
Stroma AReactive Invasion Front Areas (SARIFA)—A New Easily to Determine Biomarker in Colon Cancer—Results of a Retrospective Study

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Groups
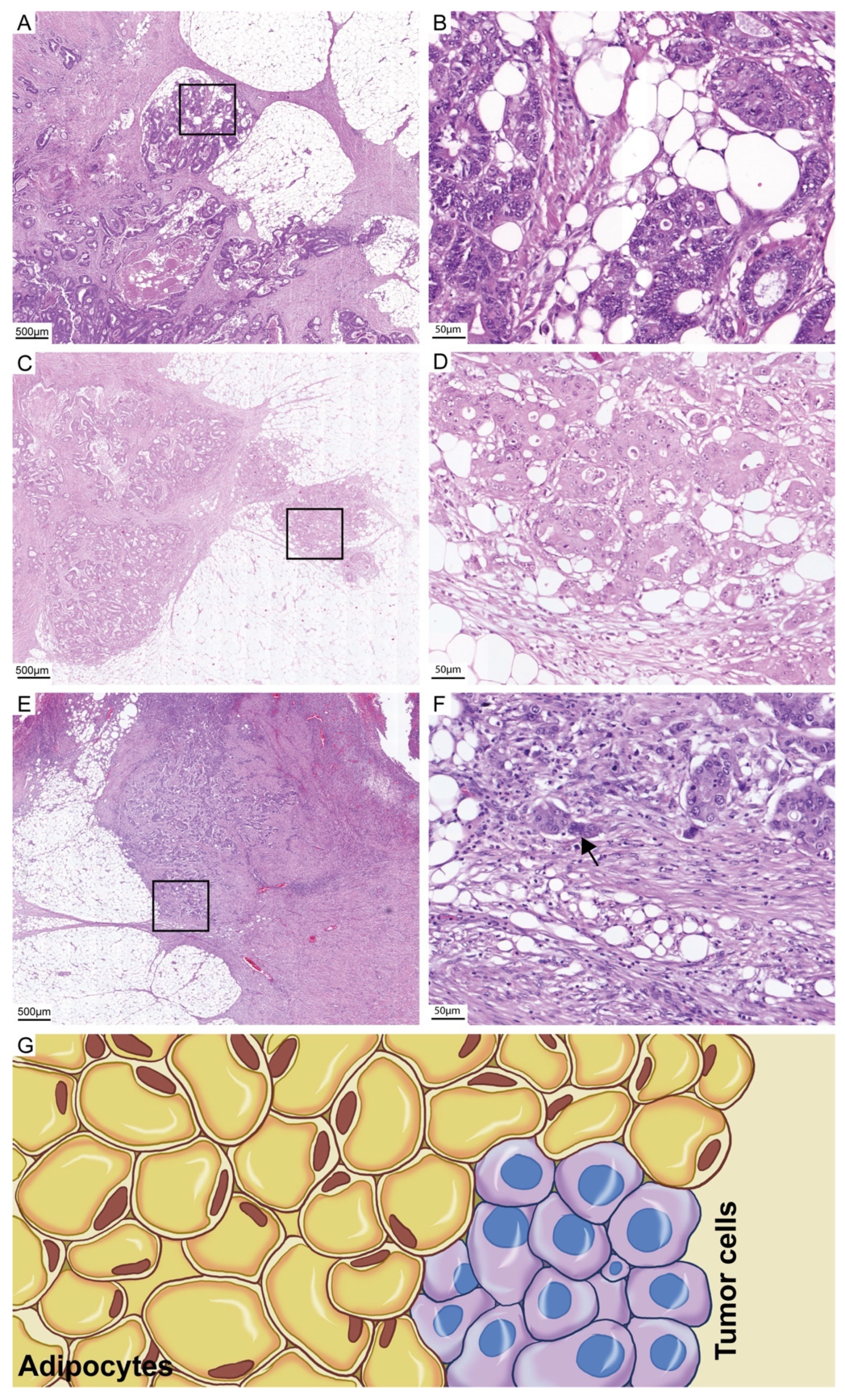
2.2. Definition and Assessment of SARIFA and Other Morphological Biomarkers
2.3. Statistical Analysis
3. Results
3.1. Duration of the Assessment and Interobserver Variability
3.2. Clinicopathological Characteristics
3.3. Characteristics of SARIFA-Positive Adenocarcinomas
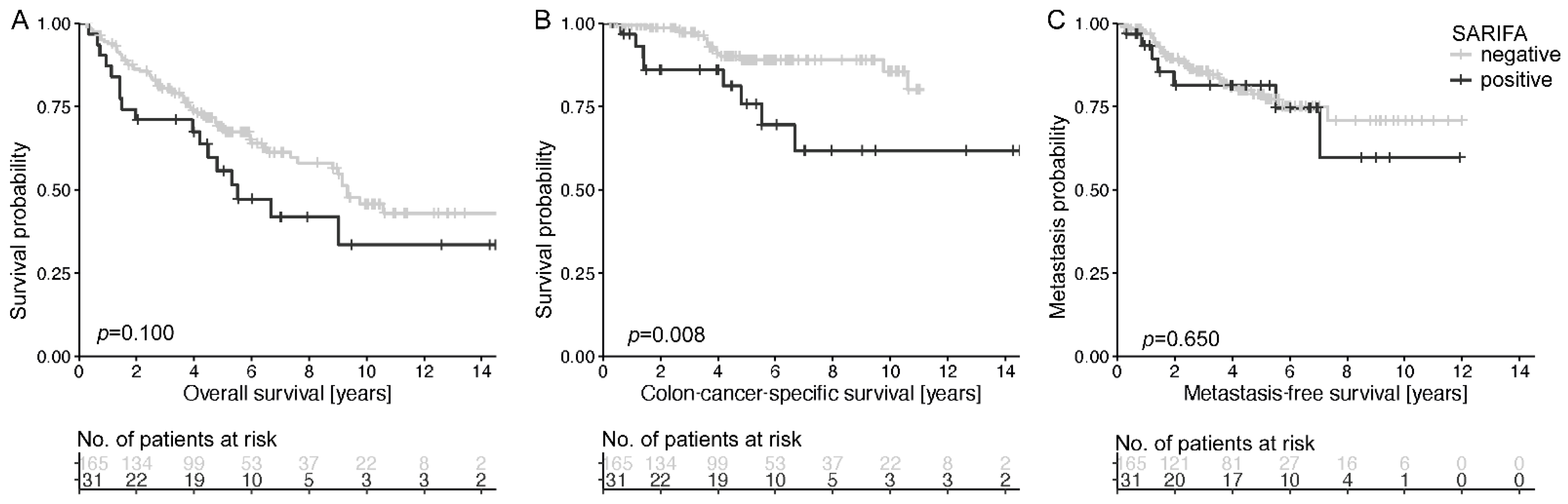
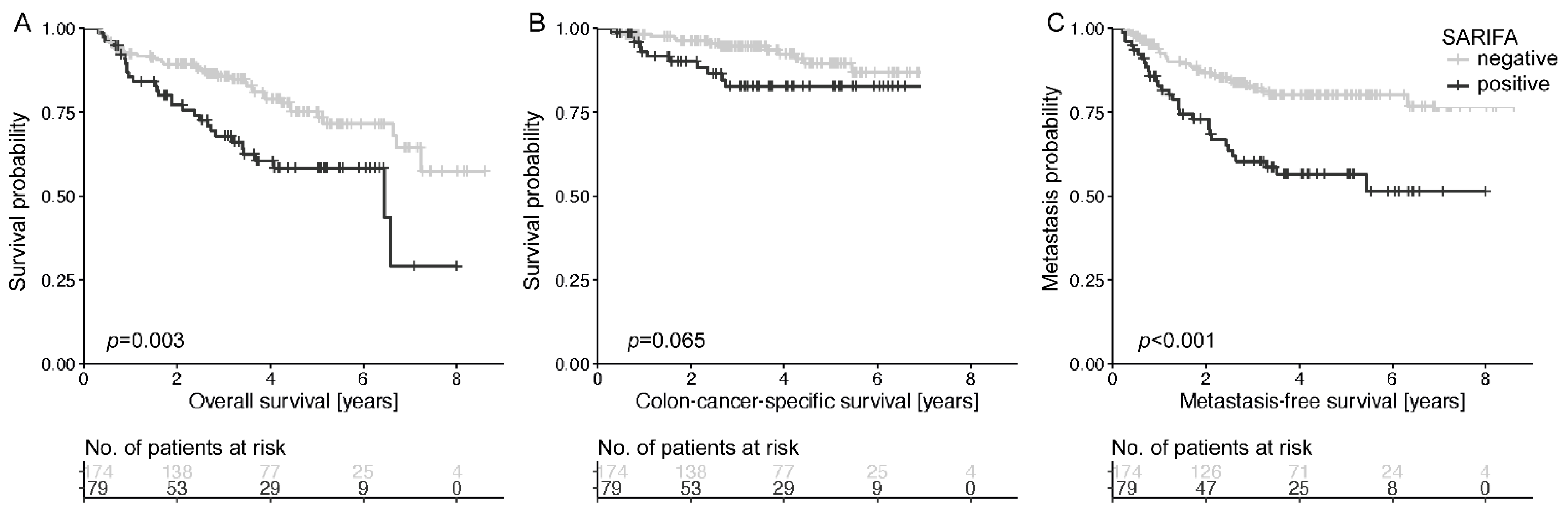
3.4. Univariate Prognostic Analyses
3.5. Multivariate Cox Regression
3.6. Analysis of SARIFA in T Stage Subgroups
3.7. Slide-Based Frequency of SARIFA and Correlation with Other Morphological Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Fleming, M.; Ravula, S.; Tatishchev, S.F.; Wang, H.L. Colorectal carcinoma: Pathologic aspects. J. Gastrointest. Oncol. 2012, 3, 153–173. [Google Scholar] [CrossRef] [PubMed]
- Marzouk, O.; Schofield, J. Review of histopathological and molecular prognostic features in colorectal cancer. Cancers 2011, 3, 2767–2810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jass, J.R.; Atkin, W.S.; Cuzick, J.; Bussey, H.J.; Morson, B.C.; Northover, J.M.; Todd, I.P. The grading of rectal cancer: Historical perspectives and a multivariate analysis of 447 cases. Histopathology 1986, 10, 437–459. [Google Scholar] [CrossRef] [PubMed]
- Jass, J.R.; Love, S.B.; Northover, J.M. A new prognostic classification of rectal cancer. Lancet 1987, 1, 1303–1306. [Google Scholar] [CrossRef]
- Jass, J.R.; Ajioka, Y.; Allen, J.P.; Chan, Y.F.; Cohen, R.J.; Nixon, J.M.; Radojkovic, M.; Restall, A.P.; Stables, S.R.; Zwi, L.J. Assessment of invasive growth pattern and lymphocytic infiltration in colorectal cancer. Histopathology 1996, 28, 543–548. [Google Scholar] [CrossRef]
- Koelzer, V.H.; Lugli, A. The tumor border configuration of colorectal cancer as a histomorphological prognostic indicator. Front. Oncol. 2014, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Jin, M.; Roth, R.; Rock, J.B.; Washington, M.K.; Lehman, A.; Frankel, W.L. The impact of tumor deposits on colonic adenocarcinoma AJCC TNM staging and outcome. Am. J. Surg. Pathol. 2015, 39, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Basnet, S.; Lou, Q.F.; Liu, N.; Rana, R.; Shah, A.; Khadka, M.; Warrier, H.; Sigdel, S.; Dhakal, S.; Devkota, A.; et al. Tumor deposit is an independent prognostic indicator in patients who underwent radical resection for colorectal cancer. J. Cancer 2018, 9, 3979–3985. [Google Scholar] [CrossRef]
