
Expression of X-Linked Inhibitor of Apoptosis Protein (XIAP) in Breast Cancer Is Associated with Shorter Survival and Resistance to Chemotherapy

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Breast Cancer Samples and Expression Profiling
2.2. Expression Data Analysis
2.3. Statistical Analysis
3. Results
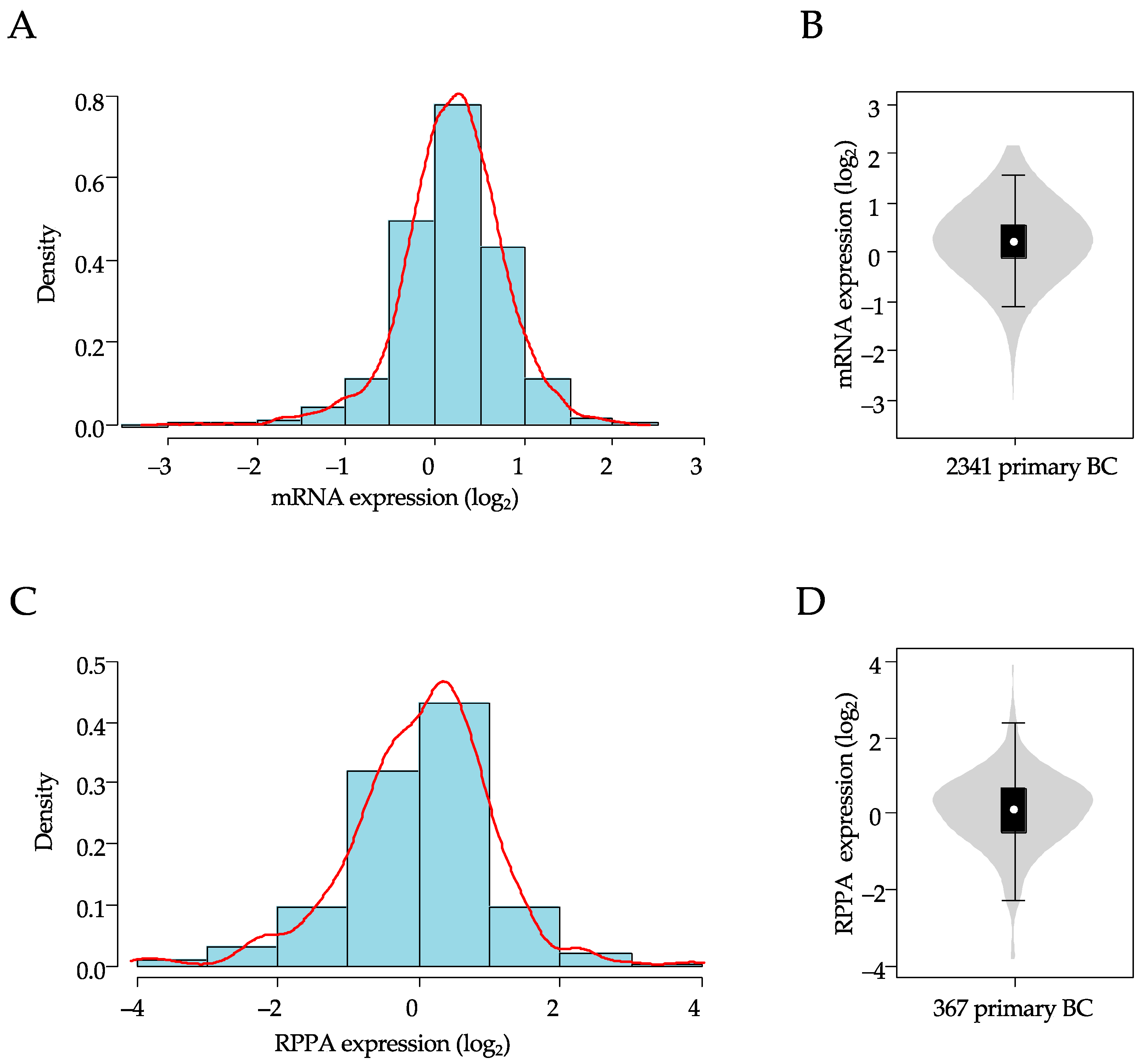
3.1. Patient Population and XIAP Expression
3.2. Correlations of XIAP Expression with Clinicopathological Features
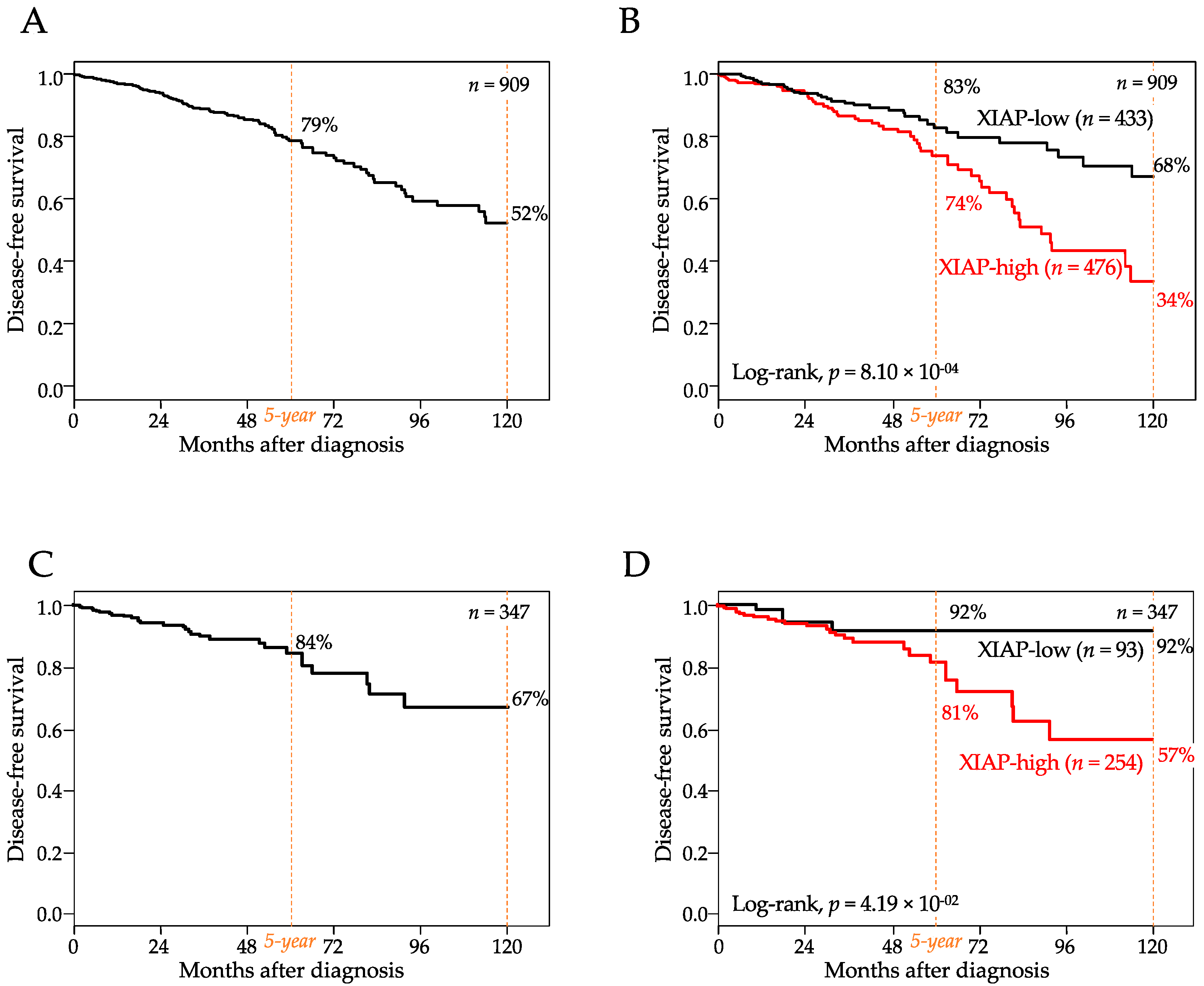
3.3. Correlations of XIAP Expression with Disease-Free Survival
3.4. Correlations of XIAP Expression with Pathological Response to Chemotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lewis, J.; Burstein, E.; Reffey, S.B.; Bratton, S.B.; Roberts, A.B.; Duckett, C.S. Uncoupling of the signaling and caspase-inhibitory properties of X-linked inhibitor of apoptosis. J. Biol. Chem. 2004, 279, 9023–9029. [Google Scholar] [CrossRef] [Green Version]
- Gyrd-Hansen, M.; Meier, P. IAPs: From caspase inhibitors to modulators of NF-κB, inflammation and cancer. Nat. Rev. Cancer 2010, 10, 561–574. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. The Hallmarks of Cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Jost, P.J.; Vucic, D. Regulation of Cell Death and Immunity by XIAP. Cold Spring Harb. Perspect. Biol. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Harlin, H.; Reffey, S.B.; Duckett, C.S.; Lindsten, T.; Thompson, C.B. Characterization of XIAP-deficient mice. Mol. Cell. Biol. 2001, 21, 3604–3608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tu, H.; Costa, M. XIAP’s Profile in human cancer. Biomolecules 2020, 10, 1493. [Google Scholar] [CrossRef]
- Evans, M.K.; Sauer, S.J.; Nath, S.; Robinson, T.J.; Morse, M.A.; Devi, G.R. X-linked inhibitor of apoptosis protein mediates tumor cell resistance to antibody-dependent cellular cytotoxicity. Cell Death Dis. 2016, 7, e2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allensworth, J.L.; Aird, K.M.; Aldrich, A.J.; Batinic-Haberle, I.; Devi, G.R. XIAP inhibition and generation of reactive oxygen species enhances TRAIL sensitivity in inflammatory breast cancer cells. Mol. Cancer Ther. 2012, 11, 1518–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Wu, Z.; Mei, Y.; Wu, M. XIAP inhibits autophagy via XIAP-Mdm2-p53 signalling. EMBO J. 2013, 32, 2204–2216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalaoui, N.; Vaux, D.L. Recent advances in understanding