
Radiomic Based Machine Learning Performance for a Three Class Problem in Neuro-Oncology: Time to Test the Waters?

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
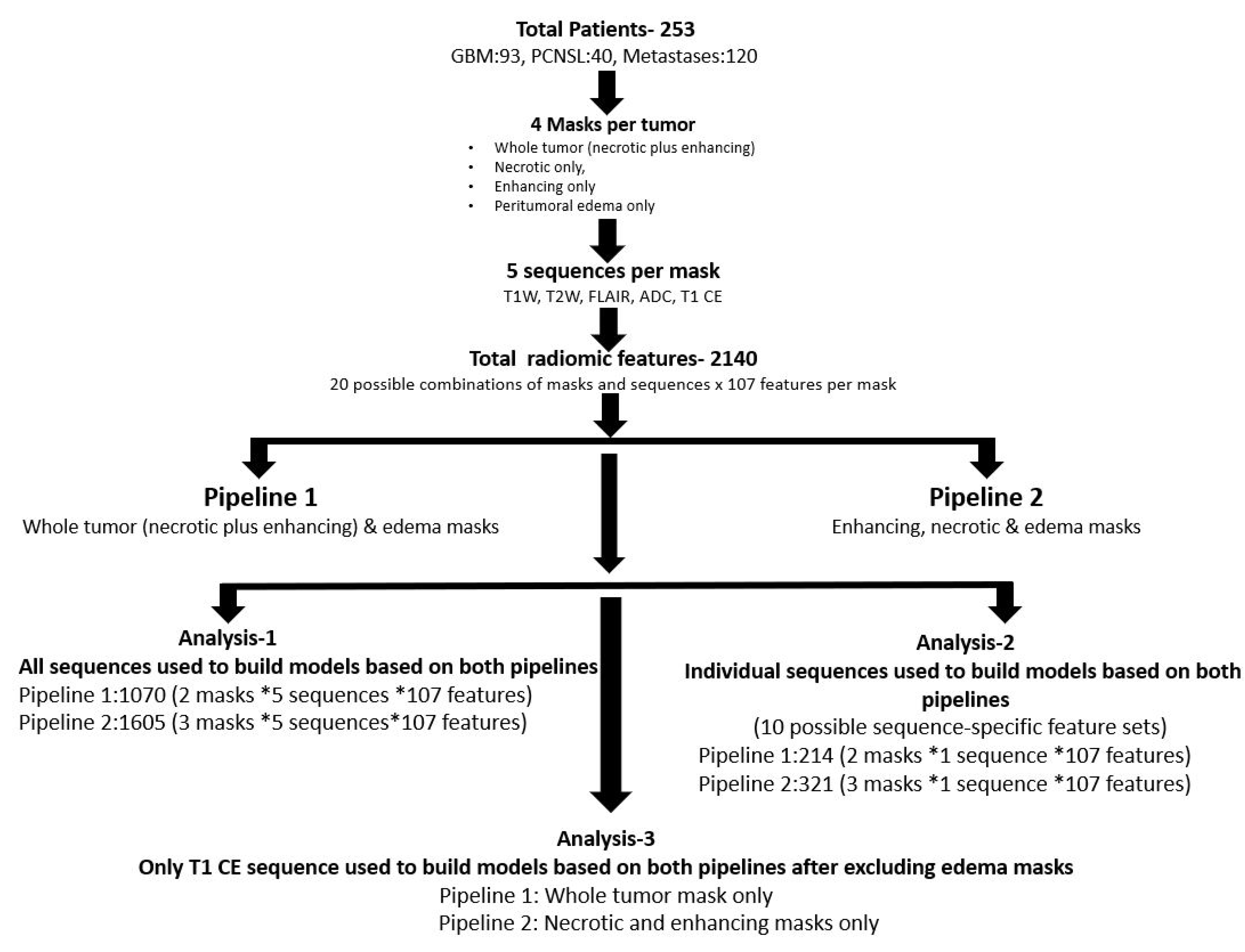
2. Materials and Methods
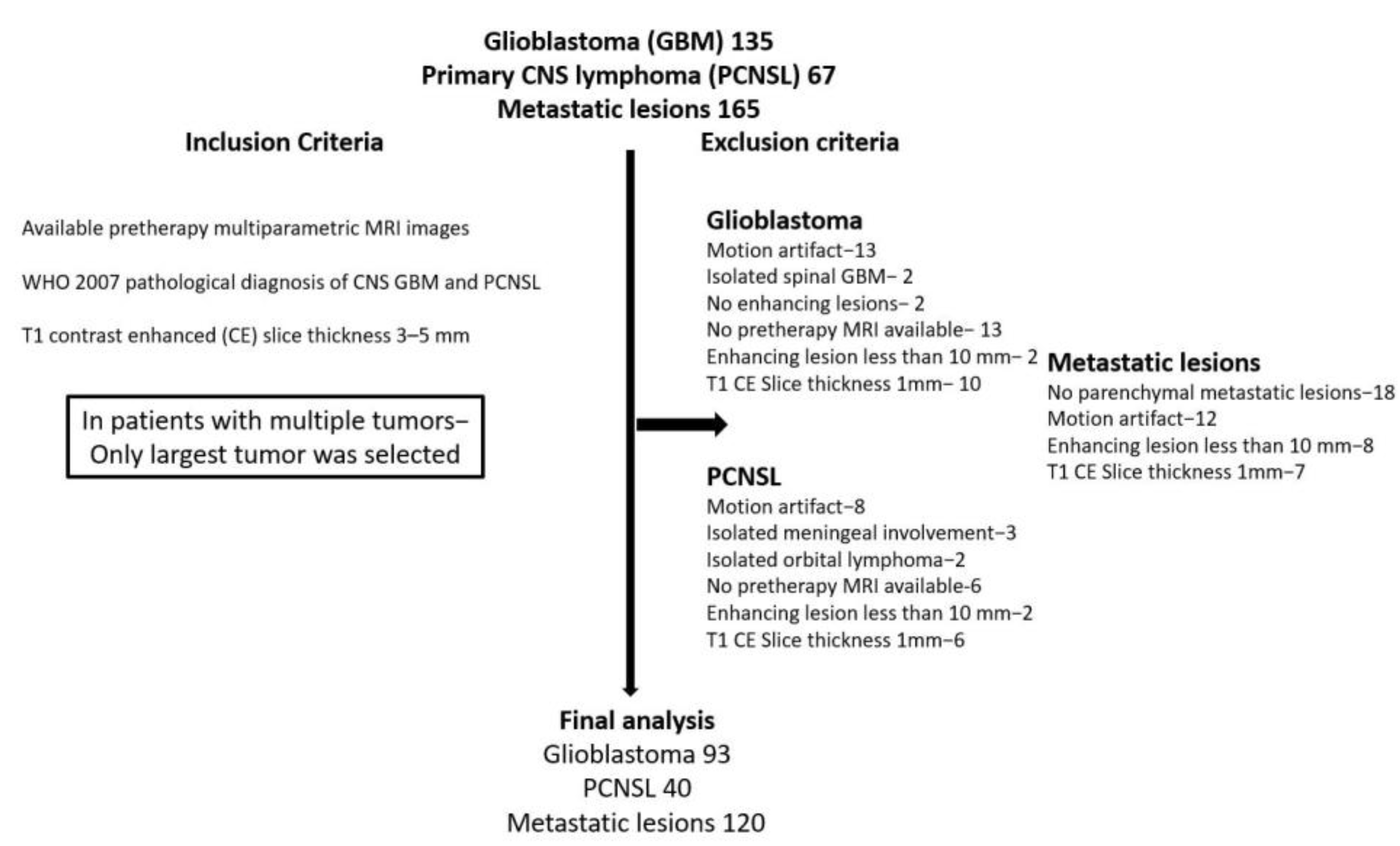
2.1. Data Collection
2.2. Image Acquisition
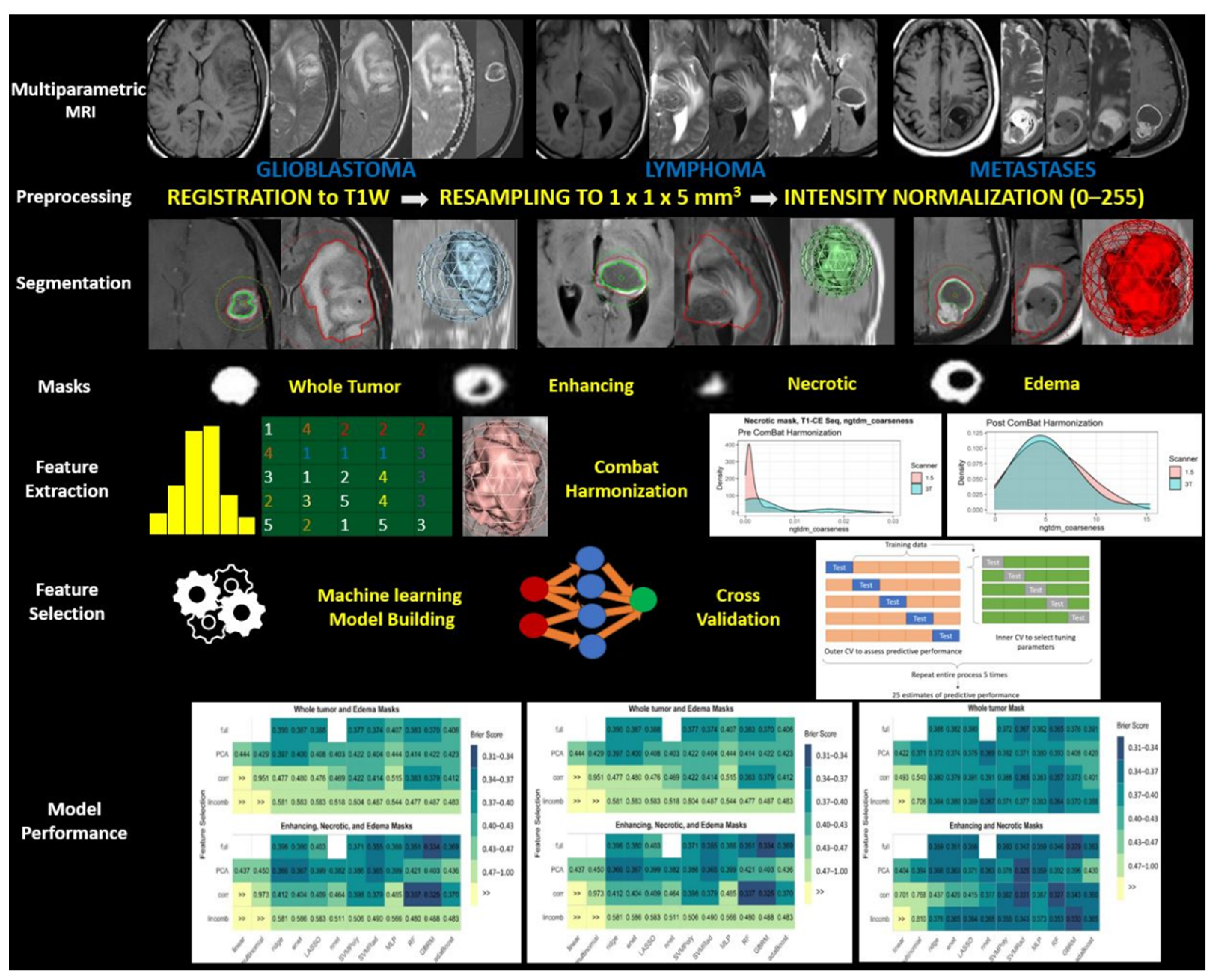
2.3. Image Pre-Processing
2.4. Tumor Segmentation/Region of Interest Delineation
2.5. Texture Feature Extraction
2.6. Feature Harmonization
2.7. Feature Selection
2.8. Model Fitting
2.9. Classifier Model Performance Evaluation
3. Statistical Analysis
4. Results
4.1. Patient Characteristics
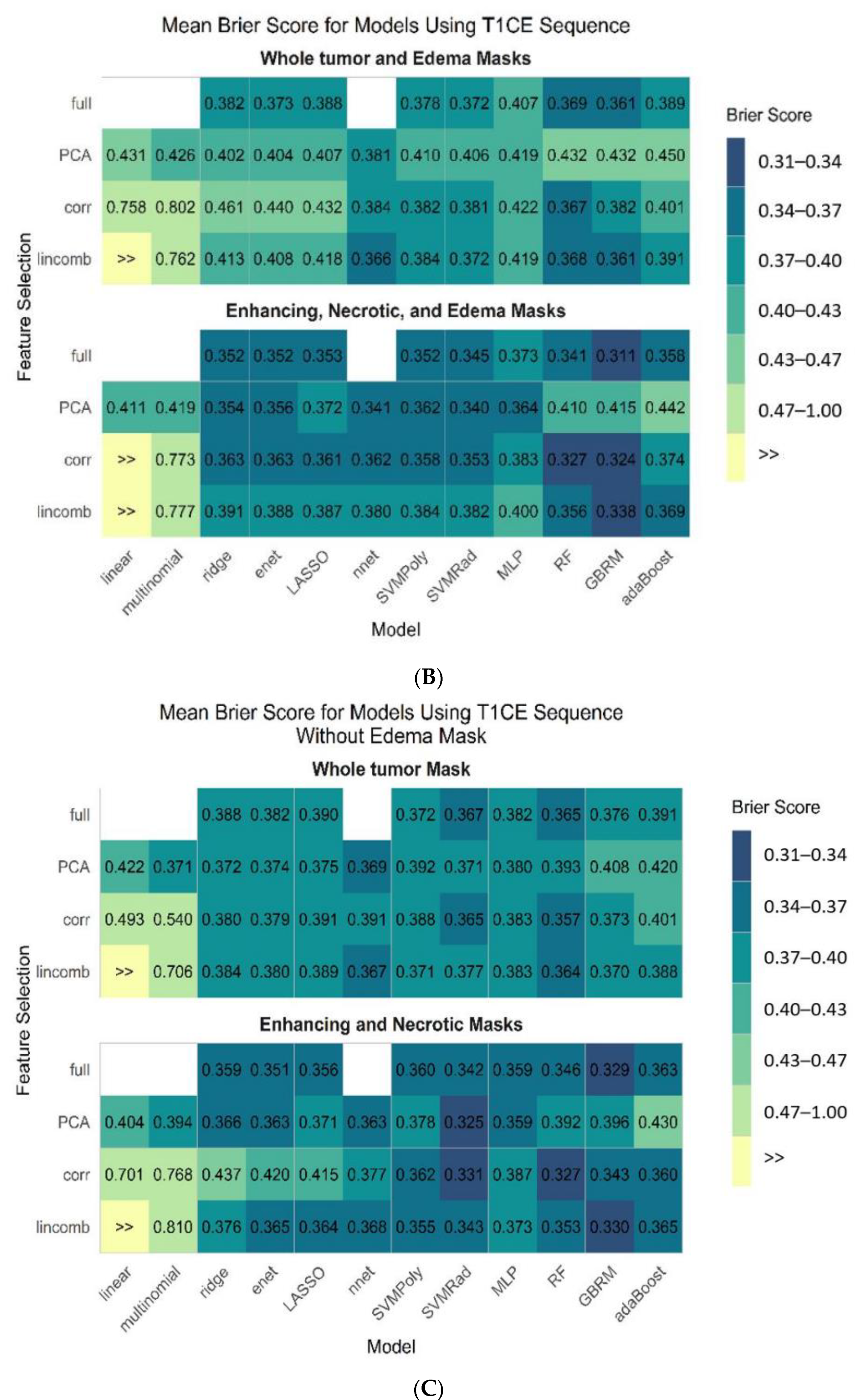
4.2. Model Performance
4.3. Tumor Subregions Performance
4.4. Comparison of Predictive Performance between Two Pipelines
4.5. Feature Importance of the Models
4.6. Confusion Matrix for the Best Performing Model
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclosures
References
- Law, M.; Cha, S.; Knopp, E.A.; Johnson, G.; Arnett, J.; Litt, A.W. High-grade gliomas and solitary metastases: Differentiation by using perfusion and proton spectroscopic MR imaging. Radiology 2002, 222, 715–721. [Google Scholar] [CrossRef]
- Soni, N.; Priya, S.; Bathla, G. Texture analysis in cerebral gliomas: A review of the literature. AJNR Am. J. Neuroradiol. 2019, 40, 928–934. [Google Scholar] [CrossRef] [Green Version]
- Neska-Matuszewska, M.; Bladowska, J.; Sąsiadek, M.; Zimny, A. Differentiation of glioblastoma multiforme, metastases and primary central nervous system lymphomas using multiparametric perfusion and diffusion MR imaging of a tumor core and a peritumoral zone-Searching for a practical approach. PLoS ONE 2018, 13, e0191341. [Google Scholar] [CrossRef] [PubMed]
