
The Reality of Lung Cancer Paradox: The Impact of Body Mass Index on Long-Term Survival of Resected Lung Cancer. A French Nationwide Analysis from the Epithor Database

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Epithor, the French National Database of General Thoracic Surgery
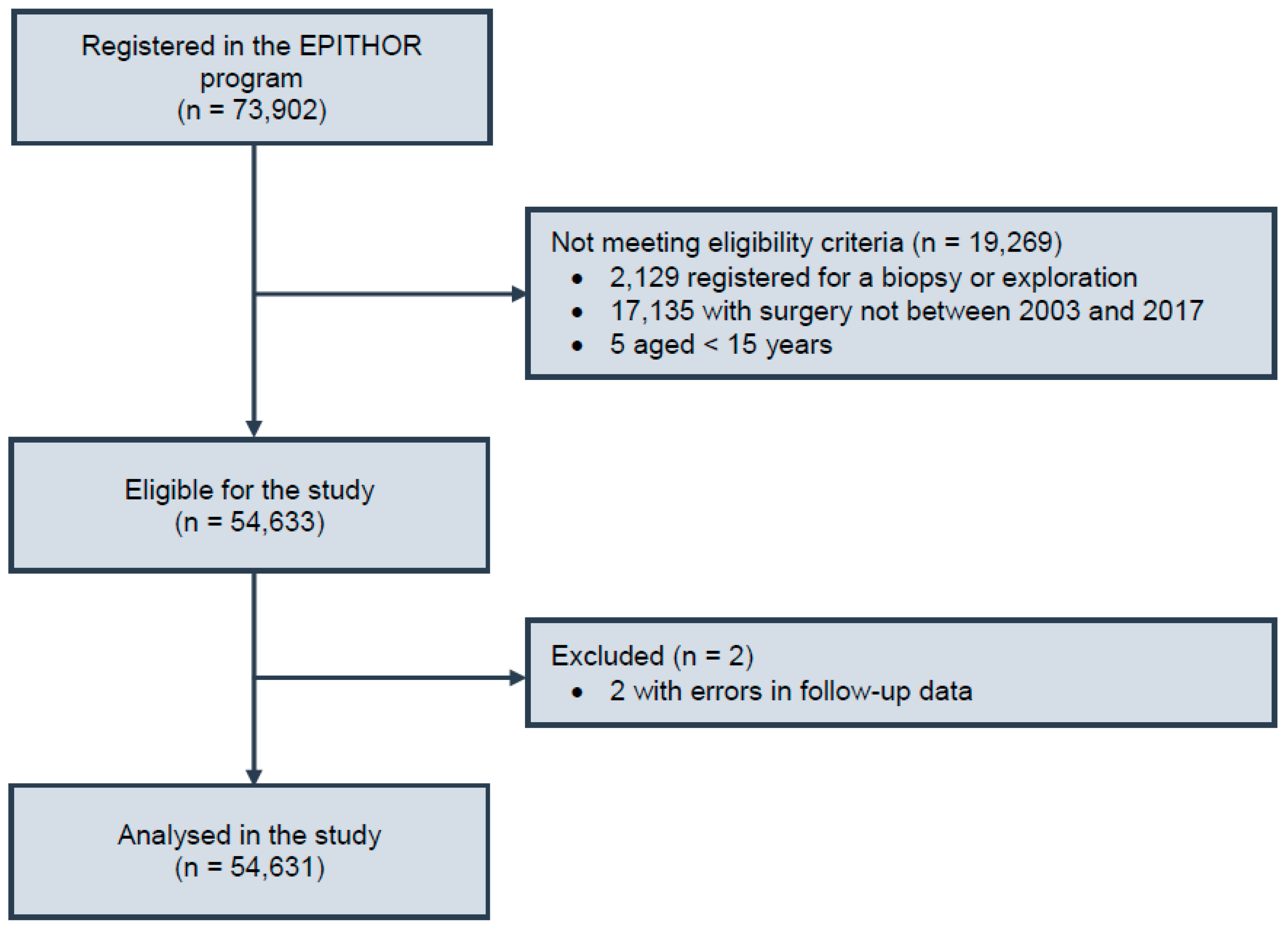
2.2. Patient Population
2.3. Retrieved Clinical Variables
2.4. Outcome Definition
2.5. Statistical Analysis
3. Results
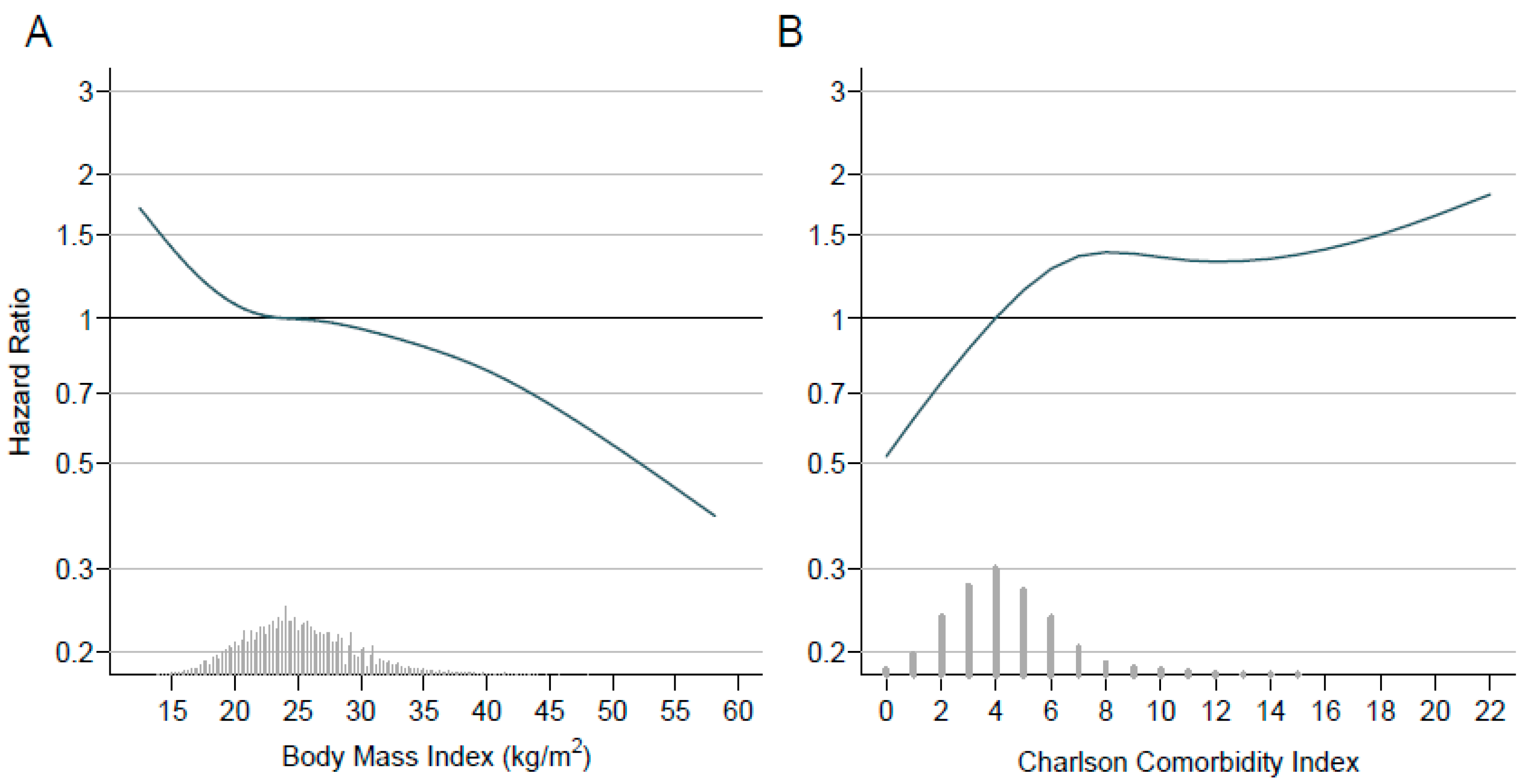
3.1. Correlations of BMI
3.2. Survival
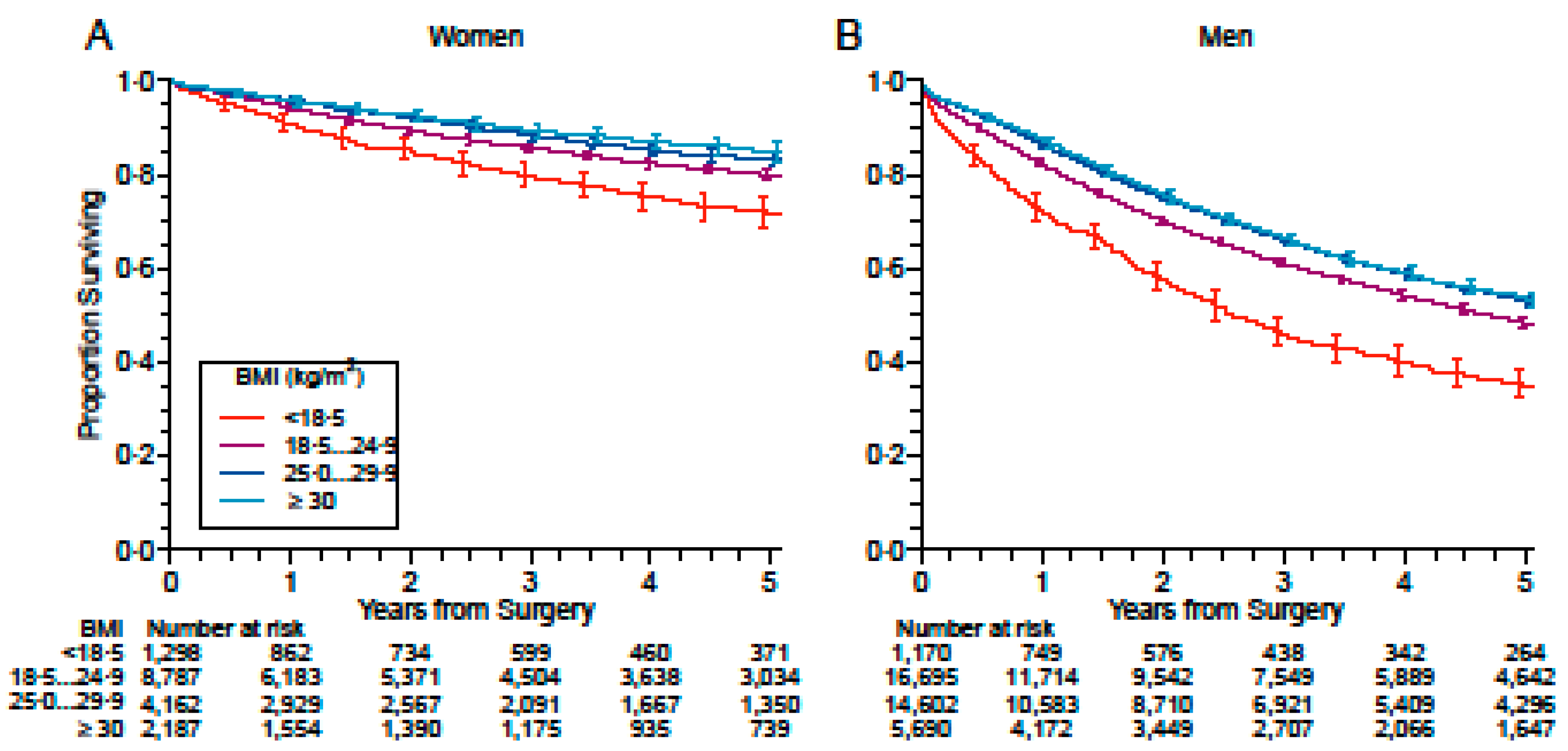
3.3. Stratification by Sex
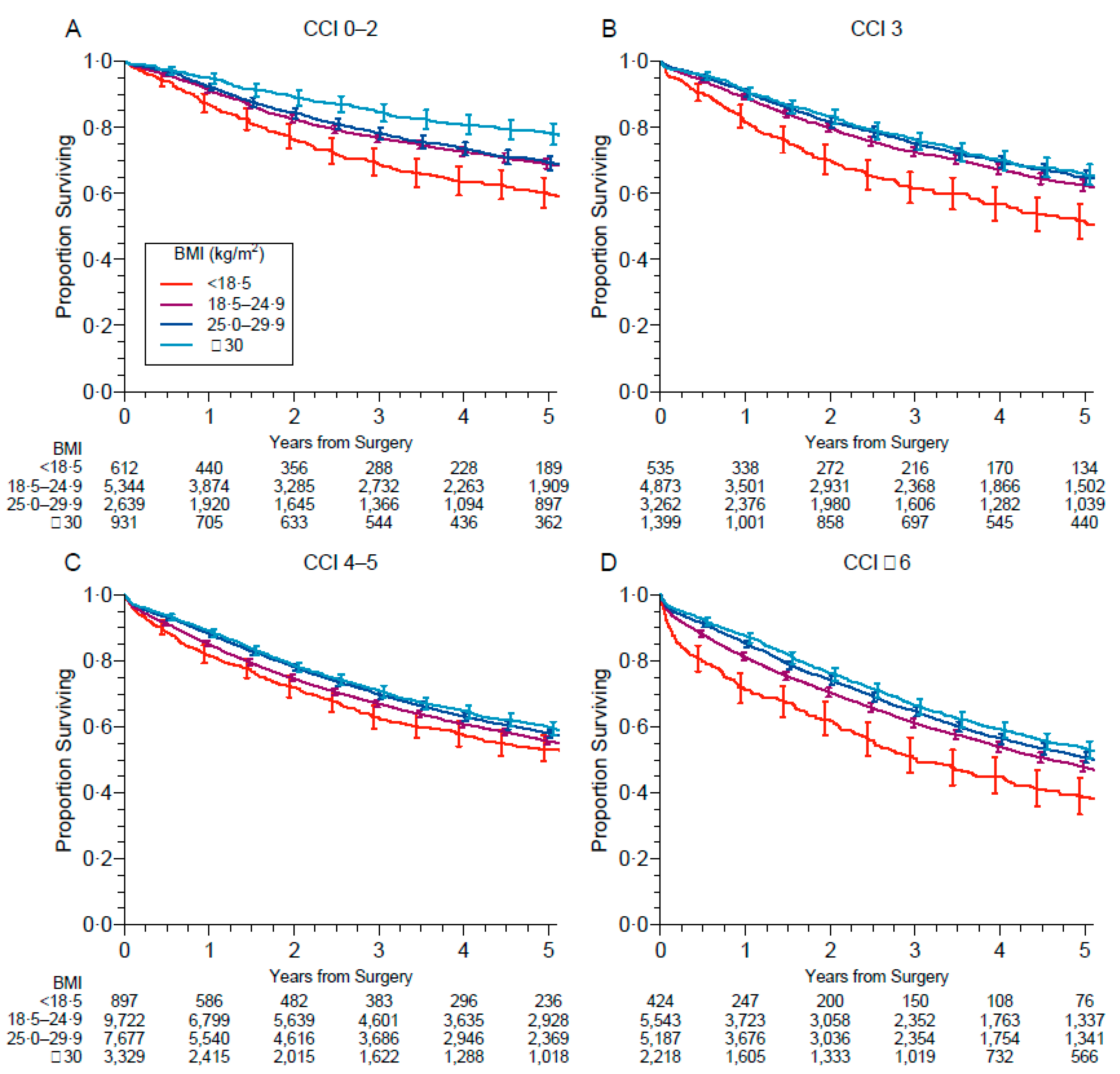
3.4. Subgroup Exploratory Analyses
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 March 2021).
- Stephen, N. Causes, consequences, and treatment of metabolically unhealthy fat distribution. Lancet Diabetes Endocrinol. 2020, 8, 616–627. [Google Scholar]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, pathophysiology, and management of obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Hillers-Ziemer, L.E.; Williams, A.E.; Janquart, A.; Grogan, C.; Thompson, V.; Sanchez, A.; Arendt, L.M. Obesity-Activated Lung Stromal Cells Promote Myeloid Lineage Cell Accumulation and Breast Cancer Metastasis. Cancers 2021, 13, 1005. [Google Scholar] [CrossRef] [PubMed]
- Cerda, C.; Sanchez, C.; Climent, B.; Vazquez, A.; Iradi, A.; El Amrani, F.; Bediaga, A.; Saez, G.T. Oxidative Stress and DNA Damage in Obesity-Related Tumorigenesis. In Oxidative Stress and Inflammation in Non-Communicable Diseases—Molecular Mechanisms and Perspectives in Therapeutics; Camps, J., Ed.; Book Series: Advances in Experimental Medicine and Biology; Springer: New York, NY, USA, 2014; Volume 824, pp. 5–17. [Google Scholar] [CrossRef]
- Saltiel, A.R.; Olefsky, J.M. Inflammatory mechanisms linking obesity and metabolic disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Sarode, P.; Schaefer, M.B.; Grimminger, F.; Seeger, W.; Savai, R. Macrophage and Tumor Cell Cross-Talk Is Fundamental for Lung Tumor Progression: We Need to Talk. Front. Oncol. 2020, 10, 324. [Google Scholar] [CrossRef] [Green Version]