inhibitor of apoptosis proteins. F1000Research 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.K.; Brown, M.C.; Geradts, J.; Bao, X.; Robinson, T.J.; Jolly, M.K.; Vermeulen, P.B.; Palmer, G.M.; Gromeier, M.; Levine, H.; et al. XIAP regulation by MNK links MAPK and NFκB signaling to determine an aggressive breast cancer phenotype. Cancer Res. 2018, 78, 1726–1738. [Google Scholar] [CrossRef] [Green Version]
- Ono, H.; Iizumi, Y.; Goi, W.; Sowa, Y.; Taguchi, T.; Sakai, T. Ribosomal protein S3 regulates XIAP expression independently of the NF-κB pathway in breast cancer cells. Oncol. Rep. 2017, 38, 3205–3210. [Google Scholar] [CrossRef]
- Yu, Y.; Jin, H.; Xu, J.; Gu, J.; Li, X.; Xie, Q.; Huang, H.; Li, J.; Tian, Z.; Jiang, G.; et al. XIAP overexpression promotes bladder cancer invasion in vitro and lung metastasis in vivo via enhancing nucleolin-mediated Rho-GDIβ mRNA stability. Int. J. Cancer 2018, 142, 2040–2055. [Google Scholar] [CrossRef] [Green Version]
- Liston, P.; Young, S.S.; Mackenzie, A.E.; Korneluk, R.G. Life and death decisions: The role of the IAPs in modulating programmed cell death. Apoptosis 1997, 2, 423–441. [Google Scholar] [CrossRef] [PubMed]
- Owens, T.W.; Foster, F.M.; Tanianis-Hughes, J.; Cheung, J.Y.; Brackenbury, L.; Streuli, C.H. Analysis of inhibitor of apoptosis protein family expression during mammary gland development. BMC Dev. Biol. 2010, 10, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.L. Mechanisms of apoptosis resistance in breast cancer. In Breast Cancer and Molecular Medicine; Piccart, M.J., Hung, M.-C., Solin, L.J., Cardoso, F., Wood, W.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2006; pp. 841–858. ISBN 978-3-540-28266-2. [Google Scholar]
- Abbas, R.; Larisch, S. Targeting XIAP for promoting cancer cell death-the story of ARTS and SMAC. Cells 2020, 9, 663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holcik, M.; Lefebvre, C.; Yeh, C.; Chow, T.; Korneluk, R.G. A new internal-ribosome-entry-site motif potentiates XIAP-mediated cytoprotection. Nat. Cell Biol. 1999, 1, 190–192. [Google Scholar] [CrossRef]
- Shahar, N.; Larisch, S. Inhibiting the inhibitors: Targeting anti-apoptotic proteins in cancer and therapy resistance. Drug Resist. Updates 2020, 52, 100712. [Google Scholar] [CrossRef]
- Tamm, I.; Kornblau, S.M.; Segall, H.; Krajewski, S.; Welsh, K.; Kitada, S.; Scudiero, D.A.; Tudor, G.; Qui, Y.H.; Monks, A.; et al. Expression and prognostic significance of IAP-family genes in human cancers and myeloid leukemias. Clin. Cancer Res. 2000, 6, 1796. [Google Scholar]
