
Regorafenib in Recurrent Glioblastoma Patients: A Large and Monocentric Real-Life Study

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
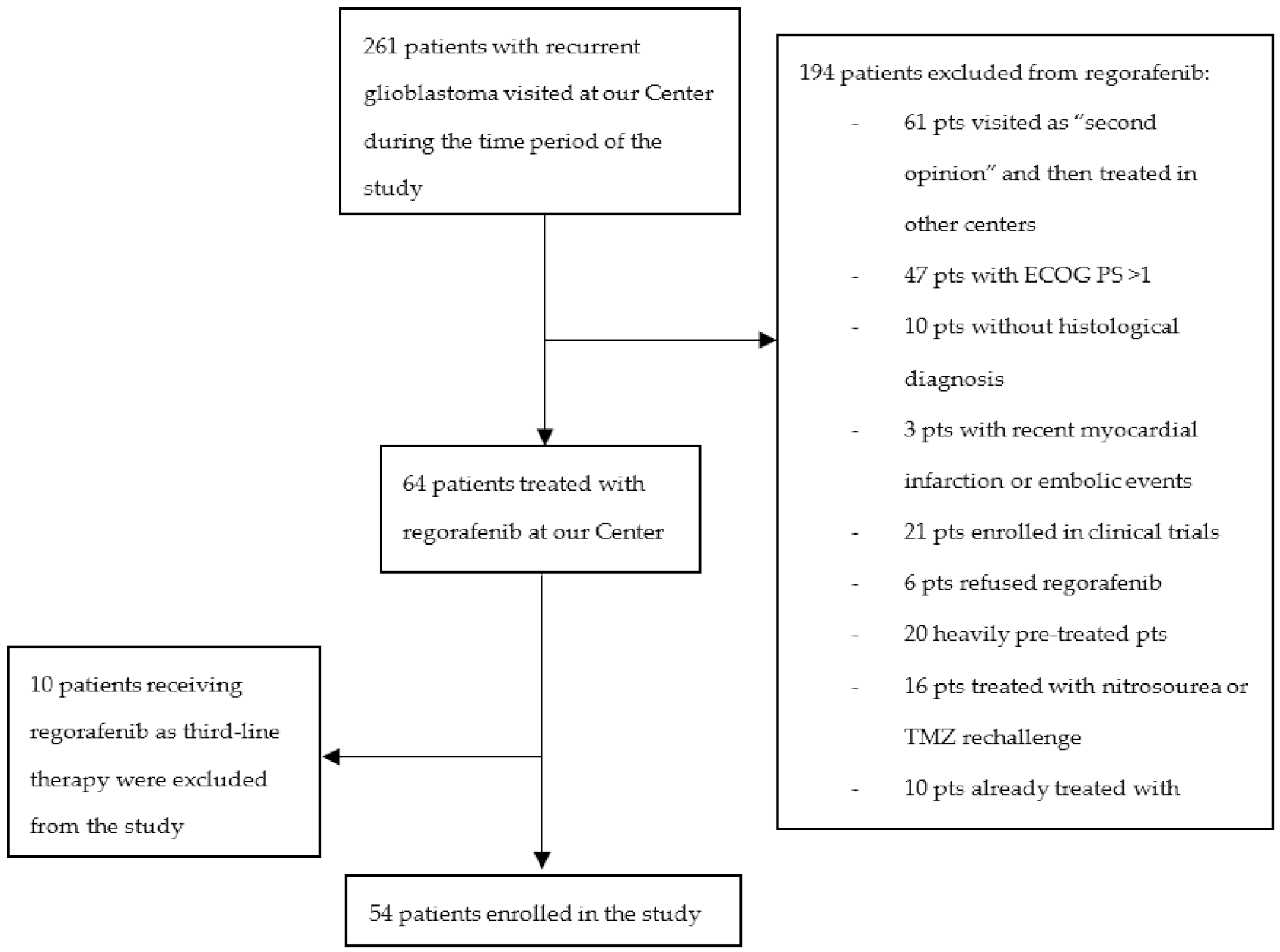
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro-Oncology 2020, 22, iv1–iv96. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Rønning, P.A.; Helseth, E.; Meling, T.R.; Johannesen, T.B. A population-based study on the effect of temozolomide in the treatment of glioblastoma multiforme. Neuro-Oncology 2012, 14, 1178–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Tonn, J.C.; Stupp, R.; Preusser, M.; Cohen-Jonathan-Moyal, E.; Henriksson, R.; Le Rhun, E.; Balana, C.; Chinot, O.; et al. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017, 18, e315–e329. [Google Scholar] [CrossRef] [Green Version]
- Minniti, G.; Lombardi, G.; Paolini, S. Glioblastoma in Elderly Patients: Current Management and Future Perspectives. Cancers 2019, 11, 336. [Google Scholar] [CrossRef] [Green Version]
- Di Stefano, A.L.; Labussiere, M.; Lombardi, G.; Eoli, M.; Bianchessi, D.; Pasqualetti, F.; Farina, P.; Cuzzubbo, S.; Gallego-Perez-Larraya, J.; Boisselier, B.; et al. VEGFA SNP rs2010963 is associated with vascular toxicity in recurrent glioblastomas and longer response to bevacizumab. J. Neurooncol. 2015, 121, 499–504. [Google Scholar] [CrossRef]
- Birzu, C.; French, P.; Caccese, M.; Cerretti, G.; Idbaih, A.; Zagonel, V.; Lombardi, G. Recurrent Glioblastoma: From Molecular Landscape to New Treatment Perspectives. Cancers 2020, 13, 47. [Google Scholar] [CrossRef]
- Lombardi, G.; Idbaih, A.; Le Rhun, E.; Preusser, M.; Zagonel, V.; French, P. A New Landscape for Systemic Pharmacotherapy of Recurrent Glioblastoma? Cancers 2020, 12, 3775. [Google Scholar] [CrossRef]
- Lombardi, G.; Barresi, V.; Indraccolo, S.; Simbolo, M.; Fassan, M.; Mandruzzato, S.; Simonelli, M.; Caccese, M.; Pizzi, M.; Fassina, A.; et al. Pembrolizumab Activity in Recurrent High-Grade Gliomas with Partial or Complete Loss of Mismatch Repair Protein Expression: A Monocentric, Observational and Prospective Pilot Study. Cancers 2020, 12, 2283. [Google Scholar] [CrossRef]