- Bhaskaran, K.; Douglas, I.; Forbes, H.; Silva, I.D.S.; Leon, D.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5·24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Liu, Y.; Shao, H.; Zheng, X. Obesity Paradox in Lung Cancer Prognosis: Evolving Biological Insights and Clinical Implications. J. Thorac. Oncol. 2017, 12, 1478–1488. [Google Scholar] [CrossRef] [Green Version]
- Jaspan, V.; Lin, K.; Popov, V. The impact of anthropometric parameters on colorectal cancer prognosis: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2021, 159, 103232. [Google Scholar] [CrossRef]
- Kumar, S.; Mahmud, N.; Goldberg, D.S.; Datta, J.; Kaplan, D.E. Disentangling the obesity paradox in upper gastrointestinal cancers: Weight loss matters more than body mass index. Cancer Epidemiol. 2021, 72, 101912. [Google Scholar] [CrossRef] [PubMed]
- Lam, V.K.; Bentzen, S.M.; Mohindra, P.; Nichols, E.M.; Bhooshan, N.; Vyfhuis, M.; Scilla, K.A.; Feigenberg, S.J.; Edelman, M.J.; Feliciano, J.L. Obesity is associated with long-term improved survival in definitively treated locally advanced non-small cell lung cancer (NSCLC). Lung Cancer 2017, 104, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Hervochon, R.; Bobbio, A.; Guinet, C.; Mansuet-Lupo, A.; Rabbat, A.; Régnard, J.-F.; Roche, N.; Damotte, D.; Iannelli, A.; Alifano, M. Body Mass Index and Total Psoas Area Affect Outcomes in Patients Undergoing Pneumonectomy for Cancer. Ann. Thorac. Surg. 2017, 103, 287–295. [Google Scholar] [CrossRef] [Green Version]
- Fukumoto, K.; Mori, S.; Shintani, Y.; Okami, J.; Ito, H.; Ohtsuka, T.; Toyooka, S.; Mori, T.; Watanabe, S.-I.; Asamura, H.; et al. Impact of the preoperative body mass index on the postoperative outcomes in patients with completely resected non-small cell lung cancer: A retrospective analysis of 16,503 cases in a Japanese Lung Cancer Registry Study. Lung Cancer 2020, 149, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P.A.; Berbis, J.; Falcoz, P.E.; Le