- Shi, Y.-H.; Ding, W.-X.; Zhou, J.; He, J.-Y.; Xu, Y.; Gambotto, A.A.; Rabinowich, H.; Fan, J.; Yin, X.-M. Expression of X-linked inhibitor-of-apoptosis protein in hepatocellular carcinoma promotes metastasis and tumor recurrence. Hepatology 2008, 48, 497–507. [Google Scholar] [CrossRef] [Green Version]
- Dizdar, L.; Jünemann, L.M.; Werner, T.A.; Verde, P.E.; Baldus, S.E.; Stoecklein, N.H.; Knoefel, W.T.; Krieg, A. Clinicopathological and functional implications of the inhibitor of apoptosis proteins survivin and XIAP in esophageal cancer. Oncol. Lett. 2018, 15, 3779–3789. [Google Scholar] [CrossRef]
- Gao, X.; Zhang, L.; Wei, Y.; Yang, Y.; Li, J.; Wu, H.; Yin, Y. Prognostic value of XIAP level in patients with various cancers: A systematic review and meta-analysis. J. Cancer 2019, 10, 1528–1537. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhu, J.; Tang, Y.; Li, F.; Zhou, H.; Peng, B.; Zhou, C.; Fu, R. X-linked inhibitor of apoptosis positive nuclear labeling: A new independent prognostic biomarker of breast invasive ductal carcinoma. Diagn. Pathol. 2011, 6, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, A.R.; Siraj, A.K.; Ahmed, M.; Bu, R.; Pratheeshkumar, P.; Alrashed, A.M.; Qadri, Z.; Ajarim, D.; Al-Dayel, F.; Beg, S.; et al. XIAP over-expression is an independent poor prognostic marker in Middle Eastern breast cancer and can be targeted to induce efficient apoptosis. BMC Cancer 2017, 17, 640. [Google Scholar] [CrossRef]
- Pluta, P.; Jeziorski, A.; Cebula-Obrzut, A.P.; Wierzbowska, A.; Piekarski, J.; Smolewski, P. Expression of IAP family proteins and its clinical importance in breast cancer patients. Neoplasma 2015, 62, 666–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.C.; Liu, Q.; Dai, J.Q.; Yin, Z.Q.; Tang, L.; Ma, Y.; Lin, X.L.; Wang, H.X. Tissue microarray analysis of X-linked inhibitor of apoptosis (XIAP) expression in breast cancer patients. Med. Oncol. 2014, 31, 764. [Google Scholar] [CrossRef] [PubMed]
- Arora, J.; Sauer, S.J.; Tarpley, M.; Vermeulen, P.; Rypens, C.; Van Laere, S.; Williams, K.P.; Devi, G.R.; Dewhirst, M.W. Inflammatory breast cancer tumor emboli express high levels of anti-apoptotic proteins: Use of a quantitative high content and high-throughput 3D IBC spheroid assay to identify targeting strategies. Oncotarget 2017, 8, 25848–25863. [Google Scholar] [CrossRef] [Green Version]