- Hase, K.; Shatney, C.; Johnson, D.; Trollope, M.; Vierra, M. Prognostic value of tumor “budding” in patients with colorectal cancer. Dis. Colon. Rectum 1993, 36, 627–635. [Google Scholar] [CrossRef]
- Ueno, H.; Murphy, J.; Jass, J.; Mochizuki, H.; Talbot, I. Tumourbudding’as an index to estimate the potential of aggressiveness in rectal cancer. Histopathology 2002, 40, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Flejou, J.F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Mitrovic, B.; Schaeffer, D.F.; Riddell, R.H.; Kirsch, R. Tumor budding in colorectal carcinoma: Time to take notice. Mod. Pathol. 2012, 25, 1315–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koelzer, V.H.; Zlobec, I.; Lugli, A. Tumor budding in colorectal cancer—Ready for diagnostic practice? Hum. Pathol. 2016, 47, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.; Schafer, E.; Jakubowicz, E.; Mayr, P.; Ihringer, R.; Anthuber, M.; Schenkirsch, G.; Schaller, T.; Markl, B. Interobserver variability in the H&E-based assessment of tumor budding in pT3/4 colon cancer: Does it affect the prognostic relevance? Virchows Arch. 2018, 473, 189–197. [Google Scholar] [CrossRef]
- Kinoshita, O.; Kishimoto, M.; Murayama, Y.; Kuriu, Y.; Nakanishi, M.; Sakakura, C.; Otsuji, E.; Yanagisawa, A. The number of metastatic lymph nodes exhibiting poorly differentiated clusters predicts survival in patients with pStage III colorectal cancer. Int. J. Colorectal Dis. 2016, 31, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Barresi, V.; Branca, G.; Vitarelli, E.; Tuccari, G. Micropapillary pattern and poorly differentiated clusters represent the same biological phenomenon in colorectal cancer: A proposal for a change in terminology. Am. J. Clin. Pathol. 2014, 142, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Bonetti, L.R.; Barresi, V.; Bettelli, S.; Domati, F.; Palmiere, C. Poorly differentiated clusters (PDC) in colorectal cancer: What is and ought to be known. Diagn. Pathol. 2016, 11, 1–4. [Google Scholar]
- Ueno, H.; Kajiwara, Y.; Shimazaki, H.; Shinto, E.; Hashiguchi, Y.; Nakanishi, K.; Maekawa, K.; Katsurada, Y.; Nakamura, T.; Mochizuki, H.; et al. New criteria for histologic grading of colorectal cancer. Am. J. Surg. Pathol. 2012, 36, 193–201. [Google Scholar] [CrossRef]