- Swinburne, N.C.; Schefflein, J.; Sakai, Y.; Oermann, E.K.; Titano, J.J.; Chen, I.; Tadayon, S.; Aggarwal, A.; Doshi, A.; Nael, K. Machine learning for semi-automated classification of glioblastoma, brain metastasis and central nervous system lymphoma using magnetic resonance advanced imaging. Ann. Transl. Med. 2019, 7, 232. [Google Scholar] [CrossRef] [PubMed]
- Bander, E.D.; Jones, S.H.; Pisapia, D.; Magge, R.; Fine, H.; Schwartz, T.H.; Ramakrishna, R. Tubular brain tumor biopsy improves diagnostic yield for subcortical lesions. J. Neurooncol. 2019, 141, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Callovini, G.M.; Telera, S.; Sherkat, S.; Sperduti, I.; Callovini, T.; Carapella, C.M. How is stereotactic brain biopsy evolving? A multicentric analysis of a series of 421 cases treated in Rome over the last sixteen years. Clin. Neurol. Neurosurg. 2018, 174, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.D.; Yan, P.F.; Wang, Y.X.; Osman, M.S.; Zhao, H.Y. Glioblastoma and primary central nervous system lymphoma: Preoperative differentiation by using MRI-based 3D texture analysis. Clin. Neurol. Neurosurg. 2018, 173, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Suh, H.B.; Choi, Y.S.; Bae, S.; Ahn, S.S.; Chang, J.H.; Kang, S.G.; Kim, E.H.; Kim, S.H.; Lee, S.K. Primary central nervous system lymphoma and atypical glioblastoma: Differentiation using radiomics approach. Eur. Radiol. 2018, 28, 3832–3839. [Google Scholar] [CrossRef] [PubMed]
- Kunimatsu, A.; Kunimatsu, N.; Kamiya, K.; Watadani, T.; Mori, H.; Abe, O. Comparison between glioblastoma and primary central nervous system lymphoma using MR image-based texture analysis. Magn. Reson. Med Sci. 2018, 17, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.T.; Liu, M.X.; Chen, Z.Y. Differential