- Bertucci, F.; Finetti, P.; Simeone, I.; Hendrickx, W.; Wang, E.; Marincola, F.M.; Viens, P.; Mamessier, E.; Ceccarelli, M.; Birnbaum, D.; et al. The immunologic constant of rejection classification refines the prognostic value of conventional prognostic signatures in breast cancer. Br. J. Cancer 2018, 119, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, R.A.; Hobbs, B.; Collin, F.; Beazer-Barclay, Y.D.; Antonellis, K.J.; Scherf, U.; Speed, T.P. Exploration, normalization, and summaries of high density oligonucleotide array probe level data. Biostatistics 2003, 4, 249–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertucci, F.; Finetti, P.; Viens, P.; Birnbaum, D. EndoPredict predicts for the response to neoadjuvant chemotherapy in ER-positive, HER2-negative breast cancer. Cancer Lett. 2014, 355, 70–75. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [Green Version]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [Green Version]
- Van De Vijver, M.J.; He, Y.D.; Van’t Veer, L.J.; Dai, H.; Hart, A.A.; Voskuil, D.W.; Schreiber, G.J.; Peterse, J.L.; Roberts, C.; Marton, M.J.; et al. A gene-expression signature as a predictor of survival in breast cancer. N. Engl. J. Med. 2002, 347, 1999–2009. [Google Scholar] [CrossRef] [Green Version]
- Parker, J.S.; Mullins, M.; Cheang, M.C.; Leung, S.; Voduc, D.; Vickery, T.; Davies, S.; Fauron, C.; He, X.; Hu, Z.; et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. J. Clin. Oncol. 2009, 27, 1160. [Google Scholar] [CrossRef] [PubMed]
- Sotiriou, C.; Wirapati, P.; Loi, S.; Harris, A.; Fox, S.; Smeds, J.; Nordgren, H.; Farmer, P.; Praz, V.; Haibe-Kains, B.; et al. Gene expression profiling in breast cancer: Understanding the molecular basis of histologic grade to improve prognosis. J. Natl. Cancer Inst. 2006, 98, 262–272. [Google Scholar] [CrossRef]
- Koboldt, D.C.; Fulton, R.S.; McLellan, M.D.; Schmidt, H.; Kalicki-Veizer, J.; McMichael, J.F.; Fulton, L.L.; Dooling, D.J.; Ding, L.; Mardis, E.R.; et al. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Heer, E.; Harper, A.; Escandor, N.; Sung, H.; McCormack, V.; Fidler-Benaoudia, M.M. Global burden and trends in premenopausal and postmenopausal breast cancer: A population-based study. Lancet Glob. Health 2020, 8, e1027–e1037. [Google Scholar] [CrossRef]
- U.S. Breast Cancer Statistics. Available online: https://www.breastcancer.org/symptoms/understand_bc/statistics (accessed on 20 February 2021).