Pimpec-Barthes, F.; Bernard, A.; Jougon, J.; Porte, H.; Alifano, M.; Dahan, M.; EPITHOR Group. National perioperative outcomes of pulmonary lobectomy for cancer: The influence of nutritional status. Eur. J. Cardiothorac. Surg. 2014, 45, 652–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falcoz, P.E.; Conti, M.; Brouchet, L.; Chocron, S.; Puyraveau, M.; Mercier, M.; Etievent, J.P.; Dahan, M. The Thoracic Surgery Scoring System (Thoracoscore): Risk model for in-hospital death in 15,183 patients requiring thoracic surgery. J. Thorac. Cardiovasc. Surg. 2007, 133, 325–332.e1. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Cancer du Poumon, Bilan Initiale, Collection Reccomandations et Référentiel, Ouvrage Collectif édité par l’INCa. Boulogne-Billancourt. June 2021. Available online: https://www.e-cancer.fr>file>RECOPOUM11 (accessed on 15 June 2021).
- White, I.R.; Royston, P. Imputing missing covariate values for the Cox model. Stat. Med. 2009, 28, 1982–1998. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Rabe, K.F. Precision Diagnosis and Treatment for Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 849–861. [Google Scholar] [CrossRef] [Green Version]
- Vachani, A.; Sequist, L.V.; Spira, A. AJRCCM: 100-YearAnniversary.The Shifting Landscape for Lung Cancer: Past, Present, and Future. Am. J. Respir. Crit. Care Med. 2017, 195, 1150–1160. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.C.; Pastore, C.A.; Orlandi, S.P.; Heymsfield, S.B. Obesity paradox in cancer: New insights provided by body composition. Am. J. Clin. Nutr. 2014, 99, 999–1005. [Google Scholar] [CrossRef]
- Strulov Shachar, S.; Williams, G.R. The obesity paradox in cancer-moving beyond BMI. Cancer Epidemiol. Biomark. Prev. 2017, 26, 13–16. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Peterson, L.L.; Colditz, G.A. The Plausibility of Obesity Paradox in Cancer—Point. Cancer Res. 2018, 78, 1898–1903. [Google Scholar] [CrossRef] [Green Version]