Diagnostic Value of Texture Feature Analysis of Magnetic Resonance T2 Weighted Imaging between Glioblastoma and Primary Central Neural System Lymphoma. Chin. Med. Sci. J. 2019, 34, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Yun, J.; Park, J.E.; Lee, H.; Ham, S.; Kim, N.; Kim, H.S. Radiomic features and multilayer perceptron network classifier: A robust MRI classification strategy for distinguishing glioblastoma from primary central nervous system lymphoma. Sci. Rep. 2019, 9, 5746. [Google Scholar] [CrossRef] [Green Version]
- Skogen, K.; Schulz, A.; Helseth, E.; Ganeshan, B.; Dormagen, J.B.; Server, A. Texture analysis on diffusion tensor imaging: Discriminating glioblastoma from single brain metastasis. Acta Radiol. 2018, 60, 356–366. [Google Scholar] [CrossRef]
- Qian, Z.; Li, Y.; Wang, Y.; Li, L.; Li, R.; Wang, K.; Li, S.; Tang, K.; Zhang, C.; Fan, X.; et al. Differentiation of glioblastoma from solitary brain metastases using radiomic machine-learning classifiers. Cancer Lett. 2019, 451, 128–135. [Google Scholar] [CrossRef]
- Cox, R.W. AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Comput. Biomed. Res. Int. J. 1996, 29, 162–173. [Google Scholar] [CrossRef]
- Whybra, P.; Parkinson, C.; Foley, K.; Staffurth, J.; Spezi, E. Assessing radiomic feature robustness to interpolation in (18) F-FDG PET imaging. Sci. Rep. 2019, 9, 9649. [Google Scholar] [CrossRef] [Green Version]
- Lohmann, P.; Bousabarah, K.; Hoevels, M.; Treuer, H. Radiomics in radiation oncology-basics, methods, and limitations. Strahlenther. Onkol. 2020, 196, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Cho, H.H.; Lee, H.Y.; Park, H. Clinical impact of variability on CT radiomics and suggestions for suitable feature selection: A focus on lung cancer. Cancer Imaging 2019, 19, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. Image biomarker standardisation initiative-feature definitions. arXiv 2016, arXiv:1612.07003. [Google Scholar] [CrossRef] [Green Version]