- Park, J.; Richards, C.; McMillan, D.; Horgan, P.; Roxburgh, C. The relationship between tumour stroma percentage, the tumour microenvironment and survival in patients with primary operable colorectal cancer. Ann. Oncol. 2014, 25, 644–651. [Google Scholar] [CrossRef]
- Mesker, W.E.; Junggeburt, J.; Szuhai, K.; de Heer, P.; Morreau, H.; Tanke, H.J.; Tollenaar, R.A. The carcinoma–stromal ratio of colon carcinoma is an independent factor for survival compared to lymph node status and tumor stage. Anal. Cell. Pathol. 2007, 29, 387–398. [Google Scholar] [CrossRef]
- Mesker, W.E.; Liefers, G.J.; Junggeburt, J.M.; van Pelt, G.W.; Alberici, P.; Kuppen, P.J.; Miranda, N.F.; van Leeuwen, K.A.; Morreau, H.; Szuhai, K.; et al. Presence of a high amount of stroma and downregulation of SMAD4 predict for worse survival for stage I-II colon cancer patients. Cell. Oncol. 2009, 31, 169–178. [Google Scholar] [CrossRef]
- West, N.; Dattani, M.; McShane, P.; Hutchins, G.; Grabsch, J.; Mueller, W.; Treanor, D.; Quirke, P.; Grabsch, H. The proportion of tumour cells is an independent predictor for survival in colorectal cancer patients. Br. J. Cancer 2010, 102, 1519–1523. [Google Scholar] [CrossRef] [Green Version]
- Hynes, S.O.; Coleman, H.G.; Kelly, P.J.; Irwin, S.; O’Neill, R.F.; Gray, R.T.; McGready, C.; Dunne, P.D.; McQuaid, S.; James, J.A. Back to the future: Routine morphological assessment of the tumour microenvironment is prognostic in stage II/III colon cancer in a large population-based study. Histopathology 2017, 71, 12–26. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, A.C.; Sørensen, F.B.; Lindebjerg, J.; Hager, H.; Christensen, R.d.; Kjær-Frifeldt, S.; Hansen, T.F. The prognostic value of tumour stroma ratio and tumour budding in stage II colon cancer. A nationwide population-based study. Int. J. Colorectal Dis. 2018, 33, 1115–1124. [Google Scholar] [CrossRef] [Green Version]
- Van Pelt, G.W.; Kjaer-Frifeldt, S.; van Krieken, J.; Al Dieri, R.; Morreau, H.; Tollenaar, R.; Sorensen, F.B.; Mesker, W.E. Scoring the tumor-stroma ratio in colon cancer: Procedure and recommendations. Virchows Arch. 2018, 473, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.; Banner, B.M.; Schafer, E.M.; Mayr, P.; Anthuber, M.; Schenkirsch, G.; Markl, B. Tumor proportion in colon cancer: Results from a semiautomatic image analysis approach. Virchows Arch. 2020, 477, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Bokhorst, J.; Blank, A.; Lugli, A.; Zlobec, I.; Dawson, H.; Vieth, M.; Rijstenberg, L.; Brockmoeller, S.; Urbanowicz, M.; Flejou, J. Assessment of individual tumor buds using keratin immunohistochemistry: Moderate interobserver agreement suggests a role for machine learning. Mod. Pathol. 