- Reardon, D.A.; Brandes, A.A.; Omuro, A.; Mulholland, P.; Lim, M.; Wick, A.; Baehring, J.; Ahluwalia, M.S.; Roth, P.; Bähr, O.; et al. Effect of Nivolumab vs Bevacizumab in Patients With Recurrent Glioblastoma: The CheckMate 143 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Lond. Engl. 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Demetri, G.D.; Reichardt, P.; Kang, Y.K.; Blay, J.Y.; Rutkowski, P.; Gelderblom, H.; Hohenberger, P.; Leahy, M.; von Mehren, M.; Joensuu, H.; et al. Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Lond. Engl. 2013, 381, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouche, O.; Mineur, L.; Barone, C.; et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet Lond. Engl. 2013, 381, 303–312. [Google Scholar] [CrossRef]
- Daudigeos-Dubus, E.; Le Dret, L.; Lanvers-Kaminsky, C.; Bawa, O.; Opolon, P.; Vievard, A.; Villa, I.; Pagès, M.; Bosq, J.; Vassal, G.; et al. Regorafenib: Antitumor Activity upon Mono and Combination Therapy in Preclinical Pediatric Malignancy Models. PLoS ONE 2015, 10, e0142612. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schütz, G.; Thierauch, K.-H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2011, 129, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; De Salvo, G.L.; Brandes, A.A.; Eoli, M.; Ruda, R.; Faedi, M.; Lolli, I.; Pace, A.; Daniele, B.; Pasqualetti, F.; et al. Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet Oncol. 2019, 20, 110–119. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE—Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermosifiliogr. 2020, 112, 90–92. [Google Scholar] [CrossRef]
- Kreisl, T.N.; Kim, L.; Moore, K.; Duic, P.; Royce, C.; Stroud, I.; Garren, N.; Mackey, M.; Butman, J.A.; Camphausen, K.; et al. Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 740–745. [Google Scholar] [CrossRef]
- Friedman, H.S.; Prados, M.D.; Wen, P.Y.; Mikkelsen, T.; Schiff, D.; Abrey, L.E.; Yung, W.K.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef] [Green Version]
