
Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Pancreatic Cancer: Systematic Review and Still-Open Questions

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Search Results
2.2. Clinico-Pathologic Characteristics
2.3. Molecular Data of High-TMB PDAC
2.4. Response to Immunotherapy of High-TMB PDAC
3. Discussion
4. Materials and Methods
4.1. Inclusion and Exclusion Criteria
4.2. Data Sources and Literature Search Strategy
4.3. Study Selection
4.4. Data Extraction, Synthesis, and Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic Cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Smithy, J.W.; O’Reilly, E.M. Pancreas Cancer: Therapeutic Trials in Metastatic Disease. J. Surg. Oncol. 2021, 123, 1475–1488. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 Human Cancer Genomes Reveals the Landscape of Tumor Mutational Burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef]
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.-Y.; Andre, F.; et al. ESMO Recommendations on Microsatellite Instability Testing for Immunotherapy in Cancer, and Its Relationship with PD-1/PD-L1 Expression and Tumour Mutational Burden: A Systematic Review-Based Approach. Ann. Oncol. 2019, 30, 1232–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of Tumour Mutational Burden with Outcomes in Patients with Advanced Solid Tumours Treated with Pembrolizumab: Prospective Biomarker Analysis of the Multicohort, Open-Label, Phase 2 KEYNOTE-158 Study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Schrock, A.B.; Ouyang, C.; Sandhu, J.; Sokol, E.; Jin, D.; Ross, J.S.; Miller, V.A.; Lim, D.; Amanam, I.; Chao, J.; et al. Tumor Mutational Burden Is Predictive of Response to Immune Checkpoint Inhibitors in MSI-High Metastatic Colorectal Cancer. Ann. Oncol. 2019, 30, 1096–1103. [Google Scholar] [CrossRef]
- Samstein, R.M.; Lee, C.-H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor Mutational Load Predicts Survival after Immunotherapy across Multiple Cancer Types. Nat. Genetics 2019, 51, 202–206. [Google Scholar] [CrossRef]
- Strickler, J.H.; Hanks, B.A.; Khasraw, M. Tumor Mutational Burden as a Predictor of Immunotherapy Response: Is More Always Better? Clin. Cancer Res. 2021, 27, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Gubin, M.M.; Artyomov, M.N.; Mardis, E.R.; Schreiber, R.D. Tumor Neoantigens: Building a Framework for Personalized Cancer Immunotherapy. J. Clin. Investig. 2015, 125, 3413–3421. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, J.; Du, C.; Wu, Y.; Xia, D.; Lv, W.; Hu, J. The Predictive Value of Tumor Mutation Burden on Efficacy of Immune Checkpoint Inhibitors in Cancers: A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Sholl, L.M.; Hirsch, F.R.; Hwang, D.; Botling, J.; Lopez-Rios, F.; Bubendorf, L.; Mino-Kenudson, M.; Roden, A.C.; Beasley, M.B.; Borczuk, A.; et al. The Promises and Challenges of Tumor Mutation Burden as an Immunotherapy Biomarker: A Perspective from the International Association for the Study of Lung Cancer Pathology Committee. J. Thorac. Oncol. 2020, 15, 1409–1424. [Google Scholar] [CrossRef]
