
Deep Learning with Quantitative Features of Magnetic Resonance Images to Predict Biochemical Recurrence of Radical Prostatectomy: A Multi-Center Study

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
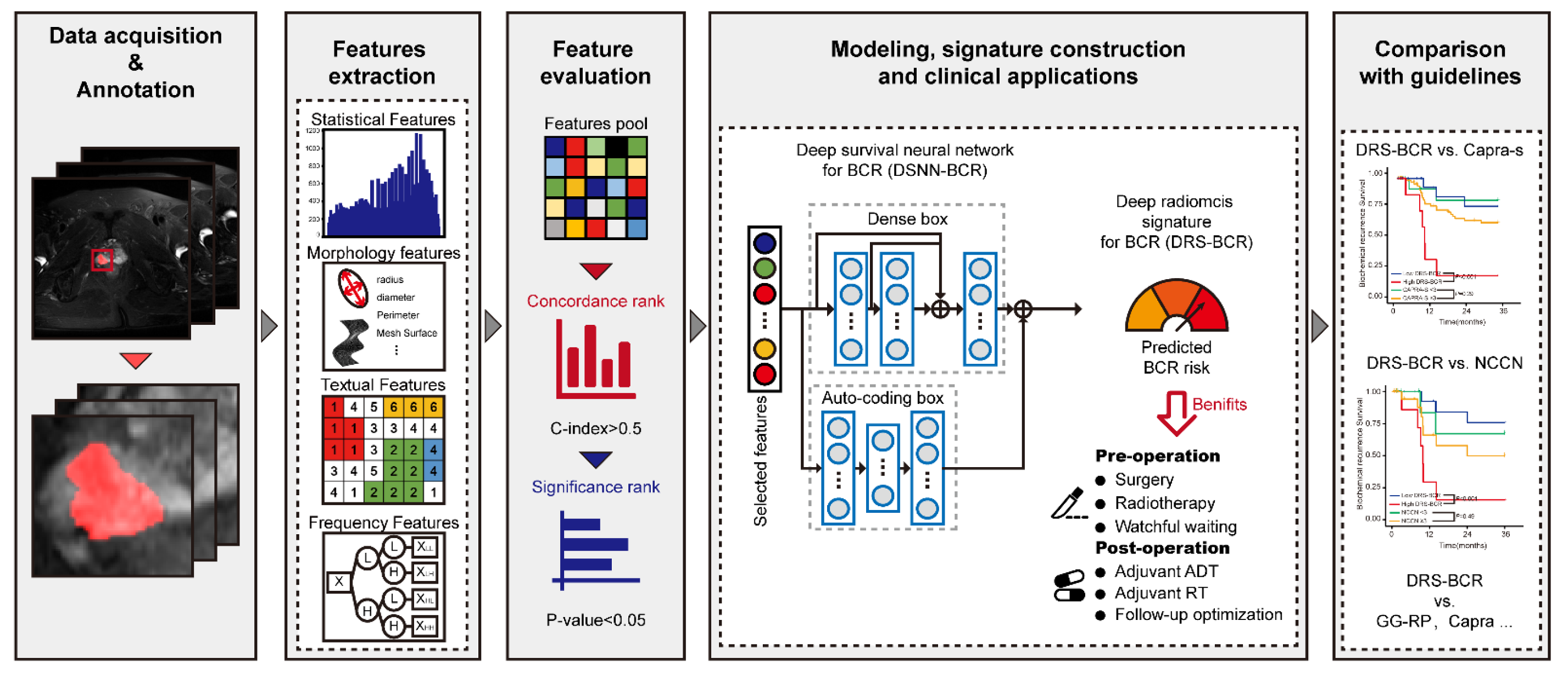
2.1. Study Design
2.2. MRI Protocol
2.3. Annotations
2.4. Radiomic Features of Mp-MRI Extraction
2.5. Deep Learning-Based Survival Analysis for Signature Construction to BCR Survival
2.6. Statistics
3. Results
3.1. Patient Characteristics
3.2. Evaluation of Quantitative Features of Mp-MRI for BCR-Free Survival
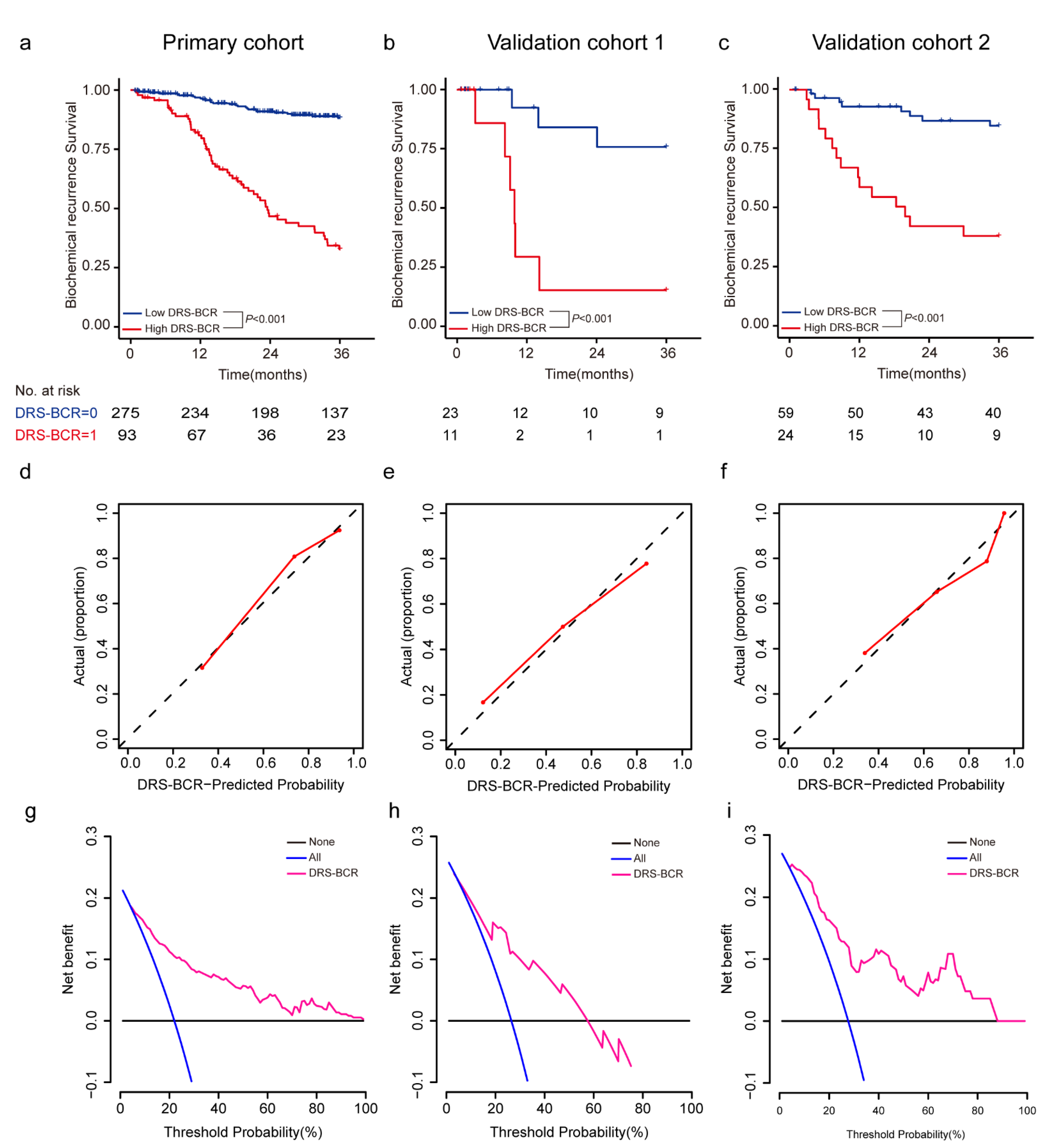
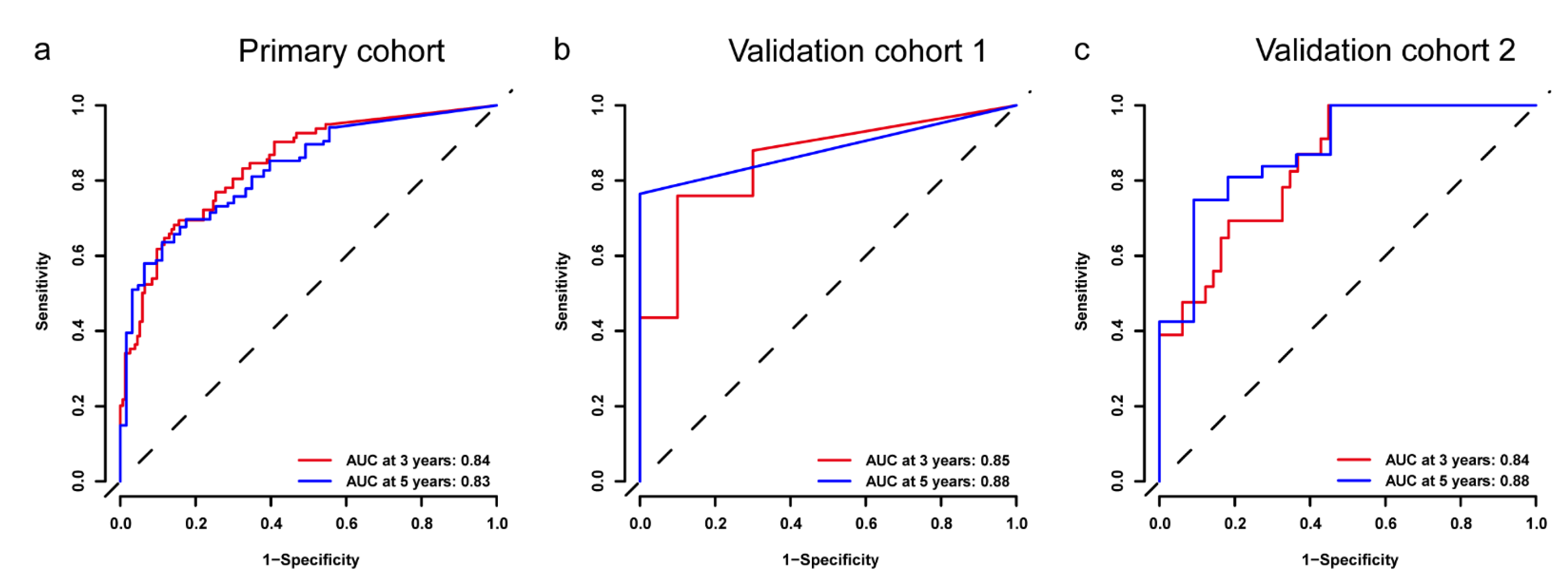
3.3. Assessment of DRS-BCR for Predicting BCR-Free Survival
3.4. Comparison between DRS-BCR and Clinical Nomogram
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Diaz, M.; Peabody, J.O.; Kapoor, V.; Sammon, J.; Rogers, C.G.; Stricker, H.; Lane, Z.; Gupta, N.; Bhandari, M.; Menon, M. Oncologic outcomes at 10 years following robotic radical prostatectomy. Eur. Urol. 2015, 67, 1168–1176. [Google Scholar] [CrossRef]
- Walz, J.; Chun, F.K.; Klein, E.A.; Reuther, A.; Saad, F.; Graefen, M.; Huland, H.; Karakiewicz, P.I. Nomogram predicting the probability of early recurrence after radical prostatectomy for prostate cancer. J. Urol. 2009, 181, 601–607. [Google Scholar] [CrossRef]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Partin, A.W. Time to prostate specific antigen recurrence after radical prostatectomy and risk of prostate cancer specific mortality. J. Urol. 2006, 176, 1404–1408. [Google Scholar] [CrossRef]
- Zelic, R.; Garmo, H.; Zugna, D.; Stattin, P.; Richiardi, L.; Akre, O.; Pettersson, A. Predicting Prostate Cancer Death with Different Pretreatment Risk Stratification Tools: A Head-to-head Comparison in a Nationwide Cohort Study. Eur. Urol. 2020, 77, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wang, S.; Dong, D.; Wei, J.; Fang, C.; Zhou, X.; Sun, K.; Li, L.; Li, B.; Wang, M.; et al. The Applications of Radiomics in Precision Diagnosis and Treatment of Oncology: Opportunities and Challenges. Theranostics 2019, 9, 1303–1322. [Google Scholar] [CrossRef]