- Brandes, A.A.; Finocchiaro, G.; Zagonel, V.; Reni, M.; Caserta, C.; Fabi, A.; Clavarezza, M.; Maiello, E.; Eoli, M.; Lombardi, G.; et al. AVAREG: A phase II, randomized, noncomparative study of fotemustine or bevacizumab for patients with recurrent glioblastoma. Neuro-Oncology. 2016, 18, 1304–1312. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, A.; Herndon, J.E.; McSherry, F.; Ravelo, A.; Lipp, E.S.; Healy, P.; Peters, K.B.; Sampson, J.H.; Randazzo, D.; Sommer, N.; et al. Single-institution retrospective review of patients with recurrent glioblastoma treated with bevacizumab in clinical practice. Health Sci. Rep. 2019, 2, e114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cloughesy, T.F.; Landolfi, J.; Hogan, D.J.; Bloomfield, S.; Carter, B.; Chen, C.C.; Elder, J.B.; Kalkanis, S.N.; Kesari, S.; Lai, A.; et al. Phase 1 trial of vocimagene amiretrorepvec and 5-fluorocytosine for recurrent high-grade glioma. Sci. Transl. Med. 2016, 8, 341ra75. [Google Scholar] [CrossRef] [Green Version]
- Cloughesy, T.F.; Petrecca, K.; Walbert, T.; Butowski, N.; Salacz, M.; Perry, J.; Damek, D.; Bota, D.; Bettegowda, C.; Zhu, J.-J.; et al. Effect of Vocimagene Amiretrorepvec in Combination With Flucytosine vs Standard of Care on Survival Following Tumor Resection in Patients With Recurrent High-Grade Glioma: A Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1939–1946. [Google Scholar] [CrossRef]
- Desjardins, A.; Gromeier, M.; Herndon, J.E.; Beaubier, N.; Bolognesi, D.P.; Friedman, A.H.; Friedman, H.S.; McSherry, F.; Muscat, A.M.; Nair, S.; et al. Recurrent Glioblastoma Treated with Recombinant Poliovirus. N. Engl. J. Med. 2018, 379, 150–161. [Google Scholar] [CrossRef]
- Santangelo, A.; Rossato, M.; Lombardi, G.; Benfatto, S.; Lavezzari, D.; De Salvo, G.L.; Indraccolo, S.; Dechecchi, M.C.; Prandini, P.; Gambari, R.; et al. A Molecular Signature associated with prolonged survival in Glioblastoma patients treated with Regorafenib. Neuro-Oncology 2020, 23, 264–276. [Google Scholar] [CrossRef]
- Indraccolo, S.; De Salvo, G.L.; Verza, M.; Caccese, M.; Esposito, G.; Piga, I.; Del Bianco, P.; Pizzi, M.; Gardiman, M.P.; Eoli, M.; et al. Phosphorylated Acetyl-CoA Carboxylase Is Associated with Clinical Benefit with Regorafenib in Relapsed Glioblastoma: REGOMA Trial Biomarker Analysis. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 4478–4484. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.T.; Swanson, K.D. Dexamethasone-Friend or Foe for Patients With Glioblastoma? JAMA Neurol. 2019, 76, 247–248. [Google Scholar] [CrossRef]