- Büttner, R.; Gosney, J.R.; Skov, B.G.; Adam, J.; Motoi, N.; Bloom, K.J.; Dietel, M.; Longshore, J.W.; López-Ríos, F.; Penault-Llorca, F.; et al. Programmed Death-Ligand 1 Immunohistochemistry Testing: A Review of Analytical Assays and Clinical Implementation in Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2017, 35, 3867–3876. [Google Scholar] [CrossRef]
- Rizvi, H.; Sanchez-Vega, F.; La, K.; Chatila, W.; Jonsson, P.; Halpenny, D.; Plodkowski, A.; Long, N.; Sauter, J.L.; Rekhtman, N.; et al. Molecular Determinants of Response to Anti-Programmed Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1) Blockade in Patients with Non-Small-Cell Lung Cancer Profiled with Targeted Next-Generation Sequencing. J. Clin. Oncol. 2018, 36, 633–641. [Google Scholar] [CrossRef]
- Budczies, J.; Allgäuer, M.; Litchfield, K.; Rempel, E.; Christopoulos, P.; Kazdal, D.; Endris, V.; Thomas, M.; Fröhling, S.; Peters, S.; et al. Optimizing Panel-Based Tumor Mutational Burden (TMB) Measurement. Ann. Oncol. 2019, 30, 1496–1506. [Google Scholar] [CrossRef] [Green Version]
- Wiesweg, M.; Mairinger, F.; Reis, H.; Goetz, M.; Walter, R.F.H.; Hager, T.; Metzenmacher, M.; Eberhardt, W.E.E.; McCutcheon, A.; Köster, J.; et al. Machine Learning-Based Predictors for Immune Checkpoint Inhibitor Therapy of Non-Small-Cell Lung Cancer. Ann. Oncol. 2019, 30, 655–657. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and Activity of Anti-PD-L1 Antibody in Patients with Advanced Cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Chen, Z.; Wu, L.; Tao, W. Novel Tumor Mutation Score versus Tumor Mutation Burden in Predicting Survival after Immunotherapy in Pan-Cancer Patients from the MSK-IMPACT Cohort. Ann. Transl. Med. 2020, 8, 446. [Google Scholar] [CrossRef] [PubMed]
- Quy, P.N.; Kanai, M.; Fukuyama, K.; Kou, T.; Kondo, T.; Yamamoto, Y.; Matsubara, J.; Hiroshima, A.; Mochizuki, H.; Sakuma, T.; et al. Association Between Preanalytical Factors and Tumor Mutational Burden Estimated by Next-Generation Sequencing-Based Multiplex Gene Panel Assay. Oncologist 2019, 24, e1401–e1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roszik, J.; Haydu, L.E.; Hess, K.R.; Oba, J.; Joon, A.Y.; Siroy, A.E.; Karpinets, T.V.; Stingo, F.C.; Baladandayuthapani, V.; Tetzlaff, M.T.; et al. Novel Algorithmic Approach Predicts Tumor Mutation Load and Correlates with Immunotherapy Clinical Outcomes Using a Defined Gene Mutation Set. BMC Med. 2016, 14, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garofalo, A.; Sholl, L.; Reardon, B.; Taylor-Weiner, A.; Amin-Mansour, A.; Miao, D.; Liu, D.; Oliver, N.; MacConaill, L.; Ducar, M.; et al. The Impact of Tumor Profiling Approaches and Genomic Data Strategies for Cancer Precision Medicine. Genome Med. 2016, 8, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budczies, J.; Kazdal, D.; Allgäuer, M.; Christopoulos, P.; Rempel, E.; Pfarr, N.; Weichert, W.; Fröhling, S.; Thomas, M.; Peters, S.; et al. Quantifying Potential Confounders of Panel-Based Tumor Mutational Burden (TMB) Measurement. Lung Cancer 2020, 142, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Shiraishi, Y.; Takeda, Y.; Sakata, S.; Matsumoto, M.; Nagano, S.; Maeda, T.; Nagata, Y.; Kitanaka, A.; Mizuno, S.; et al. Aberrant PD-L1 Expression through 3’-UTR Disruption in Multiple Cancers. Nature 2016, 534, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Melton, C.; Reuter, J.A.; Spacek, D.V.; Snyder, M. Recurrent Somatic Mutations in Regulatory Regions of Human Cancer Genomes. Nat. Genet. 2015, 47, 710–716. [Google Scholar] [CrossRef]