- Cespedes Feliciano, E.M.; Kroenke, C.H.; Caan, B.J. The Obesity Paradox in Cancer: How Important Is Muscle? Annu. Rev. Nutr. 2018, 38, 357–379. [Google Scholar] [CrossRef]
- Özdemir, B.C.; Dotto, G.P. Racial differences in cancer susceptibility and survival: More than the color of the skin? Trends Cancer 2017, 3, 181–197. [Google Scholar] [CrossRef] [Green Version]
- Icard, P.; Schussler, O.; Loi, M.; Bobbio, A.; Lupo, A.M.; Wislez, M.; Iannelli, A.; Fournel, L.; Damotte, D.; Alifano, M. Pre-Disease and Pre-Surgery BMI, Weight Loss and Sarcopenia Impact Survival of Resected Lung Cancer Independently of Tumor Stage. Cancers 2020, 12, 266. [Google Scholar] [CrossRef] [Green Version]
- Icard, P.; Iannelli, A.; Lincet, H.; Alifano, M. Sarcopenia in resected non-small cell lung cancer: Let’s move to patient-directed strategies. J. Thorac. Dis. 2018, 10 (Suppl. 26), S3138–S3142. [Google Scholar] [CrossRef]
- Alifano, M.; Falcoz, P.E.; Seegers, V.; Roche, N.; Schussler, O.; Younes, M.; Antonacci, F.; Forgez, P.; Dechartres, A.; Massard, G.; et al. Preresection serum C-reactive protein measurement and survival among patients with resectable non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2011, 142, 1161–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alifano, M.; Mansuet-Lupo, A.; Lococo, F.; Roche, N.; Bobbio, A.; Canny, E.; Schussler, O.; Dermine, H.; Régnard, J.-F.; Burroni, B.; et al. Systemic inflammation, nutritional status and tumor immune microenvironment determine outcome of resected non-small cell lung cancer. PLoS ONE 2014, 9, e106914. [Google Scholar]
- Prado, C.M.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Icard, P.; Loi, M.; Wu, Z.; Ginguay, A.; Lincet, H.; Robin, E.; Coquerel, A.; Berzan, D.; Fournel, L.; Alifano, M. Metabolic Strategies for Inhibiting Cancer Development. Adv. Nutr. 2021, 12, 1461–1480. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | No. Missing (%) | Whole Sample n = 54,631 | Underweight n = 2468 | Normal Weight n = 25,482 | Overweight n = 18,765 | Obesity n = 7877 | p |
|---|---|---|---|---|---|---|---|
