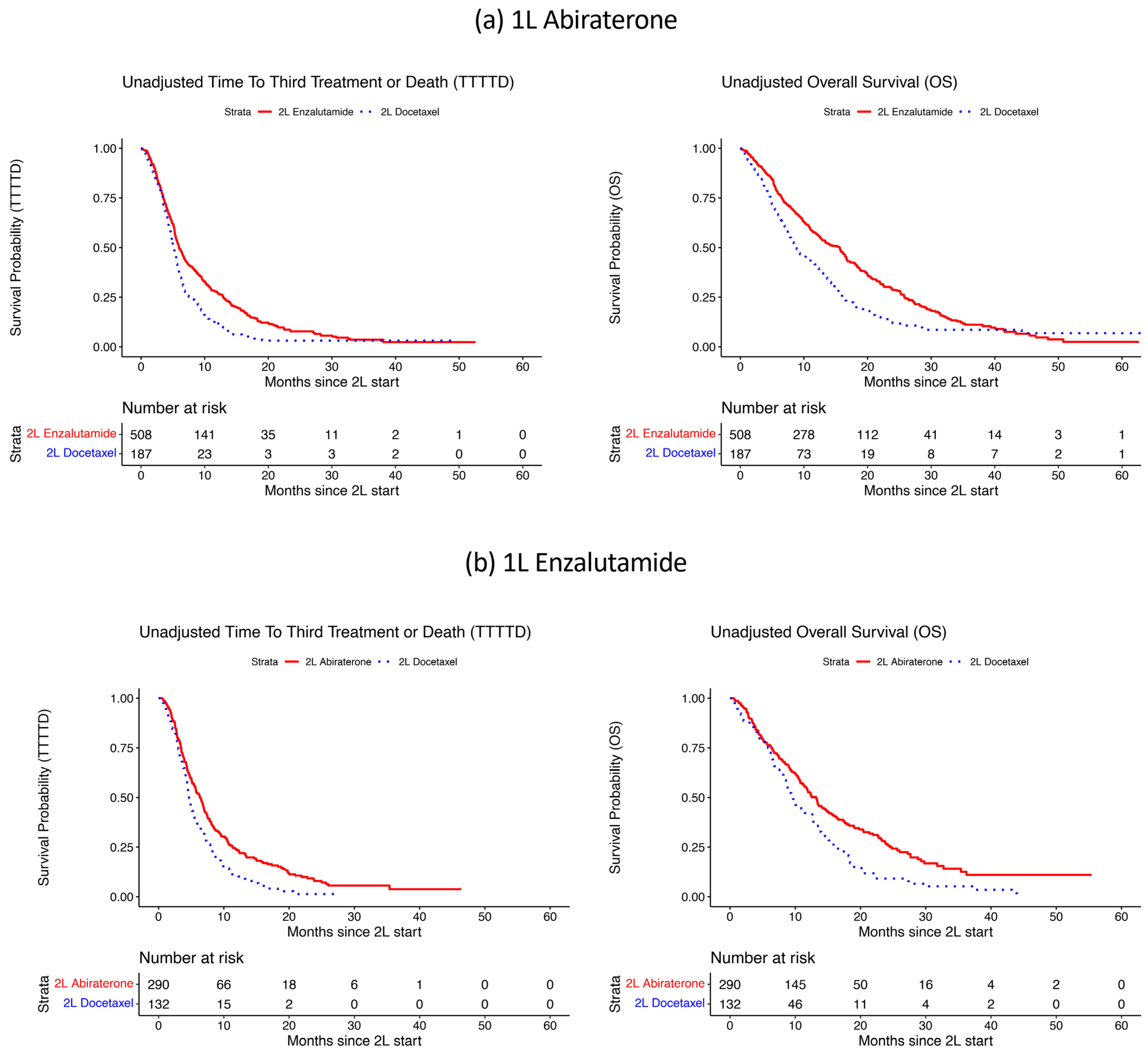
3.3. Primary TTTTD and OS Analysis
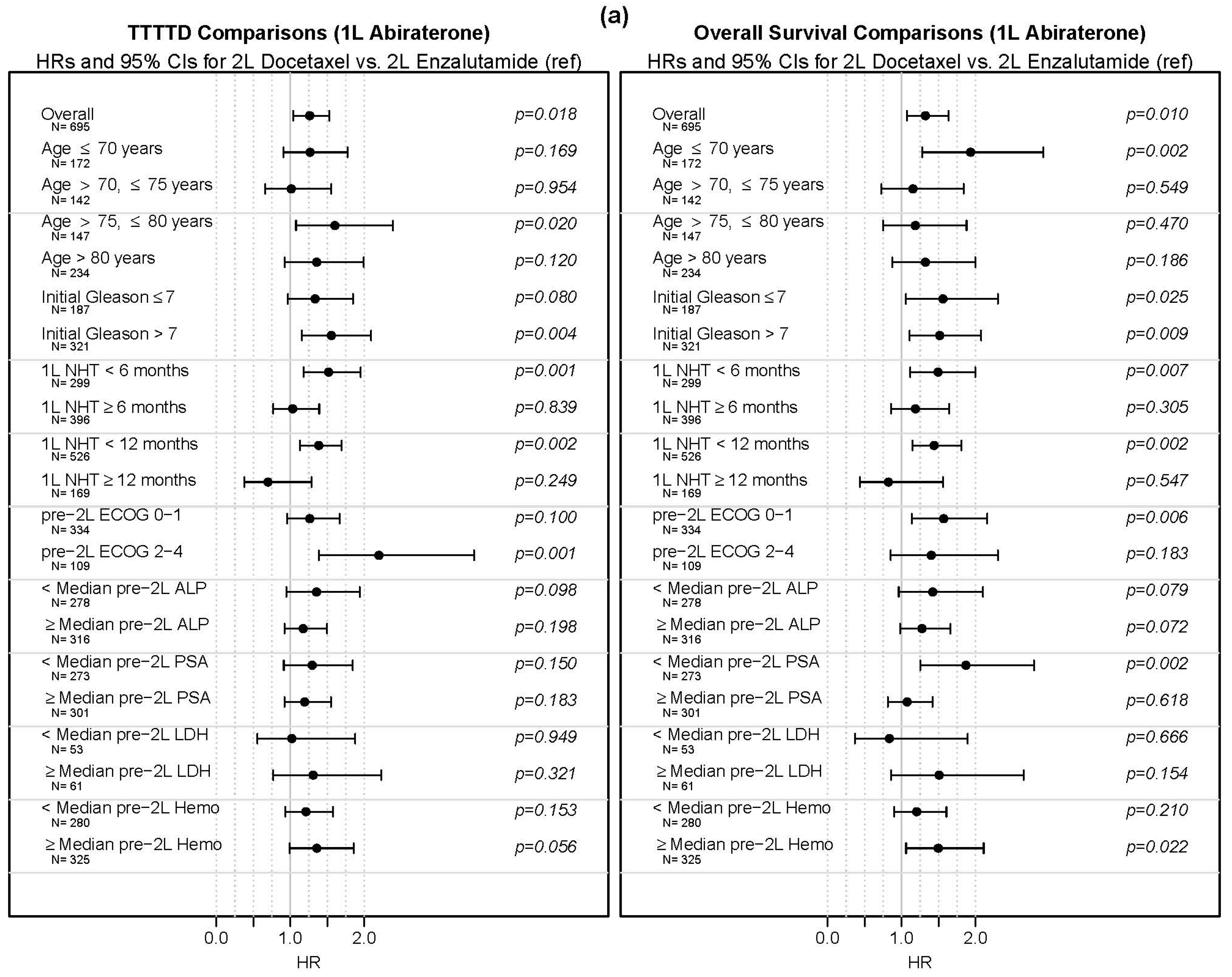
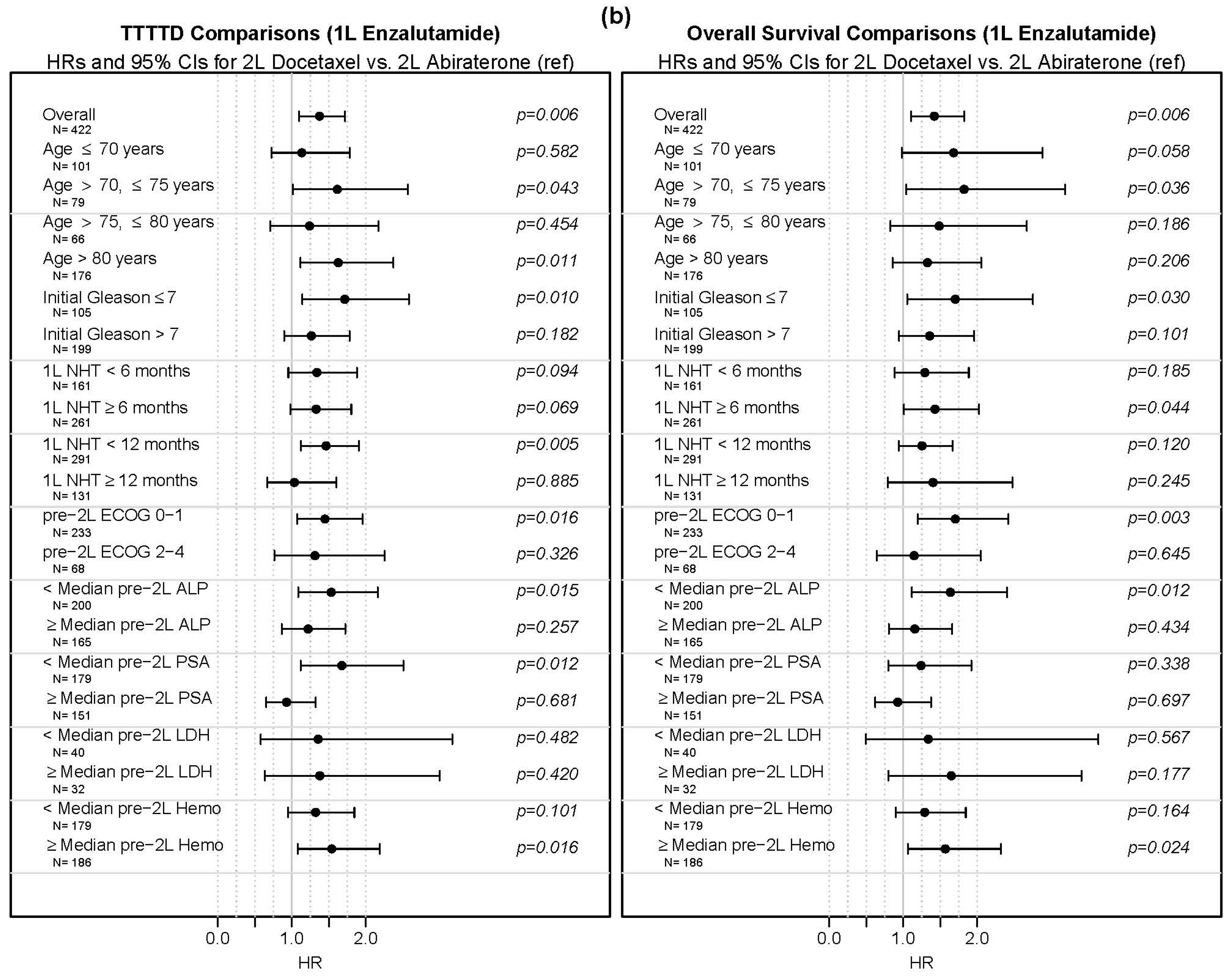
3.4. Subgroup Analyses
3.5. Post-2L Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, N.D.; de Bono, J.S.; Spears, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Ritchie, A.W.S.; Amos, C.L.; Gilson, C.; Jones, R.J.; et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N. Engl. J. Med. 2017, 377, 338–351. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.; et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Soto, A.J.; Merseburger, A.S.; Özgüroglu, M.; Uemura, H.; et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef]
- Kyriakopoulos, C.E.; Chen, Y.-H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: Long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, N.D.; Sydes, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.S.; Parker, C.C.; Russell, J.M.; Attard, G.; et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 2016, 387, 1163–1177. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. Prostate Cancer (Version 2.2021). Available online: http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 23 February 2021).