- Wood, M.A.; Nellore, A.; Thompson, R.F. Tumor Mutation Burden—From Doubts to Concerns. JAMA Oncol. 2019, 5, 1808. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Morris, L.G.T.; Chan, T.A. Panel-Based Estimates of Tumor Mutational Burden: Characterizing Unknown Unknowns. Ann. Oncol. 2019, 30, 1413–1415. [Google Scholar] [CrossRef]
- Addeo, A.; Banna, G.L.; Weiss, G.J. Tumor Mutation Burden—From Hopes to Doubts. JAMA Oncol. 2019, 5, 934. [Google Scholar] [CrossRef]
- Eggink, F.A.; Gool, I.C.V.; Leary, A.; Pollock, P.M.; Crosbie, E.J.; Mileshkin, L.; Jordanova, E.S.; Adam, J.; Freeman-Mills, L.; Church, D.N.; et al. Immunological Profiling of Molecularly Classified High-Risk Endometrial Cancers Identifies POLE-Mutant and Microsatellite Unstable Carcinomas as Candidates for Checkpoint Inhibition. OncoImmunology 2017, 6, e1264565. [Google Scholar] [CrossRef] [Green Version]
- Galuppini, F.; Pennelli, G.; Loupakis, F.; Lanza, C.; Vianello, L.; Sacchi, D.; Mescoli, C.; Salmaso, R.; Agostini, M.; Lonardi, S.; et al. BRAF p.V600E-Specific Immunohistochemical Assessment in Colorectal Cancer Endoscopy Biopsies Is Consistent with the Mutational Profiling. Histopathology 2017, 71, 1008–1011. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.J.R.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.-L.; et al. Signatures of Mutational Processes in Human Cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer Immunology. Mutational Landscape Determines Sensitivity to PD-1 Blockade in Non-Small Cell Lung Cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in Patients with Locally Advanced and Metastatic Urothelial Carcinoma Who Have Progressed Following Treatment with Platinum-Based Chemotherapy: A Single-Arm, Multicentre, Phase 2 Trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef] [Green Version]
- Snyder, A.; Makarov, V.; Merghoub, T.; Yuan, J.; Zaretsky, J.M.; Desrichard, A.; Walsh, L.A.; Postow, M.A.; Wong, P.; Ho, T.S.; et al. Genetic Basis for Clinical Response to CTLA-4 Blockade in Melanoma. N. Engl. J. Med. 2014, 371, 2189–2199. [Google Scholar] [CrossRef]
- Chen, M.; Yang, S.; Fan, L.; Wu, L.; Chen, R.; Chang, J.; Hu, J. Combined Antiangiogenic Therapy and Immunotherapy Is Effective for Pancreatic Cancer with Mismatch Repair Proficiency but High Tumor Mutation Burden: A Case Report. Pancreas 2019, 48, 1232–1236. [Google Scholar] [CrossRef]
- Grant, R.C.; Denroche, R.; Jang, G.H.; Nowak, K.M.; Zhang, A.; Borgida, A.; Holter, S.; Topham, J.T.; Wilson, J.; Dodd, A.; et al. Clinical and Genomic Characterisation of Mismatch Repair Deficient Pancreatic Adenocarcinoma. Gut 2020. [Google Scholar] [CrossRef] [PubMed]