| Period, no. (%) | 0 (0) | <0.0001 | |||||
| 2003–2006 | 7815 (14.3) | 357 (14.5) | 3888 (15.3) | 2657 (14.2) | 907 (11.5) | ||
| 2007–2010 | 13,410 (24.5) | 581 (23.5) | 6342 (24.9) | 4632 (24.7) | 1844 (23.4) | ||
| 2011–2014 | 16,851 (30.8) | 756 (30.6) | 7791 (30.6) | 5793 (30.9) | 2491 (31.6) | ||
| 2015–2017 | 16,555 (30.3) | 774 (31.4) | 7461 (29.3) | 5683 (30.3) | 2635 (33.5) | ||
| Sex, no. (%) | 1 (<0.1) | <0.0001 | |||||
| Female | 16,448 (30.1) | 1298 (52.6) | 8787 (34.5) | 4162 (22.2) | 2187 (27.8) | ||
| Male | 38,182 (69.9) | 1170 (47.4) | 16,695 (65.5) | 14,602 (77.8) | 5690 (72.2) | ||
| Age, mean (SD) y | 51 (0.1) | 64.1 (10.1) | 60.1 (10.5) | 63.0 (10.5) | 65.6 (9.5) | 65.3 (9.1) | <0.0001 |
| Weight, mean (SD) kg | 39 (<0.1) | 72.9 (15.3) | 48.5 (5.7) | 64.0 (8.6) | 78.9 (8.5) | 95.3 (12.7) | <0.0001 |
| Height, mean (SD) cm | 39 (<0.1) | 169.5 (8.4) | 167.3 (8.5) | 169.2 (8.4) | 170.4 (8.1) | 169.2 (8.6) | <0.0001 |
| Body mass index, mean (SD) kg/m2 | 39 (<0.1) | 25.3 (4.6) | 17.3 (1.0) | 22.3 (1.8) | 27.1 (1.4) | 33.2 (3.3) | <0.0001 |
| Charlson comorbidity index, mean (SD) | 0 (0.0) | 4.4 (2.2) | 3.9 (2.0) | 4.2 (2.2) | 4.6 (2.2) | 4.6 (2.1) | <0.0001 |
| Performance status, no. (%) | 2953 (5.4) | <0.0001 | |||||
| 0 | 23,479 (45.4) | 845 (36.9) | 11,689 (48.4) | 8227 (46.4) | 2704 (36.3) | ||
| 1 | 23,318 (45.1) | 1099 (48.0) | 10,301 (42.6) | 8047 (45.4) | 3861 (51.8) | ||
| 2–4 | 4881 (9.4) | 346 (15.1) | 2183 (9.0) | 1453 (8.2) | 892 (12.0) | ||
| Histology, no. (%) | 3500 (6.4) | <0.0001 | |||||
| Adenocarcinoma | 30,187 (59.0) | 1426 (61.2) | 14,561 (61.0) | 10,181 (58.0) | 3998 (54.4) | ||
| Squamous-cell carcinoma | 14,176 (27.7) | 580 (24.9) | 6204 (26.0) | 5106 (29.1) | 2276 (31.0) | ||
| Carcinoid tumor, typical | 1744 (3.4) | 54 (2.3) | 683 (2.9) | 594 (3.4) | 412 (5.6) | ||
| Large-cell carcinoma, undifferentiated | 1598 (3.1) | 96 (4.1) | 836 (3.5) | 487 (2.8) | 178 (2.4) | ||
| Large-cell carcinoma, neuroendocrine | 961 (1.9) | 51 (2.2) | 455 (1.9) | 316 (1.8) | 139 (1.9) | ||