2020, 33, 825–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacking, S.; Angert, M.; Jin, C.; Kline, M.; Gupta, N.; Cho, M.; Thomas, R.; Lee, L.; Chavarria, H.; Nasim, M. Tumor budding in colorectal carcinoma: An institutional interobserver reliability and prognostic study of colorectal adenocarcinoma cases. Ann. Diagn. Pathol. 2019, 43, 151420. [Google Scholar] [CrossRef] [PubMed]
- Kai, K.; Aishima, S.; Aoki, S.; Takase, Y.; Uchihashi, K.; Masuda, M.; Nishijima-Matsunobu, A.; Yamamoto, M.; Ide, K.; Nakayama, A. Cytokeratin immunohistochemistry improves interobserver variability between unskilled pathologists in the evaluation of tumor budding in T1 colorectal cancer. Pathol. Int. 2016, 66, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, Y.A.; Xing, X.; Harris, J.W.; Zaytseva, Y.Y.; Mitov, M.I.; Napier, D.L.; Weiss, H.L.; Mark Evers, B.; Gao, T. Adipocytes activate mitochondrial fatty acid oxidation and autophagy to promote tumor growth in colon cancer. Cell Death Dis. 2017, 8, e2593. [Google Scholar] [CrossRef]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting recommendations for tumor marker prognostic studies (REMARK): Explanation and elaboration. BMC Med. 2012, 10, 51. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Ueno, H.; Hase, K.; Hashiguchi, Y.; Shimazaki, H.; Tanaka, M.; Miyake, O.; Masaki, T.; Shimada, Y.; Kinugasa, Y.; Mori, Y.; et al. Site-specific tumor grading system in colorectal cancer: Multicenter pathologic review of the value of quantifying poorly differentiated clusters. Am. J. Surg. Pathol. 2014, 38, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Hacking, S.M.; Chakraborty, B.; Nasim, R.; Vitkovski, T.; Thomas, R. A Holistic Appraisal of Stromal Differentiation in Colorectal Cancer: Biology, Histopathology, Computation, and Genomics. Pathol. Res. Pract. 2021, 220, 153378. [Google Scholar] [CrossRef] [PubMed]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Zlobec, I.; Baker, K.; Minoo, P.; Hayashi, S.; Terracciano, L.; Lugli, A. Tumor border configuration added to TNM staging better stratifies stage II colorectal cancer patients into prognostic subgroups. Cancer 2009, 115, 4021–4029. [Google Scholar] [CrossRef]