- Humphris, J.L.; Patch, A.-M.; Nones, K.; Bailey, P.J.; Johns, A.L.; McKay, S.; Chang, D.K.; Miller, D.K.; Pajic, M.; Kassahn, K.S.; et al. Hypermutation In Pancreatic Cancer. Gastroenterology 2017, 152, 68–74.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Z.I.; Shia, J.; Stadler, Z.K.; Varghese, A.M.; Capanu, M.; Salo-Mullen, E.; Lowery, M.A.; Diaz, L.A.; Mandelker, D.; Yu, K.H.; et al. Evaluating Mismatch Repair Deficiency in Pancreatic Adenocarcinoma: Challenges and Recommendations. Clin. Cancer Res. 2018, 24, 1326–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagashima, T.; Yamaguchi, K.; Urakami, K.; Shimoda, Y.; Ohnami, S.; Ohshima, K.; Tanabe, T.; Naruoka, A.; Kamada, F.; Serizawa, M.; et al. Japanese Version of The Cancer Genome Atlas, JCGA, Established Using Fresh Frozen Tumors Obtained from 5143 Cancer Patients. Cancer Sci. 2020, 111, 687–699. [Google Scholar] [CrossRef]
- Kryklyva, V.; Linden, E.T.; Kroeze, L.I.; Voer, R.M.D.; Kolk, B.M.V.D.; Stommel, M.W.J.; Hermans, J.J.; Luchini, C.; Wood, L.D.; Hruban, R.H.; et al. Medullary Pancreatic Carcinoma Due to Somatic POLE Mutation: A Distinctive Pancreatic Carcinoma with Marked Long-Term Survival. Pancreas 2020, 49, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Kimura, R.; Ohtsuka, T.; Kubo, M.; Kajihara, A.; Fujii, A.; Watanabe, Y.; Mori, Y.; Ikenaga, N.; Nakata, K.; Shindo, K.; et al. FoundationOne® CDx Gene Profiling in Japanese Pancreatic Ductal Adenocarcinoma Patients: A Single-Institution Experience. Surgery Today 2021, 51, 619–626. [Google Scholar] [CrossRef]
- Ngo, P.; Shanshal, M.; Rojan, A. Immunotherapy in Pancreatic Cancer and the Importance of Tumour Testing. BMJ Case Rep. 2020, 13. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.; Javle, M.; Davis, R.E.; Vats, P.; Kumar-Sinha, C.; Xiao, L.; Mettu, N.B.; Parra, E.R.; Benson, A.B.; Lopez, C.D.; et al. Randomized Phase II Study of the Bruton Tyrosine Kinase Inhibitor Acalabrutinib, Alone or with Pembrolizumab in Patients with Advanced Pancreatic Cancer. J. Immunother. Cancer 2020, 8, e000587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, W.; Chen, J.; Chou, J.F.; Varghese, A.M.; Yu, K.H.; Wong, W.; Capanu, M.; Balachandran, V.; McIntyre, C.A.; Dika, I.E.; et al. Genomic Methods Identify Homologous Recombination Deficiency in Pancreas Adenocarcinoma and Optimize Treatment Selection. Clin. Cancer Res. 2020, 26, 3239–3247. [Google Scholar] [CrossRef] [PubMed]
- Salem, M.E.; Puccini, A.; Grothey, A.; Raghavan, D.; Goldberg, R.M.; Xiu, J.; Korn, W.M.; Weinberg, B.A.; Hwang, J.J.; Shields, A.F.; et al. Landscape of Tumor Mutation Load, Mismatch Repair Deficiency, and PD-L1 Expression in a Large Patient Cohort of Gastrointestinal Cancers. Mol. Cancer Res. 2018, 16, 805–812. [Google Scholar] [CrossRef] [Green Version]
- Singhi, A.D.; George, B.; Greenbowe, J.R.; Chung, J.; Suh, J.; Maitra, A.; Klempner, S.J.; Hendifar, A.; Milind, J.M.; Golan, T.; et al. Real-Time Targeted Genome Profile Analysis of Pancreatic Ductal Adenocarcinomas Identifies Genetic Alterations That Might Be Targeted with Existing Drugs or Used as Biomarkers. Gastroenterology 2019, 156, 2242–2253.e4. [Google Scholar] [CrossRef] [Green Version]