- Xia, W.; Hu, B.; Li, H.; Geng, C.; Wu, Q.; Yang, L.; Yin, B.; Gao, X.; Li, Y.; Geng, D. Multiparametric-MRI-based radiomics model for differentiating primary central nervous system lymphoma from glioblastoma: Development and cross-vendor validation. J. Magn. Reson. Imaging 2021, 53, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Hu, B.; Li, H.; Shi, W.; Tang, Y.; Yu, Y.; Geng, C.; Wu, Q.; Yang, L.; Yu, Z.; et al. Deep learning for automatic differential diagnosis of primary central nervous system lymphoma and glioblastoma: Multi-parametric magnetic resonance imaging based convolutional neural network model. J. Magn. Reson. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Lim, H.; Bae, B.K.; Hahm, M.H.; Chong, G.O.; Jeong, S.Y.; Kim, J.C. Robustness of magnetic resonance radiomic features to pixel size resampling and interpolation in patients with cervical cancer. Cancer Imaging 2021, 21, 19. [Google Scholar] [CrossRef]
- Avants, B.; Tustison, N.; Song, G. Advanced normalization tools (ANTS). Insights J. 2009, 365, 335–361. [Google Scholar]
- Haga, A.; Takahashi, W.; Aoki, S.; Nawa, K.; Yamashita, H.; Abe, O.; Nakagawa, K. Standardization of imaging features for radiomics analysis. J. Med. Investig. 2019, 66, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, R.; Pane, K.; Nicolai, E.; Salvatore, M.; Franzese, M. The impact of normalization approaches to automatically detect radiogenomic phenotypes characterizing breast cancer receptors status. Cancers 2020, 12, 0518. [Google Scholar] [CrossRef] [Green Version]