- Kubota, Y.; Petras, R.E.; Easley, K.A.; Bauer, T.W.; Tubbs, R.R.; Fazio, V.W. Ki-67-determined growth fraction versus standard staging and grading parameters in colorectal carcinoma. A multivariate analysis. Cancer 1992, 70, 2602–2609. [Google Scholar] [CrossRef] [Green Version]
- Martin, B.; Mayr, P.; Ihringer, R.; Schafer, E.M.; Jakubowicz, E.; Anthuber, M.; Schenkirsch, G.; Schaller, T.; Markl, B. Interobserver Variability in the Assessment of Tumor Budding in pT 3/4 Colon Cancer: Improvement by Supporting Immunohistochemistry? Diagnostics 2020, 10, 730. [Google Scholar] [CrossRef]
- Puppa, G.; Senore, C.; Sheahan, K.; Vieth, M.; Lugli, A.; Zlobec, I.; Pecori, S.; Wang, L.M.; Langner, C.; Mitomi, H.; et al. Diagnostic reproducibility of tumour budding in colorectal cancer: A multicentre, multinational study using virtual microscopy. Histopathology 2012, 61, 562–575. [Google Scholar] [CrossRef]
- Shivji, S.; Conner, J.R.; Barresi, V.; Kirsch, R. Poorly differentiated clusters in colorectal cancer: A current review and implications for future practice. Histopathology 2020, 77, 351–368. [Google Scholar] [CrossRef]
- Wulczyn, E.; Steiner, D.F.; Moran, M.; Plass, M.; Reihs, R.; Tan, F.; Flament-Auvigne, I.; Brown, T.; Regitnig, P.; Chen, P.C.; et al. Interpretable survival prediction for colorectal cancer using deep learning. NPJ Digit. Med. 2021, 4, 71. [Google Scholar] [CrossRef] [PubMed]
- Lengyel, E.; Makowski, L.; DiGiovanni, J.; Kolonin, M.G. Cancer as a matter of fat: The crosstalk between adipose tissue and tumors. Trends Cancer 2018, 4, 374–384. [Google Scholar] [CrossRef]
- Zhou, J.; Tang, Z.; Gao, S.; Li, C.; Feng, Y.; Zhou, X. Tumor-Associated Macrophages: Recent Insights and Therapies. Front. Oncol. 2020, 10, 188. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.B.; Schaeffer, D.F. Tumor budding as a standardized parameter in gastrointestinal carcinomas: More than just the colon. Mod. Pathol. 2018, 31, 862–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lugli, A.; Zlobec, I.; Berger, M.D.; Kirsch, R.; Nagtegaal, I.D. Tumour budding in solid cancers. Nat. Rev. Clin. Oncol. 2021, 18, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Zlobec, I.; Lugli, A. Epithelial mesenchymal transition and tumor budding in aggressive colorectal cancer: Tumor budding as oncotarget. Oncotarget 2010, 1, 651–661. [Google Scholar] [CrossRef] [Green Version]