- Tuli, R.; Shiao, S.L.; Nissen, N.; Tighiouart, M.; Kim, S.; Osipov, A.; Bryant, M.; Ristow, L.; Placencio-Hickok, V.R.; Hoffman, D.; et al. A Phase 1 Study of Veliparib, a PARP-1/2 Inhibitor, with Gemcitabine and Radiotherapy in Locally Advanced Pancreatic Cancer. EBioMedicine 2019, 40, 375–381. [Google Scholar] [CrossRef] [Green Version]
- Singhi, A.D.; Ishida, H.; Ali, S.Z.; Goggins, M.; Canto, M.; Wolfgang, C.; Meriden, Z.; Roberts, N.; Klein, A.P.; Hruban, R.H. A Histomorphologic Comparison of Familial and Sporadic Pancreatic Cancers. Pancreatology 2015, 15, 387–391. [Google Scholar] [CrossRef] [Green Version]
- Gordon-Dseagu, V.L.; Devesa, S.S.; Goggins, M.; Stolzenberg-Solomon, R. Pancreatic Cancer Incidence Trends: Evidence from the Surveillance, Epidemiology and End Results (SEER) Population-Based Data. Int. J. Epidemiol. 2018, 47, 427–439. [Google Scholar] [CrossRef] [PubMed]
- Bazzichetto, C.; Luchini, C.; Conciatori, F.; Vaccaro, V.; Di Cello, I.; Mattiolo, P.; Falcone, I.; Ferretti, G.; Scarpa, A.; Cognetti, F.; et al. Morphologic and Molecular Landscape of Pancreatic Cancer Variants as the Basis of New Therapeutic Strategies for Precision Oncology. Int. J. Mol. Sci. 2020, 21, 8841. [Google Scholar] [CrossRef]
- Luchini, C.; Capelli, P.; Scarpa, A. Pancreatic Ductal Adenocarcinoma and Its Variants. Surg. Pathol. Clin. 2016, 9, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Brosens, L.A.A.; Wood, L.D.; Chatterjee, D.; Shin, J.I.; Sciammarella, C.; Fiadone, G.; Malleo, G.; Salvia, R.; Kryklyva, V.; et al. Comprehensive Characterisation of Pancreatic Ductal Adenocarcinoma with Microsatellite Instability: Histology, Molecular Pathology and Clinical Implications. Gut 2021, 70, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Grant, R.C.; Scarpa, A.; Gallinger, S. Microsatellite Instability/Mismatch Repair Deficiency in Pancreatic Cancers: The Same or Different? Gut 2021. [Google Scholar] [CrossRef]
- Luchini, C.; Grillo, F.; Fassan, M.; Vanoli, A.; Capelli, P.; Paolino, G.; Ingravallo, G.; Renzulli, G.; Doglioni, C.; D’Amuri, A.; et al. Malignant Epithelial/Exocrine Tumors of the Pancreas. Pathologica 2020, 112, 210–226. [Google Scholar] [CrossRef]
- Cohen, R.; Heran, M.; Pudlarz, T.; Hilmi, M.; Tournigand, C.; André, T.; Rousseau, B. Traitement des cancers colorectaux par immunothérapie: Aller au-delà de MSI avec la classification moléculaire (CMS) et la charge mutationnelle. Bull. Cancer 2019, 106, 151–161. [Google Scholar] [CrossRef]
- Picard, E.; Verschoor, C.P.; Ma, G.W.; Pawelec, G. Relationships Between Immune Landscapes, Genetic Subtypes and Responses to Immunotherapy in Colorectal Cancer. Front. Immunol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Church, D.N.; Stelloo, E.; Nout, R.A.; Valtcheva, N.; Depreeuw, J.; ter Haar, N.; Noske, A.; Amant, F.; Tomlinson, I.P.M.; Wild, P.J.; et al. Prognostic Significance of POLE Proofreading Mutations in Endometrial Cancer. JNCI J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef]
- León-Castillo, A.; Britton, H.; McConechy, M.K.; McAlpine, J.N.; Nout, R.; Kommoss, S.; Brucker, S.Y.; Carlson, J.W.; Epstein, E.; Rau, T.T.; et al. Interpretation of Somatic POLE Mutations in Endometrial Carcinoma. J. Pathol. 2020, 250, 323–335. [Google Scholar] [CrossRef]