- Zamboglou, C.; Carles, M.; Fechter, T.; Kiefer, S.; Reichel, K.; Fassbender, T.F.; Bronsert, P.; Koeber, G.; Schilling, O.; Ruf, J.; et al. Radiomic features from PSMA PET for non-invasive intraprostatic tumor discrimination and characterization in patients with intermediate- and high-risk prostate cancer—A comparison study with histology reference. Theranostics 2019, 9, 2595–2605. [Google Scholar] [CrossRef]
- Chen, T.; Li, M.; Gu, Y.; Zhang, Y.; Yang, S.; Wei, C.; Wu, J.; Li, X.; Zhao, W.; Shen, J. Prostate Cancer Differentiation and Aggressiveness: Assessment With a Radiomic-Based Model vs. PI-RADS v2. J. Magn. Reason. Imaging 2019, 49, 875–884. [Google Scholar] [CrossRef] [Green Version]
- Shao, L.; Yan, Y.; Liu, Z.; Ye, X.; Xia, H.; Zhu, X.; Zhang, Y.; Zhang, Z.; Chen, H.; He, W.; et al. Radiologist-like artificial intelligence for grade group prediction of radical prostatectomy for reducing upgrading and downgrading from biopsy. Theranostics 2020, 10, 10200–10212. [Google Scholar] [CrossRef] [PubMed]
- Shiradkar, R.; Ghose, S.; Jambor, I.; Taimen, P.; Ettala, O.; Purysko, A.S.; Madabhushi, A. Radiomic features from pretreatment biparametric MRI predict prostate cancer biochemical recurrence: Preliminary findings. J. Magn. Reason. Imaging 2018, 48, 1626–1636. [Google Scholar] [CrossRef]
- Bourbonne, V.; Fournier, G.; Vallieres, M.; Lucia, F.; Doucet, L.; Tissot, V.; Cuvelier, G.; Hue, S.; Du, H.L.; Perdriel, L.; et al. External Validation of an MRI-Derived Radiomics Model to Predict Biochemical Recurrence after Surgery for High-Risk Prostate Cancer. Cancers 2020, 12, 814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourbonne, V.; Vallieres, M.; Lucia, F.; Doucet, L.; Visvikis, D.; Tissot, V.; Pradier, O.; Hatt, M.; Schick, U. MRI-Derived Radiomics to Guide Post-operative Management for High-Risk Prostate Cancer. Front. Oncol. 2019, 9, 807. [Google Scholar] [CrossRef] [PubMed]