- Um, H.; Tixier, F.; Bermudez, D.; Deasy, J.O.; Young, R.J.; Veeraraghavan, H. Impact of image preprocessing on the scanner dependence of multi-parametric MRI radiomic features and covariate shift in multi-institutional glioblastoma datasets. Phys. Med. Biol. 2019, 64, 165011. [Google Scholar] [CrossRef]
- Yin, Y.; Zhang, X.; Williams, R.; Wu, X.; Anderson, D.D.; Sonka, M. LOGISMOS—Layered optimal graph image segmentation of multiple objects and surfaces: Cartilage segmentation in the knee joint. IEEE 2010, 29, 2023–2037. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Ramón, R.; Ruiz-España, S.; Mollá-Olmos, E.; Moratal, D. Glioblastomas and brain metastases differentiation following an MRI texture analysis-based radiomics approach. Phys. Med. 2020, 76, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Lohmann, P.; Kocher, M.; Ceccon, G.; Bauer, E.K.; Stoffels, G.; Viswanathan, S.; Ruge, M.I.; Neumaier, B.; Shah, N.J.; Fink, G.R.; et al. Combined FET PET/MRI radiomics differentiates radiation injury from recurrent brain metastasis. NeuroImage Clin. 2018, 20, 537–542. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef]
- Orlhac, F.; Frouin, F.; Nioche, C.; Ayache, N.; Buvat, I. Validation of A method to compensate multicenter effects affecting CT radiomics. Radiology 2019, 291, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortin, J.P.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. Harmonization of multi-site diffusion tensor imaging data. NeuroImage Clin. 2017, 161, 149–170. [Google Scholar] [CrossRef]
- Fortin, J.-P. Harmonization of Multi-Site Imaging Data with ComBat, R Package Version 1.0.9. neuroCombat. 2021. Available online: https://github.com/Jfortin1/ComBatHarmonization (accessed on 5 May 2021).