- Birkbak, N.J.; Kochupurakkal, B.; Izarzugaza, J.M.G.; Eklund, A.C.; Li, Y.; Liu, J.; Szallasi, Z.; Matulonis, U.A.; Richardson, A.L.; Iglehart, J.D.; et al. Tumor Mutation Burden Forecasts Outcome in Ovarian Cancer with BRCA1 or BRCA2 Mutations. PLoS ONE 2013, 8, e80023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Shi, J.; Guo, H.; Yang, X.; Jiang, Y.; Long, J.; Bai, Y.; Wang, D.; Yang, X.; Wan, X.; et al. Alterations in DNA Damage Repair Genes in Primary Liver Cancer. Clin. Cancer Res. 2019, 25, 4701–4711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waddell, N.; Pajic, M.; Patch, A.-M.; Chang, D.K.; Kassahn, K.S.; Bailey, P.; Johns, A.L.; Miller, D.; Nones, K.; Quek, K.; et al. Whole Genomes Redefine the Mutational Landscape of Pancreatic Cancer. Nature 2015, 518, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Golan, T.; Hammel, P.; Reni, M.; Cutsem, E.V.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Golan, T.; O’Kane, G.M.; Denroche, R.E.; Raitses-Gurevich, M.; Grant, R.C.; Holter, S.; Wang, Y.; Zhang, A.; Jang, G.H.; Stossel, C.; et al. Genomic Features and Classification of Homologous Recombination Deficient Pancreatic Ductal Adenocarcinoma. Gastroenterology 2021. [Google Scholar] [CrossRef] [PubMed]
- Renouf, D.J.; Kavan, P.; Dhani, N.C.; Jonker, D.J.; Chia-chi Wei, A.; Hsu, T.; Tang, P.A.; Graham, B.; Tu, D.; O’Callaghan, J.C. The CCTG PA.7 trial: A randomized phase II study of gemcitabine and nab-paclitaxel vs. gemcitabine, nab-paclitaxel, durvalumab, and tremelimumab as 1st line therapy in metastatic pancreatic ductal adenocarcinoma (PDAC). J. Clin. Oncol. 2017, 35 (Suppl. S15), TPS4149. [Google Scholar] [CrossRef]
- Sodergren, M.H.; Mangal, N.; Wasan, H.; Sadanandam, A.; Balachandran, V.P.; Jiao, L.R.; Habib, N. Immunological combination treatment holds the key to improving survival in pancreatic cancer. J. Cancer Res. Clin. Oncol. 2020, 146, 2897–2911. [Google Scholar] [CrossRef]
- Royal, R.E.; Levy, C.; Turner, K.; Mathur, A.; Hughes, M.; Kammula, U.S.; Sherry, R.M.; Topalian, S.L.; Yang, J.C.; Lowy, I.; et al. Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for locally advanced or metastatic pancreatic adenocarcinoma. J. Immunother. 2010, 33, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology: A Proposal for Reporting. Meta-Analysis of Observational Studies in Epidemiology (MOOSE) Group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author, Year | Country | N of Cases with High TMB | Tumor Site in the Pancreas | Tumor Histology | TNM |
|---|---|---|---|---|---|
| Chen, 2019 [34] | China | 1 | Head | Moderately differentiated PDAC | IV |
| Grant, 2020 [35] | Canada | 9 | 6 Head, 1 Body-Tail, 2 NA | 2 cases: IPMN-associated PDAC, 3 PDAC NOS (2 with medullary areas), 1 anaplastic PDAC, 3 histology NA | 1 case IIA, 5 cases IIB, 1 case III, 2 cases IV |
| Humphris, 2017 [36] | Australia | 5 | NA | 1 case G4, 3 G2, 1 signet-ring | NA |
| Hu, 2018 [37] | USA | 7 | 1 head/body, 2 body-tail, 1 head, 3 NA | 2 conventional, 4 mucinous/colloid IPMN-associated, 1 medullary | 1 case pT4, 1 case stage IIB, 2 cases stage IV, remaining cases NA |