- Redig, A.J.; McAllister, S.S. Breast cancer as a systemic disease: A view of metastasis. J. Intern. Med. 2013, 274, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulda, S.; Gorman, A.M.; Hori, O.; Samali, A. Cellular stress responses: Cell survival and cell death. Int. J. Cell. Biol. 2010, 2010, 214074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, J.C. Dysregulation of apoptosis in cancer. J. Clin. Oncol. 1999, 17, 2941. [Google Scholar] [CrossRef]
- Pazarentzos, E.; Bivona, T.G. Adaptive stress signaling in targeted cancer therapy resistance. Oncogene 2015, 34, 5599–5606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, J.; Kearney, C.J.; Hawkins, E.D.; Silke, J.; Oliaro, J. The immuno-modulatory effects of inhibitor of apoptosis protein antagonists in cancer immunotherapy. Cells 2020, 9, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amantana, A.; London, C.A.; Iversen, P.L.; Devi, G.R. X-linked inhibitor of apoptosis protein inhibition induces apoptosis and enhances chemotherapy sensitivity in human prostate cancer cells. Mol. Cancer Ther. 2004, 3, 699–707. [Google Scholar] [PubMed]
- LaCasse, E.C. Pulling the plug on a cancer cell by eliminating XIAP with AEG35156. Cancer Let. 2013, 332, 215–224. [Google Scholar] [CrossRef]
- Cao, C.; Mu, Y.; Hallahan, D.E.; Lu, B. XIAP and survivin as therapeutic targets for radiation sensitization in preclinical models of lung cancer. Oncogene 2004, 23, 7047–7052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devi, G.R.; Beer, T.M.; Corless, C.L.; Arora, V.; Weller, D.L.; Iversen, P.L. In vivo bioavailability and pharmacokinetics of a c-MYC antisense phosphorodiamidate morpholino oligomer, AVI-4126, in solid tumors. Clin. Cancer Res. 2005, 11, 3930–3938. [Google Scholar] [CrossRef] [Green Version]
- Arora, V.; Devi, G.R.; Iversen, P.L. Neutrally charged phosphorodiamidate morpholino antisense oligomers: Uptake, efficacy and pharmacokinetics. Curr. Pharm. Biotechnol. 2004, 5, 431–439. [Google Scholar] [CrossRef]
- Panayotopoulou, E.G.; Müller, A.-K.; Börries, M.; Busch, H.; Hu, G.; Lev, S. Targeting of apoptotic pathways by SMAC or BH3 mimetics distinctly sensitizes paclitaxel-resistant triple negative breast cancer cells. Oncotarget 2017, 8, 45088–45104. [Google Scholar] [CrossRef] [PubMed]
- Cong, H.; Xu, L.; Wu, Y.; Qu, Z.; Bian, T.; Zhang, W.; Xing, C.; Zhuang, C. Inhibitor of apoptosis protein (IAP) antagonists in anticancer agent discovery: Current status and perspectives. J. Med. Chem. 2019, 62, 5750–5772. [Google Scholar] [CrossRef]
- Xie, X.; Lee, J.; Liu, H.; Pearson, T.; Lu, A.Y.; Tripathy, D.; Devi, G.R.; Bartholomeusz, C.; Ueno, N.T. Birinapant enhances gemcitabine’s antitumor efficacy in triple-negative breast cancer by inducing intrinsic pathway–dependent apoptosis. Mol. Cancer Ther. 2021, 20, 296. [Google Scholar] [CrossRef]