- De Bono, J.S.; Chowdhury, S.; Feyerabend, S.; Elliott, T.; Grande, E.; Melhem-Bertrandt, A.; Baron, B.; Hirmand, M.; Werbrouck, P.; Fizazi, K. Antitumour activity and safety of enzalutamide in patients with metastatic castration-resistant prostate cancer previously treated with abiraterone acetate plus prednisone for ≥24 weeks in Europe. Eur. Urol. 2018, 74, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Khalaf, D.J.; Annala, M.; Taavitsainen, S.; Finch, D.L.; Oja, C.; Vergidis, J.; Zulfiqar, M.; Sunderland, K.; Azad, A.A.; Kollmannsberger, C.K.; et al. Optimal sequencing of enzalutamide and abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer: A multicentre, randomised, open-label, phase 2, crossover trial. Lancet Oncol. 2019, 20, 1730–1739. [Google Scholar] [CrossRef]
- De Bono, J.S.; Smith, M.R.; Saad, F.; Rathkopf, D.E.; Mulders, P.F.; Small, E.J.; Shore, N.D.; Fizazi, K.; de Porre, P.; Kheoh, T.; et al. Subsequent chemotherapy and treatment patterns after abiraterone acetate in patients with metastatic castration-resistant prostate cancer: Post hoc analysis of COU-AA-302. Eur. Urol. 2017, 71, 656–664. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Long, L.; Moon, S.; Adamson, B.J.S.; Baxi, S.S. Comparison of population characteristics in real-world clinical oncology databases in the US: Flatiron health, SEER, and NPCR. medRxiv 2020. medRxiv:2020.03.16.20037143. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Swami, U.; McFarland, T.R.; Nussenzveig, R.; Agarwal, N. Advanced prostate cancer: Treatment advances and future directions. Trends Cancer 2020, 6, 702–715. [Google Scholar] [CrossRef]
- Agarwal, N.; McQuarrie, K.; Bjartell, A.; Chowdhury, S.; Pereira de Santana Gomes, A.J.; Chung, B.H.; Özgüroglu, M.; Soto, Á.J.; Merseburger, A.S.; Uemura, H.; et al. Health-related quality of life after apalutamide treatment in patients with metastatic castration-sensitive prostate cancer (TITAN): A randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2019, 20, 1518–1530. [Google Scholar] [CrossRef]
- Ryan, C.J.; Ke, X.; Lafeuille, M.-H.; Romdhani, H.; Kinkead, F.; Lefebvre, P.; Petrilla, A.; Pulungan, Z.; Kim, S.; D’Andrea, D.M.; et al. Management of patients with metastatic castration-sensitive prostate cancer in the real-world setting in the United States. J. Urol. 2021. [Google Scholar] [CrossRef]
- Swami, U.; Hong, A.; El-Chaar, N.N.; Nimke, D.; Ramaswamy, K.; Bell, E.J.; Sandin, R.; Agarwal, N. Real-world first-line (1L) treatment patterns in patients (pts) with metastatic castration-sensitive prostate cancer (mCSPC) in a US health insurance database. J. Clin. Oncol. 2021, 39, 5072. [Google Scholar] [CrossRef]