- Kuhn, M.a.W.; Wickham, H. Preprocessing Tools to Create Design Matrices, R Package Version 0.1.9. 2020. Available online: https://recipes.tidymodels.org/ (accessed on 5 May 2021).
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; R Development Core Team: Vienna, Austria, 2006. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Smith, B.J. Machine Learning Models and Tools, R Package Version 2.4.0. MachineShop. 2020. Available online: https://cran.r-project.org/web/packages/MachineShop/index.html (accessed on 5 May 2021).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Kocak, B.; Durmaz, E.S.; Ates, E.; Sel, I.; Turgut Gunes, S.; Kaya, O.K.; Zeynalova, A.; Kilickesmez, O. Radiogenomics of lower-grade gliomas: Machine learning-based MRI texture analysis for predicting 1p/19q codeletion status. Eur. Radiol. 2020, 30, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Salau, A.O. An image feature selection approach for dimensionality reduction based on kNN and SVM for AkT proteins. Cogent Eng. 2019, 6, 1599537. [Google Scholar] [CrossRef]
- Parker, N.R.; Khong, P.; Parkinson, J.F.; Howell, V.M.; Wheeler, H.R. Molecular heterogeneity in glioblastoma: Potential clinical implications. Front. Oncol. 2015, 5, 55. [Google Scholar] [CrossRef]
- Tian, Q.; Yan, L.F.; Zhang, X.; Zhang, X.; Hu, Y.C.; Han, Y.; Liu, Z.C.; Nan, H.Y.; Sun, Q.; Sun, Y.Z.; et al. Radiomics strategy for glioma grading using texture features from multiparametric MRI. J. Magn. Reson. Imaging 2018, 48, 1518–1528. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X.; Feng, N.; Yin, L.; He, Y.; Xu, X.; Lu, H. The effect of glioblastoma heterogeneity on survival stratification: A multimodal MR imaging texture analysis. Acta Radiol. 2018, 59, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Di Ieva, A.; Le Reste, P.J.; Carsin-Nicol, B.; Ferre, J.C.; Cusimano, M.D. Diagnostic value of fractal analysis for the differentiation of brain tumors using 3-Tesla magnetic resonance susceptibility-weighted imaging. Neurosurgery 2016, 79, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.H.; Kim, H.S.; Rim, N.J.; Kim, S.H.; Cho, K.G. Differentiation among glioblastoma multiforme, solitary metastatic tumor, and lymphoma using whole-tumor histogram analysis of the normalized cerebral blood volume in enhancing and perienhancing lesions. Am. J. Neuroradiol. 2010, 31, 1699–1706. [Google Scholar] [CrossRef] [Green Version]
- Cindil, E.; Sendur, H.N.; Cerit, M.N.; Dag, N.; Erdogan, N.; Celebi, F.E.; Oner, Y.; Tali, T. Validation of combined use of DWI and percentage signal recovery-optimized protocol of DSC-MRI in differentiation of high-grade glioma, metastasis, and lymphoma. Neuroradiology 2020, 63, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Xi, Y.B.; Kang, X.W.; Wang, N.; Liu, T.T.; Zhu, Y.Q.; Cheng, G.; Wang, K.; Li, C.; Guo, F.; Yin, H. Differentiation of primary central nervous system lymphoma from high-grade glioma and brain metastasis using arterial spin labeling and dynamic contrast-enhanced magnetic resonance imaging. Eur. J. Radiol. 2019, 112, 59–64. [Google Scholar] [CrossRef]