- Allensworth, J.L.; Sauer, S.J.; Lyerly, H.K.; Morse, M.A.; Devi, G.R. Smac mimetic Birinapant induces apoptosis and enhances TRAIL potency in inflammatory breast cancer cells in an IAP-dependent and TNF-alpha-independent mechanism. Breast Cancer Res. Treat. 2013, 137, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Dougan, S.K.; Dougan, M. Regulation of innate and adaptive antitumor immunity by IAP antagonists. Immunotherapy 2018, 10, 787–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulda, S. Promises and challenges of smac mimetics as cancer therapeutics. Clin. Cancer Res. 2015, 21, 5030–5036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaravadi, R.K.; Senzer, N.N.; Martin, L.P.; Schilder, R.J.; LoRusso, P.; Papadopoulos, K.P.; Weng, D.E.; Graham, M.; Adjei, A.A. A phase I study of birinapant (TL32711) combined with multiple chemotherapies evaluating tolerability and clinical activity for solid tumor patients. J. Clin. Oncol. 2013, 31, 2504. [Google Scholar] [CrossRef]
- Amaravadi, R.K.; Schilder, R.J.; Martin, L.P.; Levin, M.; Graham, M.A.; Weng, D.E.; Adjei, A.A. A phase I study of the SMAC-mimetic birinapant in adults with refractory solid tumors or lymphoma. Mol. Cancer Ther. 2015, 14, 2569–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalaoui, N.; Merino, D.; Giner, G.; Vaillant, F.; Chau, D.; Liu, L.; Kratina, T.; Pal, B.; Whittle, J.R.; Etemadi, N.; et al. Targeting triple-negative breast cancers with the Smac-mimetic birinapant. Cell. Death Differ. 2020, 27, 2768–2780. [Google Scholar] [CrossRef]
- Callagy, G.M.; Pharoah, P.D.; Pinder, S.E.; Hsu, F.D.; Nielsen, T.O.; Ragaz, J.; Ellis, I.O.; Huntsman, D.; Caldas, C. Bcl-2 is a prognostic marker in breast cancer independently of the nottingham prognostic index. Clin. Cancer Res. 2006, 12, 2468. [Google Scholar] [CrossRef] [Green Version]
- Van ‘t Veer, L.J.; Dai, H.; van de Vijver, M.J.; He, Y.D.; Hart, A.A.M.; Mao, M.; Peterse, H.L.; van der Kooy, K.; Marton, M.J.; Witteveen, A.T.; et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002, 415, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Chen, M.B.; Wang, L.Q.; Yang, L.; Liu, C.Y.; Lu, P.H. Bcl-2 expression predicts sensitivity to chemotherapy in breast cancer: A systematic review and meta-analysis. J. Exp. Clin. Cancer Res. 2013, 32, 105. [Google Scholar] [CrossRef] [Green Version]
- Callagy, G.M.; Webber, M.J.; Pharoah, P.D.P.; Caldas, C. Meta-analysis confirms BCL2 is an independent prognostic marker in breast cancer. BMC Cancer 2008, 8, 153. [Google Scholar] [CrossRef] [Green Version]
- Hess, K.R.; Anderson, K.; Symmans, W.F.; Valero, V.; Ibrahim, N.; Mejia, J.A.; Booser, D.; Theriault, R.L.; Buzdar, A.U.; Dempsey, P.J.; et al. Pharmacogenomic Predictor of Sensitivity to Preoperative Chemotherapy with Paclitaxel and Fluorouracil, Doxorubicin, and Cyclophosphamide in Breast Cancer. J. Clin. Oncol. 2006, 24, 4236–4244. [Google Scholar] [CrossRef] [Green Version]
- Bonnefoi, H.; Potti, A.; Delorenzi, M.; Mauriac, L.; Campone, M.; Tubiana-Hulin, M.; Petit, T.; Rouanet, P.; Jassem, J.; Blot, E.; et al. Validation of Gene Signatures That Predict the Response of Breast Cancer to Neoadjuvant Chemotherapy: A Substudy of the EORTC 10994/BIG 00-01 Clinical Trial. Lancet Oncol. 2007, 8, 1071–1078. [Google Scholar] [CrossRef]