- Freedland, S.J.; Agarwal, N.; Ramaswamy, K.; Sandin, R.; Russell, D.; Hong, A.; Yang, H.; Gao, W.; Hagan, K.; George, D.J. Real-world utilization of advanced therapies and racial disparity among patients with metastatic castration-sensitive prostate cancer (mCSPC): A Medicare database analysis. J. Clin. Oncol. 2021, 39, 5073. [Google Scholar] [CrossRef]
- George, D.J.; Agarwal, N.; Rider, J.R.; Li, B.; Shirali, R.; Sandin, R.; Hong, A.; Russell, D.; Ramaswamy, K.; Freedland, S.J. Real-world treatment patterns among patients diagnosed with metastatic castration-sensitive prostate cancer (mCSPC) in community oncology settings. J. Clin. Oncol. 2021, 39, 5074. [Google Scholar] [CrossRef]
- De Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B., Jr.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. N. Engl. J. Med. 2011, 364, 1995–2005. [Google Scholar] [CrossRef]
- Ryan, C.J.; Smith, M.R.; de Bono, J.S.; Molina, A.; Logothetis, C.J.; de Souza, P.; Fizazi, K.; Mainwaring, P.; Piulats, J.M.; Vogelzang, N.J.; et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N. Engl. J. Med. 2013, 368, 138–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrylak, D.P.; Tangen, C.M.; Hussain, M.H.; Lara, P.N.; Jones, J.A.; Taplin, M.E.; Burch, P.A.; Berry, D.; Moinpour, C.; Kohli, M.; et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N. Engl. J. Med. 2004, 351, 1513–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Theodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, G.A.; Barrie, S.E.; Jarman, M.; Rowlands, M.G. Novel steroidal inhibitors of human cytochrome P45017. alpha.-Hydroxylase-C17, 20-lyase): Potential agents for the treatment of prostatic cancer. J. Med. Chem. 1995, 38, 2463–2471. [Google Scholar] [CrossRef]
- Barrie, S.; Potter, G.; Goddard, P.; Haynes, B.; Dowsett, M.; Jarman, M. Pharmacology of novel steroidal inhibitors of cytochrome P45017α (17α-hydroxylase/C17–20 lyase). J. Steroid Biochem. Mol. Biol. 1994, 50, 267–273. [Google Scholar] [CrossRef]
- Odonnell, A.G.; Judson, I.; Dowsett, M.; Raynaud, F.; Dearnaley, D.P.; Mason, M.G.; Harland, S.J.; Robbins, A.S.; Halbert, G.; Nutley, B.; et al. Hormonal impact of the 17 α-hydroxylase/C 17, 20-lyase inhibitor abiraterone acetate (CB7630) in patients with prostate cancer. Br. J. Cancer 2004, 90, 2317–2325. [Google Scholar] [CrossRef]
- Li, Z.; Alyamani, M.; Li, J.; Rogacki, K.; Abazeed, M.; Upadhyay, S.K.; Balk, S.P.; Taplin, M.-E.; Auchus, R.J.; Sharifi, N. Redirecting abiraterone metabolism to fine-tune prostate cancer anti-androgen therapy. Nature 2016, 533, 547–551. [Google Scholar] [CrossRef] [Green Version]
- Tran, C.; Ouk, S.; Clegg, N.J.; Chen, Y.; Watson, P.A.; Arora, V.; Wongvipat, J.; Smith-Jones, P.M.; Yoo, D.; Kwon, A.; et al. Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science 2009, 324, 787–790. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.-L.; Horbinski, C.M.; Garzotto, M.; Qian, D.Z.; Beer, T.M.; Kyprianou, N. Tubulin-targeting chemotherapy impairs androgen receptor activity in prostate cancer. Cancer Res. 2010, 70, 7992–8002. [Google Scholar] [CrossRef] [Green Version]