| Carcinoid tumor, atypical | 609 (1.2) | 23 (1.0) | 232 (1.0) | 236 (1.3) | 118 (1.6) | ||
| Small-cell lung carcinoma | 474 (0.9) | 18 (0.8) | 212 (0.9) | 175 (1.0) | 68 (0.9) | ||
| Sarcomatoid carcinoma | 385 (0.8) | 32 (1.4) | 210 (0.9) | 101 (0.6) | 41 (0.6) | ||
| Other | 997 (1.9) | 50 (2.1) | 474 (2.0) | 354 (2.0) | 116 (1.6) | ||
| Stage | 14,887 (27.3) | <0.0001 | |||||
| 0/occult | 186 (0.5) | 11 (0.6) | 96 (0.5) | 58 (0.4) | 19 (0.3) | ||
| I | 21,374 (53.8) | 952 (52.8) | 9776 (52.6) | 7413 (54.3) | 3222 (56.7) | ||
| II | 7391 (18.6) | 352 (19.5) | 3531 (19.0) | 2518 (18.4) | 985 (17.3) | ||
| III | 8454 (21.3) | 341 (18.9) | 3942 (21.2) | 2950 (21.6) | 1215 (21.4) | ||
| IV | 2339 (5.9) | 147 (8.2) | 1237 (6.7) | 709 (5.2) | 245 (4.3) | ||
| Surgical procedure, no. (%) | 0 (0) | <0.0001 | |||||
| Pneumonectomy | 5516 (10.1) | 236 (9.6) | 2738 (10.7) | 1878 (10.0) | 662 (8.4) | ||
| Other | 49,115 (89.9) | 2232 (90.4) | 22,744 (89.3) | 16,887 (90.0) | 7215 (91.6) | ||
| Side, no. (%) | 305 (0.6) | 0.071 | |||||
| Right | 31,412 (57.8) | 1460 (59.3) | 14,721 (58.1) | 10,760 (57.7) | 4447 (56.8) | ||
| Left | 22,914 (42.2) | 1000 (40.7) | 10,609 (41.9) | 7904 (42.3) | 3386 (43.2) |
| Features | Unadjusted | Model 1 | Model 2 | Model 3 * |
|---|---|---|---|---|
| n = 54,631 | n = 54,631 | n = 54,631 | n = 54,376 | |
| Deaths = 17,094 | Deaths = 17,094 | Deaths = 17,094 | Deaths = 17,043 | |
| BMI category | ||||
| Underweight | 1.24 (1.16–1.33) | 1.61 (1.50–1.72) | 1.50 (1.40–1.61) | 1.51 (1.41–1.63) |
| Normal weight | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Overweight | 0.95 (0.92–0.98) | 0.81 (0.79–0.84) | 0.83 (0.80–0.86) | 0.84 (0.81–0.87) |
| Obesity | 0.88 (0.84–0.92) | 0.79 (0.76–0.83) | 0.79 (0.75–0.83) | 0.80 (0.76–0.84) |
| Period | ||||
| 2003–2006 | — | 1 (reference) | 1 (reference) | 1 (reference) |
| 2007–2010 | — | 0.92 (0.88–0.97) | 0.93 (0.89–0.98) | 0.94 (0.90–0.99) |
| 2011–2014 | — | 0.93 (0.89–0.97) | 0.96 (0.92–1.01) | 0.98 (0.94–1.03) |
| 2015–2017 | — | 1.00 (0.95–1.04) | 1.05 (1.00–1.10) | 1.08 (1.03–1.14) |