- Iwamoto, T.; Bianchini, G.; Booser, D.; Qi, Y.; Coutant, C.; Shiang, C.Y.-H.; Santarpia, L.; Matsuoka, J.; Hortobagyi, G.N.; Symmans, W.F.; et al. Gene Pathways Associated with Prognosis and Chemotherapy Sensitivity in Molecular Subtypes of Breast Cancer. J. Natl. Cancer Inst. 2011, 103, 264–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabchy, A.; Valero, V.; Vidaurre, T.; Lluch, A.; Gomez, H.; Martin, M.; Qi, Y.; Barajas-Figueroa, L.J.; Souchon, E.; Coutant, C.; et al. Evaluation of a 30-Gene Paclitaxel, Fluorouracil, Doxorubicin, and Cyclophosphamide Chemotherapy Response Predictor in a Multicenter Randomized Trial in Breast Cancer. Clin. Cancer Res. 2010, 16, 5351–5361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desmedt, C.; Di Leo, A.; de Azambuja, E.; Larsimont, D.; Haibe-Kains, B.; Selleslags, J.; Delaloge, S.; Duhem, C.; Kains, J.-P.; Carly, B.; et al. Multifactorial Approach to Predicting Resistance to Anthracyclines. J. Clin. Oncol. 2011, 29, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Hatzis, C.; Pusztai, L.; Valero, V.; Booser, D.J.; Esserman, L.; Lluch, A.; Vidaurre, T.; Holmes, F.; Souchon, E.; Wang, H.; et al. A Genomic Predictor of Response and Survival Following Taxane-Anthracycline Chemotherapy for Invasive Breast Cancer. JAMA 2011, 305, 1873–1881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popovici, V.; Chen, W.; Gallas, B.G.; Hatzis, C.; Shi, W.; Samuelson, F.W.; Nikolsky, Y.; Tsyganova, M.; Ishkin, A.; Nikolskaya, T.; et al. Effect of Training-Sample Size and Classification Difficulty on the Accuracy of Genomic Predictors. Breast Cancer Res. 2010, 12, R5. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | n | Global | XIAP mRNA | ||
|---|---|---|---|---|---|
| n (%) | Mean (Range) | p-Value * | |||
| Age at diagnosis (year) | 3.81 × 10−2 | ||||
| ≤50 | 991 | 991 (42%) | 0.23 (−2.3–2.0) | ||
| >50 | 1343 | 1343 (58%) | 0.17 (−3.0–2.1) | ||
| Pathological type | 4.35 × 10−2 | ||||
| IDC | 1211 | 1211 (75%) | 0.19 (−3.0–2.1) | ||
| ILC | 215 | 215 (13%) | 0.12 (−2.4–1.3) | ||
| other | 190 | 190 (12%) | 0.17 (−2.6–2.0) | ||
| Pathological lymph node (pN) | 9.21 × 10−2 | ||||
| negative | 517 | 517 (44%) | 0.06 (−3.0–2.0) | ||
| positive | 670 | 670 (56%) | 0.17 (−2.1–1.9) | ||
| Pathological size (pT) | 0.2 | ||||
| pT1 | 321 | 321 (23%) | 0.21 (−2.4–1.93) | ||
| pT2-3 | 1070 | 1070 (77%) | 0.12 (−3.0–2.0) | ||
| Genomic grade (GGI) | 1.15 × 10−3 | ||||
| low | 758 | 758 (32%) | 0.24 (−2.4–2.0) | ||
| high | 1583 | 1583 (68%) | 0.18 (−3.0–2.1) | ||
| ER status ** | 1.73 × 10−12 | ||||
| negative | 917 | 917 (39%) | 0.1 (−2.6–2.1) | ||
| positive | 1424 | 1424 (61%) | 0.26 (−3.0–2.0) | ||
| PR status ** | 4.68 × 10−7 | ||||
| negative | 1419 | 1419 (61%) | 0.15 (−3.0–2.1) | ||
| positive | 922 | 922 (39%) | 0.27 (−2.7–1.9) | ||
| HER2 status ** | 0.355 | ||||
| negative | 2068 | 2068 (88%) | 0.2 (−3.0–2.1) | ||
| positive | 273 | 273 (12%) | 0.17 (−1.6–1.8) | ||
| Molecular subtype mRNA status | 2.86 × 10−14 | ||||
| HR+/HER2− | 1382 | 1382 (59%) | 0.26 (−3.0–2.0) | ||
| HER2+ | 273 | 273 (12%) | 0.17 (−1.6–1.8) | ||
| TN | 686 | 686 (29%) | 0.07 (−2.6–2.1) | ||
| PAM50 subtypes | 6.93 × 10−23 | ||||
| basal | 641 | 641 (27%) | 0.06 (−2.6–2.1) | ||
| HER2 | 320 | 320 (14%) | 0.12 (−3.0–1.9) | ||
| luminal A | 668 | 668 (29%) | 0.27 (−2.4–2.0) | ||
| luminal B | 516 | 516 (22%) | 0.35 (−1.8–2.0) | ||
| normal-like | 196 | 196 (8%) | 0.14 (−1.7–1.9) | ||
| DFS event | no | 809 | 809 (89%) | 0.13 (−3.0–2.0) | 1.55 × 10−2 |
| yes | 100 | 100 (11%) | 0.33 (−1.8–1.5) | ||
| 5-year DFS [95% CI] | 909 | 79% [74–84] | |||