| Nagashima, 2019 [38] | Japan | 0/131 | NA | NA | NA |
| Kryklyva, 2020 [39] | The Netherlands | 1 | Head | Medullary PDAC | IIA |
| Kimura, 2020 [40] | Japan | 0/17 | NA | NA | NA |
| Ngo, 2020 [41] | USA | 1 | Tail | PDAC | IIB |
| Overman, 2020 [42] | USA | 0/2 | NA | Only 2 long survivor PDAC have been tested for TMB: they were TMB-low and MSS | NA |
| Park, 2020 [43] | USA | 5/50 HRD PDAC | NA | PDAC | |
| Salem, 2018 [44] | USA | 12/870 | NA | PDAC | NA |
| Singhi, 2019 [45] | USA | 5/1021 | NA | PDAC | NA |
| Tuli, 2019 [46] | USA | 1 | NS | PDAC | NS |
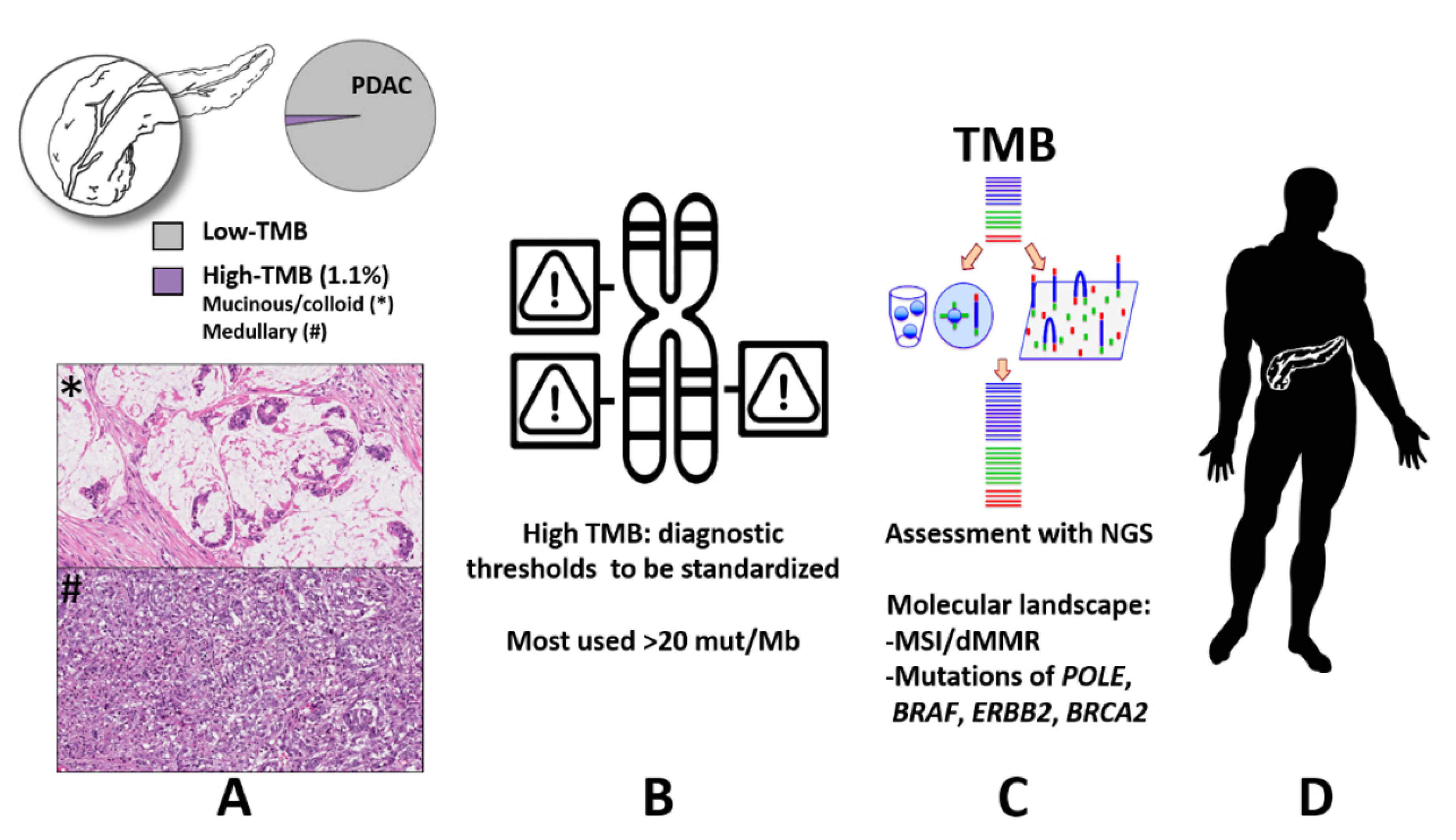
| TOTAL | - | 22/2091 (1.1%) | H: 64%, BT: 36% | 80% PDAC, 14% IPMN-associated mucinous/colloid; 4% medullary; 2% signet ring | I: 0%; II: 60%; III: 7%; IV: 33% |
| Author, Year | N of Cases with High TMB # | TMB Value (mut per Mb) | Method of NGS/TMB Measurement | MMR/MSI Status * | Data on Molecular Profile | Summary of Therapeutic Strategies | Data on Survival |
|---|---|---|---|---|---|---|---|
| Chen, 2019 [34] | 1 | 14.9 | NGS on cell-free DNA from blood; 156 genes-panel, Illumina platform | Stable (IHC) | ERBB2 amplification and mutation. Other mutations in UGTIA1, GSTPI and MTHFR | RCT (gemcitabine); trastuzumab; erlotinib; antiangiogenic therapy; immunotherapy (pembrolizumab) | Dead 20 months after diagnosis |
| Grant, 2020 [35] | 9 | Median: 25.93 | WGS, Illumina platform | All MSI (paper on MSI PDAC) | More JAK1 and ACV2RA, Less KRAS and SMAD4 mutations | Surgical resection except of IV stage patients. Two patients had adjuvant IT (1 partial response, 1 disease free), 2 no AT (1 alive with disease, recurrence in mesentery, at 33.1 months, 1 alive without disease at 104 months); 3 NAT (2 dead, 1 alive, received adjuvant IT), 3 AT (gemcitabine, alive and disease- free after 42, 44, and 107 months, respectively) | |
| Humphris, 2017 [36] | 5 | Threshold 12 mut/Mb, Mean value: 31.8 | WGS | 4 MSI, 1 microsatellite stable | 1 case with somatic homozygous deletion of MSH2, 1 case MHL1 hypermethylation, 1 case MSH2 desrupting rearrangement, 1 case MSH2 somatic splice site, 1 case unknown | NA | NA |
| Hu, 2018 [37] | 7 | Threshold 12 mut/Mb, Mean value: 51,3 for cases with MSI/dMMR, 54 for a pathogenic BRCA2 mutated PDAC | MSK-IMPACT (341 cancer-associated gene panel) | 6 MSI/dMMR PDAC | 2 cases with germline MSH2 mutations, 2 with germline PMS2 mutation, 1 germline MLH1, 1 germline MSH6, 1 unspecified pathogenic BRCA2 mutation | MSI/dMMR cases: 1 case FOLFIRINOX and FOLFIRI in a neoadjuvant context, followed IT with anti-PD-1: partial response for over 22 months; 1 case: distal pancreatectomy, adjuvant gemcitabine, GVAX, progression and new diagnoses of bladder and gastric cancer, complete response with IT with anti–PD-1 therapy after 2 years; distal pancreatectomy and hemicolectomy (concomitant colorectal cancer); adjuvant 5-fluorouracil and RT: no recurrence in 26 years after surgery; 1 patient pancreaticoduodenectomy, adjuvant gemcitabine, capecitabine, RT, then progression, FOLFOX: no recurrence after 36 months; 1 patient: IT with anti-PD-1 therapy: significant but unspecified regression; 1 case: metastatic PDAC, FOLFIRINOX, gemcitabine, and nab-paclitaxel, then IT with anti-PD-L1; then progression to death 30 months after the diagnosis. | |