| Sex, no. (%) | ||||
| Female | — | 1 (reference) | 1 (reference) | 1 (reference) |
| Male | — | 3.07 (2.93–3.22) | 2.90 (2.77–3.04) | 2.90 (2.77–3.04) |
| Age (per decade) | — | 1.08 (1.05–1.10) | 1.06 (1.04–1.09) | 1.09 (1.07–1.11) |
| Charlson comorbidity index (per point until a score of 6 **) | — | 1.11 (1.10–1.13) | 1.09 (1.07–1.10) | 1.09 (1.07–1.10) |
| Performance status | ||||
| 0 | — | — | 1 (reference) | 1 (reference) |
| 1 | — | — | 1.22 (1.18–1.27) | 1.20 (1.16–1.25) |
| 2–4 | — | — | 1.67 (1.59–1.76) | 1.61 (1.53–1.70) |
| Surgical procedure | ||||
| Pneumonectomy | — | 1.75 (1.67–1.83) | 1.69 (1.61–1.77) | 1.24 (1.18–1.30) |
| Other | — | 1 (reference) | 1 (reference) | 1 (reference) |
| Side | ||||
| Right | — | 1 (reference) | 1 (reference) | 1 (reference) |
| Left | — | 0.98 (0.95–1.01) | 0.98 (0.95–1.01) | 0.98 (0.95–1.01) |
| Histology | ||||
| Adenocarcinoma | — | — | 1 (reference) | 1 (reference) |
| Squamous-cell carcinoma | — | — | 1.04 (1.00–1.08) | 1.06 (1.02–1.10) |
| Carcinoid tumor, typical | — | — | 0.29 (0.23–0.37) | 0.34 (0.27–0.43) |
| Large-cell carcinoma, undifferentiated | — | — | 1.32 (1.22–1.43) | 1.27 (1.18–1.38) |
| Large-cell carcinoma, neuroendocrine | — | — | 1.32 (1.19–1.47) | 1.32 (1.19–1.47) |
| Carcinoid tumor, atypical | — | — | 0.54 (0.43–0.67) | 0.56 (0.45–0.70) |
| Small-cell lung carcinoma | — | — | 1.66 (1.45–1.90) | 1.65 (1.44–1.89) |
| Sarcomatoid carcinoma | — | — | 1.62 (1.38–1.89) | 1.57 (1.34–1.83) |
| Other | — | — | 1.18 (1.05–1.32) | 1.18 (1.05–1.33) |
| Stage | ||||
| I | — | — | — | 1 (reference) |
| II | — | — | — | 1.62 (1.54–1.71) |
| III | — | — | — | 2.33 (2.22–2.44) |
| IV | — | — | — | 2.93 (2.73–3.14) |
| BMI Category | Females n = 16,448 Deaths = 2109 | Males n = 38,183 Deaths = 14,985 | p |
|---|---|---|---|
| Unadjusted | |||
| Underweight | 1.49 (1.29–1.71) | 1.51 (1.40–1.64) | 0.83 |
| Normal weight | 1 (reference) | 1 (reference) | — |
| Overweight | 0.81 (0.72–0.90) | 0.85 (0.82–0.88) | 0.37 |