| Pathological complete response (pCR) | 5.81 × 10−4 | ||||
| no | 922 | 922 (77%) | 0.26 (−1.4–2.1) | ||
| yes | 281 | 281 (23%) | 0.15 (−2.3–1.9) | ||
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| n | HR [95%CI] | p-Value | n | HR [95%CI] | p-Value | |
| Age at diagnosis, >50 vs. ≤50 years | 909 | 1.24 [0.81–1.88] | 0.323 | |||
| Genomic grade (GGI), high vs. low | 909 | 1.30 [0.81–2.07] | 0.275 | |||
| Pathological lymph node, pos. vs. neg. | 776 | 2.05 [1.32–3.18] | 1.40 × 10−3 | 776 | 1.94 [1.23–3.05] | 4.03 × 10−3 |
| Pathological size, pT2-3 vs. pT1 | 908 | 1.15 [0.74–1.79] | 0.536 | |||
| Pathological type, ILC vs. IDC | 909 | 0.54 [0.28–1.04] | 0.182 | |||
| Pathological type, other vs. IDC | 0.99 [0.55–1.81] | |||||
| Mol. subtype, HER2+ vs. HR+/HER2− | 909 | 2.18 [1.31–3.63] | 7.72 × 10−4 | 776 | 1.70 [0.95–3.04] | 0.073 |
| Mol. subtype, TN vs. HR+/HER2− | 2.13 [1.32–3.43] | 776 | 2.57 [1.52–4.35] | 4.35 × 10−4 | ||
| Amsterdam 70-gene risk, high vs. low | 909 | 2.46 [1.31–4.60] | 4.89 × 10−3 | 776 | 1.77 [0.92-3.41] | 0.086 |
| Recurrence Score risk, high vs. low | 909 | 1.60 [0.98–2.60] | 0.168 | |||
| Recurrence Score risk, intermediate vs. low | 1.33 [0.70–2.51] | |||||
| XIAP continuous expression | 909 | 1.59 [1.17–2.15] | 2.77 × 10−3 | 776 | 1.67 [1.20–2.31] | 2.07 × 10−3 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| n | OR [CI95] | p-Value | n | OR [CI95] | p-Value | |
| Age at diagnosis, >50 vs. ≤50 years | 1202 | 0.86 [0.68–1.10] | 0.262 | |||
| Genomic grade (GGI), high vs. low | 1203 | 2.10 [1.70–2.80] | 7.65 × 10−7 | 1203 | 1.60 [1.20–2.10] | 2.72 × 10−3 |
| Pathological type, ILC vs. IDC | 510 | 1.60 [0.63–4.30] | 0.397 | |||
| Pathological type, other vs. IDC | 510 | 0.75 [0.46–1.20] | 0.314 | |||
| Mol. subtype, HER2+ vs. HR+/HER2− | 1203 | 3.80 [2.70–5.40] | 1.12 × 10−10 | 1203 | 3.40 [2.40–4.80] | 7.85 × 10−9 |
| Mol. subtype, TN vs. HR+/HER2− | 1203 | 3.60 [2.80–4.70] | 2.22 × 10−15 | 1203 | 3.00 [2.30–4.00] | 3.96 × 10−11 |
| XIAP continuous expression | 1203 | 0.59 [0.46–0.76] | 5.12 × 10−4 | 1203 | 0.67 [0.52–0.87] | 1.28 × 10−2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devi, G.R.; Finetti, P.; Morse, M.A.; Lee, S.; de Nonneville, A.; Van Laere, S.; Troy, J.; Geradts, J.; McCall, S.; Bertucci, F. Expression of X-Linked Inhibitor of Apoptosis Protein (XIAP) in Breast Cancer Is Associated with Shorter Survival and Resistance to Chemotherapy. Cancers 2021, 13, 2807. https://doi.org/10.3390/cancers13112807
Devi GR, Finetti P, Morse MA, Lee S, de Nonneville A, Van Laere S, Troy J, Geradts J, McCall S, Bertucci F. Expression of X-Linked Inhibitor of Apoptosis Protein (XIAP) in Breast Cancer Is Associated with Shorter Survival and Resistance to Chemotherapy. Cancers. 2021; 13(11):2807. https://doi.org/10.3390/cancers13112807
Chicago/Turabian StyleDevi, Gayathri R., Pascal Finetti, Michael A. Morse, Seayoung Lee, Alexandre de Nonneville, Steven Van Laere, Jesse Troy, Joseph Geradts, Shannon McCall, and Francois Bertucci. 2021. "Expression of X-Linked Inhibitor of Apoptosis Protein (XIAP) in Breast Cancer Is Associated with Shorter Survival and Resistance to Chemotherapy" Cancers 13, no. 11: 2807. https://doi.org/10.3390/cancers13112807