- Cookson, M.S.; Aus, G.; Burnett, A.L.; Canby-Hagino, E.D.; D’Amico, A.V.; Dmochowski, R.R.; Eton, D.T.; Forman, J.D.; Goldenberg, S.L.; Hernandez, J.; et al. Variation in the definition of biochemical recurrence in patients treated for localized prostate cancer: The American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel report and recommendations for a standard in the reporting of surgical outcomes. J. Urol. 2007, 177, 540–545. [Google Scholar]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Liu, Z.; Pleiss, G.; van der Maaten, L.; Weinberger, K. Convolutional Networks with Dense Connectivity. IEEE Trans. Pattern Anal. Mach. Intell 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coates, A.; Ng, A.Y. The Importance of Encoding Versus Training with Sparse Coding and Vector Quantization. In Proceedings of the 28th International Conference on Machine Learning, ICML 2011, Bellevue, WA, USA, 28 June–2 July 2011. [Google Scholar]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef]
- Kingma, D.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980. Available online: https://arxiv.org/abs/1412.6980 (accessed on 30 January 2017).
- Hu, M.B.; Yang, T.; Hu, J.M.; Zhu, W.H.; Jiang, H.W.; Ding, Q. Prognostic factors in Chinese patients with prostate cancer receiving primary androgen deprivation therapy: Validation of Japan Cancer of the Prostate Risk Assessment (J-CAPRA) score and impacts of pre-existing obesity and diabetes mellitus. Int. J. Clin. Oncol. 2018, 23, 591–598. [Google Scholar] [CrossRef]
- Lichtensztajn, D.Y.; Gomez, S.L.; Sieh, W.; Chung, B.I.; Cheng, I.; Brooks, J.D. Prostate cancer risk profiles of Asian-American men: Disentangling the effects of immigration status and race/ethnicity. J. Urol. 2014, 191, 952–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.; Kim, H.J.; Jeon, S.S.; Kwak, C.; Sung, G.T.; Kwon, T.G.; Park, J.Y.; Paick, S.H. Establishment of Korean prostate cancer database by the Korean Urological Oncology Society. Investig. Clin. Urol. 2017, 58, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, N.; Nakai, Y.; Miyake, M.; Anai, S.; Inoue, T.; Fujii, T.; Konishi, N.; Fujimoto, K. Trends in risk classification and primary therapy of Japanese patients with prostate cancer in Nara urological research and treatment group (NURTG)—comparison between 2004–2006, 2007–2009, and 2010–2012. BMC Cancer 2017, 17, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punnen, S.; Freedland, S.J.; Presti, J.C., Jr.; Aronson, W.J.; Terris, M.K.; Kane, C.J.; Amling, C.L.; Carroll, P.R.; Cooperberg, M.R. Multi-institutional validation of the CAPRA-S score to predict disease recurrence and mortality after radical prostatectomy. Eur. Urol. 2014, 65, 1171–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Xu, C.; Lee, H.J.; Ren, S.; Zi, X.; Zhang, Z.; Wang, H.; Yu, Y.; Yang, C.; Gao, X.; et al. A genomic and epigenomic atlas of prostate cancer in Asian populations. Nature 2020, 580, 93–99. [Google Scholar] [CrossRef]
- Schulman, C.C.; Debruyne, F.M.; Forster, G.; Selvaggi, F.P.; Zlotta, A.R.; Witjes, W.P. 4-Year follow-up results of a European prospective randomized study on neoadjuvant hormonal therapy prior to radical prostatectomy in T2-3N0M0 prostate cancer. European Study Group on Neoadjuvant Treatment of Prostate Cancer. Eur. Urol. 2000, 38, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Labrie, F.; Cusan, L.; Gomez, J.L.; Diamond, P.; Suburu, R.; Lemay, M.; Tetu, B.; Fradet, Y.; Belanger, A.; Candas, B. Neoadjuvant hormonal therapy: The Canadian experience. Urology 1997, 49, 56–64. [Google Scholar] [CrossRef]
- McClintock, T.R.; von Landenberg, N.; Cole, A.P.; Lipsitz, S.R.; Gild, P.; Sun, M.; Fletcher, S.A.; Roghmann, F.; Menon, M.; Nguyen, P.L.; et al. Neoadjuvant Androgen Deprivation Therapy Prior to Radical Prostatectomy: Recent Trends in Utilization and Association with Postoperative Surgical Margin Status. Ann. Surg. Oncol. 2019, 26, 297–305. [Google Scholar] [CrossRef]
- Klingenberg, S.; Jochumsen, M.R.; Ulhøi, B.P.; Fredsøe, J.; Sørensen, K.D.; Borre, M.; Bouchelouche, K. 68Ga-PSMA PET/CT for Primary Lymph Node and Distant Metastasis NM Staging of High-Risk Prostate Cancer. J. Nucl. Med. 2021, 62, 214–220. [Google Scholar] [CrossRef]
- Giesel, F.L.; Kesch, C.; Yun, M.; Cardinale, J.; Haberkorn, U.; Kopka, K.; Kratochwil, C.; Hadaschik, B.A. 18F-PSMA-1007 PET/CT detects micrometastases in a patient with biochemically recurrent prostate cancer. Clin. Genitourin Cancer 2017, 15, e497–e499. [Google Scholar] [CrossRef] [Green Version]