| Obesity | 0.72 (0.63–0.84) | 0.83 (0.79–0.88) | 0.069 |
| Model 1 * | |||
| Underweight | 1.41 (1.23–1.62) | 1.55 (1.43–1.68) | 0.25 |
| Normal weight | 1 (reference) | 1 (reference) | — |
| Overweight | 0.78 (0.70–0.87) | 0.83 (0.80–0.86) | 0.35 |
| Obesity | 0.68 (0.58–0.78) | 0.79 (0.75–0.83) | 0.049 |
| Model 2 † | |||
| Underweight | 1.38 (1.20–1.58) | 1.53 (1.42–1.66) | 0.19 |
| Normal weight | 1 (reference) | 1 (reference) | |
| Overweight | 0.81 (0.73–0.91) | 0.83 (0.80–0.86) | 0.69 |
| Obesity | 0.73 (0.63–0.84) | 0.80 (0.76–0.84) | 0.22 |
| Model 3 ‡ | |||
| Underweight | 1.38 (1.20–1.59) | 1.55 (1.42–1.68) | 0.18 |
| Normal weight | 1 (reference) | 1 (reference) | |
| Overweight | 0.82 (0.73–0.91) | 0.84 (0.81–0.87) | 0.65 |
| Obesity | 0.73 (0.63–0.84) | 0.81 (0.77–0.86) | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alifano, M.; Daffré, E.; Iannelli, A.; Brouchet, L.; Falcoz, P.E.; Le Pimpec Barthes, F.; Bernard, A.; Pages, P.B.; Thomas, P.A.; Dahan, M.; et al. The Reality of Lung Cancer Paradox: The Impact of Body Mass Index on Long-Term Survival of Resected Lung Cancer. A French Nationwide Analysis from the Epithor Database. Cancers 2021, 13, 4574. https://doi.org/10.3390/cancers13184574
Alifano M, Daffré E, Iannelli A, Brouchet L, Falcoz PE, Le Pimpec Barthes F, Bernard A, Pages PB, Thomas PA, Dahan M, et al. The Reality of Lung Cancer Paradox: The Impact of Body Mass Index on Long-Term Survival of Resected Lung Cancer. A French Nationwide Analysis from the Epithor Database. Cancers. 2021; 13(18):4574. https://doi.org/10.3390/cancers13184574
Chicago/Turabian StyleAlifano, Marco, Elisa Daffré, Antonio Iannelli, Laurent Brouchet, Pierre Emmanuel Falcoz, Françoise Le Pimpec Barthes, Alain Bernard, Pierre Benoit Pages, Pascal Alexandre Thomas, Marcel Dahan, and et al. 2021. "The Reality of Lung Cancer Paradox: The Impact of Body Mass Index on Long-Term Survival of Resected Lung Cancer. A French Nationwide Analysis from the Epithor Database" Cancers 13, no. 18: 4574. https://doi.org/10.3390/cancers13184574