- Chawla, S.; Zhang, Y.; Wang, S.; Chaudhary, S.; Chou, C.; O’Rourke, D.M.; Vossough, A.; Melhem, E.R.; Poptani, H. Proton magnetic resonance spectroscopy in differentiating glioblastomas from primary cerebral lymphomas and brain metastases. J. Comput. Assist. Tomogr. 2010, 34, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Julià-Sapé, M.; Coronel, I.; Majós, C.; Candiota, A.P.; Serrallonga, M.; Cos, M.; Aguilera, C.; Acebes, J.J.; Griffiths, J.R.; Arús, C. Prospective diagnostic performance evaluation of single-voxel 1H MRS for typing and grading of brain tumours. NMR Biomed. 2012, 25, 661–673. [Google Scholar] [CrossRef]
- Zhang, P.; Liu, B. Differentiation among glioblastomas, primary cerebral lymphomas, and solitary brain metastases using diffusion-weighted imaging and diffusion tensor imaging: A PRISMA-compliant meta-analysis. ACS Chem. Neurosci. 2020, 11, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Kim, S.; Chawla, S.; Wolf, R.L.; Knipp, D.E.; Vossough, A.; O’Rourke, D.M.; Judy, K.D.; Poptani, H.; Melhem, E.R. Differentiation between glioblastomas, solitary brain metastases, and primary cerebral lymphomas using diffusion tensor and dynamic susceptibility contrast-enhanced MR imaging. Am. J. Neuroradiol. 2011, 32, 507–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.H.; Hong, C.T.; Tsai, F.Y.; Chen, W.Y.; Chen, C.Y.; Chan, W.P. Anatomical relationships between medullary veins and three types of deep-seated malignant brain tumors as detected by susceptibility-weighted imaging. J. Chin. Med. Assoc. 2020, 83, 164–169. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | GBM | PCNSL | Metastases |
|---|---|---|---|
| Patients (253) | 93 | 40 | 120; breast (29); |
| lung (91) | |||
| Age in years (mean ± SD) | 62 ± 11 | 62 ± 13 | 62 ± 10 |
| Gender | |||
| Male | 52 | 22 | 54 |
| Female | 41 | 18 | 66 |
| Localization | |||
| Supratentorial | 91 | 33 | Breast (17); lung (62) |
| Infratentorial | 2 | 4 | Breast (6); lung (14) |
| Both | 0 | 3 | Breast (6); lung (15) |
| Multiplicity | |||
| Single | 83 | 19 | Breast (21); lung (64) |
| Two | 5 | 8 | Breast (2); lung (9) |
| ≥Two (multiple) | 5 | 13 | Breast (6); lung (18) |
| Necrosis | |||
| Yes | 92 | 10 | Breast (19); lung (68) |
| No | 1 | 30 | Breast (10); lung (23) |
| Whole Tumor and Edema Masks | Necrotic, Enhancing, and Edema Masks | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sequence | Model | Feature Selection | Brier Score Mean (95% CI) | Accuracy Mean (95% CI) | p-Value | Model | Feature Selection | Brier Score Mean (95% CI) | Accuracy Mean (95% CI) | p-Value |
| T1-CE | gbrm | full | 0.361 (0.222, 0.528) | 0.756 (0.660, 0.863) | - | gbrm | full | 0.311 (0.223, 0.466) | 0.796 (0.667, 0.880) | - |
| T1W | gbrm | full | 0.405 (0.292, 0.553) | 0.735 (0.620, 0.863) | 0.0028 | gbrm | full | 0.340 (0.231, 0.463) | 0.771 (0.680, 0.900) | 0.0155 |
| T2W | rf | corr | 0.381 (0.280, 0.481) | 0.730 (0.660, 0.804) | 0.1582 | gbrm | corr | 0.340 (0.224, 0.506) | 0.772 (0.608, 0.863) | 0.0216 |
| ADC | rf | lincomp | 0.420 (0.320, 0.520) | 0.705 (0.600, 0.784) | 0.0002 | gbrm | corr | 0.349 (0.197, 0.505) | 0.756 (0.686, 0.843) | 0.0034 |
| FLAIR | rf | full | 0.418 (0.334, 0.511) | 0.699 (0.608, 0.765) | <0.0001 | gbrm | full | 0.353 (0.242, 0.479) | 0.768 (0.680, 0.863) | 0.0092 |
| Using All (Multiparametric MRI) Sequences | ||||||||||||
| Rank | Masks | Model | Feature Selection | Mean Brier | 95% CI Brier | Mean Multi-AUC | 95% CI Multi-AUC | |||||
| 1 | N, E, edema | gbrm | corr | 0.325 | (0.232, 0.488) | 0.910 | (0.833, 0.959) | |||||
| 2 | N, E, edema | gbrm | full | 0.334 | (0.215, 0.434) | 0.900 | (0.832, 0.963) | |||||