- Lombardi, G.; Del Bianco, P.; Brandes, A.A.; Eoli, M.; Rudà, R.; Ibrahim, T.; Lolli, I.; Rizzato, S.; Daniele, B.; Pace, A.; et al. Patient-reported outcomes in a phase II randomised study of regorafenib compared with lomustine in patients with relapsed glioblastoma (the REGOMA trial). Eur. J. Cancer 2021, 155, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Kebir, S.; Rauschenbach, L.; Radbruch, A.; Lazaridis, L.; Schmidt, T.; Stoppek, A.-K.; Pierscianek, D.; Stuschke, M.; Forsting, M.; Sure, U.; et al. Regorafenib in patients with recurrent high-grade astrocytoma. J. Cancer Res. Clin. Oncol. 2019, 145, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Tzaridis, T.; Gepfner-Tuma, I.; Hirsch, S.; Skardelly, M.; Bender, B.; Paulsen, F.; Schaub, C.; Weller, J.; Schäfer, N.; Herrlinger, U.; et al. Regorafenib in advanced high-grade glioma: A retrospective bicentric analysis. Neuro-Oncology 2019, 21, 954–955. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (%) |
|---|---|
| No. of patients | 54 (100) |
| Median Age (range) | 55 (30–77) |
| Gender | |
| Male | 38/54 (70.4) |
| Female | 16/54 (29.6) |
| Type of first surgery | |
| Radical surgery | 28/54 (52) |
| Partial surgery | 26/54 (48) |
| Stupp protocol completed | |
| yes | 35/54 (65) |
| no | 19/54 (35) |
| Median time from diagnosis to regorafenib therapy | 14.3 months |
| ECOG performance status | |
| 0–1 | 54 (100) |
| Surgery at time of recurrence | 16/54 (29.6) |
| Corticosteroid use | |
| yes | 22/54 (40.7) |
| no | 32/54 (59.3) |
| IDH mutation status | |
| wild-type | 49/54 (90.7) |
| mutated | 5/54 (9.3) |
| MGMT methylation status | |
| methylated | 28/53 (52.8) |
| unmethylated | 25/53 (47.2) |
| Third-line therapy | |
| yes | 35/54 (65) |
| no | 19/54 (25) |
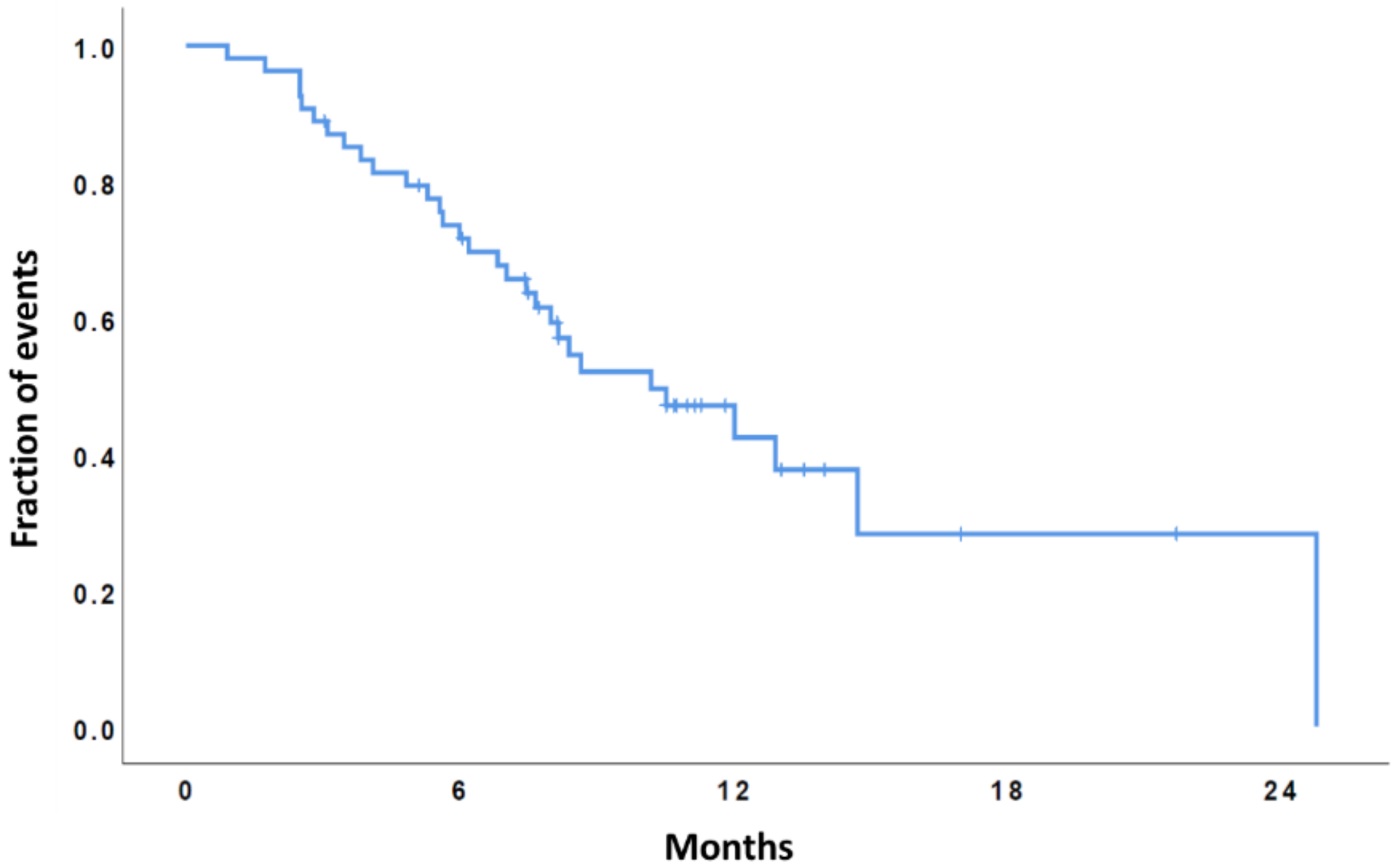
| Variable | OS | |||
|---|---|---|---|---|
| Median (Months) | 95% CI | p | ||
| MGMT Status | 0.20 | |||
| Met Unmet | 10.2 7.6 | 4.5–15.8 3.7–11.6 | ||
| IDH status | 0.37 | |||
| wt mut | 10.2 Not reached | 6.9–14.4 | ||
| Age | 0.17 | |||
| ≤65 years >65 years | 12.03 7.4 | 6.6–17.4 5.9–8.9 | ||
| Second surgery | 0.3 | |||
| yes | 12.9 | 4.4–21.4 | ||