- Van Soest, R.J.; van Royen, M.E.; de Morrée, E.S.; Moll, J.M.; Teubel, W.; Wiemer, E.A.C.; Mathijssen, R.H.; de Wit, R.; van Weerden, W.M. Cross-resistance between taxanes and new hormonal agents abiraterone and enzalutamide may affect drug sequence choices in metastatic castration-resistant prostate cancer. Eur. J. Cancer 2013, 49, 3821–3830. [Google Scholar] [CrossRef] [PubMed]
- Van Soest, R.J.; de Morrée, E.S.; Kweldam, C.F.; de Ridder, C.M.; Wiemer, E.A.C.; Mathijssen, R.H.; de Wit, R.; van Weerden, W.M. Targeting the androgen receptor confers in vivo cross-resistance between enzalutamide and docetaxel, but not cabazitaxel, in castration-resistant prostate cancer. Eur. Urol. 2015, 67, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Lombard, A.P.; Liu, L.; Cucchiara, V.; Liu, C.; Armstrong, C.M.; Zhao, R.; Yang, J.C.; Lou, W.; Evans, C.P.; Gao, A.C. Intra vs inter cross-resistance determines treatment sequence between taxane and AR-targeting therapies in advanced prostate cancer. Mol. Cancer Ther. 2018, 17, 2197–2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Wit, R.; de Bono, J.; Sternberg, C.N.; Fizazi, K.; Tombal, B.; Wülfing, C.; Kramer, G.; Eymard, J.-C.; Bamias, A.; Carles, J.; et al. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N. Engl. J. Med. 2019, 381, 2506–2518. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1L Therapy | Population | Outcome | 2L Therapy | N | Events | Median Survival, Months (95% CI) |
|---|---|---|---|---|---|---|
| Abiraterone | Overall | TTTTD | Enzalutamide | 508 | 422 | 5.9 (5.6, 6.7) |
| Docetaxel | 187 | 161 | 5.1 (4.7, 5.7) | |||
| OS | Enzalutamide | 508 | 352 | 15.6 (12.7, 16.7) | ||
| Docetaxel | 187 | 144 | 8.7 (7.7, 11.6) | |||
| 1L NHT < 6 months | TTTTD | Enzalutamide | 184 | 154 | 5.9 (5.4, 7.1) | |
| Docetaxel | 115 | 104 | 5.0 (4.7, 5.7) | |||
| OS | Enzalutamide | 184 | 128 | 15.1 (11.0, 18.4) | ||
| Docetaxel | 115 | 91 | 9.1 (7.7, 12.1) | |||
| 1L NHT ≥ 6 months | TTTTD | Enzalutamide | 324 | 268 | 6.0 (5.5, 7.0) | |
| Docetaxel | 72 | 57 | 5.5 (4.3, 6.6) | |||
| OS | Enzalutamide | 324 | 224 | 15.6 (12.8, 16.7) | ||
| Docetaxel | 72 | 53 | 8.4 (6.3, 13.2) | |||
| 1L NHT < 12 months | TTTTD | Enzalutamide | 362 | 306 | 5.6 (5.3, 6.4) | |
| Docetaxel | 164 | 148 | 5.0 (4.6, 5.5) | |||
| OS | Enzalutamide | 362 | 263 | 12.5 (10.9, 15.6) | ||
| Docetaxel | 164 | 132 | 8.1 (7.3, 10.3) | |||
| 1L NHT ≥ 12 months | TTTTD | Enzalutamide | 146 | 116 | 8.2 (5.9, 10.1) | |
| Docetaxel | 23 | 13 | 8.5 (4.7, -) | |||
| OS | Enzalutamide | 146 | 89 | 18.9 (16.5, 24.6) | ||