- Sanseverino, R.; Intilla, O.; di Mauro, U.; Molisso, G.; Addesso, M.; Napodano, G. Predictive Factors of Nodal Micrometastasis in Patients with Organ Confined Prostate Cancer. Anticancer Res. 2017, 37, 2082–2083. [Google Scholar]
- Chen, S.; Zhu, G.; Yang, Y.; Wang, F.; Xiao, Y.T.; Zhang, N.; Bian, X.; Zhu, Y.; Yu, Y.; Liu, F.; et al. Single-cell analysis reveals transcriptomic remodellings in distinct cell types that contribute to human prostate cancer progression. Nat. Cell Biol. 2021, 23, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Murray, N.P.; Aedo, S.; Fuentealba, C.; Reyes, E.; Salazar, A.; Lopez, M.A.; Minzer, S.; Orrego, S.; Guzman, E. Minimal Residual Disease Defines the Risk and Time to Biochemical Failure in Patients with Pt2 and Pt3a Prostate Cancer Treated With Radical Prostatectomy: An Observational Prospective Study. Urol. J. 2020, 17, 262–270. [Google Scholar] [PubMed]
- Jindal, I.; Nokleby, M.; Chen, X. Learning Deep Networks from Noisy Labels with Dropout Regularization. In Proceedings of the 2016 IEEE 16th International Conference on Data Mining (ICDM), Barcelona, Spain, 12–15 December 2016; pp. 967–972. [Google Scholar]
- Pan, S.J.; Yang, Q. A Survey on Transfer Learning. IEEE Trans. Knowl. Data Eng. 2010, 22, 1345–1359. [Google Scholar] [CrossRef]
- Osman, S.O.S.; Leijenaar, R.T.H.; Cole, A.J.; Lyons, C.A.; Hounsell, A.R.; Prise, K.M.; O’Sullivan, J.M.; Lambin, P.; McGarry, C.K.; Jain, S. Computed Tomography-based Radiomics for Risk Stratification in Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 448–456. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PC (PUTH) | VC (BJFH) | VC2 (PUPH) | p | |
|---|---|---|---|---|
| n = 368 | n = 34 | n = 83 | ||
| No. of BCR event (%) | 99 (27.1) | 16 (47.1) | 31 (37.3) | 0.016 |
| Age (Median) | 70 | 68.5 | 68.0 | 0.275 |
| PSA (Median) | 10.7 | 9.89 | 13.4 | 0.883 |
| GG-NB | 0.125 | |||
| 1 | 138 | 13 | 29 | |
| 2 | 114 | 10 | 23 | |
| 3 | 63 | 6 | 14 | |
| 4 | 89 | 3 | 11 | |
| 5 | 81 | 2 | 6 | |
| cT | 0.436 | |||
| 2 | 221 | 15 | 44 | |
| 3 | 264 | 19 | 39 | |
| 4 | 9 | |||
| pT | 0.687 | |||
| 1 | 2 | 1 | ||
| 2 | 303 | 22 | 57 | |
| 3 | 165 | 12 | 22 | |
| 4 | 15 | 3 | ||