- Grigore, A.D.; Jolly, M.K.; Jia, D.; Farach-Carson, M.C.; Levine, H. Tumor Budding: The Name is EMT. Partial EMT. J. Clin. Med. 2016, 5, 51. [Google Scholar] [CrossRef] [PubMed]
- Tarin, D.; Thompson, E.W.; Newgreen, D.F. The fallacy of epithelial mesenchymal transition in neoplasia. Cancer Res. 2005, 65, 5996–6000; discussion 6000-1. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | n = 196 | SARIFA-Positive (n = 31) | SARIFA-Negative (n = 165) | p-Value/p-Value Adjusted * | ||||
|---|---|---|---|---|---|---|---|---|
| Median Age [years] | 71 (64–79) | 70 (64–74) | 72(64–79) | 0.129/1.0 | ||||
| Median Follow-up (95% CI) [years] | 6.4 (5.6–7.1) | 6.0 (5.5–6.6) | 7.0 (5.0–9.1) | 0.581/1.0 | ||||
| Median Lymph Node Harvest (n) | 20 (13–30) | 20 (15–40) | 19 (13–29) | 0.254/1.0 | ||||
| Positive Lymph Nodes (n) | 0 (0–1) | 1 (0–4) | 0 (0–1) | 0.002/0.036 | ||||
| Sex | 0.843/1.0 | |||||||
| female | 83 | 42% | 14 | 45% | 69 | 42% | ||
| male | 113 | 58% | 17 | 55% | 96 | 58% | ||
| T status | 0.229/1.0 | |||||||
| pT3 | 172 | 88% | 25 | 81% | 147 | 89% | ||
| pT4 | 24 | 12% | 6 | 19% | 18 | 11% | ||
| N status | 0.009/0.144 | |||||||
| negative | 119 | 61% | 12 | 39% | 107 | 65% | ||
| positive | 77 | 39% | 19 | 61% | 58 | 35% | ||
| Grading | 0.020/0.280 | |||||||
| low grade | 137 | 70% | 16 | 52% | 121 | 73% | ||
| high grade | 59 | 30% | 15 | 48% | 44 | 27% | ||
| Vascular Invasion | 0.098/1.0 | |||||||
| negative | 176 | 90% | 25 | 81% | 151 | 91% | ||
| positive | 20 | 10% | 6 | 19% | 14 | 9% | ||
| Lymphatic Vessel Invasion | 0.602/1.0 | |||||||
| negative | 164 | 84% | 25 | 81% | 139 | 84% | ||
| positive | 32 | 16% | 6 | 19% | 26 | 16% | ||
| Tumor Budding | 0.004/0.068 | |||||||
| Bd1 | 161 | 82% | 20 | 65% | 141 | 86% | ||
| Bd2 | 23 | 12% | 6 | 19% | 17 | 10% | ||
| Bd3 | 12 | 6% | 5 | 16% | 7 | 4% | ||
| Location | 0.841/1.0 | |||||||
| right sided | 120 | 61% | 20 | 65% | 100 | 61% | ||
| left sided | 76 | 39% | 11 | 36% | 65 | 39% | ||
| MSS | 0.773/1.0 | |||||||
| stable | 172 | 88% | 28 | 90% | 144 | 87% | ||
| instable | 24 | 12% | 3 | 10% | 21 | 13% | ||
| Adjuvant Chemotherapy | 0.123/1.0 | |||||||
| no | 107 | 55% | 13 | 42% | 94 | 57% | ||
| yes | 89 | 45% | 18 | 58% | 71 | 43% | ||
| Distant Metastasis | 0.624/1.0 | |||||||
| no | 158 | 81% | 24 | 77% | 134 | 81% | ||
| yes | 38 | 19% | 7 | 23% | 31 | 19% | ||
| Death | 0.113/1.0 | |||||||
| no | 115 | 59% | 14 | 45% | 101 | 61% | ||