| no | 8.6 | 4.7–12.5 | ||
| Steroid at baseline | 0.09 | |||
| yes | 7.4 | 4.7–10.2 | ||
| no | 12.9 | 9.2–16.6 | ||
| Third Line therapy | 0.8 | |||
| yes no | 10.2 8.0 | 6.3–14.02 0.01–16.9 | ||
| Variables | OS | |
|---|---|---|
| HR (95% CI) | p | |
| MGMT status (unmet vs. met) | 1.4 (0.6–3.05) | 0.3 |
| Age (≤65 vs. >65) | 0.4 (0.1–1.2) | 0.1 |
| Steroid at Baseline (no vs. yes) | 0.4 (0.2–1.06) | 0.07 |
| Overall Responses according to RANO Criteria | No. (%) |
|---|---|
| Complete Response | 0 (0) |
| Partial Response | 4 (7.4) |
| Objective Response Rate | 4 (7.4) |
| Stable Disease | 21 (38.9) |
| Disease Control rate | 25 (46.3) |
| Progressive Disease | 29 (53.7) |
| Adverse Events | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
| Hand and Foot skin reaction | 17 (31%) | 3 (5%) | 4 (7%) | |
| Hypertension | 7 (13%) | 3 (5%) | ||
| Fatigue | 17 (31%) | 7 (13%) | 1 (2%) | |
| Mucositis | 8 (15%) | 5 (9%) | 1 (2%) | |
| Dysphonia | 5 (9%) | |||
| Fever | 10 (18%) | 4 (7%) | ||
| Diarrhea | 6 (11%) | 1 (2%) | ||
| Blood Bilirubin Increased | 8 (15%) | 3 (5%) | ||
| Hypertransaminasaemia | 5 (9%) | 1 (2%) | 2 (4%) | |
| Serum Amylase/Lipase Increased | 1 (2%) | 1 (2%) | ||
| Skin Rash | 5 (9%) | 4 (5%) | 3 (5%) | 1 (2%) |
| Thrombocytopenia | 5 (9%) | 2 (4%) | ||
| Hypothyroidism | 2 (4%) | 1 (2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardi, G.; Caccese, M.; Padovan, M.; Cerretti, G.; Pintacuda, G.; Manara, R.; Di Sarra, F.; Zagonel, V. Regorafenib in Recurrent Glioblastoma Patients: A Large and Monocentric Real-Life Study. Cancers 2021, 13, 4731. https://doi.org/10.3390/cancers13184731
Lombardi G, Caccese M, Padovan M, Cerretti G, Pintacuda G, Manara R, Di Sarra F, Zagonel V. Regorafenib in Recurrent Glioblastoma Patients: A Large and Monocentric Real-Life Study. Cancers. 2021; 13(18):4731. https://doi.org/10.3390/cancers13184731
Chicago/Turabian StyleLombardi, Giuseppe, Mario Caccese, Marta Padovan, Giulia Cerretti, Giovanna Pintacuda, Renzo Manara, Francesca Di Sarra, and Vittorina Zagonel. 2021. "Regorafenib in Recurrent Glioblastoma Patients: A Large and Monocentric Real-Life Study" Cancers 13, no. 18: 4731. https://doi.org/10.3390/cancers13184731