| Nagashima, 2019 [38] | 0/131 | NA | WES | NA | NA | NA | NA |
| Kryklyva, 2020 [39] | 1 | 111 | NGS with 30 genes-panel, Illumina platform | Stable (IHC and NGS) | POLE, ERBB2, GNAS, KRAS, MAP2K1, TP53 | Surgical resection, no AT | Alive free of disease 5 years after surgery |
| Kimura, 2020 [40] | 0/17 | NA | WES | NA | NA | NA | NA |
| Ngo, 2020 [41] | 1 | High (NS) | Not specified | MSI (Lynch syndrome) | MSH2 germline mutation | Lynch syndrome; NAT with gemcitabine and nab- paclitaxel, surgical resection, AT with FOLFIRINOX, liver metastasis, IT with pembrolizumab (stable disease after 30 months) | |
| Overman, 2020 [42] | 0/2 | NS | NA | NA | NA | NA | NA |
| Park, 2020 [43] | 5/50 # HRD PDAC | 8 as threshold, which can be considered low but was used for correlations with HRD/BRCA genes mutations, NS the exact value for each case | NGS with OncoKB / MSK-IMPACT | NA | 1 case KRAS, TP53, SMAD4, BRCA2 biallelic inactivation; 1 case KRAS, TP53, CDKN2A, BRCA2 biallelic inactivation; 1 case KRAS, SMAD4, ARID1A, BRCA2 biallelic inactivation: 1 case KRAS, SMAD4, BRCA2 biallelic inactivation; 1 case KRAS, TP53, CDKN2A, SMAD4. | NA | NA |
| Salem, 2018 [44] | 12/870 | 17 as threshold, NS the exact value for each case | NGS SureSelect XT assay | 5/12 hTMB and MSS, 7/12 MSI | NA | NA | NA |
| Singhi, 2019 [45] | 5/1021 | 20 as threshold, NS the exact value for each case | Illumina HiSeq technology, | 1/5 MSI | One case had both MSI and high-TMB (MLH1 promoter hypermethylation), with BRAF p.V600E, other: NS | NA | NA |
| Tuli, 2019 [46] | 1 | 23.4 | NGS (targeted, Foundation Medicine) | MSI | CHEK2, MLH1 mutations | NS | 22 months OS |
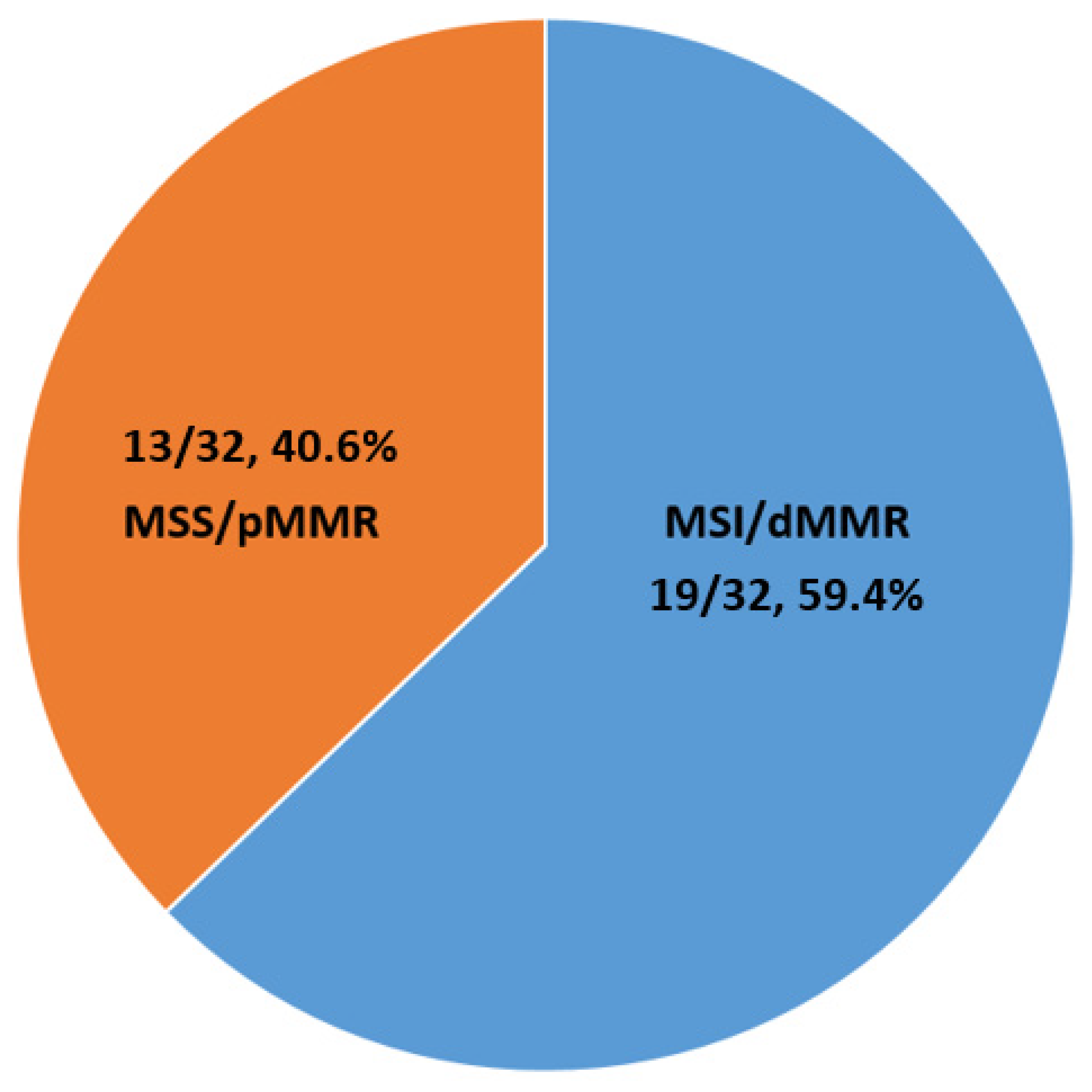
| TOTAL | Total of 47; 22/2091 # (1.1%) | Mean value: 37.6 | NGS | 19/32 MSI * | Of note: MMR genes, POLE, HRD | 8 cases received IT, with different responses (6 partial, 2 complete). | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lawlor, R.T.; Mattiolo, P.; Mafficini, A.; Hong, S.-M.; Piredda, M.L.; Taormina, S.V.; Malleo, G.; Marchegiani, G.; Pea, A.; Salvia, R.; et al. Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Pancreatic Cancer: Systematic Review and Still-Open Questions. Cancers 2021, 13, 3119. https://doi.org/10.3390/cancers13133119
Lawlor RT, Mattiolo P, Mafficini A, Hong S-M, Piredda ML, Taormina SV, Malleo G, Marchegiani G, Pea A, Salvia R, et al. Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Pancreatic Cancer: Systematic Review and Still-Open Questions. Cancers. 2021; 13(13):3119. https://doi.org/10.3390/cancers13133119
Chicago/Turabian StyleLawlor, Rita T., Paola Mattiolo, Andrea Mafficini, Seung-Mo Hong, Maria L. Piredda, Sergio V. Taormina, Giuseppe Malleo, Giovanni Marchegiani, Antonio Pea, Roberto Salvia, and et al. 2021. "Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Pancreatic Cancer: Systematic Review and Still-Open Questions" Cancers 13, no. 13: 3119. https://doi.org/10.3390/cancers13133119