| death | 81 | 41% | 17 | 55% | 64 | 39% | ||
| Colon-Cancer-Specific Survival | 0.014/0.210 | |||||||
| no | 173 | 88% | 23 | 74% | 150 | 91% | ||
| death | 23 | 12% | 8 | 26% | 15 | 9% | ||
| Five Year Survival (n = 152) | 0.272/1.0 | |||||||
| survived | 92 | 60% | 13 | 50% | 79 | 63% | ||
| death | 60 | 40% | 13 | 50% | 47 | 37% | ||
| Variable | n = 253 | SARIFA-Positive (n = 79) | SARIFA-Negative (n = 174) | p-Value * | ||||
|---|---|---|---|---|---|---|---|---|
| Median Age [years] | 71 (61–77) | 72 (61–78) | 71 (61–77) | 0.658/1.0 | ||||
| Median Follow-up [years] | 4.2 (4.0–4.4) | 4.2 (3.9–4.5) | 4.2 (3.7–4.7) | 0.094/0.595 | ||||
| Median Lymph Node Harvest (n) | 38 (29–49) | 36 (28–53) | 39 (30–49) | 0.695/1.0 | ||||
| Positive Lymph Nodes (n) | 0 (0–2) | 1 (0–4) | 0 (0–1) | <0.001/0.009 | ||||
| Sex | 0.02/0.160 | |||||||
| female | 110 | 44% | 43 | 54% | 67 | 39% | ||
| male | 143 | 57% | 36 | 46% | 107 | 62% | ||
| T status | <0.001/0.009 | |||||||
| pT3 | 179 | 71% | 43 | 54% | 136 | 78% | ||
| pT4 | 74 | 29% | 36 | 46% | 38 | 22% | ||
| N status | <0.001/0.009 | |||||||
| negative | 144 | 57% | 25 | 32% | 119 | 68% | ||
| positive | 109 | 43% | 54 | 68% | 55 | 32% | ||
| Grading | 0.015/0.150 | |||||||
| low grade | 213 | 84% | 60 | 76% | 153 | 88% | ||
| high grade | 40 | 16% | 19 | 24% | 21 | 12% | ||
| Vascular Invasion | 0.016/0.150 | |||||||
| negative | 218 | 86% | 62 | 79% | 156 | 90% | ||
| positive | 35 | 14% | 17 | 21% | 18 | 10% | ||
| Lymphatic Vessel Invasion | <0.001/0.009 | |||||||
| negative | 197 | 78% | 50 | 63% | 147 | 85% | ||
| positive | 56 | 22% | 29 | 37% | 27 | 16% | ||
| Tumor Budding | <0.001/0.009 | |||||||
| Bd1 | 161 | 63% | 33 | 42% | 128 | 74% | ||
| Bd2 | 50 | 20% | 27 | 34% | 23 | 13% | ||
| Bd3 | 42 | 17% | 19 | 24% | 23 | 13% | ||
| Location | 0.785/1.0 | |||||||
| right | 139 | 55% | 42 | 53% | 97 | 56% | ||
| left | 114 | 45% | 37 | 47% | 77 | 44% | ||
| MSS | 0.580/1.0 | |||||||
| stable | 213 | 84% | 68 | 86% | 145 | 83% | ||
| instable | 40 | 16% | 11 | 14% | 29 | 17% | ||
| Adjuvant Chemotherapy | 0.009/0.108 | |||||||
| no | 164 | 65% | 42 | 53% | 122 | 70% | ||
| yes | 89 | 35% | 37 | 47% | 52 | 30% | ||
| Distant Metastasis | <0.001/0.009 | |||||||
| no | 192 | 76% | 48 | 61% | 144 | 83% | ||
| yes | 61 | 24% | 31 | 39% | 30 | 17% | ||
| Death | 0.009/0.108 | |||||||
| no | 185 | 73% | 49 | 62% | 136 | 78% | ||