| Docetaxel | 23 | 12 | 16.0 (12.4, -) | |||
| Enzalutamide | Overall | TTTTD | Abiraterone | 290 | 226 | 6.3 (5.5, 7.0) |
| Docetaxel | 132 | 117 | 4.7 (4.4, 5.4) | |||
| OS | Abiraterone | 290 | 182 | 13.2 (11.4, 15.0) | ||
| Docetaxel | 132 | 103 | 9.7 (8.6, 12.6) | |||
| 1L NHT < 6 months | TTTTD | Abiraterone | 92 | 72 | 4.8 (4.2, 6.3) | |
| Docetaxel | 69 | 63 | 4.4 (3.7, 5.3) | |||
| OS | Abiraterone | 92 | 66 | 9.8 (6.7, 13.5) | ||
| Docetaxel | 69 | 58 | 7.0 (6.3, 9.3) | |||
| 1L NHT ≥ 6 months | TTTTD | Abiraterone | 198 | 154 | 6.8 (6.2, 8.0) | |
| Docetaxel | 63 | 54 | 5.3 (4.4, 8.2) | |||
| OS | Abiraterone | 198 | 116 | 14.0 (11.9, 17.6) | ||
| Docetaxel | 63 | 45 | 12.8 (10.9, 16.6) | |||
| 1L NHT < 12 months | TTTTD | Abiraterone | 184 | 140 | 5.7 (5.0, 7.0) | |
| Docetaxel | 107 | 96 | 4.5 (4.1, 5.3) | |||
| OS | Abiraterone | 184 | 125 | 10.4 (8.4, 12.0) | ||
| Docetaxel | 107 | 87 | 8.8 (7.7, 11.5) | |||
| 1L NHT ≥ 12 months | TTTTD | Abiraterone | 106 | 86 | 6.9 (5.9, 8.5) | |
| Docetaxel | 25 | 21 | 7.2 (4.9, 14.8) | |||
| OS | Abiraterone | 106 | 57 | 19.1 (14.7, 24.2) | ||
| Docetaxel | 25 | 16 | 15.1 (10.0, -) |
| 1L Therapy | Outcome | 2L Therapy | N | HR (95% CI) | p |
|---|---|---|---|---|---|
| Abiraterone | TTTTD | Enzalutamide | 508 | 1.00 (ref) | |
| Docetaxel | 187 | 1.26 (1.04, 1.53) | 0.018 | ||
| OS | Enzalutamide | 508 | 1.00 (ref) | ||
| Docetaxel | 187 | 1.32 (1.07, 1.64) | 0.009 | ||
| Enzalutamide | TTTTD | Abiraterone | 290 | 1.00 (ref) | |
| Docetaxel | 132 | 1.36 (1.09, 1.70) | 0.008 | ||
| OS | Abiraterone | 290 | 1.00 (ref) | ||
| Docetaxel | 132 | 1.40 (1.09, 1.80) | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swami, U.; Sinnott, J.A.; Haaland, B.; Sayegh, N.; McFarland, T.R.; Tripathi, N.; Maughan, B.L.; Rathi, N.; Sirohi, D.; Nussenzveig, R.; et al. Treatment Pattern and Outcomes with Systemic Therapy in Men with Metastatic Prostate Cancer in the Real-World Patients in the United States. Cancers 2021, 13, 4951. https://doi.org/10.3390/cancers13194951
Swami U, Sinnott JA, Haaland B, Sayegh N, McFarland TR, Tripathi N, Maughan BL, Rathi N, Sirohi D, Nussenzveig R, et al. Treatment Pattern and Outcomes with Systemic Therapy in Men with Metastatic Prostate Cancer in the Real-World Patients in the United States. Cancers. 2021; 13(19):4951. https://doi.org/10.3390/cancers13194951
Chicago/Turabian StyleSwami, Umang, Jennifer Anne Sinnott, Benjamin Haaland, Nicolas Sayegh, Taylor Ryan McFarland, Nishita Tripathi, Benjamin L. Maughan, Nityam Rathi, Deepika Sirohi, Roberto Nussenzveig, and et al. 2021. "Treatment Pattern and Outcomes with Systemic Therapy in Men with Metastatic Prostate Cancer in the Real-World Patients in the United States" Cancers 13, no. 19: 4951. https://doi.org/10.3390/cancers13194951