| 3 | N, E, edema | rf | corr | 0.337 | (0.269, 0.455) | 0.899 | (0.805, 0.948) | |||||
| 4 | N, E, edema | rf | full | 0.351 | (0.278, 0.466) | 0.893 | (0.819, 0.962) | |||||
| 5 | N, E, edema | svmRad | full | 0.355 | (0.259, 0.468) | 0.878 | (0.762, 0.947) | |||||
| Using T1-CE Sequence | ||||||||||||
| Rank | Masks | Model | Feature Selection | Mean Brier | 95% CI Brier | Mean Multi-AUC | 95% CI Multi-AUC | |||||
| 1 | N, E, edema | gbrm | full | 0.311 | (0.223, 0.466) | 0.908 | (0.820, 0.959) | |||||
| 2 | N, E, edema | gbrm | corr | 0.324 | (0.229, 0.430) | 0.904 | (0.841, 0.964) | |||||
| 3 | N, E, edema | rf | corr | 0.327 | (0.265, 0.451) | 0.907 | (0.808, 0.954) | |||||
| 4 | N, E, edema | gbrm | lincomb | 0.338 | (0.225, 0.541) | 0.892 | (0.797, 0.950) | |||||
| 5 | N, E, edema | svmRad | PCA | 0.340 | (0.253, 0.443) | 0.894 | (0.824, 0.955) | |||||
| Using T1-CE Sequence without Edema Mask | ||||||||||||
| Rank | Masks | Model | Feature Selection | Mean Brier | 95% CI Brier | Mean Multi-AUC | 95% CI Multi-AUC | |||||
| 1 | N, E | svmRad | PCA | 0.325 | (0.255, 0.485) | 0.894 | (0.255, 0.485) | |||||
| 2 | N, E | rf | corr | 0.327 | (0.261, 0.458) | 0.905 | (0.261, 0.458) | |||||
| 3 | N, E | gbrm | full | 0.329 | (0.230, 0.473) | 0.902 | (0.230, 0.473) | |||||
| 4 | N, E | gbrm | lincomb | 0.330 | (0.219, 0.446) | 0.901 | (0.219, 0.446) | |||||
| 5 | N, E | svmRad | corr | 0.331 | (0.237, 0.425) | 0.895 | (0.237, 0.425) | |||||
| Sequence | Whole Tumor and Edema Masks | Necrotic, Enhancing, and Edema Masks | ||||||
|---|---|---|---|---|---|---|---|---|
| Model | Feature Selection | Brier Score Mean (95% CI) | Accuracy Mean (95% CI) | Model | Feature Selection | Brier Score Mean (95% CI) | Accuracy Mean (95% CI) | |
| All sequences | gbrm | full | 0.370 (0.236, 0.460) | 0.732 (0.627, 0.824) | gbrm | corr | 0.325 (0.232, 0.488) | 0.771 (0.608, 0.843) |
| T1-CE | gbrm | full | 0.361 (0.222, 0.528) | 0.756 (0.660, 0.863) | gbrm | full | 0.311 (0.223, 0.466) | 0.796 (0.667, 0.880) |
| T1-CE without edema mask | rf | corr | 0.357 (0.262, 0.443) | 0.752 (0.620, 0.843) | svmRad | PCA | 0.325 (0.255, 0.485) | 0.782 (0.686, 0.860) |
| Observed Tumor Type | ||||
|---|---|---|---|---|
| Predicted | Metastatic | PCNSL | GBM | Total |
| Metastatic | 39.1% | 4.5% | 5.1% | 48.7% |
| PCNSL | 2.5% | 9.8% | 1.0% | 13.3% |
| GBM | 5.8% | 1.5% | 30.7% | 38.0% |
| Total | 47.4% | 15.8% | 36.8% | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priya, S.; Liu, Y.; Ward, C.; Le, N.H.; Soni, N.; Pillenahalli Maheshwarappa, R.; Monga, V.; Zhang, H.; Sonka, M.; Bathla, G. Radiomic Based Machine Learning Performance for a Three Class Problem in Neuro-Oncology: Time to Test the Waters? Cancers 2021, 13, 2568. https://doi.org/10.3390/cancers13112568
Priya S, Liu Y, Ward C, Le NH, Soni N, Pillenahalli Maheshwarappa R, Monga V, Zhang H, Sonka M, Bathla G. Radiomic Based Machine Learning Performance for a Three Class Problem in Neuro-Oncology: Time to Test the Waters? Cancers. 2021; 13(11):2568. https://doi.org/10.3390/cancers13112568
Chicago/Turabian StylePriya, Sarv, Yanan Liu, Caitlin Ward, Nam H. Le, Neetu Soni, Ravishankar Pillenahalli Maheshwarappa, Varun Monga, Honghai Zhang, Milan Sonka, and Girish Bathla. 2021. "Radiomic Based Machine Learning Performance for a Three Class Problem in Neuro-Oncology: Time to Test the Waters?" Cancers 13, no. 11: 2568. https://doi.org/10.3390/cancers13112568