| death | 68 | 27% | 30 | 38% | 38 | 22% | ||
| Colon-Cancer-Specific Survival | 0.105/0.595 | |||||||
| no | 229 | 90% | 68 | 86% | 161 | 92% | ||
| death | 24 | 10% | 11 | 14% | 13 | 8% | ||
| Five Year Survival (n = 117) | 0..085/0.595 | |||||||
| survived | 65 | 56% | 20 | 44% | 45 | 63% | ||
| death | 52 | 44% | 25 | 56% | 27 | 38% | ||
| Variation | Group A (n = 196) | Group B (n = 253) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Colon-Cancer-Specific Survival | Metastasis | Overall Survival | |||||||
| HR | CI | p | HR | CI | p | HR | CI | p | |
| T-status | 1.4 | 0.4–5.0 | 0.57 | 2.1 | 1.9–3.6 | 0.01 | 1.4 | 0.8–2.4 | 0.20 |
| N-status | 1.8 | 0.7–4.6 | 0.26 | 3.1 | 1.6–5.7 | <0.001 | 2.0 | 1.2–3.5 | 0.01 |
| Age | 1.1 | 1.0–1.1 | 0.02 | 1.0 | 0.9–1.0 | 0.15 | 1.05 | 1.0–1.1 | <0.001 |
| V | 0.9 | 0.3–3.2 | 0.89 | 1.0 | 0.5–2.0 | 0.99 | 0.9 | 0.4–1.7 | 0.65 |
| L | 1.3 | 0.4–4.1 | 0.65 | 1.6 | 0.9–2.8 | 0.14 | 1.5 | 0.9–2.7 | 0.13 |
| Grading | 0.9 | 0.4–2.2 | 0.82 | 1.5 | 0.8–3.0 | 0.23 | 2.0 | 1.0–3.8 | 0.04 |
| Tumor Budding | 0.9 | 0.5–1.9 | 0.88 | 0.9 | 0.7–1.3 | 0.59 | 1.1 | 0.8–1.5 | 0.71 |
| Location | 1.9 | 0.8–4.5 | 0.14 | 0.9 | 0.5–1.5 | 0.64 | 1.2 | 0.7–2.0 | 0.52 |
| MSS | 0.3 | 0.0–2.6 | 0.29 | 0.7 | 0.3–1.6 | 0.39 | 0.7 | 0.3–1.5 | 0.40 |
| SARIFA | 3.5 | 1.3–9.1 | 0.01 | 1.5 | 0.8–2.6 | 0.18 | 1.5 | 0.9–2.5 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, B.; Grosser, B.; Kempkens, L.; Miller, S.; Bauer, S.; Dhillon, C.; Banner, B.M.; Brendel, E.-M.; Sipos, É.; Vlasenko, D.; et al. Stroma AReactive Invasion Front Areas (SARIFA)—A New Easily to Determine Biomarker in Colon Cancer—Results of a Retrospective Study. Cancers 2021, 13, 4880. https://doi.org/10.3390/cancers13194880
Martin B, Grosser B, Kempkens L, Miller S, Bauer S, Dhillon C, Banner BM, Brendel E-M, Sipos É, Vlasenko D, et al. Stroma AReactive Invasion Front Areas (SARIFA)—A New Easily to Determine Biomarker in Colon Cancer—Results of a Retrospective Study. Cancers. 2021; 13(19):4880. https://doi.org/10.3390/cancers13194880
Chicago/Turabian StyleMartin, Benedikt, Bianca Grosser, Lana Kempkens, Silvia Miller, Svenja Bauer, Christine Dhillon, Bettina Monika Banner, Eva-Maria Brendel, Éva Sipos, Dmytro Vlasenko, and et al. 2021. "Stroma AReactive Invasion Front Areas (SARIFA)—A New Easily to Determine Biomarker in Colon Cancer—Results of a Retrospective Study" Cancers 13, no. 19: 4880. https://doi.org/10.3390/cancers13194880