| GG-RP | 0.173 | |||
| 1 | 82 | 4 | 13 | |
| 2 | 127 | 10 | 28 | |
| 3 | 93 | 8 | 18 | |
| 4 | 65 | 9 | 8 | |
| 5 | 118 | 3 | 16 | |
| SM | 0.172 | |||
| Positive | 170 | 12 | 38 | |
| Negative | 315 | 21 | 45 | |
| EPE | 0.639 | |||
| Positive | 171 | 11 | 25 | |
| Negative | 314 | 23 | 58 | |
| SVI | 0.940 | |||
| Positive | 67 | 4 | 11 | |
| Negative | 418 | 30 | 72 | |
| CAPRA | 0.248 | |||
| Low | 53 | 9 | 10 | |
| Intermediate | 168 | 12 | 34 | |
| High | 148 | 13 | 39 |
| HR | p | PC (n = 369) | VC1 (n = 34) | VC2 (n = 83) | |
|---|---|---|---|---|---|
| GG-RP | 1.645 | 0.001 | 0.583 [0.53–0.636] | 0.564 [0.419–0.709] | 0.689 [0.601–0.777] |
| CAPRA-S | 1.339 | <0.001 | 0.677 [0.62–0.734] | 0.654 [0.49–0.818] | 0.654 [0.544–0.764] |
| NCCN | 1.9022 | <0.001 | 0.586 [0.548–0.624] | 0.535 [0.408–0.662] | 0.583 [0.498–0.668] |
| CAPRA | 1.306 | <0.001 | 0.677 [0.618–0.736] | 0.552 [0.385–0.719] | 0.614 [0.509–0.719] |
| DRS-BCR | 1.705 | <0.001 | 0.802 | 0.811 | 0.794 |
| [0.758–0.846] | [0.722–0.9] | [0.718–0.87] | |||
| DRC-BCR | 1.654 | <0.001 | 0.807 [0.76–0.854] | 0.794 [0.685–0.903] | 0.8 [0.723–0.877] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, Y.; Shao, L.; Liu, Z.; He, W.; Yang, G.; Liu, J.; Xia, H.; Zhang, Y.; Chen, H.; Liu, C.; et al. Deep Learning with Quantitative Features of Magnetic Resonance Images to Predict Biochemical Recurrence of Radical Prostatectomy: A Multi-Center Study. Cancers 2021, 13, 3098. https://doi.org/10.3390/cancers13123098
Yan Y, Shao L, Liu Z, He W, Yang G, Liu J, Xia H, Zhang Y, Chen H, Liu C, et al. Deep Learning with Quantitative Features of Magnetic Resonance Images to Predict Biochemical Recurrence of Radical Prostatectomy: A Multi-Center Study. Cancers. 2021; 13(12):3098. https://doi.org/10.3390/cancers13123098
Chicago/Turabian StyleYan, Ye, Lizhi Shao, Zhenyu Liu, Wei He, Guanyu Yang, Jiangang Liu, Haizhui Xia, Yuting Zhang, Huiying Chen, Cheng Liu, and et al. 2021. "Deep Learning with Quantitative Features of Magnetic Resonance Images to Predict Biochemical Recurrence of Radical Prostatectomy: A Multi-Center Study" Cancers 13, no. 12: 3098. https://doi.org/10.3390/cancers13123098